
Abstract
Background
Smartphone-based interventions are a potentially effective way to minimize alcohol-related harm in young adult, non-dependent drinkers. This pilot study is the first to evaluate the benefits and feasibility of a personalized alcohol harm-minimization intervention delivered via smartphones.
Methods
Within a single-blind, randomized controlled design, 45 young adults were randomly assigned to either the intervention app (n = 25; 18 females; Mage = 21.36 years, SDage = 4.15 years) or the control app (n = 20; 18 females; Mage = 22.75; SDage = 4.41). The two primary outcomes were frequency of risky drinking and drinking-related harms, and the secondary outcome was frequency of protective behavioral strategies (PBS) use. All outcomes were measured at baseline and immediately post-intervention. Using the Enlight framework [1], usability was evaluated via structured one-on-one phone interviews with a subgroup of six participants from the intervention group (3 females; Mage = 19.5 years, SDage = 1.64).
Results
There was no significant reduction in the primary outcomes from baseline to post-intervention across the groups. For the secondary outcome, the application of PBS within drinking contexts increased at follow-up for those in the intervention group but not for control participants. End-users rated the app as highly usable but had some concerns with repetition of the app-recommended strategies.
Conclusions
This intervention, designed to reduce risky drinking behaviors among young adults, was rated as highly usable and was shown to increase the application of harm minimization strategies within drinking contexts. While the intervention and its delivery show promise, it did not appear to mitigate risky drinking behaviors. Implications of this research and future directions are discussed.
Trial Registration
This trial is registered at the Australian New Zealand Clinical Trials Registry: BLINDED.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Overview
Traditionally, alcohol reduction interventions available to young adults include motivational interviewing (MI) or cognitive behavioral therapy (CBT), which aim to modify cognitions regarding alcohol use and are delivered by a therapist in a health care service setting (e.g., [2]). However, as the findings from recent ecological momentary assessment (EMA) studies show, the strongest predictors of young adults’ drinking behaviors are not stable factors (i.e., dispositional drinking motivations), but rather dynamic factors within the drinking context (i.e., social interpersonal factors) [3, 4]. Given that these risk factors occur within the drinking context (rather than just within the person), intervention is required that extends beyond the standard treatment context (e.g., therapist office) and offers real-time support during the moments when the risk factors are present. A further limiting feature of these traditional forms of alcohol interventions is that the young person is required to initiate professional help in primary and secondary health care settings. Young people experiencing drinking-related problems underutilize professional treatment for a variety of reasons (e.g., shame, financial reasons, geographical barriers) (e.g., [5, 6]). Finding useful, accessible, and confidential ways to reduce risky drinking among young people remains a key research and health priority.
This pilot study reports on the evaluation of a smartphone-delivered intervention that targets situation-specific risk factors which are known to precipitate young adults’ risky drinking. The evaluation of the intervention occurred in two parts as per guidelines described by the Medical Research Council [7]; (1) using a randomized controlled design, the preliminary findings of the intervention were examined, and (2) employing a qualitative study design, the usability and acceptability of the intervention were evaluated.
Protective Behavioral Strategies
One approach that has shown promise when used as part of a multicomponent alcohol reduction intervention is protective behavioral strategies (PBS)—simple behavioral techniques designed to reduce drinking and/or drinking-associated harm such as drink driving [8]. PBS [8] may be separated into three subtypes: stopping or limiting consumption (e.g., setting drinking limits), changing the manner of drinking (e.g., avoiding drinking games, drinking beer instead of spirits), and avoiding serious hazards associated with drinking (e.g., organizing a designated driver).
Evidence for Protective Behavioral Strategies
Cross-sectional evidence suggests that individuals who participate in interventions employing PBS as well as other components (e.g., personalized feedback regarding drinking levels, information on drinking consequences) are less inclined to drink in a risky manner [9, 10]. For example, a recent study [11] found that participants who were provided with a multicomponent brief intervention that included personalized feedback, enhancement of motivation, goal development, and PBS meaningfully reduced the number of heavy drinking days (in the prior 30 days), 3 months after the intervention (M = 2.56 heavy drinking days, SD = 3.26) as compared to baseline (M = 3.05 heavy drinking, SD = 4.05). Focused evaluations of PBS have also shown it to be an effective mediator within multicomponent interventions (e.g., [12, 13]).
Despite PBS showing promise within multicomponent intervention contexts, when delivered as a stand-alone intervention (without other intervention components), it is not shown as effective [14, 15]. For example, a recent study [14] found that 1 month post-intervention, participants who had received the PBS intervention showed no meaningful difference in the maximum number of drinks they had consumed on a single occasion in the prior 30 days (M = 7.25 number of drinks, SD = 3.93) compared to a control group (M = 7.91 number of drinks, SD = 4.09).
Two reasons may account for these weak findings regarding the application of PBS as a stand-alone intervention. First, a single delivery of PBS at one point in time is unlikely to be sufficient to facilitate sustained change in an individual’s drinking habits. Rather, repetition and consistent reminders of these strategies may better facilitate behavior change [16, 17]. Second, these psychoeducational interventions did not tailor the provision of PBS to the individual’s drinking context, their momentary affective state, or the types of drinking-based goals they wanted to achieve (e.g., reduction in consumption or drinking-related consequences).
Factors to Inform Drinking Interventions
Recent EMA studies [3, 4] have shown momentary affect and social interpersonal factors within the drinking context as significant determinants of young adults’ drinking behaviors. Dvorak and colleagues found daily negative affect predictive of subsequent heavy drinking, whereas daily positive affect was predictive of drinking-related harm. Thus, whether the valence of affect is negative or positive may have important implications for either heavy drinking or drinking-related harm. In terms of the social interpersonal context, Kuntsche and colleagues found young adults who experienced social situations marked by interactions with same-sex friends at drinking establishments, as more likely to drink in a risky manner, compared to when they were not exposed to these types of situations. Finally, health behavior change interventions are enhanced with the inclusion of goal-setting. Indeed, there is a significant body of research that supports the applicability and utility of goal-setting within alcohol behavior changes [18, 19]. As such, implementation of PBS interventions should be sufficiently flexible to tailor messages and strategies to individuals’ momentary affect, social drinking context, and drinking-related goal.
Ecological Momentary Intervention
Ecological momentary intervention (EMI) is defined as a method to intervene upon behavior in the moment [20] via a mobile device. EMI enables the delivery of a PBS-based intervention tailored to individuals’ affective state, social context, and drinking-related goal. This in-the-moment modality offers many technological advantages over traditional intervention formats (e.g., therapist delivered), including the following: (a) EMIs can use EMA data to provide support that is personalized and tailored to the individual’s context [21], and (b) using “decision rules,” EMI can deliver information in a timely manner close to the target behavior (e.g., [22]), which is more effective than delayed interventions (e.g., [23]). Furthermore, smartphone apps appear to overcome several help-seeking barriers to treatment, including enhanced accessibility, affordability, and anonymity [24, 25]. Due to these advantages, there has been a surge in the number of interventions delivered via smartphone apps for both non-dependent drinkers [26] and dependent drinkers [27]. Specifically relevant to this study, a number of smartphone apps have been developed which incorporate harm minimization strategies (e.g., protective strategies) to support persons to drink in a safe manner [28, 29]. To illustrate, consider Telecoach, a smartphone app which included self-monitoring of alcohol use followed immediately by harm-minimization strategies [30]. Compared to a waitlist group, alcohol frequency was significantly reduced at follow-up. This suggests that the dissemination of protective strategies immediately following self-monitoring could generate a reduction in drinking frequency.
Current Study
The EMI framework provides several strengths in delivering alcohol reduction interventions, making it a popular intervention modality. Though as yet, an EMI that delivers PBS that are tailored to an individual’s goals and drinking context, in the moment, has not been trialed. To address this, Minimise was developed by our research team to deliver a range of PBS over a sustained period of time (28 days), tailored to the user’s drinking goal (i.e., reduce alcohol and/or drinking-related consequences), their momentary affective state (i.e., negative or positive), and their social, interpersonal context (i.e., who they are with). The first part of this pilot study (part one) is to assess the benefit of this intervention. The specific research questions (RQs) of this component of the study include the following.
RQ1
To what extent do individuals who receive Minimise report a reduction in the two primary outcomes of frequency of risky single occasion drinking (RSOD, five or more standard drinks consumed in a single setting) and alcohol-related harms (e.g., interpersonal disputes) compared to individuals in the control group?
RQ2
To what extent do individuals who receive the Minimise app exhibit an increase in the secondary outcome of frequency of PBS use in comparison to those in the control group?
The second aim of this study (part two) is to explore the usability and acceptability of the Minimise application. The objectives of this component of the study are to determine the following.
RQ3
To what extent do users of Minimise perceive the app as a usable device to facilitate reductions in risky drinking behaviors?
RQ4
To what extent do users of Minimise perceive the app as an acceptable device to reduce risky drinking behaviors?
Part One: Preliminary Findings
Method
Design
To examine preliminary findings of Minimise (RQ1 and RQ2), a single-blind, randomized controlled design was performed using a two-arm parallel sequence in which the primary outcomes (drinking behaviors) and secondary outcomes (PBS use) were measured at baseline and immediately post the intervention. This study was approved by the authors’ Ethics Committee board, and all procedures were in accordance with the National Health and Medical Research Council [7]. Refer to Electronic Supplementary Material 1.5 for Consolidated Standards of Reporting Trials Checklist.
Randomization and Blinding
Following screening and completion of the baseline questionnaire, eligible participants were randomly assigned to the intervention or control group using a pre-determined computerized sequence by Qualtrics (www.qualtrics.com). At the end of the baseline questionnaire, the presentation of the app-download instructions was randomized, alternating between how to download the self-monitoring InstantSurvey smartphone app [31] or the intervention Minimise app. Participants were fully blinded as to which group they were assigned to (i.e., they did not know which app corresponded to the intervention or control group). Once participants had completed the follow-up assessment (immediately post the intervention period), they were informed as to which group they were in and debriefed. Those in the control group were offered the intervention app (Minimise) after the debrief.
Study Population
Participants were recruited via invitations on social media (e.g., Facebook), and from advertisements placed within a large metropolitan university campus. Participants were eligible for the trial if they answered yes to the following criteria in the baseline survey: (a) aged 18–35 years, (b) access to an iPhone, (c) reported being motivated to reduce alcohol use, and (d) consume alcohol, on average, at least once a week.
Participants
Intervention
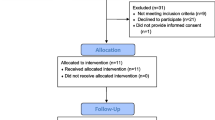
A total of 25 individuals aged between 18 and 35 years (18 females; Mage = 21.36 years, SDage = 4.15 years) completed the baseline assessment and were randomized to download the Minimise app (see Fig. 1). After downloading the app, three participants were lost to follow-up. This reduced the sample of participants who completed all phases of the intervention study (i.e., baseline and follow-up) to 22.

The CONSORT depicting participant flow
Control
A total of 20 individuals aged between 18 and 32 years (18 females; Mage = 22.75; SDage = 4.41) completed the baseline assessment and were randomized to download the InstantSurvey app (see Fig. 1). After downloading the app, four participants were lost to follow-up. This reduced the sample of participants who completed all phases of the control study (i.e., baseline and follow-up) to 16.
The Applications
Intervention App
Minimise is a smartphone app developed by the authors and delivered via a native platform. The app delivers PBS tailored to the users’ goals and drinking context. On first use, the user needs to input their personally developed ID from the app and into the online survey portal (this allows the researchers to associate the users’ baseline information with their app information). Minimise will then ask the user which goals they want to achieve from the app: (a) reduce the amount of alcohol they consume and/or (b) reduce their experience of adverse drinking-related consequences (see Electronic Supplementary Material 1.1, Fig. 1). Once the goals are selected, this information is stored in the app and informs the algorithm of PBS delivery (detailed below). Following this, the user receives two notifications per day, once at 11:00 a.m. and again at 8:00 p.m., for 28 consecutive days. These notifications ask the user to complete a short self-monitoring survey which examines (a) drinking behaviors: current drinking intention (i.e., do you intend to drink today?), if alcohol had been consumed since the last assessment and if so how much (on a 1–10 scale), and if the user has experienced adverse drinking-related consequences (i.e., work/study, unwell, interpersonal difficulties); (b) drinking context: social interpersonal context (i.e., are you with other people or alone?), positive affect (i.e., do you feel happy?), and negative affect (i.e., do you feel stressed?); and (c) PBS use for alcohol consumption (i.e., did you use a strategy to manage your alcohol use?) and drinking-related harm (i.e., did you use a strategy to manage drinking-related harm?)
During this short self-monitoring survey, if the user indicates that they are drinking or that they intend to drink, they immediately receive a message alerting them to “please review your strategies”, which is located under the “strategies” tab within the app (see Electronic Supplementary Material 1.1, Fig. 2). Three strategies are delivered within the app and tailored to the users’ (i) goals (i.e., to reduce alcohol use and/or alcohol harm), (ii) current affect (i.e., positive or negative affect), and (iii) social context (i.e., alone or with other people; refer to Electronic Supplementary Material 1.3 to view algorithm in detail). While Minimise includes a total of 21 different PBS built into the app, only three PBS were delivered per drinking event. Of the 21 strategies embedded within Minimise, 11 were derived from the PBS Scale [8], while 10 strategies were developed for this study (Electronic Supplementary Material 1.3). In addition, Minimise allows the user to review their drinking statistics at any time (including percentage of days of PBS use, percentage of days of risky drinking; refer to Electronic Supplementary Material 1.1, Fig. 3).
Control App
InstantSurvey is a smartphone app developed by the authors and delivered via a native platform. On first use, the user needs to input their personally developed ID from the app and into the online survey portal (this allows the researchers to associate the users’ baseline information with their app information). The smartphone application will thereafter comprise alcohol self-monitoring functions (see Electronic Supplementary Material 1.2 for screenshots of these functions). Similar to Minimise, the app delivers two messages per day, once at 11:00 a.m. and again at 8:00 p.m., for 28 consecutive days. This message asks the user to complete a short self-monitoring survey which examines similar items as the Minimise app (i.e., drinking behaviors and drinking context). The InstantSurvey app does not provide any information regarding PBS, has no feedback to the user, and does not allow the user to review their data. Rather, the app was simply comprised the self-monitoring assessments.
Measures
Using an online survey, the following was assessed at baseline: basic demographics (i.e., age and gender), the Alcohol Use Disorders Identification Test (AUDIT), and primary and secondary outcomes. Immediately post the intervention, the primary and secondary outcomes were reassessed.
The AUDIT was used to identify the level of drinking-related problems exhibited by the sample at baseline [32]. The AUDIT is a 10-item questionnaire that examines consumption, dependence, and drinking-related problems (α = 0.79). Items 1 to 8 are scored on a 5-point rating scale (0 = never, 5 = daily), and questions 9 to 10 are scored on a 3-point rating scale (0 = no, 2 = yes, in the past year). Research indicates that AUDIT scores from 8 to 15 represent a moderate level of risky drinking, with scores above 15 being representative of more problematic use [33].
Primary Outcome
To assess the primary outcomes—frequency of RSOD and drinking-related harm—the following questions were asked: “over the past two weeks how many times did you (a) consume more than four Australian standard drinks (ASDs; 10 g ethanol), (b) experience difficulties with work and/or study due to your drinking (RSOD), (c) experience interpersonal difficulties due to your drinking, and (d) felt physically unwell due to your drinking?” Items were scored on a 4-point rating scale (0 = never, 1 = 1–2 times, 2 = 3–4 times, 3 = more than 4 times). The items and scales were developed for this study.
Secondary Outcome
To assess the secondary outcomes regarding the frequency of applying PBS, participants were asked, “over the past two weeks how many times did you (a) use a PBS to control the amount of alcohol you drank (PBS alcohol) and (b) use a PBS to reduce harm when drinking (PBS harm)?”. Items were scored on a 4-point rating scale (0 = never, 1 = 1–2 times, 2 = 3–4 times, 3 = more than 4 times).
Results
Data Analytic Procedure
For the preliminary analyses, independent sample t tests were employed to determine if there were differences in the baseline characteristics of age and AUDIT total score and a Pearson’s chi-square was used to assess if there were differences in the gender proportions between the groups (i.e., intervention and control). For the main analysis, mixed-effect models were used to assess the influence of time, group, and interaction of time by group on the primary and secondary outcomes. In each model, intercept and time were included as random effects and group was modeled as a fixed effect. Furthermore, a Poisson distribution was assumed in these mixed models given that the outcomes were measured as count variables (e.g., frequency of risky drinking in the prior 2 weeks).
Missing values were evident at follow-up for both the primary and secondary outcome variables (see Electronic Supplementary Material 1.4 for more information). Little’s Missing Completely at Random test revealed that the data across each of the outcomes were missing completely at random; X2 (2, N = 45) = 6.09, p = .99. Therefore, all available data were used in the main analyses using full-information maximum likelihood estimation. Analyses were performed using Mplus [34].
Adherence Statistics
Adherence with the app was calculated as the percentage of days the individual was engaged with the app, out of the possible 28. For the intervention group, a total of 25 participants responded to 953 prompts, out of a possible 1400 prompts (68%) across 552 days (out of a possible 700). On average, participants in the intervention group engaged with the app on 22.08 days (SD = 9.70) out of a possible 28, giving an adherence rate of 79%. Participants in the intervention group provided close to two reports per day (M = 1.72; SD = 0.63) out of two. Preliminary analyses were conducted to evaluate whether adherence (i.e., total number of days responded to the app) was influenced by age and gender, and whether adherence was associated with a difference in outcomes at follow-up. The results found adherence to the Minimise app was unrelated to age (r = .20, p = .40) and gender (r = .24, p = .30). Furthermore, adherence to Minimise was not significantly related to changes in any of the outcomes at follow-up (RSOD, r = .14, p = .56; work difficulties, r = − .12, p = .61; interpersonal, r = − .25, p = .28; unwell, r = .01, p = .96; PBS alcohol use, r = .02, p = .94; and PBS harm, r = −.16, p = .48). This suggests that there was no difference in outcomes at follow-up for those who engaged in Minimise more so than others.
The 20 participants in the control group responded to 906 prompts (out of a possible 1120; 81%), across 442 days of self-monitoring (out of 560). On average, participants in the control group reported a response on 22.1 days out of 28 (SD = 8.55), giving an adherence rate of 79%. Participants in the control group were providing close to two self-reports each day (M = 1.96, SD = 0.50) out of two. In terms of the relationship between adherence and demographics, the findings revealed that adherence was not significantly related to gender (r = .37, p = .17), though it was negatively correlated with age (r = − .56, p = .03), suggesting that older participants engaged with the app less than younger participants. Furthermore, results found that adherence to InstantSurvey was negatively correlated with changes at follow-up in the outcome of being unwell due to drinking (r = − .57 p = .03) and the frequency of PBS use for alcohol consumption (r = − .56 p = .03). There was no significant association between adherence and change in the other outcomes at follow-up (RSOD, r = − .29, p = .29; work difficulties, r = − .31, p = .26; interpersonal, r = − .03, p = .91; PBS harm, r = − .32, p = .25).
Preliminary Analysis
Preliminary analyses were conducted to evaluate if there were significant differences observed across the groups for the baseline characteristics including age, gender, AUDIT total score, origin of birth, and occupation (as shown in Table 1). There were no significant differences between the groups for these demographic and alcohol-related measures.
Main Analysis
Mean Differences Between Group and Time for Primary and Secondary Outcomes
Sample means for the primary (i.e., RSOD and drinking-related harm) and secondary outcomes (i.e., PBS use for alcohol consumption and harm) at baseline and follow-up, across the groups (intervention and control), are presented in Table 2. There were no significant differences at baseline in the primary or secondary outcomes across the intervention or control, suggesting that at baseline, the groups were similar to each other. At follow-up, there was no significant change in the primary outcomes across the groups, whereas, for the secondary outcomes, participants in the intervention group were shown to endorse PBS for alcohol use (M = 1.61, SD = .17) and harm (M = 1.47, SD = .22) significantly more than those in the control group (M = 1.07, SD = .20; M = 0.63, SD = .25, respectively) at follow-up.
Group by Time Main and Interaction Effects
The main and interaction effects of time and group upon the primary and secondary outcomes are evident in Table 3. There was no significant main or interaction effect of time or group upon the primary outcomes. There was a significant interaction of time by group in predicting changes in the secondary outcomes of PBS use for alcohol consumption (B = .52, p = .03), and PBS use for alcohol-related harm (B = .82, p = .03). The proportion of variance explained by the group*time interaction was small across the measured outcomes (i.e., from 1 to 3%). Please refer to the graphical representation of these interactions in Electronic Supplementary Material 1.6 for more information.
Part Two: Usability and Acceptability
Method
Participants
Participants were selected based on obtaining a sample with an equal proportion of males and females and matched approximately for the mean age of the larger sample. The sample included three male and three female participants (Mage = 19.5 years, SDage = 1.64 years) from the intervention group. Formative usability trials have demonstrated that a sample of five participants can identify 80% of usability issues [35, 36].
Measures
Usability was assessed from the System Usability Scale (SUS) [37], and acceptability was examined through an interview schedule based on the Enlight measure [1].
System Usability Scale
The SUS [34] is an industry-standard 10-item scale (e.g., [38]) that examines the usability of a technological tool. Responses are measured on a 5-point Likert-type scale with 1 (strongly disagree) to 5 (strongly agree). The SUS yields a composite score between 0 and 100, with higher scores indicating higher perceptions of usability. A SUS score greater than 68 is considered “above average” and consistent with satisfactory usability (e.g., [39]). The SUS has been found as a reliable and valid tool among both experts and service users when assessing the usability of smartphone applications [40].
Enlight
A total of 10 open-ended questions were taken from the Enlight evaluation tool [1] and posed to participants during a one-on-one phone interview. These questions were designed to gain an in-depth understanding into the acceptability and usability of the app. Example questions include “to what extent is the app an appropriate tool to use in reducing alcohol use?” and “how easy was it to learn to use the app?”
Procedure
At the end of the intervention period, a subgroup of six participants engaged in a one-on-one phone interview with a trained research assistant who presented the following questions: basic demographics, the System Usability Scale, (SUS), and open-ended questions adapted from the Enlight categories. The mean length of the interview was 35 min (SD = 9.46).
Results
Thematic Analysis Procedure
Thematic analysis was used to identify the recurring themes from the qualitative data, as outlined by Braun and Clarke [41]. All audio recordings were transcribed verbatim and systematically double-coded independently among two researchers (RO, PS). Following an in-depth review of the coded data, independent themes were developed based on recurrent content. Both coders (RO, PS) then engaged in a cooperative discussion of themes to decide on the most pertinent and recurrent aspects of coded data. The process of refining and reviewing themes was iterative until themes were representative of the data and saturation was achieved.
Usability
Quantitative usability data indicated high usability scores among the participants with the average overall score of 74.16 (SD = 9.31), exceeding the acceptable cut-off score of 68 [42]. As shown in Table 4, participants felt that most people would be able to learn to use the app quickly and that they themselves felt confident using the app.
Acceptability
The semi-structured interviews were informed by the Enlight evaluation framework [1]. Ten open-ended questions regarding acceptability, experiences of use, and challenges of utilizing the app were asked to a subgroup of participants. Thematic analysis revealed seven broad themes which are described below: four themes were related to the advantages of the app and three related to the challenges.
Perceived Advantages of Minimise
Tailored Delivery of Protective Strategies
All participants commented that the tailored delivery of the protective strategies was useful in providing specific alcohol reduction information, relevant to their context. Indeed, users felt that receiving information, matched to their context, enabled the application of the strategies into their drinking context as they were applicable:
“There were different strategies for different scenarios so there was good advice for each environment which was easy to incorporate”
[Participant 3]
The majority of participants appreciated being prompted to use these specific strategies in the drinking context (N = 5/6). Specifically, users reported that without the prompting reminder it would be difficult to remember to implement the strategies:
“I liked the strategies the most, using those and when it prompted you if you have intentions to drink…if I wasn’t prompted I probably would’ve forgotten” [Participant 5]
Habit Formation
The users commented on how the app check-in process had become habitual. Specifically, four of the six participants experienced Minimise as part of their daily routine stating that it had become routine to check in with the app when they were also engaging with other apps (i.e., social media):
“It’s become part of my app checking habit” [Participant 3]
Some participants referred to the app as having gamification elements that they felt were fun and enjoyable to complete, which provided a short distraction from reality (N = 3/6). This further assisted the habit-formation of checking in with the Minimise app:
“It’s like having a game of bejewelled—it gives you two minutes of mindfulness”
[Participant 2]
Increased Awareness of Drinking
A prominent finding identified among all participants was that the app increased awareness in the user in two ways: first, it helped the user identify how much they were drinking, and second, there was insight into the circumstances preceding their decision to drink.
“It made me realise that I drink more than I realised and I only drink because I am with friends. I didn’t realise that before” [Participant 5]
Three participants commented that this self-awareness was particularly effective in prompting behavioral change in regard to their alcohol consumption and would have a lasting impact on their future drinking behaviors:
“Quantity wise it’s definitely going to decrease—I knew that my tolerance level was a bit low, but I used to drink anyway but now I start to see the direct effect on my health and wellbeing.”
[Participant 3]
Insight Into Current Emotional State
While it was not an intention of Minimise, four out of the six participants reported that the app had helped them to reflect on their emotions, which in turn helped to inform their decision regarding alcohol use:
“Sometimes you just don’t feel like drinking, you might be sad, but it is a mate's birthday, so you have to or a social situation where you have to. So, all those questions [in the app] helped me make the right decision.” [Participant 2]
Another user commented that the ability to monitor their emotional state helped them to understand why they were drinking:
“When I was filling in the emotions part of it every single day it made me go through a process of self-realisation - you don't often acknowledge why you drink.” [Participant 3]
Perceived Challenges of Using Minimise
Technical Issues
There were two technical issues identified by three out of six participants. First, the notification schedule was inconsistent:
“Sometimes I wouldn’t even get the notification, so I then had to open the app” [Participant 3]
Second, the slider used in the self-reports was temperamental for some items:
“Sometimes when I used to move the scale it used to get stuck. It would say this question is unanswered, but I did answer it. That used to get really annoying” [Participant 6]
These types of errors impeded upon a small number of participants’ (N = 2/6) motivation to use the app:
“The app was starting to glitch out a heap of times and I was getting really annoyed by that. I was contemplating quitting the study as I was getting sick of it”
[Participant 1]
The Strategies Were Not Unique
The main concern users had with the delivery of the PBS was that they were familiar with some of the strategies recommended within the app, and for some users (N = 3/6), this lack of novelty reduced their engagement in the app:
“I have gone in and looked at my protective strategies a few times but a lot of them I have heard about from friends and school and so I haven’t looked over them too much” [Participant 4]
Most participants (N = 4 out of 6) relied on the PBS that were novel and more specific to their situation rather than the familiar and more obvious suggestions:
“In terms of the general strategies provided like covering your drink or having a designated driver—they weren’t very specific so it wasn't that applicable”
[Participant 3]
The Lack of Certain Functions
The large proportion of users (N = 5/6) commented that they would have liked more functionality surrounding the ability to track progress while using the app. Users emphasized that if they were able to see how many drinks they were consuming on a frequent basis, and how this aligned with their goals, this would have better facilitated them to stay on track:
“It would be good to implement like a goal setting where people enter in their goals of how many drinks they want to have a week and then at the end of the week they can check” [Participant 1]
When asked how the strategies could be delivered in a more effective manner, all users mentioned that it would be useful to include a function within the app in which the strategies that had been previously applied could be referred to at any time:
“I found it confusing because you couldn’t confirm whether or not you had used a particular strategy” [Participant 4]
Discussion
Accumulated literature suggests that PBS are a promising adjunct to treatment for risky drinking (e.g., [43]). Findings have been less consistent when PBS has been offered as a stand-alone treatment (e.g., [14]). In these prior implementations, participants have typically been given strategies at a single time point that are not tailored to their context. To expand on these developments, Minimise, an EMI for young adults that combines self-monitoring functionality and tailored delivery of protective strategies, was developed. To evaluate this app, the aim of this pilot study was twofold: (1) assess the benefit of Minimise using a randomized controlled design and (2) examine the usability and acceptability of Minimise using a qualitative study design.
Outcome Findings
In terms of RQ1, no change was found in alcohol use (i.e., RSOD episodes) or drinking-related harms (i.e., interpersonal) across time or group. For RQ2, participants in the intervention group appeared to increase their use of PBS at follow-up, as compared to the control group.
The intervention was shown to be successful in increasing the users’ application of PBS; however, this increased uptake was not shown to be associated with a reduction in risky drinking behaviors, as would be expected. There are two possible reasons for this. First, participants may not have implemented the PBS in high-risk situations. For example, perhaps users only applied the strategies to situations in which they felt comfortable reducing their alcohol intake, where there was no expectation to drink excessively (e.g., family gathering). In contrast, in situations with inherent pressure to drink (e.g., social events with peers), participants may not have had the capability to implement the appropriate strategies. Interventions incorporating PBS should include other techniques that can support the user to overcome potential barriers in the implementation of the strategies, particularly in situations where external pressure to drink is high. Indeed, drink refusal skills training has been shown to promote self-efficacy and reductions in alcohol use, particularly in high risk social situations (e.g., [44, 45]). The purpose of this training is to teach the individual on how to adopt and enact more adaptive responses to social situations that involve alcohol use [46]. It would be advantageous for future app-based interventions to assess if the combination of PBS coupled with training on drink-refusal skills generates reductions in risky drinking behaviors.
Second, it is also possible that some of the PBS strategies were not as effective as anticipated. A growing body of literature shows that there are some PBS strategy subtypes that are more effective in reducing alcohol use than others. Indeed, a number of studies (e.g., [47, 48]) have shown that strategies which change the “manner of drinking” (e.g., mixing different types of alcohol) are more effective in reducing alcohol use than strategies which aim to “limit consumption” (e.g., set a limit on the number of drinks) or “avoid serious hazards” (e.g., nominate a designated driver). The current study used all available strategies from the PBS framework in order to deliver a breadth and variety of information, and the requirement to disseminate strategies that were tailored to the person’s context. Yet, this did not appear to improve the participants’ drinking behaviors. Further, there was no association between adherence to the app and subsequent positive outcomes, suggesting that more engagement with the content does not appear to effect change in drinking outcomes. Interventions utilizing PBS, therefore, may benefit from delivering only the strategies that have the strongest evidence in reducing alcohol use (i.e., manner of drinking) and excluding those that are less effective (e.g., limiting consumption and avoiding serious hazards).
Outcome Limitations
This pilot study did not include a long-term follow-up, and hence, it is possible that some of the changes in drinking may not be detected by the immediate post intervention assessment used. Indeed, research shows that changes to drinking behavior, via the application of PBS, can take time as the individual requires the opportunity to enact the strategy in order for a change to drinking habits to take effect (e.g., [49, 50]). The current study adopted this post-intervention protocol based on prior alcohol reduction EMIs (e.g., [38, 51]), which use an immediate follow-up assessment to mitigate the risk of attrition and dropout. However, it is recommended that EMI studies, designed to alter habits surrounding drinking behaviors, include a longer-follow up period to ensure that if there is an intervention effect, it is captured.
Second, these findings should be considered in light of the relatively small number of participants. While this sample size is consistent with other pilot studies (e.g., [52, 53]), it may have been more difficult to reveal a truly significant finding (given the small effect sizes). In this respect, the study needs to be considered preliminary in nature and one that provides useful information regarding feasibility and effect sizes to guide further work in this area.
Usability Findings
Interestingly, even though participants did not report a reduction in their drinking, the qualitative findings were supportive of the usability and acceptability of the Minimise app to reduce alcohol use. In particular, there were three features of the app that were well-received by the users. First, users scored Minimise high on the SUS due to its streamlined interface and well-integrated functionality. This feedback is important in delivering an intervention for substance misuse. Indeed, it is probable that there will be times in which the user will be engaging with the app when they are drinking and possibly intoxicated. Ensuring that the system is a straightforward one is essential for people to continue to engage with the app even if they are inebriated. Second, users agreed that a strength of the Minimise app was its tailored functionality. In turn, participants reported that this feature made the strategies highly transferable to the environment they were in. This finding echoes a number of research studies that show tailored information is more likely to be read, remembered, and acted upon, in contrast to generic information (e.g., [52, 54]). Finally, participants commented that the self-monitoring functionality facilitated their understanding into how much alcohol they were drinking and the complex interplay between internal states, external factors, and subsequent drinking behavior. This finding is consistent with a number of studies that have found self-monitoring useful in providing insight to and curtailing risky drinking behaviors (e.g., [55, 56]).
Usability Limitations
Notwithstanding the positive feedback regarding Minimise, qualitative feedback identified two key areas in which the app could be improved. First, some participants were already familiar with the strategies suggested by the app and were hoping instead to find new approaches to reducing their drinking. When they recognized strategies, they reported being less interested and engaged in the app. Further instruction at the outset of the study that the app provides common sense, easy-to-implement approaches that may be familiar to the user may serve to offset expectation that all the strategies will be novel and unfamiliar to the participants. A second limitation was the lack of advanced goal-setting functionality. While the self-monitoring component of Minimise was designed to facilitate monitoring and tracking of performance, more explicit messaging and prompts to remind participants of their goals (especially when they are struggling to maintain these) may be helpful. Indeed, research suggests that the mere reminder of goals can be enough to keep participants on track with their intended behavior change [57, 58].
Implications and Conclusion
There are a number of implications that warrant consideration. First, the lack of impact findings suggests that more work is needed on the specific intervention content that is delivered within this app. More broadly, this finding suggests that PBS delivered as a stand-alone intervention, repetitively and tailored to the user’s goal and context, does not appear to be a beneficial method to reduce risky drinking behaviors among young adults, at least not in the short term. Future smartphone-based research that includes PBS components should pair this with additional intervention components that have a strong evidence base (e.g., implementation intentions, e.g., [59], normative feedback, e.g., [60], and drink-refusal skills training, e.g., [61]).
Second, the results of the qualitative study demonstrate Minimise as a highly usable and acceptable tool in helping young adults reduce their alcohol consumption and drinking-related harm in their everyday life. This finding suggests that smartphone apps are a viable platform to deliver drinking-based interventions. This is especially important for those working with young people, considering how notoriously difficult they are to engage in AoD programs [62], but yet how frequently they engage with their smartphone device [63].
In conclusion, this study found that users of the Minimise app significantly increased their application of PBS. Moreover, the app itself was rated by end-users as a highly acceptable and usable device to intervene on drinking behaviors. Despite these encouraging findings, Minimise did not appear to alter drinking-related outcomes among young adults. This suggests one of two things: first, the Minimise app was not helpful in reducing the user’s drinking behaviors. Given that the usability assessment revealed the app to be user-friendly, it is possible that the limited feature of the app is the intervention used, the PBS. As research findings suggest, PBS is more effective when delivered as part of a multicomponent intervention. The second possibility is that the sample size was too small to reveal a true-positive effect. Further work is needed to examine whether this app could generate positive change in the user’s drinking behaviors if the intervention delivered was PBS coupled with other effective intervention components. Moreover, employing a large enough sample size to detect potentially small effect sizes (as evinced in the current study) is strongly recommended for future research in this area. With the significant potential that smartphone-based drinking interventions provide young people (i.e., accessibility, ease of use, no shame), it is important that we as researchers invest in developing a smartphone app that can effectively reduce harmful drinking behaviors among young people.
References
Baumel A, Faber K, Mathur N, Kane JM, Muench F. Enlight: a comprehensive quality and therapeutic potential evaluation tool for mobile and web-based eHealth interventions. J Med Internet Res. 2017;19(3):e82.
Carey KB, Scott-Sheldon LA, Carey MP, DeMartini KS. Individual-level interventions to reduce college student drinking: a meta-analytic review. Addict Behav. 2007;32(11):2469–94.
Dvorak RD, Pearson MR, Day AM. Ecological momentary assessment of acute alcohol use disorder symptoms: associations with mood, motives, and use on planned drinking days. Exp Clin Psychopharmacol. 2014;22(4):285–97.
Kuntsche E, Otten R, Labhart F. Identifying risky drinking patterns over the course of Saturday evenings: an event-level study. Psychol Addict Behav. 2015;29(3):744–52.
Hunt J, Eisenberg D. Mental health problems and help-seeking behavior among college students. J Adolesc Health. 2010;46(1):3–10.
Wu LT, Pilowsky DJ, Schlenger WE, Hasin D. Alcohol use disorders and the use of treatment services among college-age young adults. Psychiatr Serv. 2007;58(2):192–200.
National Health and Medical Research Council. Australian code for the care and use of animals for scientific purposes. 8th ed. Canberra: National Health and Medical Research Council; 2013.
Martens MP, Ferrier AG, Sheehy MJ, Corbett K, Anderson DA, Simmons A. Development of the protective behavioral strategies survey. J Stud Alcohol. 2005;66(5):698–705.
Martens MP, Pederson ER, LaBrie JW, Ferrier AG, Cimini MD. Measuring alcohol-related protective behavioral strategies among college students: further examination of the Protective Behavioral Strategies Scale. Psychol Addict Behav. 2007;21(3):307–15.
Sugarman DE, Carey KB. The relationship between drinking control strategies and college student alcohol use. Psychol Addict Behav. 2007;21(3):338–45.
Barnett NP, Murphy JG, Colby SM, Monti PM. Efficacy of counselor vs. computer-delivered intervention with mandated college students. Addict Behav. 2007;32(11):2529–48.
Dimeff LA, editor. Brief alcohol screening and intervention for college students (BASICS): a harm reduction approach. New York City: Guilford Press; 1999.
Martens MP, Taylor KK, Damann KM, Page JC, Mowry ES, Cimini MD. Protective behavioral strategies when drinking alcohol and their relationship to negative alcohol-related consequences in college students. Psychol Addict Behav. 2004;18(4):390–3.
LaBrie JW, Napper LE, Grimaldi EM, Kenney SR, Lac A. The efficacy of a standalone protective behavioral strategies intervention for students accessing mental health services. Prev Sci. 2015;16(5):663–73.
Martens MP, Smith AE, Murphy JG. The efficacy of single-component brief motivational interventions among at-risk college drinkers. J Consult Clin Psychol. 2013;81(4):691–701.
Gardner B. Habit as automaticity, not frequency. Eur Health Psychol. 2012;14(2):32–6.
Wood W, Neal DT. A new look at habits and the habit-goal interface. Psychol Rev. 2007;114(4):843–63.
Adamson SJ, Heather N, Morton V, Raistrick D. Initial preference for drinking goal in the treatment of alcohol problems: II. Treatment outcomes. Alcohol & Alcoholism. 2010;45(2):136–42.
Moos RH. Theory-based active ingredients of effective treatments for substance use disorders. Drug Alcohol Depend. 2007;88(2–3):109–21.
Heron KE, Smyth JM. Ecological momentary interventions: incorporating mobile technology into psychosocial and health behaviour treatments. Br J Health Psychol. 2010;15(1):1–39.
Nahum-Shani I, Smith SN, Tewari A, Witkiewitz K, Collins LM, Spring B, Murphy S. Just in time adaptive interventions (jitais): an organizing framework for ongoing health behavior support. Methodology Center technical report; 2014. pp. 14–126.
Cerrada CJ, Dzubur E, Blackman KC, Mays V, Shoptaw S, Huh J. Development of a just-in-time adaptive intervention for smoking cessation among Korean American emerging adults. Int J Behav Med. 2017;24(5):665–72.
Johnson M, Jackson R, Guillaume L, Meier P, Goyder E. Barriers and facilitators to implementing screening and brief intervention for alcohol misuse: a systematic review of qualitative evidence. J Public Health. 2010;33(3):412–21.
Sawares AS, Shen N, Xue Y, Abi-Jaoude A, Wiljer D. The impact of mobile apps on alcohol use disorder: a systematic review protocol. JMIR Res Protoc. 2017;6(4):e49.
Hoeppner BB, Schick MR, Kelly LM, Hoeppner SS, Bergman B, Kelly JF. There is an app for that–or is there? A content analysis of publicly available smartphone apps for managing alcohol use. J Subst Abus Treat. 2017;82:67–73.
Garnett C, Crane D, West R, Brown J, Michie S. The development of drink less: an alcohol reduction smartphone app for excessive drinkers. Transl Behav Med. 2018;9(2):296–307.
Gustafson DH, McTavish FM, Chih MY, Atwood AK, Johnson RA, Boyle MG, et al. A smartphone application to support recovery from alcoholism: a randomized clinical trial. JAMA Psychiatry. 2014;71(5):566–72.
Crane D, Garnett C, Michie S, West R, Brown J. A smartphone app to reduce excessive alcohol consumption: identifying the effectiveness of intervention components in a factorial randomised control trial. Sci Rep. 2018;8(1):4384.
Witkiewitz K, Desai SA, Bowen S, Leigh BC, Kirouac M, Larimer ME. Development and evaluation of a mobile intervention for heavy drinking and smoking among college students. Psychol Addict Behav. 2014;28(3):639–50.
Gajecki M, Andersson C, Rosendahl I, Sinadinovic K, Fredriksson M, Berman AH. Skills training via smartphone app for university students with excessive alcohol consumption: a randomized controlled trial. Int J Behav Med. 2017;24(5):778–88.
Richardson B. Instant Survey (iOS Version 2.0; Android Version 2.0) [Mobile application software]; 2015. Retrieved from https://itunes.apple.com/us/app/instantsurvey/id955226674?mt=8. Accessed 05 May 2016.
Saunders JB, Aasland OG, Babor TF, De la Fuente JR, Grant M. Development of the alcohol use disorders identification test (AUDIT): WHO collaborative project on early detection of persons with harmful alcohol consumption-II. Addiction. 1993;88(6):791–804.
Donovan DM, Kivlahan DR, Doyle SR, Longabaugh R, Greenfield SF. Concurrent validity of the Alcohol Use Disorders Identification Test (AUDIT) and AUDIT zones in defining levels of severity among out-patients with alcohol dependence in the COMBINE study. Addiction. 2006;101(12):1696–704.
Muthén LK, Muthén BO. Mplus user’s guide. 6th ed. Los Angeles: Muthén & Muthén; 1998-2011.
Singer JD, Willett JB. Applied longitudinal data analysis: modeling change and event occurrence. New York: Oxford University Press; 2003. https://doi.org/10.1093/acprof:oso/9780195152968.001.0001.
Arnaud N, Diestelkamp S, Wartberg L, Sack PM, Daubmann A, Thomasius R. Short-to midterm effectiveness of a brief motivational intervention to reduce alcohol use and related problems for alcohol intoxicated children and adolescents in pediatric emergency departments: a randomized controlled trial. Acad Emerg Med. 2017;24(2):186–200.
Haug S, Paz Castro R, Kowatsch T, Filler A, Dey M, Schaub MP. Efficacy of a web-and text messaging-based intervention to reduce problem drinking in adolescents: results of a cluster-randomized controlled trial. J Consult Clin Psychol. 2017;85(2):147–59.
Napper LE, Kenney SR, Lac A, Lewis LJ, LaBrie JW. A cross-lagged panel model examining protective behavioral strategies: are types of strategies differentially related to alcohol use and consequences? Addict Behav. 2014;39(2):480–6.
Wiers RW, Van De Luitgaarden J, Van Den Wildenberg E, Smulders FT. Challenging implicit and explicit alcohol-related cognitions in young heavy drinkers. Addiction. 2005;100(6):806–19.
Lewis JR. Sample sizes for usability studies: additional considerations. Hum Factors. 1994;36(2):368–78.
Virzi RA. Refining the test phase of usability evaluation: how many subjects is enough? Hum Factors. 1992;34(4):457–68.
Brooke J. SUS-A quick and dirty usability scale. Usability evaluation in industry. 1996;189(194):4–7.
McLellan S, Muddimer A, Peres SC. The effect of experience on system usability scale ratings. J Usability Stud. 2012;7(2):56–67.
Lewis JR, Sauro J. The factor structure of the system usability scale. In International conference on human centered design. Berlin: Springer; 2009. p. 94–103.
Kortum PT, Bangor A. Usability ratings for everyday products measured with the System Usability Scale. Int J Hum Comput Interact. 2013;29(2):67–76.
Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101.
Larimer ME, Lee CM, Kilmer JR, Fabiano PM, Stark CB, Geisner IM, et al. Personalized mailed feedback for college drinking prevention: a randomized clinical trial. J Consult Clin Psychol. 2007;75(2):285–93.
Schinke SP, Cole KC, Fang L. Gender-specific intervention to reduce underage drinking among early adolescent girls: a test of a computer-mediated, mother-daughter program. J Stud Alcohol Drugs. 2009;70(1):70–7.
Witkiewitz K, Donovan DM, Hartzler B. Drink refusal training as part of a combined behavioral intervention: effectiveness and mechanisms of change. J Consult Clin Psychol. 2012;80(3):440–9.
Oei TP, Hasking P, Phillips L. A comparison of general self-efficacy and drinking refusal self-efficacy in predicting drinking behavior. Am J Drug Alcohol Abuse. 2007;33(6):833–41.
Pearson MR, Kite BA, Henson JM. The assessment of protective behavioral strategies: comparing prediction and factor structures across measures. Psychol Addict Behav. 2012;26(3):573–84.
Dulin PL, Gonzalez VM, Campbell K. Results of a pilot test of a self-administered smartphone-based treatment system for alcohol use disorders: usability and early outcomes. Subst Abus. 2014;35(2):168–75.
Gonzalez VM, Dulin PL. Comparison of a smartphone app for alcohol use disorders with an internet-based intervention plus bibliotherapy: a pilot study. J Consult Clin Psychol. 2015;83(2):335–45.
Neighbors C, Lee CM, Atkins DC, Lewis MA, Kaysen D, Mittmann A, et al. A randomized controlled trial of event-specific prevention strategies for reducing problematic drinking associated with 21st birthday celebrations. J Consult Clin Psychol. 2012;80(5):850–62.
Wright C, Dietze PM, Agius PA, Kuntsche E, Livingston M, Black OC, et al. Mobile phone-based ecological momentary intervention to reduce young adults’ alcohol use in the event: a three-armed randomized controlled trial. JMIR mHealth uHealth. 2018;6(7):e149.
Jacobs RJ, Lou JQ, Ownby RL, Caballero J. A systematic review of eHealth interventions to improve health literacy. Health Informatics J. 2016;22(2):81–98.
Yardley L, Morrison L, Bradbury K, Muller I. The person-based approach to intervention development: application to digital health-related behavior change interventions. J Med Internet Res. 2015;17(1):e30.
Freedman MJ, Lester KM, McNamara C, Milby JB, Schumacher JE. Cell phones for ecological momentary assessment with cocaine-addicted homeless patients in treatment. J Subst Abus Treat. 2006;30(2):105–11.
Scott CK, Dennis ML, Gustafson DH. Using smartphones to decrease substance use via self-monitoring and recovery support: study protocol for a randomized control trial. Trials. 2017;18(1):374.
Michie S, Whittington C, Hamoudi Z, Zarnani F, Tober G, West R. Identification of behaviour change techniques to reduce excessive alcohol consumption. Addiction. 2012;107(8):1431–40.
Fry ML, Drennan J, Previte J, White A, Tjondronegoro D. The role of desire in understanding intentions to drink responsibly: an application of the model of goal-directed behaviour. J Mark Manag. 2014;30(5–6):551–70.
Ryan RM, Patrick H, Deci EL, Williams GC. Facilitating health behaviour change and its maintenance: interventions based on self-determination theory. European Health Psychologist. 2008;10(1):2–5.
Gollwitzer PM, Sheeran P. Implementation intentions and goal achievement: a meta-analysis of effects and processes. Adv Exp Soc Psychol. 2006;38:69–119.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic Supplementary Material
ESM 1
(DOCX 11675 kb)
Rights and permissions
About this article

Cite this article
O’Donnell, R., Richardson, B., Fuller-Tyszkiewicz, M. et al. Delivering Personalized Protective Behavioral Drinking Strategies via a Smartphone Intervention: a Pilot Study. Int.J. Behav. Med. 26, 401–414 (2019). https://doi.org/10.1007/s12529-019-09789-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12529-019-09789-0