
Abstract
Objectives
Diet may influence biochemical pathways involved in age-related changes in body composition and physical function. This study aimed to describe dietary patterns and their relationships with body composition, physical performance, and grip strength according to age and sex.
Design
Cross-sectional study.
Setting
Data were collected in the Clinical Research Center (CRC) of the Gérontopôle of the Centre Hospitalier Universitaire (CHU) of Toulouse or at participants’ homes when unable to attend the research facilities.
Participants
470 (63% female) people with a median age of 56 (38–70) years.
Measurements
The “Mediterranean-like” (i.e., plant-based foods, dairy), “Animal products” (i.e., meat, processed meat, butter, refined starch), and “Sugar and fast food” (i.e., ultra-processed and sugary foods) dietary patterns were extracted by principal component analysis. Total and trunk fat mass indexes (kg/m2), and total and appendicular lean mass indexes (kg/m2) were assessed by DXA. The physical tests comprised gait speed (m/sec), chair rise (sec), the Short Physical Performance Battery test (/12 points), and handgrip strength (kg). The associations were explored through multivariate linear regressions by sex and age groups: ≥20 to <50, ≥50 to <65, and ≥65 years.
Results
Men and women had higher adherence to the “Sugar and fast food” diet in the youngest group. Middle-aged and older women adhered more to a “Mediterranean-like” diet. Men kept a “Sugar and fast food” diet when middle-aged and changed to the “Animal products” diet when ≥65 years. Higher adherence to the “Mediterranean-like” diet was associated with lower BMI, body fat, and lean mass in middle-aged men. Higher adherence to the “Animal products” diet was associated with higher lean mass in middle-aged women, more trunk fat in young men, lower strength in middle-aged men, and higher strength in older men. Higher adherence to the “Sugar and fast food” diet was associated with higher body fat in middle-aged men but lower body fat in older men.
Conclusion
Diets composed of sugary foods, fast foods, and processed meat were associated with higher fat mass and lower strength. Men were more prone to have less healthy food intake in all age groups.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Changes in body composition happen with aging. Muscle mass tends to decrease (1), resulting in a reduced basal metabolic rate that favors an increase in body weight (2). Fat mass is redistributed in favor of a higher deposition in the abdomen. Greater adiposity in this region is associated with oxidative stress and inflammation, increasing the risk for chronic diseases (3). Fat redistribution also impacts the quality and quantity of lean mass (4), which can result in sarcopenia (1) and frailty (5).
The pattern of changes in body composition, however, can differ according to the sex (6–8): in a large cohort of US citizens, the fat mass increased monotonically up to age 85 in men, and in women, the peak occurred at age 65 (6). Another potential influencer is the environment (9). The comparison of cohorts of different generations indicates that the more recent the cohort birth, the more prevalent or higher the chance of obesity (9–11). This difference may be a result of an obesogenic environment (9), suggesting that what we eat could accelerate or intensify the “natural” changes in our body composition. Beyond calories, food contains nutrients and bioactive compounds that influence the hallmarks of aging (12). Thus, by affecting inflammation, oxidative stress, or the cellular capacity for damage repair (13), food components could impact not only body composition but also physical function.
Studying the role of the diet through dietary patterns encompasses the complexity of the overall diet (i.e., nutrient interactions and cultural aspects). Several studies have associated different dietary patterns with improvements in clinical outcomes of aging (14–17). Diets rich in fruits, vegetables, whole grain cereals, and low-fat milk have been associated with lower body fat and Body Mass Index (BMI). The contrary has been observed among people with higher adherence to dietary patterns mainly composed of meat (18). Regarding physical function, greater adherence to the “Mediterranean-Dietary Approaches to Stop Hypertension (DASH) Intervention for Neurodegenerative Delay (MIND)” was demonstrated to slow down functional decline and maintain muscle strength over time (19).
The evidence is still scarce when comparing dietary patterns across different age groups. Inelmen et al. compared the dietary habits of Italians with obesity/overweight from three age ranges: 18 to 34 years, 35 to 64 years, and 65 years or older. The authors found that whether the youngest group tended to eat more sweets and fewer fruits and vegetables, the oldest groups ate lean fish more often (20). However, we did not find a similar approach considering several components of body composition and physical function as outcomes. Thus, we aimed to investigate the cross-sectional associations of dietary patterns with body composition, physical performance, and strength in a wide age range of adults (from 20 to 80+), exploring the differences between the sexes. Additionally, we explored the potential mediating role of body composition in the diet-physical function associations.
Methods3
Participants
The present study comprised participants from the INStitute for Prevention healthy agIng and REjuvenative medicine Human Translational Cohort (INSPIRE-T cohort). The INSPIRE-T cohort is an ongoing cohort that includes persons of 20 years or older, with no upper limit of age. It consists of a 10-year observational study with follow-up visits regularly scheduled to assess biological, clinical, digital, and imaging data (21).
People were excluded from the INSPIRE-T cohort if they were not affiliated with social security, had a disease compromising life expectancy at 5 years (or 1 year for those in nursing homes), and if they were under administrative or juridical protection, guardianship, or supervision. For the present study, we further excluded those with missing valid information on dietary intake, or the outcomes (i.e., body composition, physical performance, and strength), those on hemodialysis, with moderate or severe hepatopathy, bad oral health, food allergy, and present or past anorexia or cancer (Figure 1). The cohort was divided into three groups to explore the differences in the outcomes of interest according to age: ≥20 to <50 years, ≥50 to <65 years, and ≥65 years.

Flow chart of the study. OHAT: Oral Health Assessment Tool
Study design and procedures
This cross-sectional study was performed with baseline data from the first wave of the INSPIRE-T cohort, which started on October 2019. All participants gave their written consent, and the study protocol was approved by the French Ethical Committee in Rennes (CPP Ouest V). The study protocol is available at “clinicaltrials.gov” under the registration code NCT04224038.
Data collection
Data were collected by trained clinical research members in either the Clinical Research Center (CRC) of the Gérontopôle of the Centre Hospitalier Universitaire (CHU) of Toulouse or at participants’ homes (when unable to attend the research facilities).
Outcomes
Anthropometric and body composition measurements
Weight (kg) and height (m) were assessed, followed by the calculation of the body mass index (BMI; kg/m2). Total body and trunk fat mass (kg), and total and appendicular lean mass (i.e., the sum of the lean mass in the arms and legs; kg) were assessed by Dual Energy X-Ray absorptiometry (DXA; GE Healthcare Lunar iDXA). To avoid the influence of body size, the body composition was adjusted for height squared (m2), obtaining the total (FMI; kg/m2) and the trunk fat mass indexes (Trunk FMI; kg/m2), and the total (LMI; kg/m2) and the appendicular lean mass indexes (Appendicular LMI; kg/m2) (1).
Physical function measurements
Physical function comprised the following indicators of performance and strength: gait speed, time to rise five times from a chair, the Short Physical Performance Battery (SPPB), and grip strength. Gait speed was recorded from participants walking at their usual pace at a 4-meter distance (the use of assistive devices was allowed if necessary). The faster of two attempts was used for calculating gait speed (meters/second) (22). For the time to rise five times from a chair test (seconds), participants were asked to stand up and sit down five times as quickly as possible on a straight-backed chair without armrests. Participants’ arms should be kept crossed over the chest during the attempts. The time from the initial sitting to the final standing position at the end of the fifth stand was recorded with a stopwatch and used for analysis (22).
The SPPB test included the two previous tests (gait speed, time to rise five times) and static balance. The balance test started with the participant standing in semi-tandem. If the participant could stay in this position for 10 seconds, a further full tandem position was tested (10 seconds). If the participant could not hold the semi-tandem for 10 seconds, the assessment was performed with the feet in the side-by-side position. The static balance test resulted in a score of 0 to 4 (22). A score of 0 to 4 was also assigned for gait speed and time to rise five times tests: those who could not complete the test were scored with 0; those who completed the test received a score of 1 to 4, according to the quartiles of needed time to complete the test. SPPB scores ranged from 0 to 12 (higher is better) (22). Grip strength was the maximum isometric strength on a hydraulic hand-held dynamometer Jamar®. After a learning trial, two attempts were performed with both hands with the participants in the standard position: “seated in a chair with the shoulder adducted and neutrally rotated, elbow flexed at 90°, and the forearm and wrist in a neutral position” (23).
Dietary data
The habitual food referred to the previous four months’ intake was assessed with a non-quantitative Food Frequency Questionnaire (FFQ) -developed based on the study of Estaquio et al. with a large sample of French adults (24). The frequencies of consumption (never or rarely; less than once a week; once a week; two or three times a week; four to six times a week; once or more a day) were converted to a daily frequency (0; 0.071; 0.143; 0.358; 0.714; 1 or more times per day) to standardize the variables for the extraction of the dietary patterns. The conversion to a daily frequency has been made by dividing the weekly frequency (or the mean when a range was asked) by 7 days.
The 34 food items of the FFQ were reduced into 18 food groups (Table S1), followed by a data-driven principal component analysis (PCA). The PCA calculates the inter-correlation between the food groups to combine those mostly related to generate the dietary patterns (factors). Three main dietary patterns were retained based on the eigenvalue greater than 1.30 (25) and the examination of the breaking point in the scree plot (26). The adequacy was confirmed by the significant Bartlett test of sphericity (p < 0.001) and by a Kaiser-Meier-Olkin (KMO) test equal to 0.573 (0.5 is the minimal acceptable) (27).
After being rotated by the orthogonal transformation VARIMAX (maximize the differences), the food groups with an absolute factor loading >0.30 were retained for the interpretation of the dietary patterns (28). The label of each pattern was based on the foods most strongly correlated to it. The level of compliance of the participants to the dietary patterns is represented by the factor score (the sum of the consumption frequency of all food groups weighted by the food group factor loading), with a higher factor score meaning better compliance to the dietary pattern. The food groups with a negative factor loading were kept presenting the complexity of eating habits.
Three dietary patterns were extracted: 1) “Mediterranean-like”, characterized by positive factor loadings for legumes, dairy products, wholegrain cereals, fruits, vegetables, and vegetal oil; 2) “Animal products”, consisting of positive factor loadings for meat and poultry, charcuterie, refined cereals, and butter or margarine, and a negative factor loading for breakfast cereals; and 3) “Sugar and fast food”, in which there were positive loadings for salted biscuits, pre-prepared and fast foods, soft drinks, desserts, sweets and pastries, and a negative loading for fish (Tables S1 and S2).
Covariates
The following confounding factors were assessed by questionnaires and considered in the adjusted models: visit date (to control potential seasonal bias on dietary intake), number of medications, presence or absence of hypertension and/or diabetes (compiled as “common non-communicable chronic diseases”), presence or absence of depression, educational level (i.e., higher or lower than a college degree), living status (i.e., living alone or living not alone), and physical activity during leisure time (min/week) assessed by the International Physical Activity Questionnaire (IPAQ) (29).
Extremes values in the leisure time physical activity were identified using the Tukey’s method, with values above three interquartile range from the third quartile value excluded from the analysis to avoid any impact on the linear regressions (30).
Statistical analysis
The distribution of the continuous variables was checked through the Shapiro-Wilk test. As all the continuous variables did not follow a Gaussian distribution they were expressed as median (interquartile range). The binary and categorical variables were indicated as absolute (n) and relative (%) numbers.
The characteristics of the participants were compared across the three age groups by Chi-square for categorical data and by Kruskal-Wallis for continuous data. The adherence to each dietary pattern was explored according to the age groups through the Kruskal-Wallis test and the sex using the Wilcoxon Rank Sum test. The associations of body composition and physical function with each dietary pattern were assessed by multiple linear regression models stratified by sex and age group and adjusted for the covariates previously described. The robust Maximum Likelihood method was used when the distribution of the residuals was not Gaussian. The models were corrected for multiple comparisons by the Benjamini-Hochberg procedure with a false discovery rate (FDR) of 0.25 (31), and the corrections are exposed in Table S6. The effect size of all significant results was calculated using the Cohen’s f2 effect size (small: ≥0.10; medium: ≥0.25; large: ≥0.40) (32).
A secondary analysis was performed to verify if the associations between the dietary patterns, physical performance, and muscle strength were mediated by body composition (FMI and appendicular LMI). The mediation analysis was built using the structural equation modeling framework to draw the direct pathway (links the dietary patterns and the physical function while adjusts for body composition) and the indirect pathway (links the dietary pattern to physical function through the body composition) (33). The models included the same covariates of the linear regression, except visit date, which is only related to the diet but not to the other outcomes of the model (Figure S1). The model goodness of fit was demonstrated by a Standardized Root Mean Square Residual (SRMR) score lower than 0.08. Other indexes exist but SRMR was the only one that could be executed since the robust Maximum Likelihood method was applied to the model.
In the case where grip strength was associated to a dietary pattern, exploratory analysis on muscle quality (i.e., the ratio of muscle strength to muscle mass in the arms) could be performed to deepen the results and the information on the relationships between muscle and dietary pattern.
All the statistical analyses were undertaken using the Stata Software package (StataCorp LLC, College Station, Texas, USA) version 17, and the level of statistical significance was reached for p-values < 0.05.
Results
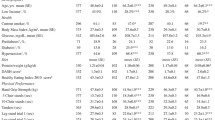
The present study encompassed 470 participants (63% female), median age 56 (IQR: 38–70) years. All socioeconomic and lifestyle variables significantly differed among age groups, except sex and the leisure time spent in physical activities, which was in average 180 minutes per week (Table 1). The indicators of fat mass increased with the increase of age, and no difference was observed in terms of lean mass. However, the oldest group showed significantly lower physical performance and grip strength (Table 1). Regarding the diet, we observed greater adherence to the “Sugar and fast food” dietary pattern in the youngest group of women and men (≥20 and <50 years). After this age range, the diet profile differed between the sexes: women had better adherence to the “Mediterranean-like” diet in the middle and older age groups; men maintained greater adherence to the “Sugar and fast food” dietary pattern until the age 65 and then switched to the “Animal products” dietary pattern (Figure 2 and Table S3).

Dietary patterns adherence according to the age groups and sex
Dietary patterns, body composition, physical performance, and muscle strength
The associations between dietary patterns and body composition (Table 2) and physical performance and grip strength (Table 3) were explored in each age group according to sex.
Young group (≥20 to <50 years old)
In young women, no dietary pattern was associated with body composition, physical performance, or grip strength. In young men, a higher intake of “Animal products” was associated with higher fat mass in the trunk.
Middle-aged group (≥50 to <65 years old)
In middle-aged women, a higher intake of “Animal products” was significantly associated with greater total lean mass.
Among middle-aged men, greater adherence to the “Mediterranean-like” diet was associated with lower BMI, fat (total and in the trunk), and lean mass (total and appendicular). On the other hand, a greater intake of a “Sugar and fast food” diet was associated with higher fat mass (total and in the trunk). Greater intake of «Animal products» was associated with lower grip strength.
Older group (≥65 years old)
In older women, no dietary pattern was significantly associated with body composition, physical performance, or grip strength.
The older men with greater adherence to the “Sugar and fast food” diet showed lower fat mass (total and in the trunk), while higher intake of the “Animal products” diet was associated with higher grip strength.
Secondary analysis
The Structural Equation Modeling (SEM) indicated that the significant associations between “Animal products” dietary pattern and strength were not mediated by fat mass or appendicular lean mass (they were significant through the direct pathway, but not through indirect pathways) (Figure S1 and Table S4).
As the direction of the association between the “Animal products” diet and grip strength was opposite between middle-aged and older men, we further explored the relationship of this dietary pattern with muscle quality in these groups (Table S5). Greater adherence to the “Animal products” diet was significantly associated with lower muscle quality in middle-aged men (β: -0.42, 95%CI: −0.75 to −0.10), but with better muscle quality in older men (β: 0.16, 95%CI: 0.03 to 0.29).
Discussion
The pattern of food intake differed across the age-ranges and according to the sex. Men and women showed higher adherence to the “Sugar and fast food” diet in the youngest age range. After this age, however, the pattern of adherence changed: women adhered more to a “Mediterranean-like” diet in both middle-aged (≥50 to <65 years) and older groups (≥65 years); men kept in “Sugar and fast food” diet when middle-aged, and changed to greater adherence to the “Animal products” dietary pattern after age 65. The dietary patterns were significantly associated with body composition and physical function, especially in men in middle age. The more adherence to a “Mediterranean-like” diet, the lower BMI and body fat, but also lean mass in middle-aged men. A higher intake of “Animal products” was associated with higher lean mass in middle-aged women but with a higher trunk fat in young men. Regarding physical function, while a higher intake of this dietary pattern was associated with lower grip strength in middle-aged men, in older men it was associated with greater strength. Opposite associations were also observed for the “Sugar and fast food” dietary pattern among men: greater adherence was associated with higher body fat in middle-aged group and lower body fat in the older group.
The preference for a diet rich in ultra-processed foods and lacking fruits and vegetables, as the “Sugar and fast food” dietary pattern, is often related to the low cost of these foods, lack of time, skills, and facilities to cook, their widespread presence, preferred taste, and emotional responses (34). As the food components of this dietary pattern are energy-dense (35), it is not a surprise that greater intake has been associated with higher fat mass, as observed in the middle-aged men. These findings are in accordance with pooled data from cross-sectional studies that indicated a 39% higher risk of overweight/obesity with the highest consumption of ultra-processed foods (36). In addition, in a crossover randomized controlled trial the ad libitum consumption for two weeks of an ultra-processed diet resulted in an energy intake 500 kcal higher than the alternate diet. As a result, participants had their body weight increased by ~1kg and body fat by ~0.5kg (37).
It is important to mention that among men over 65 years, greater adherence to the “Sugar and fast food” dietary pattern was significantly associated with reduced body fat, suggesting a risk of malnutrition (38). Ultra-processed foods are poor in proteins, fibers, micronutrients, and bioactive compounds (35). Thus, the “Sugar and fast food” dietary pattern may not provide enough essential nutrients for this stage of life (35). In older adults, the consumption of ultra-processed foods was already reported to increase the risk of frailty (39) and grip strength decline (40).
A higher intake of the “Animal products” diet was associated with higher lean mass in middle-aged women but with a higher trunk fat in young men and reduced grip strength in middle-aged men. Meat is an important food source of high-quality protein and B vitamins essential to skeletal muscle; however, it also contains high amounts of saturated (SFA) and trans fatty acids (FA), especially when red-processed (which was the main type of meat in this dietary pattern). SFA and trans FA increase the circulating levels of pro-inflammatory markers (41). We confirmed that in middle-aged men, higher intake of “Animal products” was associated with lower muscle quality. Myosteatosis and the local inflammation as consequence of the SFA and trans fatty acids intake can lead to mitochondrial dysfunction, compromising the synthesis of ATP and increasing the levels of reactive oxygen species (ROS) (42). This scenario favors the development of insulin resistance (IR) and impairs the fiber contractility, essential to muscle strength (43). It has been demonstrated that the aging-associated immune-inflammatory changes occur first in men than in women, which may explain the negative association at an early age for men (44).
The intake of processed meat (e.g. ham, bacon, sausages) have been associated with lower grip strength in the literature (45). Processed meat has been additionally related to increased risk of frailty (46) and to impaired agility and lower-extremity physical function (47). It is noteworthy that among older men, the relationship between the “Animal products” diet and grip strength was opposite of that of middle-aged men. In the older group, higher intake of this dietary pattern was associated with higher grip strength and better muscle quality. A potential hypothesis emerges from the concept of the “muscle clock”, in which the time of day when the intake of proteins occurs influences muscle response: the higher the intake at breakfast, the higher the grip strength compared to when protein is eaten primarily at dinner (48). It has been observed that the percentage of protein intake at breakfast tends to be significantly higher in older adults compared to middle-aged counterparts (49).
On the contrary, the substitution of processed meat with fish, legumes, dairy, or nuts has been associated with a reduced risk of functional impairment (46, 47). Since the foods contained in the “Mediterranean-like” diet are rich in antioxidants and nutrients with anti-inflammatory properties, this could mitigate the increased inflammatory environment associated with aging. In our population, however, the results are conflicting. In middle-aged men, a higher adherence to this diet was associated with lower body fat and lower lean mass. This finding suggests that at least for men, the amount of protein achieved with the “Mediterranean-like” dietary pattern may is not enough, requiring either increasing the protein sources presented in this diet (e.g., legumes and dairy) or including other foods rich in protein but low in fat, such as lean meat and eggs.
The major limitation of this study is the cross-sectional design: it does not allow us to determine any causality; we cannot trace the trajectory of the changes in dietary pattern adherence, body composition, and physical performance and strength; it can lead to “unexpected” results. Applying a retrospective food questionnaire has intrinsic bias related to memory; in addition, the use of a non-quantitative FFQ makes it unfeasible to estimate the nutritional intake of the participants. The results of this study should be interpreted with caution, as it is based on a population with higher economic and educational levels and with a good global lifestyle. Despite these limitations, this study provides concise information on the role of eating habits on body composition, physical performance, and muscle strength in a wide age range of men and women, corroborating in the understanding of the changes observed with aging. Future analysis from INSPIRE cohort will allow us to confirm the associations.
Conclusions
We found different profiles of food intake between men and women in the age groups, with men being more prone to a less healthy food intake in all ages. The dietary patterns were significantly associated with body composition and physical function mainly in middle age. Diets composed of sugary foods, fast foods, and processed meat were associated with higher fat mass and lower grip strength. This work reinforce the need for preventive strategies to reduce the intake of ultra-processed foods and high-fat meat to minimize the impact of aging on body composition and physical function. Furthermore, these preventive strategies should be adapted according to the sex since their differences in dietary habits and food preferences.
Availability of data and materials: The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European Consensus on Definition and Diagnosis. 2019, 48, 16, doi:https://doi.org/10.1093/ageing/afy169.
JafariNasabian, P.; Inglis, J.E.; Reilly, W.; Kelly, O.J.; Ilich, J.Z. Aging Human Body: Changes in Bone, Muscle and Body Fat with Consequent Changes in Nutrient Intake. J. Endocrinol. 2017, 234, R37–R51, doi:https://doi.org/10.1530/JOE-16-0603.
Tzanetakou, I.P.; Katsilambros, N.L.; Benetos, A.; Mikhailidis, D.P.; Perrea, D.N. “Is Obesity Linked to Aging?”: Adipose Tissue and the Role of Telomeres. Ageing Res. Rev. 2012, 11, 220–229, doi:https://doi.org/10.1016/j.arr.2011.12.003.
Melton, L.J.; Khosla, S.; Crowson, C.S.; O’Connor, M.K.; O’Fallon, W.M.; Riggs, B.L. Epidemiology of Sarcopenia. J. Am. Geriatr. Soc. 2000, 48, 625–630.
Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in Older Adults: Evidence for a Phenotype. J. Gerontol. Ser. A 2001, 56, M146–M157, doi:https://doi.org/10.1093/gerona/56.3.M146.
Kelly, T.L.; Wilson, K.E.; Heymsfield, S.B. Dual Energy X-Ray Absorptiometry Body Composition Reference Values from NHANES. PLOS ONE 2009, 4, e7038, doi:https://doi.org/10.1371/journal.pone.0007038.
Kirk, B.; Bani Hassan, E.; Brennan-Olsen, S.; Vogrin, S.; Bird, S.; Zanker, J.; Phu, S.; Meerkin, J.D.; Heymsfield, S.B.; Duque, G. Body Composition Reference Ranges in Community-Dwelling Adults Using Dual-Energy X-Ray Absorptiometry: The Australian Body Composition (ABC) Study. J. Cachexia Sarcopenia Muscle 2021, 12, 880–890, doi:https://doi.org/10.1002/jcsm.12712.
Xiao, Z.; Guo, B.; Gong, J.; Tang, Y.; Shang, J.; Cheng, Y.; Xu, H. Sex- and Age-Specific Percentiles of Body Composition Indices for Chinese Adults Using Dual-Energy X-Ray Absorptiometry. Eur. J. Nutr. 2017, 56, 2393–2406, doi:https://doi.org/10.1007/s00394-016-1279-9.
Allman-Farinelli, M.A.; Chey, T.; Bauman, A.E.; Gill, T.; James, W.P.T. Age, Period and Birth Cohort Effects on Prevalence of Overweight and Obesity in Australian Adults from 1990 to 2000. Eur. J. Clin. Nutr. 2008, 62, 898–907, doi:https://doi.org/10.1038/sj.ejcn.1602769.
Reither, E.N.; Hauser, R.M.; Yang, Y. Do Birth Cohorts Matter? Age-Period-Cohort Analyses of the Obesity Epidemic in the United States. Soc. Sci. Med. 1982 2009, 69, 1439–1448, doi:https://doi.org/10.1016/j.socscimed.2009.08.040.
Wong, T.-J.; Yu, T.; Chang, L.-Y.; Lao, X.Q. Birth Cohort, Sex and Educational Disparities in the Trajectories of Body Mass Index in Taiwan: A Longitudinal Study. BMC Public Health 2022, 22, 409, doi:https://doi.org/10.1186/s12889-022-12762-4.
Sierra, F. The Emergence of Geroscience as an Interdisciplinary Approach to the Enhancement of Health Span and Life Span. Cold Spring Harb. Perspect. Med. 2016, 6, a025163, doi:https://doi.org/10.1101/cshperspect.a025163.
Malcomson, F.C.; Mathers, J.C. Nutrition and Ageing. Subcell. Biochem. 2018, 90, 373–424, doi:https://doi.org/10.1007/978-981-13-2835-0_13.
Shannon, O.M.; Ashor, A.W.; Scialo, F.; Saretzki, G.; Martin-Ruiz, C.; Lara, J.; Matu, J.; Griffiths, A.; Robinson, N.; Lillà, L.; et al. Mediterranean Diet and the Hallmarks of Ageing. Eur. J. Clin. Nutr. 2021, 75, 1176–1192, doi:https://doi.org/10.1038/s41430-020-00841-x.
Chen, X.; Maguire, B.; Brodaty, H.; O’Leary, F. Dietary Patterns and Cognitive Health in Older Adults: A Systematic Review. J. Alzheimers Dis. JAD 2019, 67, 583–619, doi:https://doi.org/10.3233/JAD-180468.
Zhang, J.; Wang, Q.; Hao, W.; Zhu, D. Long-Term Food Variety and Dietary Patterns Are Associated with Frailty among Chinese Older Adults: A Cohort Study Based on CLHLS from 2014 to 2018. Nutrients 2022, 14, doi:https://doi.org/10.3390/nu14204279.
Ren, L.; Tang, Y.; Yang, R.; Hu, Y.; Wang, J.; Li, S.; Yu, M.; Jiang, Y.; Liu, Z.; Wu, Y.; et al. Plant-Based Dietary Pattern and Low Muscle Mass: A Nation-Wide Cohort Analysis of Chinese Older Adults. BMC Geriatr. 2023, 23, 569, doi:https://doi.org/10.1186/s12877-023-04265-7.
Tucker, L.A. Milk Fat Intake and Telomere Length in U.S. Women and Men: The Role of the Milk Fat Fraction. Oxid. Med. Cell. Longev. 2019, 2019, 1574021, doi:https://doi.org/10.1155/2019/1574021.
Talegawkar, S.A.; Jin, Y.; Simonsick, E.M.; Tucker, K.L.; Ferrucci, L.; Tanaka, T. The Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) Diet Is Associated with Physical Function and Grip Strength in Older Men and Women. Am. J. Clin. Nutr. 2022, 115, 625–632, doi:https://doi.org/10.1093/ajcn/nqab310.
Inelmen, E.M.; Toffanello, E.D.; Enzi, G.; Sergi, G.; Coin, A.; Busetto, L.; Manzato, E. Differences in Dietary Patterns between Older and Younger Obese and Overweight Outpatients. J. Nutr. Health Aging 2008, 12, 3–8, doi:https://doi.org/10.1007/BF02982157.
Guyonnet, S.; Rolland, Y.; Takeda, C.; Ousset, P.-J.; Ader, I.; Davezac, N.; Dray, C.; Fazilleau, N.; Gourdy, P.; Liblau, R.; et al. The INSPIRE Bio-Resource Research Platform for Healthy Aging and Geroscience: Focus on the Human Translational Research Cohort (The INSPIRE-T Cohort). J. Frailty Aging 2021, 10, 110–120, doi:https://doi.org/10.14283/jfa.2020.38.
Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A Short Physical Performance Battery Assessing Lower Extremity Function: Association with Self-Reported Disability and Prediction of Mortality and Nursing Home Admission. J. Gerontol. 1994, 49, M85–94, doi:https://doi.org/10.1093/geronj/49.2.m85.
Fess E.E.; Moran C.A. Clinical Assessment Recommendations; American Society of Hand Therapists, 1981
Estaquio, C.; Kesse-Guyot, E.; Deschamps, V.; Bertrais, S.; Dauchet, L.; Galan, P.; Hercberg, S.; Castetbon, K. Adherence to the French Programme National Nutrition Santé Guideline Score Is Associated with Better Nutrient Intake and Nutritional Status. J. Am. Diet. Assoc. 2009, 109, 1031–1041, doi:https://doi.org/10.1016/j.jada.2009.03.012.
Kim, J.; Jo, I. Grains, Vegetables, and Fish Dietary Pattern Is Inversely Associated with the Risk of Metabolic Syndrome in South Korean Adults. J. Am. Diet. Assoc. 2011, 111, 1141–1149, doi:https://doi.org/10.1016/j.jada.2011.05.001.
Cattell, R.B. The Scree Test For The Number Of Factors. Multivar. Behav. Res. 1966, 1, 245–276, doi:https://doi.org/10.1207/s15327906mbr0102_10.
Hutcheson, G.D. The Multivariate Social Scientist; SAGE Publications, Ltd: London, 1999
Santos, R. de O.; Gorgulho, B.M.; Castro, M.A. de; Fisberg, R.M.; Marchioni, D.M.; Baltar, V.T. Principal Component Analysis and Factor Analysis: Differences and Similarities in Nutritional Epidemiology Application. Rev. Bras. Epidemiol. 2019, 22, e190041, doi:https://doi.org/10.1590/1980-549720190041.
Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395, doi:https://doi.org/10.1249/01.MSS.0000078924.61453.FB.
Tukey, J.W. Exploratory Data Analysis; Addison-Wesley, 1977
McDonald JH. Multiple Comparisons. In Handbook of Biological Statistics; Sparky House Publishing: Baltimore, Maryland, 2014; pp. 254–260.
Cohen, J. Statistical Power Analysis for the Behavioral Sciences; 2nd ed.; L. Erlbaum Associates: Hillsdale, N.J., 1988; ISBN 978-0-8058-0283-2.
Stein, C.M.; Morris, N.J.; Hall, N.B.; Nock, N.L. Structural Equation Modeling. Methods Mol. Biol. Clifton NJ 2017, 1666, 557–580, doi:https://doi.org/10.1007/978-1-4939-7274-6_28.
Munt, A.E.; Partridge, S.R.; Allman-Farinelli, M. The Barriers and Enablers of Healthy Eating among Young Adults: A Missing Piece of the Obesity Puzzle: A Scoping Review. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2017, 18, 1–17, doi:https://doi.org/10.1111/obr.12472.
Monteiro, C.A.; Cannon, G.; Moubarac, J.-C.; Levy, R.B.; Louzada, M.L.C.; Jaime, P.C. The UN Decade of Nutrition, the NOVA Food Classification and the Trouble with Ultra-Processing. Public Health Nutr. 2018, 21, 5–17, doi:https://doi.org/10.1017/S1368980017000234.
Pagliai, G.; Dinu, M.; Madarena, M.P.; Bonaccio, M.; Iacoviello, L.; Sofi, F. Consumption of Ultra-Processed Foods and Health Status: A Systematic Review and Meta-Analysis. Br. J. Nutr. 2021, 125, 308–318, doi:https://doi.org/10.1017/S0007114520002688.
Hall, K.D.; Ayuketah, A.; Brychta, R.; Cai, H.; Cassimatis, T.; Chen, K.Y.; Chung, S.T.; Costa, E.; Courville, A.; Darcey, V.; et al. Ultra-Processed Diets Cause Excess Calorie Intake and Weight Gain: An Inpatient Randomized Controlled Trial of Ad Libitum Food Intake. Cell Metab. 2019, 30, 67–77.e3, doi:https://doi.org/10.1016/j.cmet.2019.05.008.
Cederholm, T.; Jensen, G.L.; Correia, M.I.T.D.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.; et al. GLIM Criteria for the Diagnosis of Malnutrition - A Consensus Report from the Global Clinical Nutrition Community. Clin. Nutr. Edinb. Scotl. 2019, 38, 1–9, doi:https://doi.org/10.1016/j.clnu.2018.08.002.
Sandoval-Insausti, H.; Blanco-Rojo, R.; Graciani, A.; López-García, E.; Moreno-Franco, B.; Laclaustra, M.; Donat-Vargas, C.; Ordovás, J.M.; Rodríguez-Artalejo, F.; Guallar-Castillón, P. Ultra-Processed Food Consumption and Incident Frailty: A Prospective Cohort Study of Older Adults. J. Gerontol. A. Biol. Sci. Med. Sci. 2020, 75, 1126–1133, doi:https://doi.org/10.1093/gerona/glz140.
Zhang, S.; Gu, Y.; Rayamajhi, S.; Thapa, A.; Meng, G.; Zhang, Q.; Liu, L.; Wu, H.; Zhang, T.; Wang, X.; et al. Ultra-Processed Food Intake Is Associated with Grip Strength Decline in Middle-Aged and Older Adults: A Prospective Analysis of the TCLSIH Study. Eur. J. Nutr. 2022, 61, 1331–1341, doi:https://doi.org/10.1007/s00394-021-02737-3.
Santos, S.; Oliveira, A.; Lopes, C. Systematic Review of Saturated Fatty Acids on Inflammation and Circulating Levels of Adipokines. Nutr. Res. N. Y. N 2013, 33, 687–695, doi:https://doi.org/10.1016/j.nutres.2013.07.002.
Li, C.-W.; Yu, K.; Shyh-Chang, N.; Jiang, Z.; Liu, T.; Ma, S.; Luo, L.; Guang, L.; Liang, K.; Ma, W.; et al. Pathogenesis of Sarcopenia and the Relationship with Fat Mass: Descriptive Review. J. Cachexia Sarcopenia Muscle 2022, 13, 781–794, doi:https://doi.org/10.1002/jcsm.12901.
Batsis, J.A.; Villareal, D.T. Sarcopenic Obesity in Older Adults: Aetiology, Epidemiology and Treatment Strategies. Nat. Rev. Endocrinol. 2018, 14, 513–537, doi:https://doi.org/10.1038/s41574-018-0062-9.
Hägg, S.; Jylhävä, J. Sex Differences in Biological Aging with a Focus on Human Studies. eLife 2021, 10, doi:https://doi.org/10.7554/eLife.63425.
Gedmantaite, A.; Celis-Morales, C.A.; Ho, F.; Pell, J.P.; Ratkevicius, A.; Gray, S.R. Associations between Diet and Handgrip Strength: A Cross-Sectional Study from UK Biobank. Mech. Ageing Dev. 2020, 189, 111269, doi:https://doi.org/10.1016/j.mad.2020.111269.
Struijk, E.A.; Banegas, J.R.; Rodríguez-Artalejo, F.; Lopez-Garcia, E. Consumption of Meat in Relation to Physical Functioning in the Seniors-ENRICA Cohort. BMC Med. 2018, 16, 50, doi:https://doi.org/10.1186/s12916-018-1036-4.
Struijk, E.A.; Fung, T.T.; Sotos-Prieto, M.; Rodriguez-Artalejo, F.; Willett, W.C.; Hu, F.B.; Lopez-Garcia, E. Red Meat Consumption and Risk of Frailty in Older Women. J. Cachexia Sarcopenia Muscle 2022, 13, 210–219, doi:https://doi.org/10.1002/jcsm.12852.
Aoyama, S.; Kim, H.-K.; Hirooka, R.; Tanaka, M.; Shimoda, T.; Chijiki, H.; Kojima, S.; Sasaki, K.; Takahashi, K.; Makino, S.; et al. Distribution of Dietary Protein Intake in Daily Meals Influences Skeletal Muscle Hypertrophy via the Muscle Clock. Cell Rep. 2021, 36, 109336, doi:https://doi.org/10.1016/j.celrep.2021.109336.
Krok-Schoen, J.L.; Jonnalagadda, S.S.; Luo, M.; Kelly, O.J.; Taylor, C.A. Nutrient Intakes from Meals and Snacks Differ with Age in Middle-Aged and Older Americans. Nutrients 2019, 11, doi:https://doi.org/10.3390/nu11061301.
Funding
Funding: The present work was performed in the context of the INSPIRE Program, a research platform supported by grants from the Region Occitanie/Pyrénées-Méditerranée (Reference number: 1901175) and the European Regional Development Fund (ERDF) (Project number: MP0022856).
Author information
Authors and Affiliations
Contributions
Authors’ contributions: LL, NAGF, and PSB designed research. LL and NAGF conducted research. LL analyzed data. LL and NAGF wrote the paper. YR, SG, and PSB, critically revised the paper. LL and NAGF had primary responsibility for final content. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate: All the participants gave their written consent, and the study protocol was approved by the French Ethical Committee in Rennes (CPP Ouest V). The study protocol is available at “clinicaltrials.gov” under the registration code NCT04224038.
Competing interests: The authors declare that they have no competing interests.
Electronic Supplementary Material
Rights and permissions
About this article

Cite this article
Lengelé, L., Grande de França, N.A., Rolland, Y. et al. Body Composition, Physical Function, and Dietary Patterns in People from 20 to Over 80 Years Old. J Nutr Health Aging 27, 1047–1055 (2023). https://doi.org/10.1007/s12603-023-2025-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12603-023-2025-7