
Abstract
The purpose of this study was to investigate whether there are any age-related differences in impact characteristics during running between healthy older and younger men. Ten healthy older (age: 58.7 ± 2.5 years) male and ten healthy younger (age: 22.3 ± 1.6 years) male recreational runners ran on a treadmill at three different running speeds (i.e. 2.2 m/s, 2.8 m/s, and 3.2 m/s). Tri-axial accelerometers (Noraxon, USA) were firmly attached to the tibia and the sternum. Gait parameters, three-dimensional peak tibial accelerations, peak sternum accelerations and shock attenuation were calculated during the stance phase of running. The ANOVA repeated measures was applied at an alpha level of .05. Older runners showed greater impact on the sternum, leading to reduced shock attenuation compared with younger runners (p < .05). In addition, older runners showed a shorter lag between peak resultant accelerations experienced by the upper body and peak acceleration experienced by the lower leg compared with younger runners (p < .05). This study suggests that the intensity (i.e. speed and duration) and types of exercise should be carefully considered for older adults because of lower shock attenuation of the body and changes in coordination strategy between the segments in high-impact activities like running.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
Regular running provides many health benefits for those in middle and old age including improved cardiovascular health [1], bone mineral density [2] and motor skills function [3]. However, repetitive high impacts during running may play a role in the development of running-related overuse injuries in older runners because of age-related decrease in function [4]. In the process of aging, the human body loses muscle strength [5] and flexibility [6], and changes running biomechanics [4, 7,8,9]. Older runners decrease running velocity, stride length [4], and knee range of motion [7] while greater ground reaction force impact peaks and loading rates have been observed in older runners compared with younger runners [7]. It has been suggested that the older body’s reduced ability to attenuate high-impact forces during running may lead to a higher incidence of lower extremity joint injuries in an older population [7, 10, 11].
Several studies have compared the differences in joint kinematics and kinetics between young adult runners and older adult runners to understand age-related adaptations in running biomechanics [4, 7,8,9, 12]. Reduced lower extremity joint motion [7, 12] in older runners is thought to be related to a reduced impact-attenuation ability compared with young runners. Previous studies suggest that older adults redistribute mechanical demands in the lower extremity during walking [13, 14] and running [15]. However, little is known about the impact-attenuation ability of older individuals during high impact exercise like running. The magnitude of impact on the body and the response to reduce high impacts from the ground during running in older runners haven’t been well investigated in previous studies. Thus, a better understanding of impact characteristics in older runners may help to mitigate lower extremity joint injury in this population [16].
An accelerometer has been widely used as a portable and reliable device for the measurement of the impact at initial contact (i.e. within 50 ms of touchdown) in running since positive correlations were found between the peak accelerations from the accelerometer and the impact variables such as impact peak and its loading rate measured by a force plate [17,18,19]. Repetitive impact, such as when the foot strikes the ground during running, can be measured by accelerometers as the accelerometer signals are clearly differentiated by running style (i.e. foot strike pattern, stride length and lower extremity joint angles) as well as running surface and footwear compliance [20]. The findings from accelerometers regarding age-related changes in impact characteristics have shown an important dynamic role of the upper body of the older person in impact attenuation during walking [21, 22]. However, to our knowledge, there are no studies that have investigated the impact attenuation ability of older individuals during running when impacts are more pronounced. Furthermore, biomechanics studies of older runners should measure three dimensional impact because acceleration in the medial–lateral (M–L) and anterior–posterior (A–P) axes contributes a substantial amount to overall impact [21, 22] and they are closely related to stability and control of movement in the older adult [21,22,23]. Therefore, the purpose of this study was to investigate impact characteristics of older runners using tri-axial accelerometers for a better understanding of their strategy to attenuate impacts. We adopted the term, impact acceleration to represent the magnitude of impact at an initial contact of stance phase during running [24]. The first hypothesis was that older runners would show greater magnitudes of impact accelerations compared with younger runners. The second hypothesis was that older runners would show a lower impact attenuation, calculated by a relative reduction of impact acceleration on the upper body with respect to impact acceleration on the lower leg [25], compared with younger runners. Also, it was expected that the magnitudes of impact and the level of impact attenuation would increase with increased running speed for both groups of runners.
2 Method
2.1 Participants
Ten healthy older (age: 58.7 ± 2.5 years, mass: 72.3 ± 7.4 kg, height: 171.1 ± 4.7 cm, BMI: 24.7 ± 2.1, weekly running: 4.4 ± 2.4 h) and ten healthy younger (age: 22.3 ± 1.6 years, mass: 73.5 ± 5.2 kg, height: 176.2 ± 6.7 cm, BMI: 23.8 ± 2.1, weekly running: 1.5 ± 1.3 h) male recreational runners participated in the study. There were significant differences in age and weekly exercise levels between two groups (p < .05) but no difference in mass, height, or BMI. Subject criteria included no lower extremity injuries within the past six months, rearfoot striker, minimum running distance of 10 km/week, the ability to run comfortably on a treadmill, and a time of under one hour for 10 km of running. The running shoe was not standardized and each participant wore their own shoes to perform their natural running patterns [26]. The research was approved by the Korea National Sport University ethics committee and written consent was obtained from each participant prior to the start of the experiment (Ethics ID: 20,150,618–693, 20,180,611–046).
2.2 Procedure
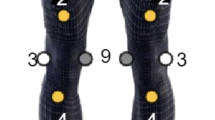
Two tri-axial accelerometers (Noraxon, USA, model: DTS 519 3D accelerometer, mass: 2.4 g, size: 20 mm by 15 mm by 7 mm, operational range of 100–400 g) were firmly attached to the middle of the runner’s right tibia and the sternum with double sided tape and elastic straps (Fig. 1). The orthogonal coordinate system was set in the tibia [27]. To measure vertical acceleration on the tibia, the vertical axis of the accelerometer was set in the direction (+) aligned with the longitudinal axis of the tibia. Due to the shape of the bone surface of the tibia, the direction (+) of the A–P axis of the accelerometer was pointing approximately 45 degrees medially [28]. The direction (+) of the M–L axis was set perpendicular to the plane created by the vertical and A–P axes. The vertical axis of the accelerometer on the sternum was aligned with the direction (+) pointing upward while the A–P and M–L axes were set with the axes perpendicular to the vertical axis, respectively [29] (Fig. 1). After an adaptation period of running on a treadmill (Bertec, USA) built into the floor, the subjects were asked to run at three different speeds (2.2 m/s, 2.8 m/s and 3.2 m/s). The running shoe was not standardized and each participant wore their own shoes to perform their own natural running patterns. The order of running speed was randomly assigned to avoid a learning effect. The last ten steps of the right foot during the three minutes running trials were selected for analysis [30]. Data was collected at 500 Hz and low-pass filtered at 50 Hz [31].

Orientation of 3 axes for each tri-axial accelerometer on the participant
2.3 Data Analysis
The data was imported into software (Visual 3D, C-Motion, USA) to calculate running parameters such as contact time, stride time, stride length and stride frequency [30]. Figure 2 shows the three-dimensional accelerations and the resultant value on the tibia during running at 2.8 m/s. Peak tibial acceleration (PTA) and peak sternum acceleration (PSA) for all three axes and their resultant accelerations (Eq. 1) during the stance phase of running were calculated for comparison. A method for detecting heel contact and toe off using an accelerometer was applied to determine the stance phase of running [32]. Shock attenuation (SA) using longitudinal and resultant acceleration was determined by calculating the percentage of peak acceleration from the sternum with respect to the peak acceleration from the tibia [33,34,35] (Eq. 2). Data were processed by using a custom written Matlab code (Mathworks, USA).
L, peak acceleration in the longitudinal axis; ML, peak acceleration in the M–L axis; AP, peak acceleration in the A–P axis
SA, shock attenuation; PTA, peak tibial acceleration, PSA, peak sternum acceleration.

Time normalized accelerations in three axes and the resultant value on the tibia during running at 2.8 m/s. G = 9.8 m/s2, L, longitudinal axis; ML, medial–lateral axis; AP, anterior–posterior axis; R, resultant value
3 2.4 Statistical analysis
A sample size from each group was determined using the results of a previous study [21] regarding upper body accelerations in older adults. The mean and standard deviation of peak accelerations in the A–P axis from the aforementioned study were utilized to calculate the effect size of 1.34 (G-power software), with a statistical power set to .8 and an alpha level of .05. Based on the analysis of G-power, a minimum of eight participants for each group was required to compare the differences between the two groups. The normality test (Kolmogorov–Smirnov & Shapiro–Wilk) was conducted if the variables met the criteria for parametric statistics. All statistical comparisons were made using the 2 (age effect) × 3 (speed effect) ANOVA repeated measures with the least significant differences method for post-hoc analysis at an alpha level of .05 (SPSS Inc., USA). p values, effect size (η2) and power (β) were reported in the statistical analysis results.
4 Results
4.1 Gait Parameters
Table 1 shows the results of age (older runners vs. younger runners) and running speed (i.e. 2.2 m/s, 2.8 m/s, and 3.2 m/s) effects on gait parameters. Older runners showed a shorter contact time and stride time compared with younger runners while both groups of runners tended to decrease contact time and stride time with increased running speed (p < .01). Older runners showed a shorter stride length and higher stride frequency compared with younger runners while both groups of runners tended to increase stride length and stride frequency with increased running speed (p < .01).
4.2 Peak Tibial Acceleration (PTA)
Table 2 shows the results of age and running speed effects on PTA. In the longitudinal direction, there were no differences in PTA between the two age groups while both groups of runners increased PTA with increased running speed (p < .01). In the M–L direction, there were no differences in PTA between the two groups while both groups of runners increased maximum PTA with increased running speed (p < .01). In the A–P direction, there were no differences in PTA between the two groups while both groups of runners showed increased minimum PTA with an increased running speed (p < .01).
4.3 Peak Sternum Acceleration (PSA)
In the comparisons of PSA, older runners showed greater PSA in the longitudinal direction, compared with younger runners while a speed effect on PSA was observed in both groups of runners (Table 2, p < .01). Furthermore, in the A–P direction, older runners also showed greater maximum PSA compared with younger runners (p = .04). Finally, in the M–L direction, there were no differences in PSA between the two groups while both groups of runners increased maximum PSA with increased running speed (p < .01). In addition, there was an interaction effect as younger runners tended to show a greater increase in PSA in the M–L direction with increased running speed compared with older runners (p = .02).
4.4 Resultant Acceleration and Shock Attenuation (SA)
Figure 3 represents the comparison of the resultant accelerations on the tibia and the sternum between the two groups. Table 3 shows the comparisons of resultant accelerations and shock attenuations between the two groups at three running speeds. Regarding the magnitude of the resultant accelerations (i.e. summation of all three acceleration components), older runners showed greater resultant acceleration on the sternum compared with younger runners (p < .01) while both groups of runners showed increased resultant sternum acceleration with an increased running speed (p < .01). Furthermore, older runners showed earlier peak accelerations at the sternum compared with younger runners while no speed effect was observed on the time to peak resultant accelerations for either group of runners (Fig. 3, Table 3, p < .01). When calculating SA using peak acceleration along the longitudinal axis, older runners showed significantly lower SA compared with younger runners (p = .01). Furthermore, when considering peak resultant accelerations of the tibia and the sternum in the calculation, SA was also lower in older runners compared with younger runners (p < .01). There was a speed effect on SA using resultant accelerations for both groups of runners (p < .05). In addition, older runners showed greater increment in SA with an increased running speed compared with younger runners but it was not statistically significant.

Comparisons of the resultant accelerations between the two groups at three running speeds (* indicates significant differences in the magnitude and timing of peak resultant acceleration at an alpha level of .05.)
5 Discussion
The purpose of this study was to investigate whether any age-related differences exist in the magnitude of impact and the level of impact attenuation of the body during running between healthy older and younger runners. There were no significant differences in the magnitude of impact on the lower leg between the two groups, but greater magnitude of peak acceleration on the upper body was observed in older runners compared with younger runners. In the longitudinal axis PSA was approximately 17–19% higher in older runners and in the A–P axis PSA was approximately 21–24% higher in older runners. Using resultant accelerations, about 18% higher PSA was also observed in the older group compared with the younger group. Thus, the first hypothesis that older runners will show greater impact on the body compared with younger runners was partially supported. Furthermore, SA was approximately 29–48% lower in the longitudinal axis and 25–36% lower using resultant accelerations in the older group compared with the younger group. Thus, the second hypothesis that older runners will show a lower level of shock attenuation (SA) compared with younger runners was also supported.
There were no differences between the two groups in the magnitudes of impact on the lower leg using accelerometers. A study compared ground reaction forces and lower extremity kinematics between 16 older (55–65 years old) and 13 younger (20–35 years old) runners at a preferred and a controlled running speed, respectively [7]. The finding showed that, using a force plate under controlled speed of running at 3.3 m/s, greater impact peak and loading rate was observed in older runners when compared with younger runners. However, our results regarding the magnitude of impact on the tibia using accelerometers showed similar levels of impact on the lower leg between the two age groups. The values of peak tibial acceleration in this study ranged from 5 to 7 g for the longitudinal axis, 3.5–5 g for ML axis, and 2–3 g for AP axis, which are comparable to the values under similar experimental settings in previous studies [35,36,37,38]. Previous studies have suggested that peak acceleration using a bone-mounted accelerometer and impact peak and loading rate collected by a force plate are reasonably correlated during walking and running [17, 27]. However, this relationship becomes weaker with a skin-mounted accelerometer [39] and it is also dependent on the attachment methods and placement location of accelerometers [20]. Our findings suggest no age effect on the magnitude of impact using a tri-axial accelerometer on the tibia as both groups of runners experience similar levels of impact on the lower leg during running. However, because of the expected decreased in bone mineral density (BMD) and weaker muscle structure with the aging process [40,41,42], it is suggested that older adults exposed to repetitive high impact during running may be more vulnerable to bone and muscle injuries of lower extremity joints [9, 16].
When comparing PSA along the longitudinal and A–P axes as well as the resultant PSA (i.e. summation of all three acceleration components) between the two groups, the older runners experienced a greater amount of impact on the upper body than the younger runners. Previous studies have emphasized the importance of the upper body in controlling movement stability and coordinating joint coupling with lower extremity joints [21, 22, 43, 44]. Specifically, due to greater weight distributed on the upper body compared to the lower body [44], controlling upper body movement plays an important dynamic role in attenuating impact [21, 23]. Previous observations suggest that the upper body of older adults becomes stiffer than that of young adults with a loss of effective control of lower body motion during walking [21]. This increased rigidity of the upper body due to reduced pelvic rotation both in the sagittal and the transverse plane [22, 23, 45] and diminished balance control by the lumbar and the cervical hinges [23] may compromise the function of the upper body as an attenuator to high impact during running as well. Our findings revealed that older runners demonstrated greater magnitudes of impact on the upper body, possibly caused by the changes in running biomechanics due to potentially decreased trunk function.
The impact from the ground is transmitted to the upper body during running and its magnitude can be reduced with the use of protective mechanisms by the runner [7]. Older runners reduce speed [7] and modify gait parameters as they have a shorter stride length and higher stride frequency compared with younger runners [8]. This is also supported by our findings in gait parameters. In addition, it has been reported that older adults reduce the range of knee flexion–extension and hip joint loading in the frontal plane by decreasing their hip adduction angle during running [14]. This indicates that older runners carefully adjust many biomechanical factors to reduce the effect of high impact generated from contact with the ground.
A study has suggested that shock attenuation and energy absorption during the impact phase of running are increased with increased stride length [46]. The results indicated that increased stride length creates more flex in the knee which contributes to increased overall shock attenuation and energy absorption by the knee compared with the ankle and hip joints. More specifically, a study has reported that older runners tend to show a more flexed knee at initial contact but reduction in the total range of knee flexion–extension during the stance phase of running at a speed of 3.1 m/s compared with young runners [8]. This increase in knee flexion at heel contact may adapt the role of active muscles in impact attenuation in the lower extremity [47], which may compensate for stiff and weak lower extremity joints in older runners [7]. However, decreased range of knee flexion throughout the impact phase during running is observed in older runners [8]. This change would be linked to weak eccentric contractions surrounding the knee which may compromise the function of adequate energy absorption within the musculoskeletal system [46, 47]. Previous studies also supported the idea that modifying knee joint motion plays an important role in adjusting the impact characteristics of runners [47, 48]. However, older runners tend to decrease stride length with more knee extension during the impact phase [8] and this strategy may be disadvantageous to absorption of impact on the body during running [46]. Furthermore, a study suggests that older runners take more steps (approximately 21%) in the same distance due to a shorter step length [7], eventually, accumulating a greater amount of impact compared to that of the younger runners. Thus, it is important to understand how biological structures (i.e. ligament, cartilage, tendon, bone and muscle) in the older runner respond to rapid high impact as well as to accumulated amounts of impact during a longer period of running and this warrants further study.
The main finding of this study was that older runners demonstrated a lower impact attenuation by the upper body during running compared with their younger counterparts. It has been suggested that restricted trunk motion due to rigidity increased by aging may reduce the coordination between the lower leg and upper body during walking [22]. In our comparison of the timing of peak resultant accelerations between the two groups, older runners showed a shorter lag between peak acceleration experienced by the lower leg and peak acceleration experienced by the upper body compared with younger runners (Fig. 3). Whether these shorter timings of accelerations between the lower leg and upper body reflect a more cautious and conservative running strategy requires further attention. In addition, investigating how kinematic variables such as trunk and lower extremity joint angles and angular velocities are linked to decreased impact attenuation of in older runners would be beneficial to understanding the mechanism of impact attenuation. On the other hand, a compensatory mechanism (i.e. transferring the mechanical loads from the ankle to the hip joint) has been reported during walking in older adults [49, 50]. Furthermore, weaker ankle plantar-flexors and knee extensors in older adults may also compromise the ability of impact attenuation and transfer the loads from the ankle and knee to the hip and upper body during running. Interestingly, even though older runners demonstrated a lower degree of impact attenuation of the body, they increased SA up to 35% with an increased running speed. Therefore, our study revealed that a possible protective mechanism to high intensity or increased demands created by a faster running speed may activate in older runners. However, it is still questionable if this increment in SA is enough to compensate for the older runner’s potential age-related reduced biomechanical functions when both groups of runners are exposed to the same amount of impact.
There are some limitations and implications in this study that need to be addressed for a proper interpretation of the results. First, due to skin laxity, a skin-mounted accelerometer would overestimate actual impact compared with the impact measured by a bone-mounted accelerometer [51]. Furthermore, it is expected that this effect would be amplified in older-aged individuals. A study showed that there are regional variations in skin elasticity of the body with a general trend toward decreased skin elasticity with age [52]. Studies have suggested that a lighter accelerometer on the skin with a firm attachment would be critical in order to reduce skin movement for the measurement [51, 53]. We used a light weight accelerometer with a mass of 2.4 g to reduce the effect of skin movement artefact [54] and selected the proper attachment method [20, 54]. Careful preparation of the method and interpretation of the results when using a skin-mounted accelerometer is necessary. Second, we chose to label the components of acceleration from a tri-axial accelerometer on the tibia as A–P and M–L accelerations, which, in some instances, may not be well aligned with the direction of running. However, our study calculated the resultant acceleration of all three axes using a tri-axial accelerometer to avoid the issue of the alignment of the device to the tibia [34]. Third, different placements of an accelerometer on the tibia may not give comparable data [19] because linear acceleration is influenced by tibial angular motion and the distance of the device with respect to the ankle joint may differ [55]. Fourth, the current findings also indicate that measuring accelerations only in the longitudinal direction underestimates the total impact at the tibia (approximately 12–19%) and the sternum (approximately 2–3%) compared with determining three-dimensional vector summed resultant accelerations. When considering the contributions from accelerations in the M–L and A–P axes to overall impact, the resultant acceleration may suggest a better understanding of the impact mechanism during running in regards to age, gender, skill level, movement patterns and so on. Thus, it is recommended that future studies investigating impact characteristics (i.e. peak acceleration and shock attenuation) during running measure all three axial components and the resultant value for a better estimation of overall impact. Fifth, the older runners who participated in this study comprised a small healthy and active group of middle-aged runners whose running mechanics may not differ from those of the young runners. Therefore, future study needs to include a wider range of fitness levels in the older population for generalization of the findings. Finally, it is also suggested that controlled running shoes may minimize the effect of running shoes (i.e. shoe cushioning and design) on running impacts and biomechanics.
6 Conclusion
Investigating impact characteristics of running biomechanics in older runners would suggest the need for a proper training method and intensity that concentrates on maintaining physical health by reducing running related musculo-skeletal injuries. Based on the findings of this study, older runners demonstrated greater upper body impact due to a lower impact-attenuation rate which may increase loads on the musculo-skeletal system compared with younger runners. Thus, the intensity (i.e. speed and duration) and types of exercise for older adults should be carefully considered because of reduced control of the body with high-impact exercise like running. A future investigation of kinematic and kinetic changes using a motion-capture system would be helpful for developing a proper exercise program and specific shoe design and cushioning for older runners.
References
Kusy, K., & Zielinski, J. (2014). Aerobic capacity in speed-power athletes aged 20–90 years vs endurance runners and untrained participants. Scandinavian Journal of Medicine & Science in Sports, 24, 68–79. https://doi.org/10.1111/j.1600-0838.2012.01496.x
Martyn-St James, M., & Carroll, S. (2009). A meta-analysis of impact exercise on postmenopausal bone loss: The case for mixed loading exercise programmes. British Journal of Sports Medicine, 43, 898–908. https://doi.org/10.1136/bjsm.2008.052704
Power, G. A., Dalton, B. H., Behm, D. G., Doherty, T. J., Vandervoort, A. A., & Rice, C. L. (2012). Motor unit survival in lifelong runners is muscle dependent. Medicine & Science in Sports & Exercise, 44, 1235–1242. https://doi.org/10.1249/MSS.0b013e318249953c
Devita, P., Fellin, R. E., Seay, J. F., Ip, E., Stavro, N., & Messier, S. P. (2016). The Relationships between age and running biomechanics. Medicine & Science in Sports & Exercise, 48, 98–106. https://doi.org/10.1249/MSS.0000000000000744
McGibbon, C. A. (2003). Toward a better understanding of gait changes with age and disablement: Neuromuscular adaptation. Exercise and Sport Sciences Reviews, 31, 102–108. https://doi.org/10.1097/00003677-200304000-00009
Vandervoort, A. A., Chesworth, B. M., Cunningham, D. A., Paterson, D. H., Rechnitzer, P. A., & Koval, J. J. (1992). Age and sex effects on mobility of the human ankle. The Journals of Gerontology, 47, M17-21. https://doi.org/10.1093/geronj/47.1.m17
Bus, S. A. (2003). Ground reaction forces and kinematics in distance running in older-aged men. Medicine & Science in Sports & Exercise, 35, 1167–1175. https://doi.org/10.1249/01.MSS.0000074441.55707.D1
Fukuchi, R. K., & Duarte, M. (2008). Comparison of three-dimensional lower extremity running kinematics of young adult and elderly runners. Journal of Sports Sciences, 26, 1447–1454. https://doi.org/10.1080/02640410802209018
Korhonen, M. T., Mero, A. A., Alen, M., Sipila, S., Hakkinen, K., Liikavainio, T., Viitasalo, J. T., Haverinen, M. T., & Suominen, H. (2009). Biomechanical and skeletal muscle determinants of maximum running speed with aging. Medicine & Science in Sports & Exercise, 41, 844–856. https://doi.org/10.1249/MSS.0b013e3181998366
Matheson, G. O., Macintyre, J. G., Taunton, J. E., Clement, D. B., & Lloyd-Smith, R. (1989). Musculoskeletal injuries associated with physical activity in older adults. Medicine & Science in Sports & Exercise, 21, 379–385.
Pollock, M. L., Carroll, J. F., Graves, J. E., Leggett, S. H., Braith, R. W., Limacher, M., & Hagberg, J. M. (1991). Injuries and adherence to walk/jog and resistance training programs in the elderly. Medicine & Science in Sports & Exercise, 23, 1194–1200.
Fukuchi, R. K., Stefanyshyn, D. J., Stirling, L., Duarte, M., & Ferber, R. (2014). Flexibility, muscle strength and running biomechanical adaptations in older runners. Clinical Biomechanics (Bristol, Avon), 29, 304–310. https://doi.org/10.1016/j.clinbiomech.2013.12.007
DeVita, P., & Hortobagyi, T. (2000). Age causes a redistribution of joint torques and powers during gait. Journal of Applied Physiology, 88, 1804–1811. https://doi.org/10.1152/jappl.2000.88.5.1804
Giarmatzis, G., Jonkers, I., Baggen, R., & Verschueren, S. (2017). Less hip joint loading only during running rather than walking in elderly compared to young adults. Gait & Posture, 53, 155–161. https://doi.org/10.1016/j.gaitpost.2017.01.020
Jin, L., & Hahn, M. E. (2019). Comparison of lower extremity joint mechanics between healthy active young and middle age people in walking and running gait. Scientific Reports, 9, 5568. https://doi.org/10.1038/s41598-019-41750-9
Kline, P. W., & Williams, D. S., 3rd. (2015). Effects of normal aging on lower extremity loading and coordination during running in males and females. International Journal of Sports Physical Therapy, 10, 901–909.
Cheung, R. T. H., Zhang, J. H., Chan, Z. Y. S., An, W. W., Au, I. P. H., MacPhail, A., & Davis, I. S. (2019). Shoe-mounted accelerometers should be used with caution in gait retraining. Scandinavian Journal of Medicine & Science in Sports, 29, 835–842. https://doi.org/10.1111/sms.13396
Hennig, E. M., & Lafortune, M. A. (1991). Relationships between ground reaction force and tibial bone acceleration parameters. Journal of Applied Biomechanics, 7, 303–309.
Ryu, S., Lee, Y. S., & Park, S. K. (2021). Impact signal differences dependent on the position of accelerometer attachment and the correlation with the ground reaction force during running. International Journal of Precision Engineering and Manufacturing, 22, 1791–1798. https://doi.org/10.1007/s12541-021-00483-4
Sheerin, K. R., Reid, D., & Besier, T. F. (2019). The measurement of tibial acceleration in runners-A review of the factors that can affect tibial acceleration during running and evidence-based guidelines for its use. Gait & Posture, 67, 12–24. https://doi.org/10.1016/j.gaitpost.2018.09.017
Kavanagh, J. J., Barrett, R. S., & Morrison, S. (2004). Upper body accelerations during walking in healthy young and elderly men. Gait & Posture, 20, 291–298. https://doi.org/10.1016/j.gaitpost.2003.10.004
Van Emmerik, R. E., McDermott, W. J., Haddad, J. M., & Van Wegen, E. E. (2005). Age-related changes in upper body adaptation to walking speed in human locomotion. Gait & Posture, 22, 233–239. https://doi.org/10.1016/j.gaitpost.2004.09.006
Mazza, C., Iosa, M., Pecoraro, F., & Cappozzo, A. (2008). Control of the upper body accelerations in young and elderly women during level walking. Journal of NeuroEngineering and Rehabilitation, 5, 30. https://doi.org/10.1186/1743-0003-5-30
Napier, C., Fridman, L., Blazey, P., Tran, N., Michie, T. V., & Schneeberg, A. (2022). Differences in peak impact accelerations among foot strike patterns in recreational runners. Front Sports Act Living, 4, 802019. https://doi.org/10.3389/fspor.2022.802019
Reenalda, J., Maartens, E., Buurke, J. H., & Gruber, A. H. (2019). Kinematics and shock attenuation during a prolonged run on the athletic track as measured with inertial magnetic measurement units. Gait & Posture, 68, 155–160. https://doi.org/10.1016/j.gaitpost.2018.11.020
Hunter, J. G., Smith, A. M. B., Sciarratta, L. M., Suydam, S., Shim, J. K., & Miller, R. H. (2020). Standardized lab shoes do not decrease loading rate variability in recreational runners. Journal of Applied Biomechanics. https://doi.org/10.1123/jab.2019-0337
Lafortune, M. A. (1991). Three-dimensional acceleration of the tibia during walking and running. Journal of Biomechanics, 24, 877–886. https://doi.org/10.1016/0021-9290(91)90166-k
Wei, Q., Wang, Z., Woo, J., Liebenberg, J., Park, S. K., Ryu, J., & Lam, W. K. (2018). Kinetics and perception of basketball landing in various heights and footwear cushioning. PLoS ONE, 13, e0201758. https://doi.org/10.1371/journal.pone.0201758
Fazio, P., Granieri, G., Casetta, I., Cesnik, E., Mazzacane, S., Caliandro, P., Pedrielli, F., & Granieri, E. (2013). Gait measures with a triaxial accelerometer among patients with neurological impairment. Neurological Sciences, 34, 435–440. https://doi.org/10.1007/s10072-012-1017-x
Park, S. K., Jeon, H. M., Lam, W. K., Stefanyshyn, D., & Ryu, J. (2019). The effects of downhill slope on kinematics and kinetics of the lower extremity joints during running. Gait & Posture, 68, 181–186. https://doi.org/10.1016/j.gaitpost.2018.11.007
Giandolini, M., Poupard, T., Gimenez, P., Horvais, N., Millet, G. Y., Morin, J. B., & Samozino, P. (2014). A simple field method to identify foot strike pattern during running. Journal of Biomechanics, 47, 1588–1593. https://doi.org/10.1016/j.jbiomech.2014.03.002
Purcell, B., Peter Channells, J., James, D., & Barrett, R. (2006). Use of accelerometers for detecting foot-ground contact time during running. In Proceedings of proceedings of SPIE—The international society for optical engineering.
Dufek, J. S., Mercer, J. A., Teramoto, K., Mangus, B. C., & Freedman, J. A. (2008). Impact attenuation and variability during running in females: A lifespan investigation. Journal of Sport Rehabilitation, 17, 230–242.
Sinclair, J. (2016). Sex differences in shock attenuation during running. Central European Journal of Sport Sciences and Medicine, 15, 37–42.
Chambon, N., Sevrez, V., Ly, Q. H., Gueguen, N., Berton, E., & Rao, G. (2014). Aging of running shoes and its effect on mechanical and biomechanical variables: Implications for runners. Journal of Sports Sciences, 32, 1013–1022. https://doi.org/10.1080/02640414.2014.886127
Creaby, M. W., & Franettovich Smith, M. M. (2016). Retraining running gait to reduce tibial loads with clinician or accelerometry guided feedback. Journal of Science and Medicine in Sport, 19, 288–292. https://doi.org/10.1016/j.jsams.2015.05.003
Sheerin, K. R., Besier, T. F., Reid, D., & Hume, P. A. (2018). The one-week and six-month reliability and variability of three-dimensional tibial acceleration in runners. Sports Biomechanics, 17, 531–540. https://doi.org/10.1080/14763141.2017.1371214
Wood, C. M., & Kipp, K. (2014). Use of audio biofeedback to reduce tibial impact accelerations during running. Journal of Biomechanics, 47, 1739–1741. https://doi.org/10.1016/j.jbiomech.2014.03.008
Greenhalgh, A., Sinclair, J., Protheroe, L., & Chockalingam, N. (2012). Predicting impact shock magnitude: which ground reaction force variable should we use? International Journal of Sports Science and Engineering, 6, 225–231.
Larsson, L., Grimby, G., & Karlsson, J. (1979). Muscle strength and speed of movement in relation to age and muscle morphology. Journal of Applied Physiology: Respiratory, Environmental and Exercise Physiology, 46, 451–456. https://doi.org/10.1152/jappl.1979.46.3.451
Riggs, B. L., & Melton, L. J., 3rd. (1986). Involutional osteoporosis. The New England Journal of Medicine, 314, 1676–1686. https://doi.org/10.1056/NEJM198606263142605
Vandervoort, A. A., & McComas, A. J. (1986). Contractile changes in opposing muscles of the human ankle joint with aging. Journal of Applied Physiology, 61, 361–367. https://doi.org/10.1152/jappl.1986.61.1.361
Menz, H. B., Lord, S. R., & Fitzpatrick, R. C. (2003). Acceleration patterns of the head and pelvis when walking on level and irregular surfaces. Gait & Posture, 18, 35–46. https://doi.org/10.1016/s0966-6362(02)00159-5
Winter, D. A. (1995). Human balance and posture control during standing and walking. Gait & Posture, 3, 193–214.
Saunders, J. B., Inman, V. T., & Eberhart, H. D. (1953). The major determinants in normal and pathological gait. The Journal of Bone and Joint Surgery, 35-A, 543–558.
Derrick, T. R., Hamill, J., & Caldwell, G. E. (1998). Energy absorption of impacts during running at various stride lengths. Medicine & Science in Sports & Exercise, 30, 128–135. https://doi.org/10.1097/00005768-199801000-00018
Edwards, W. B., Derrick, T. R., & Hamill, J. (2012). Musculoskeletal attenuation of impact shock in response to knee angle manipulation. Journal of Applied Biomechanics, 28, 502–510. https://doi.org/10.1123/jab.28.5.502
McMahon, T. A., Valiant, G., & Frederick, E. C. (1987). Groucho running. Journal of Applied Physiology, 62, 2326–2337. https://doi.org/10.1152/jappl.1987.62.6.2326
Judge, J. O., Davis, R. B., 3rd., & Ounpuu, S. (1996). Step length reductions in advanced age: The role of ankle and hip kinetics. The Journals of Gerontology, Series A: Biological Sciences and Medical Sciences, 51, M303-312. https://doi.org/10.1093/gerona/51a.6.m303
Silder, A., Heiderscheit, B., & Thelen, D. G. (2008). Active and passive contributions to joint kinetics during walking in older adults. Journal of Biomechanics, 41, 1520–1527. https://doi.org/10.1016/j.jbiomech.2008.02.016
Kim, W., Voloshin, A. S., Johnson, S. H., & Simkin, A. (1993). Measurement of the impulsive bone motion by skin-mounted accelerometers. Journal of Biomechanical Engineering, 115, 47–52. https://doi.org/10.1115/1.2895470
Malm, M., Samman, M., & Serup, J. (1995). In vivo skin elasticity of 22 anatomical sites: The vertical gradient of skin extensibility and implications in gravitational aging. Skin Research and Technology, 1, 61–67. https://doi.org/10.1111/j.1600-0846.1995.tb00019.x
Forner-Cordero, A., Mateu-Arce, M., Forner-Cordero, I., Alcantara, E., Moreno, J. C., & Pons, J. L. (2008). Study of the motion artefacts of skin-mounted inertial sensors under different attachment conditions. Physiological Measurement, 29, N21-31. https://doi.org/10.1088/0967-3334/29/4/N01
Saha, S., & Lakes, R. S. (1977). The effect of soft tissue on wave-propagation and vibration tests for determining the in vivo properties of bone. Journal of Biomechanics, 10, 393–401. https://doi.org/10.1016/0021-9290(77)90015-x
Lafortune, M. A., & Hennig, E. M. (1991). Contribution of angular motion and gravity to tibial acceleration. Medicine & Science in Sports & Exercise, 23, 360–363.
Acknowledgements
This study was supported by the National Research Foundation of Korea (NRF) grant funded by Korea government (MSIT) (Grant number: 2019RIF1A1061371) and Fila Holdings (Seoul, Korea). We thank Junghyun Woo, Msc, for data collection and analysis and Donna Mae Humber for her professional editing for the manuscript.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Park, SK., Stefanyshyn, D., Ryu, S. et al. Comparisons of Age-Related Changes in Impact Characteristics Between Healthy Older and Younger Runners. Int. J. Precis. Eng. Manuf. 23, 1465–1476 (2022). https://doi.org/10.1007/s12541-022-00720-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12541-022-00720-4