
Abstract
Purpose
The present study tested the efficacy of a theory-based online intervention comprising motivational (autonomy support) and volitional (implementation intention) components to reduce pre-drinking alcohol consumption and alcohol-related harm.
Method
Undergraduate students (N = 202) completed self-report measures of constructs from psychological theories, pre-drinking alcohol consumption, and alcohol-related harm at baseline and were randomly assigned to one of four intervention conditions in a 2 (autonomy support: present/absent) × 2 (implementation intention: present/absent) design. Participants completed follow-up measures of all variables at 4 weeks post-intervention. All participants received national guidelines on alcohol consumption and an e-mail summary of intervention content at its conclusion. Participants also received weekly SMS messages in the 4-week post-intervention period restating content relevant to their intervention condition.
Results
Neither statistically significant main effect for either the autonomy support or implementation intention intervention components nor an interaction effect was found on the outcome measures. However, statistically significant reductions in pre-drinking alcohol consumption and alcohol-related harm were observed across all groups at follow-up, when compared to baseline.
Conclusion
Reductions in outcome measures were likely related to elements common to each condition (i.e., provision of national guidelines, assessment of outcome measures, e-mail summary, and SMS messages), rather than motivational and volitional components.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Pre-drinking refers to the practice of consuming alcohol prior to attending an event, where alcohol consumption often continues [1,2,3]. Pre-drinkers consume more alcohol and are more likely to experience alcohol-related harm, relative to those who do not pre-drink on a drinking occasion [4, 5]. Pre-drinking is common in university and college populations, where students tend to consume alcohol at hazardous levels and consider excessive alcohol consumption as integral to the “university experience” [6,7,8,9,10]. Students tend to engage in pre-drinking in an attempt to reduce their overall expenditure on alcohol by purchasing alcohol at lower prices from retailers (e.g., supermarkets, grocery stores) to consume in a private setting, as opposed to at a bar or nightclub, and to maximize intoxication prior to attending a subsequent event [7, 11]. Given the inherent risks associated with pre-drinking, there is a need to develop pre-drinking interventions that seek to reduce excessive alcohol consumption and the associated risk of alcohol-related harm [12].
Several alcohol interventions have been developed to reduce excessive alcohol consumption behaviors among university and college students [13, 14]. Many of these interventions draw from psychological theories of social cognition and motivation that include constructs known to influence alcohol consumption (e.g., normative feedback and planning approaches) [15,16,17]. Such interventions work by attempting to target these motivational and social cognitive constructs in an attempt to elicit concomitant behavior change [18]. Two theories that have been applied to alcohol consumption, and received considerable attention in the literature on health behavior change, are self-determination theory [19] and the theory of planned behavior [20]. The following sections explain the fundamental elements of these theoretical approaches in relation to behavior change and the basis for the development of the intervention.
Self-Determination Theory and the Theory of Planned Behavior
Self-determination theory is an organismic theory of motivation, which makes the distinction between different forms of motivation. Specifically, motivation is proposed to exist on a continuum ranging from controlled to autonomous. Controlled motivation refers to engaging in a behavior for mostly extrinsic or externally regulated reasons that are not entirely self-determined. For example, an individual may wish to reduce their alcohol consumption because others will be disappointed with them if they do not or because the individual will feel embarrassed if they fail to do so. Conversely, autonomous motivation reflects engaging in behavior for intrinsic or personally relevant reasons. For example, an individual might reduce their alcohol consumption because it carries personally endorsed benefits (e.g., to health and well-being). Self-determination theory has been applied to predict individuals’ motivation in relation to pre-drinking [21], following research finding that autonomous motivation is a key component in relation to individuals’ keeping alcohol consumption within recommended guidelines [16]. The theory has also been adopted as a basis for interventions aimed at changing health behavior with autonomy-supportive interpersonal styles as a key means to promote autonomous motivation and subsequent health behavior change [22, 23].
In contrast to self-determination theory, the theory of planned behavior is a social cognitive theory that posits intentions as the most proximal antecedent of behavior [20]. Intentions are motivational in nature and reflect an individual’s assessment of how much effort they are prepared to invest in pursuing the behavior. Intentions are a function of three sets of belief-based variables: attitude (i.e., the individual’s positive or negative evaluation of behavior engagement), subjective norm (i.e., perceived social influence surrounding behavioral engagement), and perceived behavioral control (i.e., control over behavioral engagement). These three sets of beliefs influence behavior indirectly via the mediation of intention. Perceived behavioral control is also conceptualized as predicting behavior directly, in instances where an individual’s perceptions of control over the behavior match reality. The theory has demonstrated efficacy in predicting intentions and behavior across multiple health behaviors, with meta-analyses demonstrating that attitudes and perceived behavioral control have the strongest effects on behavior through intentions [24]. There is also evidence to suggest that interventions targeting constructs in the theory, particularly attitudes and perceived behavioral control are effective in changing behavior [25].
Self-determination theory and the theory of planned behavior have been integrated to form a comprehensive account of how individuals’ motivational orientations lead them to form consistent belief-based evaluations and intentions to engage in behavior [26]. The integrated account suggests that self-determined motives serve as distal predictors of behavior through the belief-based constructs in the theory. The process involved is likely due to individuals strategically aligning their sets of beliefs with respect to future participation in the health behavior (e.g., attitudes, perceived behavioral control) with their motives. For example, an individual might be autonomously motivated to reduce their pre-drinking alcohol consumption because it is consistent with their internalized sense of self (e.g., reducing alcohol consumption services personally relevant internalized long-term goals, such as studying for an exam), which leads them to align their attitudes to be consistent with their autonomous motives and hold positive attitudes toward making such reductions in the future, which influences their intentions and subsequent behavior with respect to alcohol. Research has supported the motivational sequence proposed in the integrated model [27] and also demonstrated its efficacy as a basis for intervention [23].
Self-determination theory and the theory of planned behavior are theories that aim to explain motivation across multiple behaviors, contexts, and populations, and they have been applied to many health behaviors [28,29,30] including alcohol consumption [31,32,33]. Parallels can be drawn between these perspectives and specific motivational models that have been developed to explain alcohol consumption. Prominent among these models is Cox and Klinger’s [34] motivational account of alcohol consumption. The model proposes that the consumption of alcohol leads individuals to form expectations of the affective and instrumental effects of alcohol consumption, which influence the individual’s decisions to approach alcohol use in the future. These affective and instrumental effects are analogous to the belief-based evaluations that form the basis of an individual’s intentions to engage in alcohol consumption (i.e., attitude, subjective norm), and decision on whether or not to drink (i.e., intention), from the theory of planned behavior. However, there are also clear distinctions and unique components to the approaches adopted in the current research. For example, the theory of planned behavior also identifies on facilitating factors or barriers with respect to future alcohol consumption, similar to self-efficacy. In addition, self-determination theory focuses on the quality, rather than absolute quantity, of motivation with respect to engaging in, or reducing, alcohol consumption (e.g., controlled or autonomous). In summary, the integration of these theories in the current research offers comprehensive account of alcohol consumption and a basis for intervention that are likely to be effective in changing behavior [35].
Volitional Approaches to Behavior Change
Although the theory of planned behavior, self-determination theory, and integrated approaches based on both have demonstrated efficacy in predicting and changing health behavior [16, 24, 35, 36], a substantial shortfall in the relation between intention and behavior has been noted [37, 38]. This suggests that individuals do not always act in accordance with their intentions, termed inclined abstainers [39] or unsuccessful intenders [38]. The intention-behavior “gap” has been an important area of inquiry and may depend in part on factors such as the individual’s level of self-control, or ability to plan [40, 41], leading researchers to conclude that intention is a necessary, yet not sufficient, requirement for behavior change [42]. Gollwitzer and Brandstätter [43] proposed implementation intentions as a means to overcome limitations in self-regulation that impede enacting intentions. According to Gollwitzer [44], simply forming an intention (e.g., “I intend to consume less alcohol when pre-drinking”) is not sufficient to enact the stated behavior. An implementation intention prompts individuals to augment their intentions to include “if-then” plans, which require individuals to identify a cue in the environment and explicitly link it with the intended action (e.g., “If I finish a drink, I will then have a non-alcoholic drink to consume less alcohol when pre-drinking”). Implementation intentions have been successful in facilitating health behavior change in a range of contexts [42] and, given environmental influences that relate to alcohol consumption (e.g., being offered an alcoholic beverage at a party), may have particular relevance for reducing pre-drinking excessive alcohol consumption [45]. If individuals can identify relevant cues in the pre-drinking environment, these can be used to call the individual to the intended action, resulting in reduced alcohol consumption and risk of experiencing alcohol-related harm.
Implementation intentions are proposed to work by intervening in the post-intentional phase of decision making. Specifically, Heckhausen [46] proposed a model of action phases that distinguishes between motivational and volitional phases in the processes that lead to behavior enactment. The motivational phase includes constructs leading up to and including intention (e.g., autonomous motivation, belief-based evaluations such as attitudes), preceding a volitional stage where that intention may or may not lead to concomitant behavior. Therefore, the generation of implementation intentions may facilitate the attainment of intended behaviors in the volitional stage by specifying important cue-based responses that are consistent with the target behavior (e.g., reductions in pre-drinking alcohol consumption). Research from a self-determination theory perspective has demonstrated that implementation intentions appear more effective when an individual’s reasons for forming them are more autonomously motivated [47, 48]. Individuals who show high self-regulation—the ability to exert control over behavior—tend to exhibit autonomous motivation, likely because the enactment of the intended behavior brings about a personally meaningful or relevant outcome, as opposed to behaviors that are enacted due to external contingencies [49]. Drawing from these theoretical perspectives, targeting the motivational and volitional phases of behavior through the facilitation of autonomous motivation and the formation of consistent implementation intentions may lead individuals to reduce their pre-drinking alcohol consumption than either approach in isolation.
The Present Study
Given the importance of motivational and volitional factors in behavior change consistent with dual-phase models, interventions that include components that target motivation and planning are likely to maximize behavioral engagement and may be appropriate for individuals with low intentions or who lack the self-regulatory capacity to enact these intentions. In the present study, we aimed to test an intervention that targets both motivational and volitional phases, consistent with previous integrative approaches applied to alcohol consumption and goal pursuit [47, 50]. The intervention was developed based on previous developmental work from component theories and recent research conducted with the target population of pre-drinking university students [7, 21, 51]. To target the motivational phase, we provided participants with an autonomy-supportive exercise in which they were instructed to reflect on reducing pre-drinking alcohol consumption in terms of key concepts related to autonomy, which would facilitate autonomous motivation [52]. To target the volitional stage, we informed participants that goals were more likely attained when individuals form if-then plans to enact these goals and instructed participants to form implementation intentions following recent best practice recommendations in the literature [42]. The intervention therefore consisted of four groups: an autonomy support-only group that received only the autonomy support component of the intervention, an implementation intention-only group that received only the implementation intention component of the intervention, a combined group that received both autonomy support and implementation intention components, and a control group that received neither intervention component. The intervention was delivered online, as this was considered a preferable medium for university students engaging in health behavioral interventions, which could be implemented with high reach at low cost, and was likely to benefit at-risk populations who may not seek health services in relation to their alcohol consumption [53,54,55].
We hypothesized main effects for the intervention in reducing pre-drinking alcohol consumption and alcohol-related harm in the autonomy support-only and implementation intention-only groups compared to the control group. In addition, based on previous research which found that individuals were more likely to adhere to implementation intentions when they are autonomously motivated to perform the target behavior [47], we hypothesized that the group receiving both the autonomy support and implementation intention intervention components would experience greater reductions in pre-drinking alcohol consumption than the groups receiving either of the components alone, and the control group.
Methods
Design and Procedure
The study used a 2 (autonomy support: present vs. absent) × 2 (implementation intention: present vs. absent) randomized controlled design, with students completing a questionnaire and receiving the intervention at baseline, and a follow-up questionnaire, 4 weeks later. Students were directed to the online study as displayed through Qualtrics™, which comprised an information sheet detailing the study and an instruction to click “next” if they consented to participate, or otherwise close their browser window. Participants completed baseline measures of alcohol consumption and alcohol-related harm, as well as theory-based measures. Next, participants were randomly assigned to an experimental condition through use of a Qualtrics™ randomization tool that assigned a condition number at random to each participant. The program then proceeded to display elements relevant to that condition based on the number (1 = control; 2 = autonomy support-only; 3 = implementation intention-only; 4 = combined).
Participants in all conditions were initially shown the Australian National Health and Medical Research Council (NHMRC) guidelines on alcohol consumption to reduce the per-occasion and lifetime risk of harm [56]. Participants assigned to the intervention conditions were then presented with the autonomy support intervention content (i.e., the autonomy support-only) or the implementation intention intervention content (i.e., the implementation intention-only) or both the autonomy support and implementation intention components (i.e., the combined condition). The content of the autonomy support condition consisted of an exercise in which the participant was instructed to respond to five autonomy-supportive text prompts, presented one at a time, on successive pages (e.g., “Identifying some of the negative consequences of pre-drinking can be a good first step in forming your plan to reduce your pre-drinking alcohol consumption. Reducing your pre-drinking alcohol consumption will help you to avoid some of these negative consequences you may experience when pre-drinking excessively”). These prompts were developed following guidelines regarding autonomy-supportive communication [52]. The content of the implementation intention condition provided participants with a general definition of an implementation intention and an example specific to reducing pre-drinking alcohol consumption (e.g., “If I finish an alcoholic beverage during a pre-drinking session, I will then drink a glass of water to help reduce my pre-drinking alcohol consumption”). Participants were then asked either to select implementation intentions from the examples provided or to form their own implementation intentions following the if-then format or both. Participants in the combined condition completed the autonomy support component, followed by the implementation intention component, according to their order in terms of action phases [46].
An automated e-mail was sent to all participants on completion of the intervention thanking them for their participation; restating the NHMRC guidelines; providing them with a summary of their responses and, if applicable, their statements from the autonomy support exercise and/or their implementation intentions; and providing them with a reminder to monitor their e-mail inbox for the invitation to complete the follow-up questionnaire in 4 weeks’ time. Prior to follow-up, participants were sent an automated SMS message relevant to their condition each week over 4 weeks (i.e., participants assigned to the control group received restated NHMRC guidelines, participants assigned to the autonomy-support, implementation-only, and combined conditions, received SMS messages related to the respective content received), consistent with previous research [57]. At follow-up, participants completed the same measures of pre-drinking alcohol consumption and alcohol-related harm, the theory-based measures, and a measure of goal progress.
Recruitment Procedures
The recruitment strategy involved printed posters and messages advertising the study, which directed eligible students to a URL to the intervention questionnaire hosted on the Qualtrics platform. Posters were placed around university campuses, in Facebook advertisements targeting university students with an interest in alcohol, and through an online system to a university-based participant pool. Participants were eligible if they were over 18 years of age, and had engaged in pre-drinking (defined as “the practice of consuming alcohol prior to attending a subsequent social event, where alcohol consumption often continues”) in the previous 12 months. Participants were informed that they would be taking part in an intervention to reduce pre-drinking alcohol consumption; however, they were blinded as to the purpose of the intervention components and the content of other conditions.
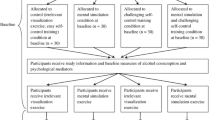
Figure 1 shows the progression of participants through the intervention from baseline to follow-up. Thirteen participants did not complete the intervention at baseline, leaving a sample of a 202 participants (Mage = 20.95 years; SDage = 4.02 years; 147 [72.77%] female). A total of 117 (57.92%) participants completed the 4-week follow-up questionnaire (Mage = 20.86 years; SDage = 3.89 years; 87 [74.36%] female). Table 1 includes age and gender information for each condition, at baseline and follow-up. The majority of participants at baseline (86.63%) and follow-up (91.45%) reported that they were pursuing degrees in health-related faculties.Footnote 1 Participants in the final sample completed the intervention between August 2015 and June 2016, coinciding with the beginning of second semester, and first semester, respectively. Recruitment and enrolment for the intervention occurred over two semesters; however, there was no effect of month of enrolment in the intervention on pre-drinking alcohol consumption or alcohol-related harm at baseline, nor follow-up, evidenced by one-way ANOVA (ps > .232) and non-parametric Kruskal-Wallis tests (ps > .150).

Participant flow diagram
Measures
Hazardous Alcohol Consumption
We used the Alcohol Use Disorders Identification Test (AUDIT-C) [58] as an indication of hazardous alcohol consumption. The AUDIT-C comprises four statements regarding hazardous alcohol consumption behavior and outcomes (e.g., “How often did you have a drink containing alcohol in the past year?”), with responses scored from 0 (e.g., “never”) to 4 (e.g., “6 or more times a week”), and is summed to derive a total score ranging from 0 to 12, with higher scores indicative of hazardous alcohol consumption.
Outcome Measures
Participants reported their pre-drinking alcohol consumption for each of the previous 4 weeks in standard drink equivalents, with the aid of a pictorial guide detailing common beverage containers and their respective standard drink totals [56]. Weekly pre-drinking alcohol consumption was summed to create a monthly score, consistent with previous research [16].
Alcohol-related harm was measured using the Brief Young Adult Alcohol Consequences Scale (B-YAACQ) [59], comprising 24 statements related to the experience of alcohol-related harm (e.g., “I have done something I have later regretted because of drinking”), with participants responding “yes” or “no” via radio button whether each statement is true of them. Although the B-YAACQ was developed for use over a 12-month period, we amended the time frame to refer to the 4-week period at baseline and follow-up, to ascertain an effect of the intervention, consistent with previous research [60].
Theory of Planned Behavior Measures
We measured participants’ attitude, subjective norm, perceived behavioral control, and intentions, regarding reducing pre-drinking alcohol consumption between baseline and follow-up, based on previous research [21]. For attitude, we used a six-point bipolar adjective scale with a common stem (“reducing my pre-drinking alcohol consumption over the next four weeks would be… bad/good”; Cronbach’s α = 0.87 [baseline]; 0.89 [follow-up]). Subjective norm was assessed using three statements (e.g., “people who are important to me would want me to reduce my alcohol consumption during pre-drinking sessions”) with participants responding on a scale from 1 (“strongly disagree”) to 6 (“strongly agree”). Unfortunately, participant scores for subjective norm were unavailable, due to a programming error in the online questionnaire. Perceived behavioral control was also assessed using three statements (e.g., “If I wanted to, I could reduce my pre-drinking alcohol consumption”) and a similar response scale from 1 (“strongly disagree”) to 6 (“strongly agree”; Cronbach’s α = 0.77 [baseline]; 0.84 [follow-up]). Intention was measured using three items (e.g., “I intend to reduce my pre-drinking alcohol consumption over the next four weeks”) and a similar response scale from 1 (“strongly disagree”) to 6 (“strongly agree”). Item scores were averaged (Cronbach’s α = 0.98 [baseline]; 0.98 [follow-up]).
Self-Determined Goals
A measure of goal self-concordance [47] was used to reflect the extent to which participants pursued the goal of reducing their pre-drinking alcohol consumption for autonomous or controlled reasons. Participants provided responses to four statements reflecting controlled (e.g., “because somebody wants me to, or because I’ll get something from somebody if I do”) and autonomous (e.g., “because you really believe that it’s an important goal to have. You endorse it freely and value it wholeheartedly”) reasons, on a Likert-type response scale from 1 (“not at all for this reason”) to 9 (“completely because of this reason”). Consistent with Ryan and Connell’s [61] work on the relative autonomy index, which has been supported in a recent meta-analysis [62], we adopted the approach of Koestner et al. [47] to compute our measure of self-concordance by subtracting scores on controlled items from those on autonomous items (Cronbach’s α = 0.51 [baseline]; 0.45 [follow-up]).
Planning Ability
We included a measure of planning form the self-regulation questionnaire [63] to assess the planning ability of participants at baseline and follow-up. This measure consisted of nine items reflecting planning (e.g., “I have trouble making plans to help me reach my goals”), with response scales ranging from 1 (“strongly disagree”) to 5 (“strongly agree”). Item scores were averaged (Cronbach’s α = 0.81 [baseline]; 0.85 [follow-up]).
Results
Preliminary Analyses
Intervention Condition Variables
We developed two dichotomous variables to represent the intervention conditions for subsequent analyses. The variables denoted whether or not the participant received the autonomy support component (coded 0 or 1) or the implementation intention component (coded 0 or 1).
Alcohol-Related Variables
At baseline, the average AUDIT-C score for the sample was 4.52 (SD = 2.16), and the average pre-drinking alcohol consumption for the 4 weeks prior to was 16.07 standard drinks (SD = 17.14, mdn = 11.00). Participant B-YAACQ average scores at baseline were 6.31 (SD = 3.85). These scores were largely consistent with previous research [64,65,66]. Participants reported engaging in an average of 2.97 pre-drinking sessions per month (SD = 1.94, mdn = 3), spending $27.92 (SD = $16.72, mdn = $25.00) on pre-drinking alcohol, and AUD $42.54 (SD = $31.18, mdn = $40.00) on alcohol consumed following a pre-drinking (i.e., at the subsequent event).
Randomization Checks
To ascertain whether random allocation to conditions was successful, a MANOVA was conducted with intervention components (i.e., autonomy support: 0 or 1; implementation intention: 0 or 1) as the independent variables and age, AUDIT-C score, attitude, perceived behavioral control, planning, intention, goal self-concordance, baseline pre-drinking alcohol consumption, and alcohol-related harm as the dependent variables. The MANOVA showed no statistically significant main effect for the autonomy support (F(9,170) = 1.51, p = .150; Wilk’s Λ = 0.93; partial \( {\eta}_p^2 \) = 0.07) or implementation intention (F(9,170) = 0.32, p = .968; Wilk’s Λ = 0.98; partial \( {\eta}_p^2 \) = 0.02) components nor a statistically significant interaction effect (F(9,170) = 1.52, p = .144; Wilk’s Λ = 0.93; partial \( {\eta}_p^2 \) = 0.07). A χ2 test of contingencies showed no statistically significant difference in gender proportion between conditions: χ2(3) = 2.04, p = .565, Cramer’s V = 0.10.
Attrition Checks
To check for any bias related to attrition, a multivariate analysis of variance (MANOVA) was conducted with completion status (baseline-only, n = 61; baseline and follow-up, n = 109) as the independent variable and age, AUDIT-C score, attitude, perceived behavioral control, planning, intention, goal self-concordance, baseline pre-drinking alcohol consumption and alcohol-related harm as the dependent variables. The MANOVA was not statistically significant (F(9,160) = 0.64, p = .762, Wilk’s Λ = 0.97; partial \( {\eta}_p^2 \) =0.04), indicating that participants who completed baseline-only did not significantly differ to those who went on to complete the follow-up in terms of their responses. Chi-square tests showed that participant attrition was not related to gender (p = .820, Cramer’s V = 0.02) nor condition (p = .565, Cramer’s V = 0.10).
Manipulation Checks
We compared mean scores on goal self-congruence between participants who received the autonomy support component of the intervention (i.e., those in the autonomy support and combined conditions) and those who did not (i.e., those in the control and implementation intention conditions), using a one-way analysis of covariance (ANCOVA) with a variable indicating whether participants received the autonomy support component of the intervention (coded 0 or 1), controlling for baseline self-congruence scores. The test was not statistically significant: F(1,115) = 1.97, p = .163, \( {\eta}_p^2 \) = 0.02, indicating goal self-concordance did not differ significantly between those who received an autonomy support manipulation (M = 3.87; SE = 0.60) and those who did not (M = 2.66; SE = 0.63). Participant responses to autonomy support prompts were coded for consistency, with 33 (61.10%) participants providing responses consistent with all four prompts and the majority (n = 48 [88.90%]) providing responses consistent with at least three prompts.
Fifty-six participants selected and/or formed one or more implementation intentions, with the majority selecting or forming one (n = 24 [42.86%]), followed by two (n = 20 [35.71%]), three (n = 8 [14.29%]), four (n = 3 [5.36%), and five (n = 1 [1.79%]). Kruskal-Wallis tests indicated no statistically significant differences between the total number of implementation intentions selected or formed for pre-drinking alcohol consumption (χ2(5) = 2.47, p = .649) and alcohol-related harm (χ2(5) = 1.68, p = .794). A total of 38 participants selected one or more experimenter-provided implementation intentions only, with 18 generating at least one implementation intention either in conjunction with an experimenter-provided (12) or outright (8). The self-generated implementation intentions were assessed for compliance with instructions, scored using a dichotomous scale as to whether the content complied (1) or not (0). Six of the self-generated implementation intentions were deemed non-compliant, and 12 were deemed compliant. Mann-Whitney U tests indicated no difference between compliers and non-compliers in terms of pre-drinking alcohol consumption (compliers mdn = 7.00, non-compliers mdn = 3.50; U = 31.50, z = − 1.38, p = .169) nor alcohol-related harm (compliers mdn = 3.00, non-compliers mdn = 1.00; U = 25.00, z = − 1.85, p = .065).
Main Analyses
We conducted mixed model analyses of variance (ANOVA) with the dummy-coded variables for the autonomy support (absent = 0, present = 1) and implementation intention (absent = 0, present = 1) intervention components as between-participant factors and time (i.e., baseline, follow-up) as the within-participant factor. Separate analyses were conducted with pre-drinking alcohol consumption (total standard drinks consumed during pre-drinking sessions) and alcohol-related harm (B-YAACQ scores) as the dependent variables. This way, main effects of the control, autonomy support only, implementation intention only, and combined intervention conditions on the outcomes, along with the main effect of time and interaction effects, could be compared. Both complete-case and intention-to-treat with the last observation carried forward analyses were conducted.Footnote 2 Assumptions of sphericity and equality of error variances were met (ps > .05) prior to conducting the main analyses.
Effects of the Intervention on Pre-drinking Alcohol Consumption
ANOVAs revealed no statistically significant three-way interaction effect of time, autonomy support, and implementation intention (F(1,197) = 2.02, p = .157, \( {\eta}_p^2 \) = 0.01). There were also no statistically significant two-way interaction effects of time and autonomy support (F(1,197) = 0.08, p = .772, \( {\eta}_p^2 \) < 0.01), and time and implementation intention (F(1,197) = 0.48, p = .489, \( {\eta}_p^2 \) < 0.01), on pre-drinking alcohol consumption. A statistically significant main effect of time on pre-drinking alcohol consumption was found, with a large effect size (F(1,197) = 26.65, p < .001, \( {\eta}_p^2 \) = 0.12). Participant pre-drinking alcohol consumption at baseline (M = 17.76, SE = 1.35) was significantly different from that at follow-up (M = 13.95, SE = 1.20), a difference of 3.81 standard drinks. Finally, there were no statistically significant two-way interactions for the autonomy support and implementation intention conditions on pre-drinking consumption.
Effects of the Intervention on Alcohol-Related Harm
We found no statistically significant three-way interaction effect of time, autonomy support, and implementation intention (F(1,198) = 1.66, p = .199, \( {\eta}_p^2 \) = 0.01) and no statistically significant two-way interaction effects of time and autonomy support (F(1,198) = 0.05, p = .823, \( {\eta}_p^2 \) < 0.01) and time and implementation intention (F(1,198) = 0.36, p = .551, \( {\eta}_p^2 \) < 0.01) on alcohol-related harm. We also found the statistically significant main effect of time with a large effect size: (F(1,198) = 80.22, p < .001, \( {\eta}_p^2 \) = 0.29). Participant B-YAACQ scores at baseline (M = 6.62, SE = 0.29) were significantly reduced at follow-up (M = 4.66, SE = 0.30), a difference of 1.96. There were no statistically significant two-way interactions for the autonomy support and implementation intention conditions on pre-drinking consumption.Footnote 3
Effects of the Intervention on Psychological Variables
To check for an effect of the intervention on psychological variables, a MANCOVA was conducted with the intervention components (autonomy support and implementation intention) as independent variables and attitude, perceived behavioral control, planning, intention, and goal self-concordance as the dependent variables with the baseline measurements for each variable included as covariates. Results revealed no main multivariate effect of the autonomy support (F(5,105) = 1.40, p = .231, Wilk’s Λ = 0.93, \( {\eta}_p^2 \) = 0.07) or implementation intention (F(5,105) = 1.76, p = .129, Wilk’s Λ = 0.91, \( {\eta}_p^2 \) = 0.09) conditions, nor any interaction effect (F(5,105) = 1.66, p = .152, Wilk’s Λ = 0.92, \( {\eta}_p^2 \) = 0.08), on the dependent variables. Baseline-adjusted averaged item means for each psychological variable by intervention condition are included in Table 2.
Discussion
The aim of the present study was to test the efficacy of an online intervention based on psychological theory in reducing pre-drinking alcohol consumption in undergraduate students. The intervention targeted the motivational and volitional phases proposed in the model of action phases [46] using the techniques of autonomy support and prompting the formation of implementation intentions. While the main study hypotheses were not supported (i.e., there was no statistically significant interaction effect nor main effect of the intervention components), we found a strong, statistically significant effect of time independent of intervention components. That is, participants reduced their pre-drinking alcohol consumption by 3.81 standard drinks and experienced 1.96 fewer instances of alcohol-related harm, in the month following the intervention.
Although the main study hypotheses were not supported, the reductions in participant pre-drinking alcohol consumption and experience of alcohol-related harm independent of condition represent a finding warranting further discussion, given that university students experience a range of negative academic and personal outcomes associated with theirs and others’ alcohol consumption [7, 67] and recent meta-analytic evidence suggesting that computer-delivered college and university alcohol interventions show modest effects [68]. The lack of effects of the autonomy support and implementation intention components raises questions over the importance of these theory-based motivational and volitional strategies in changing pre-drinking behavior. The observed reductions in pre-drinking alcohol consumption and alcohol-related harm over time implicate elements that were common to all conditions contributed to behavior change (i.e., assessment of pre-drinking alcohol consumption and alcohol-related harm, provision of alcohol consumption guidelines to reduce the risk of alcohol-related harm, and sending of e-mail summary and SMS reminders) and that the inclusion of additional theory-based components had no significant effect.
Research indicates that Australians are generally unaware of alcohol consumption guidelines, especially young adult Australians and heavy drinkers [69], similar to research from the USA [70]. There is some indication that the administration of outcome measures at baseline leads to assessment reactivity among control group participants and that “attenuated” versions of university and college alcohol consumption interventions can confer treatment effects [71, 72]. Given that participants were required to quantify their alcohol consumption in standard drink equivalents prior to assignment to intervention conditions, it is likely that this assessment contributed to behavior change [71]. Similarly, participants’ completion of theory-based measures that were phrased in terms of behavior change may have led to a question-behavior effect [73]. Reflecting on personal alcohol consumption in relation to national guidelines (i.e., during the intervention and upon receiving the summary e-mail and weekly SMS messages) may have also contributed to reductions in participants’ alcohol consumption. This is likely as SMS messages are thought to improve the efficacy of health behavior interventions through enhancing participant engagement [57, 74]. Although these SMS messages were structured in order to complement the intervention content (e.g., participants receiving the autonomy support component received congruently framed messages), the lack of condition effect suggests that these messages served a prompting function as opposed to a complementary one. In summary, the assessment of pre-drinking alcohol consumption and alcohol-related harm, provision of information on alcohol consumption limits that would reduce the risk of alcohol-related harm, and the receiving of an e-mail summary and four once-weekly SMS reminders following the intervention were sufficient in eliciting reductions in these outcome variables at follow-up.
A potential issue that may partly account for the lack of effects of the motivational or volitional intervention components may be participant compliance. Participants appeared to comply more with the autonomy support component than the implementation intention component, potentially due to the autonomy support component requiring more engagement and introspection, as opposed to the planning task. However, groups receiving the autonomy support component did not score significantly higher on goal self-concordance, suggesting that the manipulation may not have been sufficient in facilitating autonomous motivation to reduce pre-drinking alcohol consumption. Previous research on online motivational interviewing has suggested that increased engagement in the intervention influences their perceptions of an online motivational interviewing intervention [75]. Specifically, participants prompted to reflect on their open-ended answers reported higher perceived relevance of the intervention, higher perceived ability to express and elaborate on their answers, and higher overall appreciation than participants who did not have the opportunity to reflect [75]. Self-determination theory-based interventions have also been more intensive, delivered “face-to-face,” often involving repeated interactions with practitioners [76]. Means to optimize participant engagement in online self-determination interventions may be an important consideration in future research.
Similarly, compliance with the implementation intention intervention was generally limited, with many participants failing to generate statements that complied with instructions and examples provided or providing responses that were not congruent with the goal of reducing pre-drinking alcohol consumption. Given that the implementation intention component was developed following many of the recommendations of planning intervention components as outlined by Hagger et al. [42], this may raise questions over the use of online implementation intention interventions to reduce pre-drinking behavior. It is likely that prompting participants to consider specific contingencies in implementation intentions (i.e., to address barriers or obstacles to successful goal attainment), or increasing the emphasis on the formation of simple and specific plans, may be useful, as some participants’ plans alluded to naïve or overly optimistic strategies that may not have been successful over the intervention period (e.g., “If I feel tipsy, then I will stop drinking”). This may be especially relevant in the university student population, where alcohol consumption is synonymous with identity and socialization, and attempts to moderate or refuse to drink excessively may be especially challenging [77, 78]. Armitage [79] found that experimenter-provided implementation intentions were more effective in reducing alcohol consumption than those that were self-generated. Other possible factors regarding the lack of effect of implementation intentions on behavior change could be that participants who opted for one or both of the experimenter-provided implementation intentions may have simply selected these options as they were easier than generating their own or to expedite progression through the intervention. It is likely that the cues outlined in the experimenter-provided implementation intentions did not arise following the intervention (e.g., the participant was not offered a drink). Future research may measure participant commitment to, and perceived success of, their implementation intentions and assess plan recall, to ascertain whether these factors influence behavior change and goal attainment.
It is important to raise the issue of the lack of power of the intervention to detect statistically significant effects. We have included a post hoc analysis indicating statistical power required to detect the effects of time, autonomy support, and implementation intentions, as well as their interactions, in Electronic Supplementary Material 3. A meta-analysis of health behavior interventions using autonomy support strategies report small-to-medium-sized effects on behavioral outcomes (ρ = 0.33 or ηp2 = 0.11; [36]). However, the effect for the current intervention is more than ten times smaller than this effect (ηp2 < 0.01); accordingly, we had very low power to detect such a small effect. Put differently, to have adequate statistical power (β = 0.80) to find a small effect of the autonomy support intervention on behavior would have required a substantially larger sample size (n = 592). Similarly, the effect size of the implementation intention intervention component in the present study is small (ηp2 < 0.01) in comparison to the small-to-medium-sized meta-analytic effect of that observed in meta-analyses of implementation intentions (d = 0.48 or ηp2 = 0.06), based on averaged effect sizes [80, 81].
So what can be deduced from these data regarding interventions to reduce pre-drinking? Certainly, our study was insufficiently powered to detect main effects of the autonomy support or implementation intention effects on pre-drinking alcohol consumption and alcohol-related harm, but considering the size of the effect and the sample size required to detect it, conducting a sufficiently powered study would require substantial resources. Furthermore, the impact of the interaction of the two components on pre-drinking also seems to be trivial in size. Nevertheless, it is important to acknowledge that such small effects may have clinical significance if implemented at the population level. This notwithstanding, the substantive effect of time, for which we had sufficient statistical power, suggests that one or more of the components common to both conditions (e.g., measurement, provision of NHMRC guidelines, e-mail summary, SMS reminders) were effective in reducing pre-drinking alcohol consumption and alcohol-related harm, providing an avenue for further investigation. A more viable endeavor may be to isolate these components and design an intervention trial that evaluates their effectiveness.
Strengths, Limitations, and Future Directions
The present study has several strengths and limitations that should be considered in light of the findings. The design of the study allowed for an online intervention to be delivered to a large proportion of university students in a preferred medium, as well as a means of testing an online autonomy supportive intervention [53, 75]. The use of a randomized controlled design, testing the motivational and volitional approaches in isolation and combination, has contributed to research in this area [47]. However, several major limitations that may influence the interpretation and application of the present findings must be discussed.
An important consideration in interpreting the findings of the present study relates to the measures used. The accuracy of participants in retrospectively recalling their alcohol consumption accurately is limited; however, there is some evidence to suggest that participant recall may at least be underestimated [70, 82]. Further, the alteration of the B-YAACQ to refer to a 4-week period may have influenced the sensitivity of the measure in terms of accounting for short-term change (e.g., it may be more likely that students would encounter certain instances of alcohol-related harm over a longer period of time). Similarly related to measures, a necessary part of the evaluation of this intervention was to ascertain whether or not it had any effect on participants’ scores on the measures of motivational and volitional constructs. Although we were unable to test this on all theory measures due to the problem with the subjective norm measure, the lack of significant differences between groups on the psychological and outcome measures suggest that the intervention did not influence participants’ beliefs nor motivation, and this may in part explain the lack of concomitant behaviour change.
Although the use of e-mail summary and SMS reminders was implemented to enhance the efficacy of the intervention components, we are unable to ascertain if these methods complemented the intervention techniques as intended. It may be that SMS reminders that are more aligned with participant responses (e.g., that reiterate or summarize their content), and measurement of their influence from the perspectives of participants, would elucidate this issue. Isolating the impact of these messages in future studies adopting a factorial design including message and no message conditions would elucidate the independent and interactive effects of messaging on behavioral outcomes. Future research may also consider allowing participants to compose their own SMS reminders or opt for goal (e.g., reducing pre-drinking alcohol consumption) or plan (e.g., implementation intention) reminders [83, 84]. The relatively short intervention length, or the low “dosage,” may have limited the efficacy of the intervention in eliciting behavior change through the autonomy support and/or implementation intention components. Increased researcher or health practitioner involvement (e.g., assessing the suitability of participant responses to intervention prompts) and “booster doses” could be used to maintain autonomous motivation or allow for alternative implementation intentions to be adopted.
Compliance issues also limit the extent to which the lack of implementation intention effect can be attributed to the technique itself or failure to form suitable implementation intentions that led to the reduction in outcome measures. The length of follow-up also precludes any speculation of the effectiveness of the component over longer periods of time, as opportunities to enact plans become evident, or the decision to reduce pre-drinking alcohol consumption becomes more internalized and autonomously motivated [85]. Given the absence of a significant effect at the follow-up period, a lagged time effect may be minimal.
Conclusion
The present study used motivational and volitional techniques (i.e., autonomy support and implementation intentions) from psychological theories of health behavior to reduce pre-drinking alcohol consumption and alcohol-related harm in a group of undergraduates. These techniques did not lead to more substantial reductions in these outcome measures in isolation, or in combination, than that experienced by participants in a control group. Given all participants were assessed on outcome variables at baseline, provided with information on alcohol consumption limits to reduce the per-occasion and lifetime risk of alcohol-related harm, and e-mail summary and SMS reminders, this may have been sufficient to account for behavior change. Future research should attempt to ascertain whether this effect can be replicated in multiple samples in similar contexts.
Notes
At baseline, students were coded as belonging to arts (n = 6; 2.97%), business (n = 8; 3.96%), education (n = 4; 1.98%), science (n = 7; 3.47%), health (n = 175; 86.63%), and humanities n = 2; (0.99%) faculties. At follow-up, students were coded as belonging to arts (n = 3; 2.56%), business (n = 3; 2.56%), education (n = 1; 0.85%), science (n = 1; 0.85%), health (n = 107; 91.45%), and humanities (n = 3; 1.71%) faculties. Participants’ scores on outcome measures did not differ as a function of their university, nor between pool and non-pool members; analyses are included in Electronic Supplementary Material 1.
Results from complete case analyses are included in Electronic Supplementary Material 2.
We also conducted our main analyses using hierarchical linear multiple regression. The analyses revealed an identical pattern of relations.
References
Pedersen ER, LaBrie JW. Partying before the party: examining prepartying behavior among college students. J Am Coll Heal. 2007;56(3):237–45. https://doi.org/10.3200/JACH.56.3.237-246.
Reed MB, Clapp JD, Weber M, Trim R, Lange J, Shillington AM. Predictors of partying prior to bar attendance and subsequent BrAC. Addict Behav. 2011;36(12):1341–3. https://doi.org/10.1016/j.addbeh.2011.07.029.
Wells S, Graham K, Purcell J. Policy implications of the widespread practice of ‘pre-drinking’ or ‘pre-gaming’ before going to public drinking establishments—are current prevention strategies backfiring? Addiction. 2009;104(1):4–9. https://doi.org/10.1111/j.1360-0443.2008.02393.x.
Labhart F, Graham K, Wells S, Kuntsche E. Drinking before going to licensed premises: an event-level analysis of predrinking, alcohol consumption, and adverse outcomes. Alcohol Clin Exp Res. 2013;37(2):284–91. https://doi.org/10.1111/j.1530-0277.2012.01872.x.
Barry AE, Stellefson ML, Piazza-Gardner AK, Chaney BH, Dodd V. The impact of pregaming on subsequent blood alcohol concentrations: an event-level analysis. Addict Behav. 2013;38(8):2374–7. https://doi.org/10.1016/j.addbeh.2013.03.014.
Hallett J, McManus A, Maycock BR, Smith J, Howat PM. “Excessive drinking—an inescapable part of university life?” A focus group study of Australian undergraduates. Open J Prev Med. 2014;4(7):14–629. https://doi.org/10.4236/ojpm.2014.47071.
Burns S, Crawford G, Hallett J, Jancey J, Portsmouth L, Hunt K, et al. Consequences of low risk and hazardous alcohol consumption among university students in Australia and implications for health promotion interventions. Open Journal of Preventive Medicine. 2015;05(01):13. https://doi.org/10.4236/ojpm.2015.51001.
Slutske WS, Hunt-Carter EE, Nabors-Oberg RE, Sher KJ, Bucholz KK, Madden PAF, et al. Do college students drink more than their non-college-attending peers? Evidence from a population-based longitudinal female twin study. J Abnorm Psychol. 2004;113(4):530–40.
Karam E, Kypri K, Salamoun M. Alcohol use among college students: an international perspective. Curr Opin Psychiatry. 2007;20(3):213–21. https://doi.org/10.1097/YCO.0b013e3280fa836c.
Kypri K, Cronin M, Wright CS. Do university students drink more hazardously than their non-student peers? Addiction. 2005;100(5):713–4.
Miller PG, Droste N. Alcohol price considerations on alcohol and illicit drug use in university students. J Alcohol Drug Depend. 2013;1(2):1–4. https://doi.org/10.4172/jaldd.1000109.
Pedersen ER. Using the solid research base on pregaming to begin intervention development: an epilogue to the special issue on pregaming. Subst Use Misuse. 2016;51:1067–73. https://doi.org/10.1080/10826084.2016.1187533.
Scott-Sheldon LAJ, Carey KB, Elliott JC, Garey L, Carey MP. Efficacy of alcohol interventions for first-year college students: a meta-analytic review of randomized controlled trials. J Consult Clin Psychol. 2014;82(2):177–88.
Larimer ME, Cronce JM. Identification, prevention, and treatment revisited: individual-focused college drinking prevention strategies 1999–2006. Addict Behav. 2007;32(11):2439–68. https://doi.org/10.1016/j.addbeh.2007.05.006.
Neighbors C, Larimer ME, Lewis MA. Targeting misperceptions of descriptive drinking norms: efficacy of a computer-delivered personalized normative feedback intervention. J Consult Clin Psychol. 2004;72(3):434–47.
Hagger MS, Lonsdale A, Chatzisarantis NLD. A theory-based intervention to reduce alcohol drinking in excess of guideline limits among undergraduate students. Br J Health Psychol. 2012;17(1):18–43. https://doi.org/10.1111/j.2044-8287.2010.02011.x.
Hagger MS, Lonsdale AJ, Koka A, Hein V, Pasi H, Lintunen T, et al. An intervention to reduce alcohol consumption in undergraduate students using implementation intentions and mental simulations: a cross-national study. Int J Behav Med. 2012;19(1):82–96.
Mullan B, Todd J, Chatzisarantis NLD, Hagger MS. Experimental methods in health psychology in Australia: implications for applied research. Aust Psychol. 2014;49(2):104–9. https://doi.org/10.1111/ap.12046.
Deci EL, Ryan RM. Intrinsic motivation and self-determination in human behaviour. New York: Plenum; 1985.
Ajzen I. The theory of planned behavior. Organ Behav Hum Decis Process. 1991;50(2):179–211. https://doi.org/10.1016/0749-5978(91)90020-t.
Caudwell KM, Hagger MS. Predicting alcohol pre-drinking in Australian undergraduate students using an integrated theoretical model. Appl Psychol Health Well Being. 2015;7(2):188–213. https://doi.org/10.1111/aphw.12044.
Williams GC, McGregor HA, Sharp D, et al. Testing a self-determination theory intervention for motivating tobacco cessation: supporting autonomy and competence in a clinical trial. Health Psychol. 2006;25(1):91–101. https://doi.org/10.1037/0278-6133.25.1.91.
Chatzisarantis NLD, Hagger MS. Effects of an intervention based on self-determination theory on self-reported leisure-time physical activity participation. Psychol Health. 2009;24(1):29–48. https://doi.org/10.1080/08870440701809533.
Sheeran P, Maki A, Montanaro E, Avishai-Yitshak A, Bryan A, Klein WMP, et al. The impact of changing attitudes, norms, and self-efficacy on health-related intentions and behavior: a meta-analysis. Health Psychol. 2016;35(11):1178–88. https://doi.org/10.1037/hea0000387.
Steinmetz H, Knappstein M, Ajzen I, Schmidt P, Kabst R. How effective are behavior change interventions based on the theory of planned behavior? A three-level meta-analysis. Z Psychol. 2016;224(3):216–33. https://doi.org/10.1027/2151-2604/a000255.
Hagger MS, Chatzisarantis NLD. Integrating the theory of planned behaviour and self-determination theory in health behaviour: a meta-analysis. Br J Health Psychol. 2009;14(2):275–302. https://doi.org/10.1348/135910708x373959.
Hagger MS, Chatzisarantis NLD. An integrated behavior change model for physical activity. Exerc Sport Sci Rev. 2014;42(2):62–9.
McEachan RRC, Conner M, Taylor NJ, Lawton RJ. Prospective prediction of health-related behaviours with the theory of planned behaviour: a meta-analysis. Health Psychol Rev. 2011;5(2):97–144. https://doi.org/10.1080/17437199.2010.521684.
Deci EL, Ryan RM. Self-determination theory: a macrotheory of human motivation, development, and health. Can Psychol. 2008;49(3):182–5. https://doi.org/10.1037/a0012801.
Hagger MS, Chatzisarantis NLD. Self-determination theory. In: Conner M, Norman P, editors. Predicting and changing health behaviour: research and practice with social cognition models. Maidenhead: Open University Press; 2015. p. 107–41.
Knee CR, Neighbors C. Self-determination, perception of peer pressure, and drinking among college students. J Appl Soc Psychol. 2002;32(3):522–43. https://doi.org/10.1111/j.1559-1816.2002.tb00228.x.
Neighbors C, Larimer ME, Markman Geisner I, Knee CR. Feeling controlled and drinking motives among college students: contingent self-esteem as a mediator. Self Identity. 2004;3(3):207–24. https://doi.org/10.1080/13576500444000029.
Cooke R, Dahdah M, Norman P, French DP. How well does the theory of planned behaviour predict alcohol consumption? A systematic review and meta-analysis. Health Psychol Rev. 2014;(ahead-of-print):1–20.
Cox WM, Klinger E. A motivational model of alcohol use. J Abnorm Psychol. 1988;97(2):168–80. https://doi.org/10.1037/0021-843X.97.2.168.
Hagger MS, Chatzisarantis NLD. The trans-contextual model of autonomous motivation in education: conceptual and empirical issues and meta-analysis. Rev Educ Res. 2016;86(2):360–407. https://doi.org/10.3102/0034654315585005.
Ng JYY, Ntoumanis M, Thøgersen-Ntoumani C, et al. Self-determination theory applied to health contexts. Perspect Psychol Sci. 2012;7(4):325–40. https://doi.org/10.1177/1745691612447309.
Hardeman W, Johnston M, Johnston DW, Bonetti D, Wareham NJ, Kinmonth AL. Application of the theory of planned behaviour in behaviour change interventions: a systematic review. Psychol Health. 2002;17(2):123–58.
Rhodes RE, Bruijn GJ. How big is the physical activity intention–behaviour gap? A meta-analysis using the action control framework. Br J Health Psychol. 2013;18(2):296–309.
Orbell S, Sheeran P. ‘Inclined abstainers’: a problem for predicting health-related behaviour. Br J Soc Psychol. 1998;37(2):151–65. https://doi.org/10.1111/j.2044-8309.1998.tb01162.x.
Sniehotta FF, Scholz U, Schwarzer R. Bridging the intention–behaviour gap: planning, self-efficacy, and action control in the adoption and maintenance of physical exercise. Psychol Health. 2005;20(2):143–60. https://doi.org/10.1348/014466604X17452.
Mullan B, Wong C, Allom V, Pack SL. The role of executive function in bridging the intention-behaviour gap for binge-drinking in university students. Addict Behav. 2011;36(10):1023–6.
Hagger MS, Luszczynska A, de Wit J, Benyamini Y, Burkert S, Chamberland PE, et al. Implementation intention and planning interventions in Health Psychology: recommendations from the Synergy Expert Group for research and practice. Psychol Health. 2016;31(7):814–39. https://doi.org/10.1080/08870446.2016.1146719.
Gollwitzer PM, Brandstätter V. Implementation intentions and effective goal pursuit. J Pers Soc Psychol. 1997;73(1):186–99. https://doi.org/10.1037/0022-3514.73.1.186.
Gollwitzer PM. Implementation intentions: strong effects of simple plans. Am Psychol. 1999;54(7):493–503.
Murgraff V, White D, Phillips K. Moderating binge drinking: it is possible to change behaviour if you plan it in advance. Alcohol Alcohol. 1996;31(6):577–82.
Heckhausen H. The Rubicon model of action phases. In: Heckhausen H, editor. Motivation and action. New York: Springer-Verlag; 1991.
Koestner R, Horberg E, Gaudreau P, et al. Bolstering implementation plans for the long haul: the benefits of simultaneously boosting self-concordance or self-efficacy. Personal Soc Psychol Bull. 2006;32(11):1547–58. https://doi.org/10.1177/0146167206291782.
Koestner R, Lekes N, Powers TA, Chicoine E. Attaining personal goals: self-concordance plus implementation intentions equals success. J Pers Soc Psychol. 2002;83(1):231–44.
Pelletier LG, Fortier MS, Vallerand RJ, Briere NM. Associations among perceived autonomy support, forms of self-regulation, and persistence: a prospective study. Motiv Emot. 2001;25(4):279–306. https://doi.org/10.1023/A:1014805132406.
Murgraff V, Abraham C, McDermott M. Reducing Friday alcohol consumption among moderate, women drinkers: evaluation of a brief evidence-based intervention. Alcohol Alcohol. 2007;42(1):37–41. https://doi.org/10.1093/alcalc/agl083.
Caudwell KM, Mullan B, Hagger MS. Combining motivational and volitional approaches to reducing excessive alcohol consumption in pre-drinkers: a theory-based intervention protocol. BMC Public Health. 2016;16(45):1–12. https://doi.org/10.1186/s12889-015-2648-7.
Y-l S, Reeve J. A meta-analysis of the effectiveness of intervention programs designed to support autonomy. Educ Psychol Rev. 2011;23(1):159–88. https://doi.org/10.1007/s10648-010-9142-7.
Kypri K, Saunders JB, Gallagher SJ. Acceptability of various brief intervention approaches for hazardous drinking among university students. Alcohol Alcohol. 2003;38(6):626–8. https://doi.org/10.1093/alcalc/agg121.
Webb TL, Joseph J, Yardley L, Michie S. Using the internet to promote health behavior change: a systematic review and meta-analysis of the impact of theoretical basis, use of behavior change techniques, and mode of delivery on efficacy. J Med Internet Res. 2010;12(1):e4. https://doi.org/10.2196/jmir.1376.
White AW, Kavanagh D, Stallman H, Klein B, Kay-Lambkin F, Proudfoot J, et al. Online alcohol interventions: a systematic review. J Med Internet Res. 2010;12(5):e62.
National Health and Medical Research Council. Australian guidelines to reduce risks from drinking alcohol. Canberra: Commonwealth of Australia; 2009. p. 179.
Fry JP, Neff RA. Periodic prompts and reminders in health promotion and health behavior interventions: systematic review. J Med Internet Res. 2009;11(2):e16. https://doi.org/10.2196/jmir.1138.
Bush K, Kivlahan DR, McDonell MB, Fihn SD, Bradley KA. The AUDIT alcohol consumption questions (AUDIT-C): an effective brief screening test for problem drinking. Arch Intern Med. 1998;158(16):1789–95. https://doi.org/10.1001/archinte.158.16.1789.
Kahler CW, Strong DR, Read JP. Toward efficient and comprehensive measurement of the alcohol problems continuum in college students: the Brief Young Adult Alcohol Consequences Questionnaire. Alcohol Clin Exp Res. 2005;29(7):1180–9. https://doi.org/10.1097/01.ALC.0000171940.95813.A5.
Kuntsche E, Labhart F. Drinking motives moderate the impact of pre-drinking on heavy drinking on a given evening and related adverse consequences—an event-level study. Addiction. 2013;108(10):1747–55. https://doi.org/10.1111/add.12253.
Ryan RM, Connell JP. Perceived locus of causality and internalization: examining reasons for acting in two domains. J Pers Soc Psychol. 1989;57(5):749–61. https://doi.org/10.1037/0022-3514.57.5.749.
Howard JL, Gagné M, Bureau JS. Testing a continuum structure of self-determined motivation: a meta-analysis. Psychol Bull. 2017;143(12):1346–77. https://doi.org/10.1037/bul0000125.
Brown JM, Miller WR, Lawendowski LA. The self-regulation questionnaire. 1999.
Hallett J, Howat P, Maycock B, McManus A, Kypri K, Dhaliwal S. Undergraduate student drinking and related harms at an Australian university: web-based survey of a large random sample. BMC Public Health. 2012;12(1):37. https://doi.org/10.1186/1471-2458-12-37.
Foster JH, Ferguson C. Alcohol ‘pre-loading’: a review of the literature. Alcohol Alcohol. 2013:agt135.
Pedersen ER, LaBrie JW, Kilmer JR. Before you slip into the night, you'll want something to drink: exploring the reasons for prepartying behavior among college student drinkers. Issues Ment Health Nurs. 2009;30(6):354–63. https://doi.org/10.1080/01612840802422623.
Hallett J, Howat P, McManus A, Meng R, Maycock B, Kypri K. Academic and personal problems among Australian university students who drink at hazardous levels: web-based survey. Health Promot J Austr. 2014;24(3):170–7.
Black N, Mullan B, Sharpe L. Computer-delivered interventions for reducing alcohol consumption: meta-analysis and meta-regression using behaviour change techniques and theory. Health Psychol Rev. 2016;10(3):341–57. https://doi.org/10.1080/17437199.2016.1168268.
Livingston M. Perceptions of low-risk drinking levels among Australians during a period of change in the official drinking guidelines. Drug Alcohol Rev. 2012;31(2):224–30. https://doi.org/10.1111/j.1465-3362.2011.00414.x.
de Visser RO, Birch JD. My cup runneth over: young people’s lack of knowledge of low-risk drinking guidelines. Drug Alcohol Rev. 2012;31(2):206–12. https://doi.org/10.1111/j.1465-3362.2011.00371.x.
Kypri K, Langley JD, Saunders JB, Cashell-Smith ML. Assessment may conceal therapeutic benefit: findings from a randomized controlled trial for hazardous drinking. Addiction. 2007;102(1):62–70. 9p
Scott-Sheldon LAJ, Carey KB, Kaiser TS, Knight JM, Carey MP. Alcohol interventions for Greek letter organizations: a systematic review and meta-analysis, 1987 to 2014. 2016. https://doi.org/10.1037/hea0000357.
Mankarious E, Kothe E. A meta-analysis of the effects of measuring theory of planned behaviour constructs on behaviour within prospective studies. Health Psychol Rev. 2015;9(2):190–204. https://doi.org/10.1080/17437199.2014.927722.
Alkhaldi G, Hamilton FL, Lau R, Webster R, Michie S, Murray E. The effectiveness of prompts to promote engagement with digital interventions: a systematic review. J Med Internet Res. 2016;18(1):e6.
Friederichs SA, Oenema A, Bolman C, Guyaux J, Van Keulen HM, Lechner L. Motivational interviewing in a web-based physical activity intervention: questions and reflections. Health Promot Int. 2015;30(3):803–15. https://doi.org/10.1093/heapro/dat069.
Fortier MS, Duda JL, Guerin E, Teixeira PJ. Promoting physical activity: development and testing of self-determination theory-based interventions. Int J Behav Nutr Phys Act. 2012;9(1):1–14. https://doi.org/10.1186/1479-5868-9-20.
Oei TPS, Morawska A. A cognitive model of binge drinking: the influence of alcohol expectancies and drinking refusal self-efficacy. Addict Behav. 2004;29(1):159–79. https://doi.org/10.1016/s0306-4603(03)00076-5.
Leontini R, Schofield T, Lindsay J, Brown R, Hepworth J, Germov J. “Social stuff” and institutional micro-processes alcohol use by students in Australian university residential colleges. Contemp Drug Probl. 2015:0091450915580970.
Armitage CJ. Effectiveness of experimenter-provided and self-generated implementation intentions to reduce alcohol consumption in a sample of the general population: a randomized exploratory trial. Health Psychol. 2009;28(5):545–53.
Bélanger-Gravel A, Godin G, Amireault S. A meta-analytic review of the effect of implementation intentions on physical activity. Health Psychol Rev. 2013;7(1):23–54. https://doi.org/10.1080/17437199.2011.560095.
Gollwitzer PM, Sheeran P. Implementation intentions and goal achievement: a meta-analysis of effects and processes. Adv Exp Soc Psychol. 2006;38 https://doi.org/10.1016/s0065-2601(06)38002-1.
Monk RL, Heim D, Qureshi A, Price A. “I have no clue what I drunk last night” using smartphone technology to compare in-vivo and retrospective self-reports of alcohol consumption. PLoS One. 2015;10(5):e0126209.
Wright CJ, Dietze PM, Crockett B, Lim MS. Participatory development of MIDY (Mobile Intervention for Drinking in Young people). BMC Public Health. 2016;16(1):1–11. https://doi.org/10.1186/s12889-016-2876-5.
Prestwich A, Perugini M, Hurling R. Can implementation intentions and text messages promote brisk walking? A randomized trial. Health Psychol. 2010;29(1):40–9. https://doi.org/10.1037/a0016993.
Koestner R, Powers TA, Milyavskaya M, Carbonneau N, Hope N. Goal internalization and persistence as a function of autonomous and directive forms of goal support. J Pers. 2015;83(2):179–90. https://doi.org/10.1111/jopy.12093.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The study was approved by the Curtin University Ethics Committee (Approval Number HR185/2014/AR1) and pre-registered with the Australian and New Zealand Clinical Trials Registry (ACTRN12614001102662).
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Caudwell, K.M., Mullan, B.A. & Hagger, M.S. Testing an Online, Theory-Based Intervention to Reduce Pre-drinking Alcohol Consumption and Alcohol-Related Harm in Undergraduates: a Randomized Controlled Trial. Int.J. Behav. Med. 25, 592–604 (2018). https://doi.org/10.1007/s12529-018-9736-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12529-018-9736-x