
Abstract
Introduction
Coronavirus disease-19 (COVID-19) has been associated with subclinical myocardial dysfunction during its acute phase and a recurring pattern of reduced basal left ventricular longitudinal strain on speckle-tracking echocardiography (STE) in hospitalized patients. But a question still remains unanswered: speckle-tracking echocardiography might also be suitable to detect residual myocardial involvement after acute stage of COVID-19?
Methods and results
We studied 100 patients recovered from COVID-19 with STE to evaluate global (GLS) and segmentar longitudinal strain (LS) and compared with a control group of 100 healthy individuals. STE was performed at a median of 130.35 ± 76.06 days after COVID-19 diagnostic. Demographic and echocardiographic parameters are similar in both groups. Left ventricular ejection faction (LVEF) and GLS were normal in COVID-19 patients (66.20 ± 1.98% and − 19.51 ± 2.87%, respectively). A reduction in mean LS for the basal segments was found in COVID-19 (16.48 ± 5.41%) when compared to control group (19.09 ± 4.31%) (p < 0.001).
Conclusion
The present study suggests that COVID-19-induced cardiac involvement could persist after recovery of the disease and may be detected by deformation abnormalities using STE. COVID-19-induced myocardial involvement often shows specific LV deformation patterns due to pronounced edema and/or myocardial damage in basal LV segments.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Coronavirus disease 2019 (COVID-19), resulting from infection with severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), is causing a worldwide pandemic with high morbidity and mortality. Until the present moment (end August, 2021), a total of 217 million people were infected, with 4.51 million deaths and 192.83 million recovered. Although the respiratory system sees the major impact of the illness, increasing reports describe important cardiac manifestations [1,2,3,4].
Myocardial injury, characterized by cardiac biomarkers elevation and/or abnormalities on transthoracic echocardiography and cardiac magnetic resonance imaging have been yet reported in hospitalized COVID-19 patients [2, 5,6,7,8,9]. This myocardial damage can be caused directly by SARS-CoV-2 virus or by immunopathological sequelae of myocardial inflammation [10,11,12] and is associated with adverse outcomes and increased mortality [2, 7, 13, 14]. In addition, residual myocardial damage after recovery of the acute phase of the disease might have a significant impact on the patients´ long-term prognosis and can culminate in SARS-CoV-2-induced myocardial fibrosis [9]. Furthermore, we suspected that systemic inflammation and hypoxemia may cause secondary myocardial injury in COVID-19.
A technique easily combined with standard echocardiographic measurements is 2-dimensional speckle-tracking echocardiography (STE), which tracks unique speckle pathways during the cardiac cycle to determine myocardial deformation and strain. Strain evaluates myocardial dysfunction and the subclinical impairment of myocardial earlier and has been shown to be more sensitive and accurate in detecting left ventricular (LV) dysfunction compared with the LV ejection fraction (LVEF), specially the Global Longitudinal Strain (GLS) [15,16,17,18]. STE quantifies myocardial deformation globally and regionally, regardless of the insonation angle or cardiac translational movements.
The analysis of segmental longitudinal strain (LS) patterns can be helpful in the identification of cardiac diseases when a characteristic abnormality is seen in conjunction with clinical data, such as the pathognomonic apical-sparing strain reduction seen in cardiac amyolidosis [19]. A recurring pattern of reduced basal left ventricular LS on STE was observed in hospitalized patients with COVID-19.
The question of whether chronic cardiac issues are present after COVID-19 recovery still remains and long-term follow-up is needed.
The aim of our study is to characterize the left ventricular LS patterns in COVID-19 recovered patients and compare with a control group of healthy patients, as whether COVID-19 could cause chronic cardiomyopathy was not known.
Methods
This study was approved by and conducted according to the Institutional Review Board. This was a single-center prospective study of a hundred nonconsecutive patients admitted to our private institution from January 11, 2021, to February 24, 2021 with recovered COVID-19 diagnosed using nasopharyngeal polymerase chain reaction testing (Rt-PCR) in 89 patients (89%) and/or serological dosage of IgM (16 patients—16%) and IgG (31 patients—31%) to undergo clinically indicated transthoracic STE.
STE was performed by an experienced echocardiographer using S6 ultrasound systems (General Electric Vingmed Ultrasound, Milwaukee, WI) at a median of 130.35 ± 76.06 days after Covid-19 diagnostic. Images were analyzed on a dedicated workstation using EchoPAC software (version 202, GE Ultrasound). Within this article, strain is referred to in absolute values. Global (GLS) and regional longitudinal deformation (LS) were assessed by determination of layer strain (basal, mid and apical levels) in all apical views based on the American Heart Association 17-segment model.
Two-D grayscale harmonic images and three consecutive cardiac cycles of each view were obtained, captured at a frame rate between 40 and 60 fps. The endocardial contour was manually adjusted, whereas only segments with accurate tracking by carefully visual evaluation were accepted to exclude imaging artifacts. Segments with poor strain curves were excluded.
LV deformation was analyzed in a control group consisted of 100 healthy patients who had no cardiopulmonary diseases according to their medical history, physical examination and electrocardiogram, who underwent echocardiography study as part of routine pre-surgical risk stratification. As in the COVID group, segments with poor strain curves were excluded.
Comparisons between groups were performed using Welch´s t test for normally distributed continuous variables, and p level of < 0.001 was considered statistically significant.
Results
A hundred patients with recovered COVID-19 underwent STE, with 1633 (96.06%) myocardial segments of a total of 1700 segments included in the analysis; 67 (3.94%) were excluded for poor quality of imaging (29 basal segments, 25 medium segments and 13 apical segments). In the control group of 1700 segments studied, 51 (3%) were excluded (22 in the basal level, 18 in medium and 11 in apical).
Comorbidities such as hypertension and diabetes are rare and diagnosed in 26 (26%) and 11 (11%) patients of the COVID-19 group, respectively. No history of cardiopathy or pulmonary disease prior to COVID-19 was described in this group.
The majority of the patients had no symptoms/mild symptoms (83%), 5 patients had moderate symptoms needing hospitalization but no intubation and 2 (2%) had severe evolution with the need of intubation and mechanical ventilation, but all the patients in the COVID-19 group recovered well although almost half of them (46%) still have mild symptoms at the moment of echocardiogram (short of breath, thoracic pain, palpitations, loss of smell and/or taste).
The mean patient age was 46.93 ± 15.24 years, and 59% were women; the mean control group age of 39.17 ± 9.25 years (p < 0.001) with 50% of women. Although this significant age difference the body surface area (BSA), the heart rate (HR) and left ventricle diastolic diameter (LVDD) were similar in both groups (respectively, BSA = 1.85 ± 0.22 m2 vs 1.82 ± 0.23 m2; p = 0.196, HR = 74,0.44 ± 13.10 bpm vs 69.55 ± 10.19 bpm; p = 0.003, and LVDD = 47.75 ± 3.70 mm vs 47.47 ± 3.78 mm; p = 0.088) (Table 1).
Although the left ventricular ejection faction (LVEF) was between the range of normality in both groups, a small but significant difference was found between the 2 groups (66.20 ± 1.98% in the COVID-19 group vs 68.60 ± 5.33% in the control group: p < 0.001).
Left ventricular GLS for the COVID-19 group was 19.51 ± 2.87% and was in between the 95%CI for normal, healthy patients with preserved LV function (19.7–95% CI: 20.4 to 18.9%) [20].
Regional LS values per myocardial segment for COVID-19 and control group are on Table 2, with no statistical difference between them all, in each group.
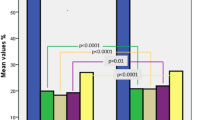
The mean LS for the basal segments was reduced in COVID-19 (16.48 ± 5.41%) when compared to control group (19.09 ± 4.31%), with statistically significant difference between the groups (p < 0.001) (Fig. 1). This reduction in LS in COVID-19 group was most prominent on anterior, inferior and septal basal segments (Table 2). LS values were similar for medium and apical segments in both groups.

Representative images of segmentar longitudinal strain (LS) presented as “bull´s-eye”. A LS of a normal subject from control group; B–F LS of 5 representative patients with recovered COVID-19 found to have a recurring pattern of reduced LS in the basal segments of the left ventricle
Discussion
To our knowledge, this is the first study in the literature evaluating LV mechanics by STE in long-term follow-up of recovered COVID-19 patients.
Indices of longitudinal strain are known to strongly correlate with the levels of lymphocytic infiltrates in endomyocardial biopsy (EMB) samples [21] and with the amount of edema detected by cardiac magnetic resonance (CMR) [22]. Moreover, the diagnostic performance of LS in acute myocarditis has been validated by showing preferential alteration of subepicardial deformation that was consistent with tissue characteristics established by CMR [23]. Therefore, although CMR and EMB are the gold standards for the diagnosis of myocarditis, the evidence shows a good correlation between echocardiographic strain and CMR [24].
Speckle-tracking echocardiography works as a “digital biopsy” and it could become an essential diagnostic tool for myocarditis and other cardiomyopathies [25].
Previous report using CMR in 100 individuals recovered from COVID-19 detected cardiovascular involvement in 78 of them, irrespective or preexisting conditions, the severity and overall course of the COVID-19 presentation, the time from the original diagnosis, or the presence of cardiac symptoms [26]. This study was corroborated by another autopsy study [27].
There are a few studies showing reduction in GLS during acute hospitalized patients, regardless of the severity of the COVID-19, even in the presence of normal LVEF [5, 9, 18, 28,29,30,31] compatible with subclinical LV dysfunction.
In corroboration to our findings, other studies using STE for diagnosis of cardiac involvement during acute COVID-19 showed reduction of LS in more than one of the basal LV segments [9, 32], despite normal LVEF and even in the presence of normal GLS. And in one study, abnormal LV deformation patterns were still observed in 3 patients after recovery from acute stage, indicating residual myocardial involvement [9]. Furthermore, CMR showed late enhancement predominantly in the basal inferolateral/anterolateral LV segments indicating myocardial fibrosis or scars, respectively [8, 9, 33]. This basal injury pattern reflects the susceptibility of certain myocardial regions to inflammatory or systemic stressors rather than a geographic predilection specific to COVID-19.
Another plausible hypothesis, more specific to COVID-19, involves the viral receptor, angiotensin-converting enzyme 2 (ACE2). This membrane-bound enzyme is responsible for production of angiotensin [1,2,3,4,5,6,7], leading to well-described anti-inflammatory and anti-thrombotic effects [34]. ACE2 is highly expressed in fat, and epicardial adipose tissue (EAT) is more prominent in the atrioventricular groove and lateral LV wall, closer to the basal segments [35]. Loss of ACE2 has been shown to result in heart failure with preserved LVEF, mediated in part by EAT inflammation. Thus, COVID-19 binding of ACE2 may occur more prominently in areas of high EAT, such as the basal LV, and cause subclinical dysfunction via inflammatory downstream effects [32].
Case reports and series of patients with various forms of myocarditis, including influenza myocarditis, have described a similar pattern of reduced basal strain on STE [36, 37]. Abnormal basal LS has also been seen in infiltrative cardiomyophaties including Anderson-Fabry disease [38].
Our study is limited in several ways. First, data were derived from a single center and the sample size was relatively small. Second, no strain on STE data was obtained from patients prior to COVID-19 infection, so the reduced basal strain was found in COVID-19-recovered patients, whether these abnormalities were previously present and thus unrelated to the infection is unknown. Third, a few percentage of cases had inadequate imaging for STE analysis of some segments. And finally, although the study raised the possibility that COVID-19 was associated with prevalent cardiac abnormalities and could potentially cause myocarditis, direct evidence remains lacking.
Conclusions
The present study suggests that COVID-19-induced cardiac involvement could persist after recovery of COVID-19 and may be detected by deformation abnormalities using STE. COVID-19-induced myocardial involvement often shows specific LV deformation patterns due to pronounced edema and/or myocardial damage in basal LV segments.
Whether myocardial viral activity in the absence of clinical evidence of myocarditis might result in long-term consequences is unknown, but the findings of our study indicate the need for ongoing investigation of the long-term cardiovascular consequences of COVID-19.
Further studies with large patient sample size will be needed to confirm and expand on our findings.
Data availability
Not applicable.
Code availability
Not applicable.
References
Babapoor-Farrokan S, Gill D, Walker J, Rasekhi RT, Bozorgnia B, Amanullah A. Myocardial injury and COVID-19: possible mechanisms. Life Sci. 2020;253: 117723. https://doi.org/10.1016/j.lfs.2020.117723.
Shi S, Qin M, Shen B, et al. Association of cardiac injury with mortality in hospitalized patients with COVID-19 in Wuhan, China. JAMA Cardiol. 2020;5(7):802–10. https://doi.org/10.1001/jamacardio.2020.0950.
Chen T, Wu D, Chen H, et al. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: retrospective study. BMJ. 2020;368: m1091. https://doi.org/10.1136/bmj.m1091.
Yang X, Yu Y, Xu J, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-center, retrospective, observational study. Lancet Respir Med. 2020;8:475–81. https://doi.org/10.1016/S2213-2600(20)30079-5.
Janus SE, Hajjari J, Karnib M, Tashtish N, Al-Kindi SG, Hoit BD. Prognostic value of left ventricular global longitudinal strain in COVID-19. Am J Cardiol. 2020;131:134–6. https://doi.org/10.1016/j.amjcard.2020.06.053.
Li Y, Li H, Zhu S, et al. Prognostic value of right ventricular longitudinal strain in COVID-19. JACC Cardiovasc Imaging. 2020;13(11):2287–99. https://doi.org/10.1016/j.jcmg.2020.04.014.
Ruan Q, Yang K, Wang W, Jiang L, Song J. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med. 2020;46(5):846–8. https://doi.org/10.1007/s00134-020-05991-x.
Huang L, Zhao P, Tang D, et al. Cardiac involvement in patients recovered from COVID-19 identified using magnetic resonance imaging. JACC Cardiovasc Imaging. 2020;13(11):2330–9. https://doi.org/10.1016/j.jcmg.2020.05.004.
Stobe S, Richter S, Seige M, Stehr S, Laufs U, Hagendorff A. Echocardiographic characteristics of patients with SARS-CoV-2 infection. Clin Res Cardiol. 2020;109(12):1549–66. https://doi.org/10.1007/s00392-020-01727-5.
Kang Y, Chen T, Mui D, et al. Cardiovascular manifestations and treatment considerations in COVID-19. Heart. 2020;106:1132–41. https://doi.org/10.1136/heartjnl-2020-317056.
Rizzo P, Vieceli Dalla Sega F, Fortini F, Marracino L, Rapezzi C, Ferrari R. COVID-19 in the heart and the lungs: could we “Notch” the inflammatory storm? Basic Res Cardiol. 2020;115(3):31. https://doi.org/10.1007/s00395-020-0791-5.
Siripanthong B, Nazarian S, Muser D, et al. Recognizing COVID-19-related myocarditis: the possible pathophysiology and proposed guideline for diagnosis and management. Heart Rhythm. 2020;17(9):1463–71. https://doi.org/10.1016/j.hrthm.2020.05.001.
Lippi G, Plebani M. Laboratory abnormalities in patients with COVID-19 infection. Clin Chem Lab Med. 2020;58(7):1131–4. https://doi.org/10.1515/cclm-2020-0198.
Sala S, Peretto G, Gramegna M, Palmisano A, Villatore A, Vignale D. Acute myocarditis presenting as a reverse takotsubo syndrome in a patient with SARS-CoV-2 respiratory infection. Eur Heart J. 2020;41(19):1861–2. https://doi.org/10.1093/eurheartj/ehaa286.
Potter E, Marwick TH. Assessment of left ventricular function by echocardiography: the case for routinely adding global longitudinal strain to ejection fraction. JACC Cardiovasc Imaging. 2018;11(2 Pt 1):260–74. https://doi.org/10.1016/j.jcmg.2017.11.017.
Carluccio E, Biagioli P, Alunni G, et al. Prognostic value of right ventricular dysfunction in heart failure with reduced ejection fraction: superiority of longitudinal strain over tricuspid annular plane systolic excursion. Circ Cardiovasc Imaging. 2018;11(1): e006894. https://doi.org/10.1161/CIRCIMAGING.117.006894.
Xie M, Li Y, Cheng TO, et al. The effect of right ventricular myocardial remodeling on ventricular function as assessed by two-dimensional speckle tracking echocardiography in patients with tetralogy of Fallot: a single center experience from China. Int J Cardiol. 2015;178:300–7. https://doi.org/10.1016/j.ijcard.2014.10.027.
Baycan OF, Barman HA, Atici A, et al. Evaluation of biventricular function in patients with COVID-19 using speckle tracking echocardiography. Int J Cardiovasc Imaging. 2020. https://doi.org/10.1007/s10554-020-01968-5.
Zito C, Longobardo L, Citro R, et al. Ten years of 2D longitudinal strain for early myocardial dysfunction detection: a clinical overview. Biomed Res Int. 2018;2018:8979407. https://doi.org/10.1155/2018/8979407.
Yingchoncharoen T, Agarwal S, Popovic Z, Marwick T. Normal ranges of left ventricular strain: a meta-analysis. J Am Soc Echocardiogr. 2013;26(2):185–91. https://doi.org/10.1016/j.echo.2012.10.008.
Kasner M, Sinning D, Escher F, et al. The utility of speckle tracking imaging in the diagnostic of acute myocarditis, as proven by endomyocardial biopsy. Int J Cardiol. 2013;168(3):3023–4. https://doi.org/10.1016/j.ijcard.2013.04.016.
Logstrup BB, Nielsen JM, Kim WY, Poulsen SH. Myocardial oedema in acute myocarditis detected by echocardiographic 2D myocardial deformation analysis. Eur Heart J Cardiovasc Imaging. 2016;17(9):1018–26. https://doi.org/10.1093/ehjci/jev302.
Caspar T, Germain P, El Ghannudi S, et al. Acute myocarditis diagnosed by layer-specific 2D longitudinal speckle tracking analysis. Echocardiography. 2016;33(1):157–8. https://doi.org/10.1111/echo.13045.
Leitman M, Vered Z, Tyomkin V, et al. Speckle tracking imaging in inflammatory heart diseases. Int J Cardiovasc Imaging. 2018;34(5):787–92. https://doi.org/10.1007/s10554-017-1284-y.
Shah SJ. 20th Annual Feigenbaum lecture: echocardiography for precision medicine-digital biopsy to deconstruct biology. J Am Soc Echocardiogr. 2019;32(11):1379-95,e2. https://doi.org/10.1016/j.echo.2019.08.002.
Puntmann VO, Carerj L, Wieters I, et al. Outcomes of cardiovascular magnetic resonance imaging in patients recently recovered from coronavirus disease 2019 (COVID-19). JAMA Cardiol. 2020;5(11):1265–73. https://doi.org/10.1001/jamacardio.2020.3557.
Lindner D, Fitzek A, Bräuninger H, et al. Association of cardiac infection with SARS-CoV-2 in confirmed COVID-19 autopsy cases. JAMA Cardiol. 2020;5(11):1281–5. https://doi.org/10.1001/jamacardio.2020.3551.
Croft LB, Krishnamoorthy P, Ro R, et al. Abnormal left ventricular global longitudinal strain by speckle tracking echocardiography in COVID-19 patients. Future Cardiol. 2020. https://doi.org/10.2217/fca-2020-0121.
Li R, Wang H, Ma F, et al. Widespread myocardial dysfunction in COVID-19 patients detected by myocardial strain imaging using 2-D speckle-tracking echocardiography. Acta Pharmacol Sin. 2021;42(10):1567–74. https://doi.org/10.1038/s41401-020-00595-z.
Krishnamoorthy P, Croft L, Ro R, et al. Biventricular strain by speckle tracking echocardiography in COVID-19: findings and possible prognostic implications. Future Cardiol. 2021;17(4):663–7. https://doi.org/10.2217/fca-2020-0100.
Wehit JM, Sosa F, Merlo P, Roberti J, Osatnik J. Identification of COVID-19-associated myocarditis by speckle-tracking transesophageal echocardiography in critical care. Acta Colomb Cuid Intensivo. 2020. https://doi.org/10.1016/j.acci.2020.11.008.
Goerlich E, Gilotra NA, Minhas AS, Bavaro N, Hays AG, Cingolani OH. Prominent longitudinal strain reduction of basal left ventricular segments in patients with coronavirus disease-19. J Card Fail. 2021;27(1):100–4. https://doi.org/10.1016/j.cardfail.2020.09.469.
Salerno M, Kwong RY. CMR in the era of COVID-19. JACC Cardiovasc Imaging. 2020;13(11):2340–2. https://doi.org/10.1016/j.jcmg.2020.06.013.
Patel VB, Mori J, McLean BA, et al. ACE2 deficiency worsens epicardial adipose tissue inflammation and cardiac dysfunction in response to diet-induced obesity. Diabetes. 2016;65(1):85–95. https://doi.org/10.2337/db15-0399.
Abbara S, Desai JC, Cury RC, Butler J, Nieman K, Reddy V. Mapping epicardial fat with multi-detector computed tomography to facilitate percutaneous transepicardial arrhythmia ablation. Eur J Radiol. 2006;57(3):417–22. https://doi.org/10.1016/j.ejrad.2005.12.030.
Ha SJ, Woo JS, Kwon SH, et al. Acute regional myocarditis with normal ventricular wall motion diagnosed by two-dimensional speckle tracking imaging. Korean J Intern Med. 2013;28(6):732–5. https://doi.org/10.3904/kjim.2013.28.6.732.
Hawwa N, Popovic ZB, Isma’eel HA. Discordant electrocardiogram left ventricular wall thickness and strain findings in influenza myocarditis. Echocardiography. 2015;32(12):1880–4. https://doi.org/10.1111/echo.13024.
Esposito R, Galderisi M, Santoro C, et al. Prominent longitudinal strain reduction of left ventricular basal segments in treatment-naïve Anderson–Fabry disease patients. Eur Heart J Cardiovasc Imaging. 2019;204:438–45. https://doi.org/10.1093/ehjci/jey108.
Funding
None.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Caiado, L.D.C., Azevedo, N.C., Azevedo, R.R.C. et al. Cardiac involvement in patients recovered from COVID-19 identified using left ventricular longitudinal strain. J Echocardiogr 20, 51–56 (2022). https://doi.org/10.1007/s12574-021-00555-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12574-021-00555-4