
Abstract
Objectives
To validate the short-form of the MNA (MNA-SF) and the cut-off point of 31 cm for calf circumference (CC) in older people in Latin America.
Methods
A cross-sectional study was conducted with 5,722 community-dwelling older subjects (range: 60-102 years) in Latin America’s five main cities: Sao Paulo (Brazil), Santiago (Chile), Havana (Cuba), Mexico DF (Mexico) and Montevideo (Uruguay). All participants underwent an interview, which included anthropometric measurements, completing the MNA and obtaining socio-demographic, nutrition and health information. The short-form of the MNA consists of only six questions from the original 18. It has two versions: one using body mass index (BMI) and the second using CC as a surrogate. Cohen’s Kappa was calculated to assess the agreement between the MNA and the MNA-SF; diagnostic tests were performed, and Receiver-operating characteristic (ROC) curves were developed. Criterion-related validity was assessed in the Chilean sample.
Results
Both version of the MNA-SF showed high sensitivity and specificity with the MNA, showing good accuracy (0.88), although higher values were estimated for malnutrition and risk of malnutrition in the total sample by sex. The cut-off point of 31 cm for CC showed high sensitivity (74.6-94.4%), specificity (72.6-100%) and good area under the ROC curve (0.87-0.95) when compared with BMI. There was good agreement between MNA and both version of MNA-SF for identifying persons with malnutrition or a risk of malnutrition in the five cities (Kappa coefficient: 0.6193-0.7852).
Conclusion
Both versions of the MNA-SF are population-screening tools of easy and fast application, with good accuracy for assessing malnutrition and risk of malnutrition in Latin American older people.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The Latin American population is aging rapidly, which implies that the prevalence and incidence of chronic diseases, disability and dependence is also increasing (1–3). The assessment of nutritional status is essential for the health of older adults, both individually and collectively. Among the indicators of nutritional status, the easiest data to obtain are anthropometric measurements, hence, the widespread use of body mass index (BMI) (3–5) and waist circumference: the latter as an indicator of metabolic risk (6). Among the instruments to measure the risk of malnutrition in older adults is the Mini Nutritional Assessment (MNA), which is widely used in older populations worldwide. This instrument was developed in the 1990s by Guigoz, Vellas and Garry (7) to assess nutritional status and rapidly diagnose malnutrition in fragile older adults (8–11). The MNA is a tool to estimate the nutritional risk of malnutrition in older people, which is essential in a context such as Latin America where older people comprise a group with high socio-economic vulnerability (3, 12, 13). It has been validated and used as a screening tool for malnutrition in countries in North America (8, 11, 14), Europe (15–17), Asia (18), Africa (19) and Latin America. In Latin America, the instrument has been used in Brazil (20), Chile (21), Cuba (22) and Mexico (23).
In 2001, the same group that authored the original instrument (7, 8, 14) developed and validated an abbreviated version of the MNA (MNA-SF) (24, 25) consisting of six questions. The MNA-SF has two variants, depending on the anthropometric measure, that incorporate BMI (MNA-SF1) or calf circumference (CC) (MNA-SF2). CC is a simple, easy and inexpensive anthropometric measure to determine, is useful when BMI is not available or cannot be determined, and does not require any effort from the older adult. Considering the usefulness of this measurement for population studies, elderly or bedridden people, or anyone with functional limitations, the fundamental objective of this study is to validate the two variants of the short-form of the MNA in people aged 60 years or more in five cities in Latin America (12) using the MNA as the gold standard.
Methods
Study population
A cross-sectional study using secondary data from the Health, Wellbeing and Aging study (SABE in Spanish) was carried out in seven cities in Latin America and the Caribbean: Bridgetown, Buenos Aires, Havana, Mexico City, Montevideo, Santiago and Sao Paulo from 1999–2001. SABE is a probabilistic, household survey, with stratified multistage sampling. The study design has been previously described (26). The study evaluated various aspects of health and well-being in the population of people aged 60 years or more in the selected cities. The information was collected simultaneously in all cities using standardised procedures, with a common protocol allowing comparative analyses. All subjects were interviewed face to face in their homes, socio-demographic information was obtained, the MNA and Mini-Mental State Examination (MMSE), were completed, and information on chronic diseases, disability and functional limitations, among others, was self-reported.
The sample consisted of 5526 adults aged 60 years or more (age range: 61–99 years) residing in the community in five Latin American cities: Sao Paulo (Brazil), Havana (Cuba), Santiago de Chile (Chile), Mexico City (Mexico) and Montevideo (Uruguay). The original sample consisted of 8,046 subjects, of whom, 2,520 were eliminated from the study because of inconsistent or missing data on the MNA or anthropometric measurements. The sample was distributed as follows:
-
1,449 subjects Sao Paulo, Brazil (loss: 29%)
-
1,220 subjects Havana, Cuba (loss: 33.9%)
-
1,160 subjects Santiago de Chile, Chile (loss: 9.6%)
-
817subjects Mexico DF, Mexico (loss: 32.6%)
-
880 subjects Montevideo, Uruguay (loss: 36.1%)
Anthropometric measurements
Anthropometric measurements were carried out by paramedical personnel specially trained for this study. The anthropometric variables considered were height, weight, CC and waist circumference. Weight and height were used to calculate BMI (BMI = total weight in kg/height2 in meters). Height was measured with a portable Harpenden stadiometer (Holtain Ltd., Croswell, UK), with the subject standing barefoot with heels together, arms at their sides, legs straight, shoulders relaxed and head aligned in the Frankfort horizontal plane with heels, buttocks, shoulder blades and the back of the head supported against a straight vertical wall or door. Measurements were recorded in cm. Weight was measured using a SECA platform scale graduated to 0.1 kg with the subject barefoot and standing on the platform.
The waist and CC were measured with a flexible steel tape to the nearest 0.1 cm. The waist circumference was measured with the subject standing, immediately above the iliac crest in a circle parallel to the floor. CC was measured at the centre of the fullest part of the calf.
MNA and MNA-SF
The MNA is a screening instrument consisting of 18 items incorporating anthropometric measurements (BMI, midarm circumference and CC), questions regarding weight loss, dietary intake and dietary parameters (daily servings of milk, poultry or fish, legumes or eggs, fruit or vegetables and liquids), global components (living independently, taking more than three medications, having an acute illness, mobility issues, neuropsychological problems, skin ulcers) and self-assessment (if they believe they are well nourished, what they think their health status is relative to others their age, etc.). The maximum score for the MNA is 30 points; the subjects were classified as normal or well nourished (≥24 points), at risk for malnutrition (17–23.5 points) and experiencing malnutrition (<17 points).
The MNA-SF, developed by Rubenstein (24, 25), is a short questionnaire consisting of six items, which correspond to questions on decreased food consumption, weight loss, mobility, presence of acute disease, neuropsychological problems and anthropometry, with two variants. One variant uses BMI, and the other replaces BMI with CC. The scores of the items are the same except for the questions following: have you suffered from acute stress or an acute disease in the past few months, and CC. In the first, instead of 1, a score of 2 is given, and the second, instead of 1, a score of 3 is given for CC ≥31 cm. In both, we assigned the same score to CC <31 cm and BMI <19 kg/m2, and the same score to CC ≥31 cm or BMI >23 kg/m2.
The maximum score of the MNA-SF in any of its variants is 14 points. The subjects were classified as normal or well-nourished if the score was ≥12 points, at nutritional risk if the score was 8–11 points, and malnourished if ≤7 points.
Ethical approval for the conduction of the survey was obtained from the Pan American Health Organization Ethical Review Committee and the institutional review board in each city.
Statistical analysis
A descriptive analysis of the variables of interest was performed. Results are expressed as mean ± standard deviation, 95% confidence intervals (95% CI) and relative frequencies expressed as percentages (%). For comparisons of socio-demographic and anthropometric variables by country and sex, a t-test, an analysis of variance (ANOVA) parametric or non-parametric and Pearson-Chi2 were used. Receiver-operating characteristic (ROC) curves were performed to validate the cut-off point of the CC, using a BMI less than 19 kg/m2 as the gold standard. Cohen’s Kappa coefficient was calculated to assess the agreement between the MNA and the MNA-SF for both variants. Logistic regressions were also performed to analyse the association between studied variables and the presence or absence of malnutrition or risk of malnutrition obtained by the MNA and the two variants of the MNA-SF.
The criterion-related and predictive validation of the MNA-SF was performed in the Chilean sample to compare appendicular skeletal muscle mass (ASM), handgrip strength and physical performance in well-nourished and malnourished subjects according to the MNA and MNA-SF. ASM was estimated using the mean of a prediction equation obtained and validated in Chile (27). The other cities’ samples did not have measures of handgrip strength. Physical performance was measured using the time for five chair stands and one leg stand for ten seconds (best time of any leg).
All statistical analyzes were performed using STATA software version STATA 14.0 (StataCorp. 2013. Stata Statistical Software: Release 13. College Station, TX: StataCorp LP).

Socio-demographic and health characteristics of the studied samples by country
Results
Descriptive statistics of the sample, by country, are presented in Table 1. Women predominate in all the samples, ranging from 60.7% in Brazil to 66.6% in Uruguay. Mexico had the lowest mean age (69.7±7.6 years) and Brazil had the highest average age (73.3 ± 8.4 years, 95% CI: 72.8-73.7 years). The average ages in Chile, Cuba and Uruguay were similar (p>0.1). Regarding the self-perception of good nutrition, the country that reported the highest percentage was Uruguay, while Cuba presented the lowest (93.9% vs. 74.1%). There were also significant differences in educational levels; Cuba had the highest educational level, followed by Uruguay, Chile, Mexico and Brazil (average education years: 7.1, 6.5, 5.7, 4.6, 3.3 years; respectively; p<0.0001). Uruguay had a high percentage of older people living alone (19.4%), and Mexico had the lowest percentage (10.1%). With regard to smoking, a high percentage of older people smoked in Cuba (27.5%), representing almost twice as many older adults who smoked in Mexico (16.2%), and more than double the rest of the cities, with Uruguay being the country with the lowest proportion of smokers (11.3%) (p<0.0001).

Nutritional and anthropometric characteristics of the studied samples by sex and city

Area under the ROC curve, sensitivity, specificity and % of subjects correctly clasificated according BMI using the calf circumference (CC) cut-off point of 31 cm

Logistic regressions for malnutrition and risk of malnutrition assessed by MNA and by the short version of MNA (MNA-SF1 y MNA-SF2)
Cuba presented a high percentage of older people with three or more chronic diseases, followed by Brazil, Uruguay, Chile and Mexico (18.1%, 13.4%, 12.4%, 9.7% and 9%; respectively).

ROC Curve for the total sample

Prevalence of malnutrition and risk of malnutrition by gender and city, using MNA (design-based)
The median scores on the MMSE of Chile, Cuba and Brazil were similar (18): Uruguay had the highest score (28) and Mexico had the lowest score (20) (Kruskal-Wallis Test: p<0.0001).
Table 2 shows the anthropometric characteristics of the sample by city and gender. In all cities, the average BMI was higher in women than in men (t -test; p<0.0001), as was obesity and abdominal obesity (Pearson Chi2 test; p<0.0001). A high percentage of overweight and obese people of both sexes was observed in all the cities with the exception of Cuba, which had 6.5% obese men and 25.7% overweight men. Chile had the highest percentage of obese men (22.7%), and Mexico had the highest percentage of overweight men (48.1%). With respect to women, 16.8% were obese in Cuba, followed by Brazil, Chile, Mexico and Uruguay (28%, 33.8%, 36.9% and 43.6%, respectively). Uruguay was the country with the highest BMI average, followed by Chile, Mexico, Brazil and Cuba (28.8, 28.0, 27.9, 26.9, 24.5 kg/m2, respectively). CC for men and women was similar in Brazil, Cuba and Uruguay, unlike Chile and Mexico, where it was higher in men than in women (t test, p<0.0001). The average waist circumference in the Cuban sample was significantly lower than in the rest of the countries (Bonferroni test, p<0.0001), and the average CC of Uruguay was higher than in Cuba or Mexico, where it was significantly lower than the rest for men and women (Bonferroni test, p<0.0001).

Handgrip strength, appendicular skeletal muscle mass and physical function in Chilean older people with Malnutrition or risk of malnutrition diagnosed with MNA, MNA-SF1 and MNA -SF2 in the Chilean sample
Table 3 shows the values of the area under the ROC curve for a BMI <19 kg/m2 and CC. The validation of the cut-off point of 31 cm for CC with a BMI in all cities had a high sensitivity (74.6–94.4%) and specificity (72.6–100%), and very good precision (0.87–0.95), being significant in all cases. The percent of older subjects correctly classified varied between 75.0% and 93.3%, and Uruguay had the lowest percentage.
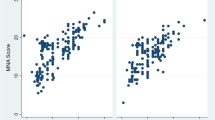
Figure 1 shows the ROC curve obtained for the total sample. The sensitivity (88.1%), specificity (70.5%) and accuracy (area under ROC curve = 0.88) were high for the cut-off point of 31 cm, with 87.1% of subjects well classified.
There was good agreement between MNA, MNA-SF1 and MNA-SF2 for identifying persons with malnutrition or a risk of malnutrition in the five cities (Kappa coefficient: Brazil = 0.7852; Chile = 0.6626; Cuba = 0.7222; Mexico = 0.6611; Uruguay = 0.6193) (29).
Figure 2 shows the design-based prevalence of malnutrition and risk of malnutrition by city and gender, with Chile having the lowest prevalence of malnutrition and Cuba having the highest prevalence (1.1% and 12.4%, respectively). The prevalence of malnutrition was higher in women than in men according to the MNA (Pearson Chi2, p<0.0001).
Table 4 shows the results of the logistic regression models for malnutrition and risk of malnutrition, applying the MNA and the two short-forms (MNA-SF1 and MNA-SF2). No association was found between malnutrition and living alone in any of the three models, so it was removed from the analysis. The adjustment in the three models was good (Hosmer-Lemeshow test, p>0.12). The variables that were associated with the presence of malnutrition or risk of malnutrition as risk factors were currently or previously smoking (p<0.06), having fewer than eight years of schooling (p<0.0001), having two or more chronic diseases (p<0.01), low MMSE scores (<13 points) and being 70 years-of-age or more (p<0.0001), adjusted for sex. It was observed that the odds ratios were similar in the three models.
Table 5 shows that normal or well-nourished Chilean older adults had higher handgrip strength, ASM and physical function than adults suffering from malnutrition or those at risk of being malnourished when considering the MNA, MNA-SF1 and MNA-SF2 scores.
Discussion
In this study, we showed that the two short-forms of the MNA (MNA-SF1 and MNASF2) are valid. They presented high sensitivity and specificity, and good accuracy (0.88) with the MNA in the total sample and by city, proving to be good tools for screening for malnutrition or risk of malnutrition in Latin American older adults. We demonstrated the validity of the cut-off of 31 cm for CC (MNA-SF2) in relation to BMI <19 kg/m2 (MNA-SF1) in five cities in Latin America. This cut-off had a high sensitivity (74.4–94.5%) and specificity (72.9–100%) and good accuracy, given by the high area under the ROC curve values obtained (0.86 to 0.95) using BMI <19 kg/m2 as the gold standard. We also obtained a good agreement between MNA and the two versions of the MNA-SF for identifying persons with malnutrition or those at risk of malnutrition in the five cities (Kappa coefficient: 0.6193-0.7852).
The MNA has been validated and used extensively and successfully to screen for malnutrition; however, to our knowledge, the short versions have not been validated in Latin America. In a study conducted in Japan by Kuzuya et al (18), the MNA and the MNA-SF were validated in a sample of 226 Japanese aged 60 years or more, with the authors finding a high percentage of malnutrition (19.9%). In Taiwan, Tsai et al (30) used a modified version of the MNA with specific cut-off points for arm and waist circumference in adults aged 60 years or more living in the community, eliminating the need for BMI (31).
In our study, the MNA-SF1 better assessed the risk of malnutrition than the MNA-SF2, which was similar to results obtained in a study conducted in Poland (32). However, when BMI is not available, the MNA-SF2 is accurate enough to screen for malnutrition or risk of malnutrition.
In a study in Spain, the two short versions of the MNA were used in nursing home residents. The authors found that both versions were capable of screening for malnutrition or risk of malnutrition, and recommended using the MNA-SF2 if BMI was not available (33).
Our results show lower rates of malnutrition in both men (1.5 to 5.1%) and women (1.3 to 8.7%) in all the cities studied; Chile had the lowest rate of malnutrition and Cuba had the highest. This result coincides with the findings of Morillas et al (34) in Spain, where the prevalence of malnutrition ranged between 3% and 5% among older people living in the community. The prevalence of the risk of malnutrition was high, reaching about a third (29.9 to 38.6%) of the studied population, with the exception of Santiago de Chile, where only 14% of the sample was at risk. With the SABE survey data, in Mexico, Franco-Álvarez et al (23) studied some determinants of malnutrition and found that there were multiple factors that influenced malnutrition in the elderly, including depression, socio-economic conditions, social support and nutrition (23).
Gonzalez et al (22) estimated rates of malnutrition with the MNA in older Cuban adults in three different scenarios and found that the instrument was useful for detecting nutritional problems (22).
It is known that malnutrition is a risk factor in the elderly, which has been widely discussed as a cause of mortality. It has also been shown that the MNA is a useful tool to detect malnutrition in hospitals (35–37). Woo et al (37) developed and validated a tool based on the MNA for nutritional purposes for elderly Chinese institutionalised individuals, which can be used to identify those with a normal nutritional status; however, in other cases, nutritional status should be evaluated in more detail (37).
In a study in Mexico, 69% of patients upon hospital admission were at risk of malnutrition or under-nutrition according to the MNA and, according to the MNA-SF, 73% of patients were at risk of being malnourished, showing moderate agreement between the two versions of the instrument (Kappa coefficient = 0.43) (35).
A good criterion-related validity of the MNA, MNA-SF1 and MNA-SF2 was demonstrated in the Chilean sample showing that normal or well-nourished Chilean older adults had higher muscle mass and function than subjects with malnutrition or risk of malnutrition as diagnosed with the MNA and MNA-SF.
The main limitation of the study was its cross-sectional design; however, this design is widely used for diagnostic and longitudinal research. Both the MNA-SF1 and MNA-SF2 estimate slightly higher values of malnutrition and a lower risk of malnutrition than the MNA, although both versions showed high sensitivity and specificity with respect to the MNA.
Among the strengths of the study is its large probabilistic sample that includes five Latin American cities, all of which followed the same protocol. This validates the use of the measures in population studies in Latin America, allowing the tool to be used to screen for nutritional risk, as it is valid, safe, simple to apply and low in cost to administer. It is known that the population aged 60 years or more is growing along with the prevalence of malnutrition, hence, the need for a user-friendly application that can be used to screen for malnutrition and risk of malnutrition.
In conclusion, the MNA-SF1 and MNA-SF2, using CC or BMI, are reliable screening tools for assessing the state of nutrition in the elderly population; they are easy to use, inexpensive and fast to administer, and are accurate when assessing malnutrition and risk of malnutrition in Latin American older people.
Acknowledgments: This study was funded by Fondecyt grant 1080589.
Ethical standards: The authors declare that the study procedures comply with the current laws of the five countries for investigation involving humans participants.
References
Albala C, Vio F. Epidemiological transition in Latin America: the case of Chile. Public Health [Internet]. 1995 Nov [cited 2015 Jan 26];109(6):431–42. Available from: http://www.ncbi.nlm.nih.gov/pubmed/8570804
Albala C, Vio F, Kain J, Uauy R. Nutrition transition in Chile: determinants and consequences. Public Health Nutr [Internet]. 2002 Feb [cited 2015 Jan 15];5(1A):123–8. Available from: http://www.ncbi.nlm.nih.gov/pubmed/12027274
Albala C, Sánchez H, Lera L, Angel B, Cea X. [Socioeconomic inequalities in active life expectancy and disability related to obesity among older people]. Rev Med Chil [Internet]. 2011 Oct;139(10):1276–85. Available from: http://www.ncbi.nlm.nih.gov/pubmed/22286726
Shetty PS, James WP. Body mass index. A measure of chronic energy deficiency in adults. FAO Food Nutr Pap [Internet]. 1994 Jan [cited 2014 Dec 22];56:1–57. Available from: http://www.ncbi.nlm.nih.gov/pubmed/7925867
WHO. Obesity. Preventing and managing the global epidemic. Report of a WHO consultation on obesity. Geneva, 3-5 June. 1997.
Lemieux S, Prud’homme D, Bouchard C, Tremblay A, Després JP. A single threshold value of waist girth identifies normal-weight and overweight subjects with excess visceral adipose tissue. Am J Clin Nutr [Internet]. 1996 Nov [cited 2014 Dec 22];64(5):685–93. Available from: http://www.ncbi.nlm.nih.gov/pubmed/8901786
Guigoz Y, Vellas J, Garry P. Mini Nutritional Assessment: A practical assessment tool for grading the nutritional state of elderly patients. Facts Res Gerontol. 1994;4(Suppl. 2):15–59.
Guigoz Y, Vellas B, Garry PJ. Assessing the nutritional status of the elderly: The Mini Nutritional Assessment as part of the geriatric evaluation. Nutr Rev [Internet]. 1996 Jan [cited 2014 Dec 15];54(1 Pt 2):S59–65. Available from: http://www.ncbi.nlm.nih.gov/pubmed/8919685
Vellas B, Garry PJ GY. Mini Nutritional Assessment (MNA): Research and practice in the elderly. 1999
Vellas B, Guigoz Y, Garry PJ, Nourhashemi F, Bennahum D, Lauque S, et al. The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients. Nutrition [Internet]. 1999 Feb [cited 2015 Apr 16];15(2):116–22. Available from: http://www.ncbi.nlm.nih.gov/pubmed/9990575
Toulouse BV, Nuremberg CS. The MNA ® revisited: what does the data tell us ? Chairmen: XIXth IAGG World Congress of Gerontology and Geriatrics. Journals Gerontol Ser A Biol Sci Med Sci. 2009;(July).
Albala C, Lebrão ML, León Díaz EM, Ham-Chande R, Hennis AJ, Palloni A, Peláez M PO. The Health, Well-Being, and Aging (“SABE”) survey: methodology applied and profile of the study population. Rev Panam Salud Pública. 2005;17(5-6):307–22.
Palloni A, Pinto-Aguirre G, Pelaez M. Demographic and health conditions of ageing in Latin America and the Caribbean. Int J Epidemiol [Internet]. 2002 Aug [cited 2015 Jan 7];31(4):762–71. Available from: http://www.ncbi.nlm.nih.gov/ pubmed/12177016
Vellas B, Garr P, Guigoz Y, editors. Mini Nutritional Assessment (MNA): Research and Practice in the Elderly. Vevey, Switzerland: Nestlé Nutrition Workshop Series Clinical & Performance Programme No. 1;1998.
Gerber V, Krieg MA, Cornuz J, Guigoz Y, Burckhardt P. Nutritional status using the Mini Nutritional Assessment questionnaire and its relationship with bone quality in a population of institutionalized elderly women. J Nutr Health Aging [Internet]. 2003 Jan [cited 2015 Jan 7];7(3):140–5. Available from: http://www.ncbi.nlm.nih.gov/pubmed/12766790
Söderhamn U, Söderhamn O. Reliability and validity of the nutritional form for the elderly (NUFFE). J Adv Nurs [Internet]. 2002 Jan [cited 2015 Jan 7];37(1):28–34. Available from: http://www.ncbi.nlm.nih.gov/pubmed/11784395
Guigoz Y. The Mini Nutritional Assessment (MNA) review of the literature—What does it tell us? J Nutr Health Aging [Internet]. 2006 [cited 2015 Jan 5];10(6):466–85; discussion 485–7. Available from: http://www.ncbi.nlm.nih.gov/pubmed/17183419
Kuzuya M, Kanda S, Koike T, Suzuki Y, Satake S, Iguchi A. Evaluation of Mini-Nutritional Assessment for Japanese frail elderly. Nutrition [Internet]. 2005 Apr [cited 2015 Jan 7];21(4):498–503. Available from: http://www.ncbi.nlm.nih.gov/ pubmed/15811771
Tsai AC, Shih C-L. A population-specific Mini-Nutritional Assessment can effectively grade the nutritional status of stroke rehabilitation patients in Taiwan. J Clin Nurs [Internet]. 2009 Jan [cited 2011 Sep 13];18(1):82–8. Available from: http:// www.ncbi.nlm.nih.gov/pubmed/18665877
Delacorte RR, Moriguti JC, Matos FD, Pfrimer K, Marchinil JS, Ferriolli E. Mininutritional assessment score and the risk for undernutrition in free-living older persons. J Nutr Health Aging [Internet]. 2004 Jan [cited 2015 Jan 7];8(6):531–4. Available from: http://www.ncbi.nlm.nih.gov/pubmed/15543428
Albala C, Bunout D, Carrasco F. Evaluación del estado nutricional en el anciano. In: Castillo C, Uauy R, Atalah E, editors. Guías Alimentarias para el Adulto Mayor Bases para la acción. 1a ed. Santiago; 1999. p. 39–52.
González Hernández A, Cuyá Lantigua M, González Escudero H, Sánchez Gutiérrez R, Cortina Martínez R, Barreto Penié J, et al. [Nutritional status of Cuban elders in three different geriatric scenarios: community, geriatrics service, nursery home]. Arch Latinoam Nutr [Internet]. 2007 Sep [cited 2015 Jan 7];57(3):266–72. Available from: http://www.ncbi.nlm.nih.gov/pubmed/18271405
Franco-Alvarez N, Avila-Funes JA, Ruiz-Arreguí L, Gutiérrez-Robledo LM. [Determinants of malnutrition risk among the older adult community: a secondary analysis of the Health, Wellbeing, and Aging Study (SABE) in Mexico]. Rev Panam Salud Publica [Internet]. 2007 Dec [cited 2015 Jan 7];22(6):369–75. Available from: http://www.ncbi.nlm.nih.gov/pubmed/18291055
Kaiser M, Bauer J, Rämasch C, Al. E. The short-form Mini Nutritional Assessment® (MNA-SF): Can it be improved to facilitate clinical use? J Nutr Heal Aging. 2009;13(suppl 2):S16.
Rubenstein L, Harker J, Salva U, Guigoz Y, Vellas B. Evaluación de la desnutrición en la práctica geriátrica: Desarrollo de la Short Form-Mini Nutritional Assessment (MNA-SF). J Geront. 2001;56A:M366–377.
Albala C, Lebrão ML, León Díaz EM, Ham-Chande R, Hennis AJ, Palloni A, et al. [The Health, Well-Being, and Aging (“SABE”) survey: methodology applied and profile of the study population]. Rev Panam Salud Publica [Internet]. 2005 Jun [cited 2014 Sep 3];17(5-6):307–22. Available from: http://www.scielosp.org/pdf/rpsp/ v17n5-6/26268.pdf
Lera L, Albala C, Ángel B, Sánchez H, Picrin Y, Hormazabal MJ, et al. [Anthropometric model for the prediction of appendicular skeletal muscle mass in Chilean older adults]. Nutr Hosp [Internet]. 2014 Mar [cited 2014 Aug 6];29(3):611–7. Available from: http://www.ncbi.nlm.nih.gov/pubmed/24559006
Urteaga R C, Ramos H RI, Atalah S E. Validación del criterio de evaluación nutricional global del adulto mayor. Rev Med Chil [Internet]. 2001 Aug [cited 2015 Jan 7];129(8). Available from: http://www.scielo.cl/scielo.php?script=sci_arttext&pid=S0034-98872001000800005&lng=en&nrm=iso&tlng=en
Altman D. Practical statistics for medical research. London: Chapman and Hall; 1991.
Tsai AC, Chang T-L, Yang T-W, Chang-Lee SN, Tsay S-F. A modified mini nutritional assessment without BMI predicts nutritional status of communityliving elderly in Taiwan. J Nutr Health Aging [Internet]. 2010 Mar [cited 2015 Jan 7];14(3):183–9. Available from: http://www.ncbi.nlm.nih.gov/pubmed/20191250
Tsai A, Chang T-L, Yang T-W, Chang-Lee SN, Tsay S-F. A modified mini nutritional assessment without BMI predicts nutritional status of community-living elderly in Taiwan. J Nutr Health Aging [Internet]. 2010 Mar [cited 2015 May 25];14(3):183–9. Available from: http://www.ncbi.nlm.nih.gov/pubmed/20191250
Kostka J, Borowiak E, Kostka T. Validation of the modified mini nutritional assessment short-forms in different populations of older people in Poland. J Nutr Health Aging [Internet]. 2014 Apr [cited 2015 Jan 8];18(4):366–71. Available from: http://www.ncbi.nlm.nih.gov/pubmed/24676316
Garcia-Meseguer MJ, Serrano-Urrea R. Validation of the revised mini nutritional assessment short-forms in nursing homes in Spain. J Nutr Health Aging [Internet]. 2013 Jan [cited 2015 Jan 8];17(1):26–9. Available from: http://www.ncbi.nlm.nih. gov/pubmed/23299374
Morillas J, García-Talavera N, Martín-Pozuelo G, Reina AB, Zafrilla P. [Detection of hyponutrition risk in non-institutionalised elderly]. Nutr Hosp [Internet]. 2006 [cited 2015 Jan 7];21(6):650–6. Available from: http://www.ncbi.nlm.nih.gov/pubmed/17147061
Reyes JGG, Zúñiga AS, Cruz MG. [Prevalence of hyponutrition in the elderly at admission to the hospital]. Nutr Hosp [Internet]. 2007 [cited 2015 Jan 7];22(6):702–9. Available from: http://www.ncbi.nlm.nih.gov/pubmed/18051996
Cuyac Lantigua M, Santana Porbén S. [The Mini Nutritional Assessment of the elderly in the practice of a hospital geriatrics service: inception, validation and operational characteristics]. Arch Latinoam Nutr [Internet]. 2007 Sep [cited 2015 Jan 7];57(3):255–65. Available from: http://www.ncbi.nlm.nih.gov/pubmed/18271404
Woo J, Chumlea WC, Sun SS, Kwok T, Lui HH, Hui E, et al. Development of the Chinese nutrition screen (CNS) for use in institutional settings. J Nutr Health Aging [Internet]. 2005 [cited 2015 Jan 7];9(4):203–10. Available from: http://www.ncbi.nlm.nih.gov/pubmed/15980920
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Lera, L., Sánchez, H., Ángel, B. et al. Mini Nutritional Assessment short-form: Validation in five Latin American cities. SABE study. J Nutr Health Aging 20, 797–805 (2016). https://doi.org/10.1007/s12603-016-0696-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12603-016-0696-z