
Abstract
This research focuses on the assessment of fluoride doses in groundwater adopting the mathematical model employed by the USEPA. A total of 456 groundwater samples were tested to assess the spatial distribution of fluoride contamination in the study areas. Three age groups (children, teens and adults) were selected for two-way pathway exposure (potential dose and dermal dose) assessment. For uncertainty and sensitivity of inputs variables, a new emerging Sobol sensitivity analysis (SSA) technique was used to determine the relative importance of inputs using Monte Carlo simulation. Three types of effects, first-order effect (FOE), second-order effect (SOE) and total effect (TE) were calculated. The results showed that 96% of the samples analysed were within the standard acceptable level (1.5 mg l−1) of WHO guidelines. The spatial distribution depicts that the eastern and south-eastern parts of the study area have the higher concentrations with the few spots of elevated concentration in the middle of the north and the south-west areas. The mean value of Hazard Index for children in the study region is less than 1, whereas the 95th percentile exceeded the value of 1 for both children and teens. The FOE shows the concentration of fluoride (Cw) is highly sensitive followed by exposure frequency (EF), intake rate (IRw) and body weight (BW). The SOE scores revealed that IRw–BW are the most important input parameters for the assessment of oral health risk. For the dermal model, the highest value of Sobol score was recorded for interactions Cw–SA for adults followed by teens and children. Further, the results show that the older-age groups have more dermal risk than the younger-age groups. The research explores the feasibility of SSA technique to investigate the effects of individual input parameters for health risk model and whether it can be applied to another contaminant.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Fluoride is ubiquitous in the environment in the form of fluoride ion in groundwater system, whether due to anthropogenic or natural addition (IPCS 2012). Poor water quality contributes to approximately 80% of the world diseases, 65% of which is contributed by endemic fluorosis alone (Adimalla and Venkatayogi 2017; Felsenfeld and Robert 1991; Karami et al. 2017; Miri et al. 2016; Narsimha and Sudarshan 2017; WHO 2011). In a developing country like India, more than 33% of the drinking resources are not suitable for consumption (Cronin et al. 2014). The fluoride contamination is affecting more than 400 million populations in the districts of Bihar, Rajasthan, Madhya Pradesh and West Bengal states of India (Chakraborti et al. 2010; Cronin et al. 2014).
In groundwater system, fluoride concentration depends upon various water-quality parameters such as pH, total solids, alkalinity and hardness (Baghania et al. 2017; Dehghani et al. 2017; Karthikeyan and Shunmugasundarraj 2000; Rostamia et al. 2017; Subba Rao et al. 1998). Samal et al. (2015) have investigated the fluoride contamination in two districts of West Bengal in water sources and agricultural soils and they had found insignificant association of total hardness and phosphate in relation with the fluoride. Furthermore, they have concluded high possibility of bioaccumulation of fluoride in the cultivated crops from contaminated soil and water. Marya et al. (2014) have determined the relationship between dental caries and dental fluorosis at different levels of fluoride in drinking water. From the analysis of results, they have found 1.13 ppm as the optimal level of fluoride with maximum caries reduction and minimum amount of aesthetical objection due to fluorosis. Kumar et al. (2017) have investigated the relationship between fluoride in water, urine, serum and fluorosis and found significant correlation between water, urine and serum fluoride. Edmunds and Smedley (2013) have investigated the association between fluoride, human bones and teeth considering fluoride ion existence. In addition, several studies by other researchers assessed its impact on human and plant considering biological, biochemical and clinical effects (Adimalla 2018; Adimalla et al. 2018a; Jacobson and Weinstein 1977; Li et al. 2018; NAS 1971; Ozsvath 2009; Singh et al. 1963).
Chilton et al. (2006) have stated that the fluoride-bearing minerals (local igneous and metamorphical rocks) are commonly found in Asia (India, Pakistan, Thailand, China and Sri Lanka) as well in African sub-continent (western and southern Africa). Li et al. (2014) have carried out hydrogeological investigation and estimated the fluoride concentration in confined aquifer underlying the first terrace of Weihe River in China. From the analysis of results, they have found fluoride enrichment in groundwater was controlled by geology especially fluoride-bearing minerals and hydrogeological conditions. They further stated that human intervention, ion exchange and mixing of different types of recharge water were the cause for fluoride enrichment.
In Indian context, granite rocks naturally contain fluoride-bearing minerals such as fluorite, apatite, biotite, mica and other minerals, which are the primary sources for fluoride (Cooper et al. 1991; Narsimha and Sudarshan 2017; Maithani et al. 1998; Jacks et al. 2005; Adimalla et al. 2018a, b). In groundwater system, high bicarbonate alkaline condition (pH range 7.5–8.6) is more conducive for fluoride dissolution (Saxena and Ahmed 2001). In addition, factors like temperature, pH, complexing and precipitating ions, cation exchange capacity and duration of water–rock interaction of minerals also influence the dissolution of fluoride in groundwater (Apambire et al. 1997). Narsimha and Sudarshan (2017) have investigated positive correlation between the pH and fluoride content in groundwater. In groundwater system, low calcium content and high fluoride concentration are found due to their low solubility (Apambire et al. 1997). In addition, sodium bicarbonate water type and high bicarbonate alkaline groundwater also ensure high probability of fluoride concentration.
It is a well-established fact that the ingestion of fluoride is associated with chemical toxicity that results in change of physical structure of bones (Miller et al. 1977; Riggs et al. 1990). Fluoride has dual effect (beneficial and detrimental effects) on the human health within narrow range. A small amount is needed to form bones, enamel and to prevent tooth decay, whereas high fluoride can adversely damage bones and teeth (Khorsandi et al. 2016; Petersen 2004; Podgorny and McLaren 2015). Some researchers reported destructive effects on the metabolism of soft tissues (kidney, liver and lungs) (Barbier et al. 2010; Yang and Liang 2011; Zhang et al. 2016) with tumbling intelligence quotient (IQ) in children (Tang et al. 2008). In addition, Bassin et al. (2006) and Choi et al. (2015) have reported possibility to induce skeletal cancer and neurotoxicological effects as a result of high fluoride concentration. Wu and Sun (2016) have investigated the groundwater fluoride contamination and potential risk associated to the local residents in alluvial plain of China. Both oral and dermal pathways were calculated due to intake of drinking of groundwater. From the analysis of results, they have found that children of alluvial plain (in China) were at the higher risk than the adults, and urgent and efficient measures are needed to take to reduce the health risk.
The World Health Organization had recommended a reference level 0.5 to 1.5 mg l−1 for fluoride and as per guidelines of US Public Health Service, the optimal concentration of fluoride in drinking water should be 0.7 mg l−1 (Kohn et al. 2001). Yadav et al. (2013) stated that more than 200 million people suffer from the deadly diseases called fluorosis due to intake of higher fluoride concentration in drinking water throughout the world. Developing countries have greater potential health consequences through intake of fluoride-containing drinking water (Adimalla 2018; Adimalla et al. 2018a, b; Huang et al. 2017; Li et al. 2018; Wu et al. 2015).
The objective of this study was to investigate concentration of fluoride in groundwater of mid-Gangetic plain in five districts of Bihar. After determination of fluoride concentration, a mathematical non-carcinogenic risk-assessment model proposed by USEPA was applied. Sobol sensitivity analysis (SSA) was applied to the Hazard quotient (HQ) model considering the three indices as first-order effect, second-order effect and total effect (TE) to the three age groups (children, teens and adults). For spatial distribution analysis of fluoride, ArcGIS 10.3 software was used.
Materials and methods
Study Area, Sampling and Analysis
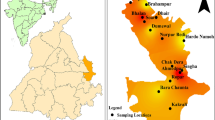
Bihar state is situated in the mid-eastern region of India. Figure 1 shows location of the sampling districts in Bihar as the highlighted part as well as the geographical location of the state of Bihar in India. Aurangabad, Gaya, Jahenabad, Nalanda and Nawada lie in west-south Bihar (WSB) with geographical locations between 24°17′19.75″N to 25°27′40.91″N and 83°59′54.16″E to 86° 3′25.42″E longitude covering the total area of 14,711 square kilometres. Sampling area is a region of the alluvial plain, situated in the southern portion of river Ganges. This area is underlain by recent unconsolidated alluvial deposits, which primarily consist of gravels, sand, silt and clay. Bedrock of this study area is composed of weathered granites with genesis and schists. The groundwater yield of the area has large variability that ranged from 5 to 200 cu m h−1. In addition, the groundwater depth varies from 2 to 14 m below the ground level. The major activity in this area is agriculture with minor mineral exploration. The major industries found in this area include stone quarries, rice mills and sugar factories (Kumar et al. 2018).

Study area with Sampling Location
A total of 456 representative groundwater samples were collected from underground sources across the study area by adopting 6 × 5 km grid size. The groundwater sources were readily available for consumption as drinking water. Sampling site, geo-positions (latitude and longitude) were recorded using Global Positioning System (model: Garmin GPS 72H). For each location, 1-L high-density polyethylene (Thermo Scientific, 1131000BPC) sample bottles were treated with dilute nitric acid overnight and rinsed with ultrapure water (Milli-Q Ultrapure Water Purification System, Model Z00QSVC01). Sample Bottles were washed thoroughly with the sampled bore well/hand pumps water before collecting the water samples. Samples were collected during the pre-monsoon season from marked locations (Fig. 1). Soon after collection at the site, in situ water-quality parameters, such as pH and conductivity, were estimated in the field using a portable instrument (Thermo Scientific Orion™ 9609BNLSLN). Collected groundwater samples were filtered using 0.45-μm membrane filter (syringe filters). To avoid wall deposition, a portion of the samples was acidified after filtration. To avoid the matrix decomposition, the non-acidified samples were stored at 4 °C in dark until completion of analysis (APHA 2005).
Fluoride Estimation Using Ion-Selective Electrode (ISE)
Fluoride concentration of the groundwater samples were determined using fluoride ISE (Thermo Scientific Orion™ 9609BNLSLN) in Thermo Scientific Orion VERSA STAR pH/ISE/Conductivity/RDO/Dissolved Oxygen Multiparameter Meter Kit. The reagents and redistilled water used for the solution preparation (or dilution) were, respectively, of analytical grade (Merk Millipore) and highest-purity milli-pore water. Prior to measurement of the unknown sample, the fluoride ISEs were calibrated by 0.1 to 5 mg l−1 standard solution prepared from 0.5 mg l−1 and 5.0 mg l−1 standard with TISAB II as per instructions provided by the vendor. The slope value for calibration curve was found to be − 58 mV/(mg l−1) at 23 °C. A Teflon-coated stirrer was placed in 100-ml plastic sampler having 50 ml of sample (25 ml standard solution/groundwater sample + 25 ml TISAB II), which was subjeced to stirring at constant rate. After dipping the Fluoride ISE (9609BNWP) into the standard solution/groundwater sample, and once reading became stable, the concentration was recorded. All protocols followed for the analysis were as per standard methods prescribed for the examination of water and wastewater (APHA 2005).
Health-Risk Assessment Model
To assess the health risk for the populations of the mid-Gangetic plain, three groups [children (3–10 years old); teens (11–20 years old); adults (21–72 years old)] were considered. The exposure to fluoride-contaminated groundwater was evaluated in terms of potential dose and dermal dose, which were calculated using the Eqs. (1) and (2) introduced by USEPA (USEPA 1989; Li et al. 2016).
where ADD ingestion denotes the average daily potential dose of fluoride ingested through drinking groundwater. The value ADDdermal calculates the amount of fluoride received by skin absorption in mg kg−1 day−1. The Cw denotes concentration of fluoride in drinking water (mg l−1), IRw is daily intake rate of water (l day−1), EF is exposure frequency (day year−1), ED is the exposure duration (year), BW is the body weight (kg), AT is the averaging time (Days), SA is surface area of skin to get exposure (cm2), Kp is coefficient of permeation (cm h−1), F is the fraction of contact surface within skin and water, and ET is the exposure duration to shower (h day−1).
The non-carcinogenic risk due to exposure of fluoride through groundwater is estimated in terms of Hazard quotient (HQ) for both ADD ingestion and ADD dermal using Eq. (3) (He and Wu 2018; He et al. 2018).
In this regard, RfD is the reference fluoride dose by specific pathway (mg kg−1 day−1). According to USEPA’s Integrated Risk Information system (IRIS), the RfD for oral and drinking ingestion is considered as 0.06 mg kg−1 day−1 (Huang et al. 2017). Reference dose for skin exposure is calculated by Eq. (4) based on USEPA conversation method from drinking RfDw to RfDdermal (Staff 2001).
where RfDdermal and RfDw are, respectively, the dermal and water reference doses, whereas ABSgi is the digestive absorption factor. The overall non-carcinogenic risk due to exposure of fluoride in groundwater is calculated in terms Hazard Index (HI) by Eq. (5)
Sobol Sensitivity Analysis (SSA)
SSA is a global sensitivity analysis tool, in which all the input parameters are varied simultaneously over the whole input space with the increasing dimensionality (Saltelli et al. 1999; Sobol 1993). SSA evaluates the relative continuation of each influential input with their interaction to the variance of the model output. SSA is an innovative approach to understand which reaction and processes have more influence on the overall system. The basic framework of SSA is variance decomposition, which provides a quantitative measure of input contribution to the output variance using Monte Carlo integration. SSA tool is the one of the most powerful variance decomposition techniques compared to the available sensitivity analysis technique (weighted average of local sensitivity analysis, partial rank correlation coefficient, multiparametric sensitivity analysis, Fourier amplitude sensitivity analysis). It calculates the extent of variability in model output considering each input parameters as single and interaction among different parameters. SSA is not intended to identify the cause of the input variability. It just indicates the impact and the extent that the model output has. The basic feature of SSA is that it does not have any underlying assumption between the model input and output with full range of input variance and their interaction between parameters. The steps involved in SSA are depicted in brief in Fig. 2.

The procedure flow chart of the Sobol sensitivity analysis (Zhang et al. 2015)
Consider the following model
where X1,…,Xp represents the independent random input variable having known probability distribution and Y scalar output. The Sobol method decomposes the output variances into the contributed associations of individual input factors. In order to estimate the influence of an input factor on the model output variance, we fix the value of Xi as xi* and vary the other input variables X1, X2,…,Xp and then calculate the change in the variance of output (Y). This conditional variance is calculated using the Eq. (7).
where the variance is taken over the (p – 1) input parameter space X−1 consisting of all the inputs except the X1. The basic framework of Sobol method’s work based on law of total variance can be represented by Eq. (8).
After normalization, we have
The first term in the Eq. (9) represents the first-order sensitivity index (FOSI) for the input Xi. i.e.
Proceeding further through decomposition, it can be reduced to second order, third order and so on. The second-order sensitivity index represents the amount of variance of Y explained by interaction of the factor Xi and Xj (i.e. sensitivity to Xi and Xj) that is calculated based on Eq. (11).
The total contribution to the output variance from the factor (first order plus all its interactions) is calculated through the total order sensitivity index (STi) proposed by Homma and Saltelli (1996), which is calculated using Eq. (12). The interested reader can find more details about the sensitivity analysis methodology in other studies (Saltelli et al. 1999; Sobol 1993; Zhang et al. 2015)
Table 1 provides additional information on model parameters. The selection input parameters would be modelled as random variables (instead of fixed-value inputs). The models (HQ ingestion and HQ dermal) were developed in Python programming using “SALib 1.1.3 package”.
Fluoride Spatial Distribution
Spatial distribution of fluoride was considered to allocate the potential elevated zone of fluoride using software ArcGIS 10.3. To map the fluoride zone, the inverse distance-weighted (IDW) method was used. IDW is a deterministic interpolation technique based on weighted mean of each parameter and the distance between the points. The basic assumption in this deterministic technique is that spatial features of points that are closer to each other are more alike than the features of those that are farther apart. The predicted value has been more influenced by the value of surrounding prediction location (Beg et al. 2011).
Results and Discussion
Analysis of Results and Spatial Distribution of Fluoride
Descriptive statistics of fluoride value of the groundwater samples of five districts are given in the Table 2. The fluoride concentrations in five districts varied from 0.1 to 3.6 mg l−1. The highest fluoride value (3.6 mg l−1) was recorded in the Nawada district followed by Gaya (2.3 mg l−1), Aurangabad (2.1 mg l−1), Jahenabad (1.6 mg l−1) and Nalanda (1.5 mg l−1). The permissible range for fluoride concentration in drinking water recommended by WHO (2004) is 0.5–1.5 mg l−1. From the analysis of results, it was found that 2% (2/112) of Aurangabad, 6% (9/156) of Gaya, 2% (1/47) of Jahenabad, and 9% (7/75) of Nawada districts have exceeded the upper bound of the acceptable level of fluoride (> 1.5 mg l−1). It was also observed that the majority of the sample had fluoride concentration below the lower bound of the recommended level (< 0.5 mg l−1). About 59% samples of Aurangabad, 50% samples of Gaya, 49% samples of Jahenabad, 62% samples of Nalanda, 27% samples of Nawada had concentrations below the lower bound level of 0.5 mg l−1. The pH value in the study region varied from 5.8 to 8.0. The highest standard deviation of pH was found for Nawada districts followed by Gaya, Aurangabad, Jahenabad and Nalanda. The value of EC ranged in the regions from 136 to 3891 µS cm−1. The highest standard deviation was recorded for the Gaya district. The large variations of the in situ parameters may be due to large geographical variability.
The spatial distributions of fluoride in drinking water in five districts in Bihar are shown in Fig. 3. The eastern and south-eastern parts of the study area mostly have the higher concentrations with a few spots of high concentrations in the middle north and south-west. The Nawada district located in the south-east region has the highest concentration of fluoride in terms of spatial extent. Groundwater in the southern and northern districts (Aurangabad, Gaya; and Jahenabad and Nalanda) has fluoride concentrations lower than 0.5 mg/l, which is less than the WHO guidelines (WHO 2004), and may lead to increased tooth decay as harmful health effect.

Spatial distribution of fluoride in groundwater in the studied areas
Risk Assessment of Fluoride
In this section, the non-carcinogenic health risk of fluoride in drinking water to the population Mid-Gangetic plain has been estimated. The ADD was estimated for different age groups that get exposure to fluoride through drinking water consumption. Table 3 shows the results of non-carcinogenic potential doses for the three age groups of study area. The average daily dose of non-carcinogenic risk of fluoride was found to be higher for the children compared to teens and adults. The 95th percentile of potential dose was found higher for children in Nawada (0.174 mg kg day−1) followed by Gaya (0.113 mg kg day−1), Nalanda (0.085 mg kg day−1), Aurangabad (0.081 mg kg day−1) and Jahenabad (0.078 mg kg day−1). In addition, it was also found that the ADD scores are higher than dermal absorption. Therefore, it can be concluded that the ingestion is the primary route of exposure to fluoride through drinking water (WHO 2004). Table 4 shows the descriptive statistics of HI values estimated for ingestion and dermal contact pathways for three age groups (Children, Teens and Adults). The mean HI value for children in all the study regions were less than 1, whereas the 95th percentile exceeded the value of 1 for both children and teens. The results lead us to conclude that children of the study are at the highest risk followed by teens and adults. The cause behind the high risk is the low BW, which results in higher exposure dose for the lower age groups (Huang et al. 2017). Akiniwa (1997) has reported 0.3 mg F kg−1 BW dose as threshold value for inducing acute intoxication to human body. None of the samples of the studied regions exceeded this threshold value. In Nawada district, the HI value of children (mean = 1.49, 95th percentile = 4.34) followed by teens (mean = 1.06, mean = 2.32) showed that these groups were at high non-carcinogenic risk due to exposure of fluoride-contaminated groundwater. Based on the analysis of results, it can be concluded that the lower age groups in the study region are specifically prone to the non-carcinogenic risk. Furthermore, it can also be concluded that a large section of the study area is also affected by the low concentration of fluoride (Fig. 3). The low concentration of fluoride may be of geogenic nature. However, this was not investigated, as the work was beyond the scope of study. The groundwater pH values in all districts are of acidic to neutral in nature, which might resist the dissolution/mobilization of fluoride in groundwater. In addition, the absence of geological minerals especially fluoride-bearing minerals like fluorite, appatite, etc., might also contribute to low fluoride concentrations. Since large variations in hydrogeology and hydrogeological conditions prevail in this region, it is difficult to come to any concrete conclusion, and therefore there arises the need for root-cause analysis. Therefore, water-quality monitoring and assessment should be carried out for preventing non-carcinogenic health effect. The alternate way to minimize this high exposure of fluoride concentration is through adoption of deep well as sources for drinking water. Huang et al. (2017) have also emphasized the preference for adoption of deep well as sources where the shallow groundwater is contaminated by high fluoride concentration.
Model Sensitivity: Sobol Scores
The uncertainty within any model output is strongly affected by availability and quality of input data. For any risk-assessment model, uncertainty occurring during the whole process of sampling and analysis can be minimized but not removed completely. Higher uncertainty is obtained, when single-point values are used to estimate the risk of a given population. To overcome such effects and calculate the most influential inputs of model, the variance decomposition SSA was performed considering sample size of 10,000 simulations. The Sensitivity analysis of model output is strongly influenced by the specific range of input parameters. The authors have selected the values listed in Table 1, appropriate for the present analysis, which were published by Huang et al. (2017). SSA calculates the effects of each input through minimizing the uncertainty in calculations through variance decomposition. SSA was performed on HQ model and the Sobol indices were calculated for four input parameters (Cw, IRw, EF, and BW) that were considered as potential dose for inducing the ingestion effect. Further, for dermal health risk, HQ dermal model was used considering six inputs (Cw, F, ETS, EF, BW, and SA) parameters. To investigate sensitivities of both the models, Sobol scores were calculated for each inputs (4 for oral model) and (6 for dermal model). Three types of Sobol scores; first-order effect (FOE), second-order (SOE) and TE were calculated.
Figure 4 shows the Sobol scores for all four input variables of the model considering three age groups (children, teens and adults). Interesting point to be noted here is that all the first-order scores for four inputs have values less than zero. Since these values are negative, we cannot interpret them in terms of relative contributions to the variance. This may be overcome by increasing the sample size, and that could be the scope of further research in this area. As stated above, first-order score does not give any clear idea about each input contribution to the output of the model. Therefore, SOE (i.e. interaction effect) and TE were further estimated for oral model. For the FOE, the highest value was recorded for Cw followed by EF, IRw and BW. That clearly shows the relative importance of each features for estimation of oral risk value. But for the TE the inputs Cw (68.91%) and EF (68.68%) approximately shows the equal effect, whereas as BW has high Sobol score than the IRw. To know the interaction effects of each variable for risk value, SOE was calculated. The high value of interaction score was found for IRw–BW followed by Cw–IRw, Cw–IRw, EF–BW, Cw–EF, IRw–EF. This result reveals that IRw–BW scores are the important input parameters for the assessment of oral health risk than the Cw alone. Similar relative importance trends were also observed for others age groups as well. The interaction effects score was recorded high for Adults for IRw–BW followed by teens and children (Fig. 4).

Sensitivity analysis based on oral HQ model for different age groups considering first-order effect (FOE), second-order effect (SOE) and total effect (TE)
Figure 5 shows the Sobol scores of six variables for dermal model considering age groups (children, teens and adults). For all age groups, the highest value Sobol scores was found for the Cw followed by those of fraction of skin contact (F) and EF and BW. The ET values for FOE were found negative which indicated the presence of possible higher-order or interaction effects. In addition, skin surface area (SA) has no contribution for the determination of dermal risk value. For the FOE, the highest value was recorded for Cw followed by fraction of skin contact, EF and BW. This clearly shows the relative importance of each features for estimation of dermal risk value. For the TE the inputs Cw contributes 78.58% for adults; 78.43% teens 76.75% for children and Cw approximately shows the equal effect both teens and adults. The SOE shows interaction effects between the contributed variables. The higher value of interaction was found for the Cw -EF followed by Cw–ETS, Cw–SA. In addition, significant interaction effect (i.e. SOE) was found between Cw and SA, which was absent during FOE and TE. The higher value of Cw–SA was recorded for adults followed by teens and children. That shows the older age groups have more dermal risk than the younger age groups.

Sensitivity analysis based on dermal HQ model for different age groups considering first-order effect (FOE), second-order effect (SOE) and Total effect (TE)
Conclusions
In this research, a total of 456 groundwater samples were investigated to assess the fluoride concentrations of the study regions. Of the 456 groundwater samples taken from the five districts, 96% of the samples are within the maximum acceptable limit of WHO guidelines. The results of spatial distribution show that Nawada district has the high concentration of fluoride distribution. In addition, the eastern and south-eastern parts of the studied areas have the higher concentrations of fluoride with a few spots in the middle north and south-west. Groundwater in the southern and northern districts (Aurangabad, Gaya and Jahenabad and Nalanda) has a fluoride concentration of lower than 0.5 mg l−1 which is less than the WHO guidelines (WHO 2004) and leads to increased tooth decay. For the FOE, the highest value was recorded for Cw followed by EF, IRw and BW. This clearly showed the relative importance of each feature for estimation of oral risk value. However, for the TE, the inputs Cw (68.91%) and EF (68.68%) are approximately same. The Sobol score of BW was found to be higher than that of the IRw. For the interaction effect (SOE), the highest value was found for IRw–BW followed by Cw–IRw, Cw–IRw, EF-BW, Cw–EF, IRw–EF. This result revealed that IRw–BW effects are the important input parameters for the assessment of oral health risk. The highest Sobol scores were recorded for Adults followed by teens and children. The SOE values for dermal model showed that the fluoride concentration and skin surface area have significant contribution towards dermal risk value. In addition, the highest value of Cw–SA was recorded for adults followed by teens and children. This result revealed that the older age groups have more dermal risk than the younger age groups. The future scope of this research can be devoted to find the effects of exposure to fluoride through other ways of contact (e.g. food) with seasonal variation.
References
Adimalla N (2018) Groundwater quality for drinking and irrigation purposes and potential health risks assessment: a case study from semi-arid region of South India. Expo Health. https://doi.org/10.1007/s12403-018-0288-8
Adimalla N, Venkatayogi S (2017) Mechanism of fluoride enrichment in groundwater of hard rock aquifers in Medak, Telangana State, South India. Environ Earth Sci 76:45
Adimalla N, Li P, Qian H (2018a) Evaluation of groundwater contamination for fluoride and nitrate in semi-arid region of Nirmal Province, South India: a special emphasis on human health risk assessment (HHRA). Hum Ecol Risk Assess. https://doi.org/10.1080/10807039.2018.1460579
Adimalla N, Vasa SK, Li P (2018b) Evaluation of groundwater quality, Peddavagu in Central Telangana (PCT), South India: an insight of controlling factors of fluoride enrichment. Model Earth Syst Environ 4:841–852
Akiniwa K (1997) Re-examination of acute toxicity of fluoride. Fluoride 30:89–104
Apambire W, Boyle D, Michel F (1997) Geochemistry, genesis, and health implications of fluoriferous groundwaters in the upper regions of Ghana. Environ Geol 33:13–24
APHA (2005) Standard methods for the examination of water and wastewater. American Public Health Association (APHA), Washington, DC
Baghania AN, Mahvib AH, Rastkaric N, Delikhoond M, Hosseinie SS, Sheikhif R (2017) Synthesis and characterization of amino-functionalized magnetic nanocomposite (Fe3O4-NH2) for fluoride removal from aqueous solution. Desalin Water Treat 65:367–374
Barbier O, Arreola-Mendoza L, Del Razo LM (2010) Molecular mechanisms of fluoride toxicity. Chem Biol Interact 188:319–333
Bassin EB, Wypij D, Davis RB, Mittleman MA (2006) Age-specific fluoride exposure in drinking water and osteosarcoma (United States). Cancer Causes Control 17:421–428
Beg M, Srivastav S, Carranza E, de Smeth J (2011) High fluoride incidence in groundwater and its potential health effects in parts of Raigarh District, Chhattisgarh, India. Curr Sci 100:750–754
Chakraborti D, Das B, Murrill MT (2010) Examining India’s groundwater quality management. Environ Sci Technol 45(1):27–32
Chilton J et al (2006) Fluoride in drinking-water. World Health 408:613–693
Choi AL et al (2015) Association of lifetime exposure to fluoride and cognitive functions in Chinese children: a pilot study. Neurotoxicol Teratol 47:96–101
Cooper C, Wickham CA, Barker DJ, Jacobsen SJ (1991) Water fluoridation and hip fracture. Jama 266:513–514
Cronin AA, Prakash A, Priya S, Coates S (2014) Water in India: situation and prospects. Water Policy 16:425–441
Dehghani MH, Faraji M, Mohammadi A, Kamani H (2017) Optimization of fluoride adsorption onto natural and modified pumice using response surface methodology: isotherm, kinetic and thermodynamic studies. Korean J Chem Eng 34:454–462
Edmunds WM, Smedley PL (2013) Fluoride in natural waters. Essentials of medical geology. Springer, Berlin, pp 311–336
Epa U (2011) Exposure factors handbook 2011 edition (final). US Environmental Protection Agency, Washington, DC
Felsenfeld AJ, Robert M (1991) A report of fluorosis in the United States secondary to drinking well water. J Am Med Assoc 265:486–488
He S, Wu J (2018) Hydrogeochemical characteristics, groundwater quality and health risks from hexavalent chromium and nitrate in groundwater of Huanhe Formation in Wuqi County, northwest China. Expo Health 5:9. https://doi.org/10.1007/s12403-018-0289-7
He X, Wu J, He S (2018) Hydrochemical characteristics and quality evaluation of groundwater in terms of health risks in Luohe aquifer in Wuqi County of the Chinese Loess Plateau, northwest China. Hum Ecol Risk Assess. https://doi.org/10.1080/10807039.2018.1531693
Homma T, Saltelli A (1996) Importance measures in global sensitivity analysis of nonlinear models. Reliab Eng Syst Saf 52:1–17
Huang D, Yang J, Wei X, Qin J, Ou S, Zhang Z, Zou Y (2017) Probabilistic risk assessment of Chinese residents’ exposure to fluoride in improved drinking water in endemic fluorosis areas. Environ Pollut 222:118–125
IPCS (2012) Environmental health criteria 227: fluorides Effects of ingested fluoride. National Academy Press, Geneva
Jacks G, Bhattacharya P, Chaudhary V, Singh K (2005) Controls on the genesis of some high-fluoride groundwaters in India. Appl Geochem 20:221–228
Jacobson J, Weinstein L (1977) Sampling and analysis of fluoride: methods for ambient air, plant and animal tissues, water, soil and foods. J Occup Environ Med 19:79–87
Karami A et al (2017) Application of response surface methodology for statistical analysis, modeling, and optimization of malachite green removal from aqueous solutions by manganese-modified pumice adsorbent. Desalin Water Treat 89:150–161
Karthikeyan G, Shunmugasundarraj A (2000) Isopleth mapping and in situ fluoride dependence on water quality in the Krishnagiri block of Tamil Nadu in South India. Fluoride 33:121–127
Khorsandi H, Mohammadi A, Karimzadeh S, Khorsandi J (2016) Evaluation of corrosion and scaling potential in rural water distribution network of Urmia, Iran. Desalin Water Treat 57:10585–10592
Kohn WG, Maas WR, Malvitz DM, Presson SM, Shaddix KK (2001) Recommendations for using fluoride to prevent and control dental caries in the United States. Morbid Mortal. Wkly Rep. 50, No. RR-14. http://www.cdc.gov/mmwr/
Kumar S, Lata S, Yadav J, Yadav J (2017) Relationship between water, urine and serum fluoride and fluorosis in school children of Jhajjar District, Haryana, India. Appl Water Sci 7:3377–3384
Kumar D, Singh A, Jha RK, Sahoo SK, Jha V (2018) Using spatial statistics to identify the uranium hotspot in groundwater in the mid-eastern Gangetic plain, India. Environ Earth Sci 77:702
Li P, Qian H, Wu J, Chen J, Zhang Y, Zhang H (2014) Occurrence and hydrogeochemistry of fluoride in shallow alluvial aquifer of Weihe River, China. Environ Earth Sci 71(7):3133–3145
Li P, Li X, Meng X, Li M, Zhang Y (2016) Appraising groundwater quality and health risks from contamination in a semiarid region of northwest China. Expo Health 8(3):361–379. https://doi.org/10.1007/s12403-016-0205-y
Li P, He X, Li Y, Xiang G (2018) Occurrence and health implication of fluoride in groundwater of loess aquifer in the Chinese Loess Plateau: a case study of Tongchuan. Expo Health, Northwest China. https://doi.org/10.1007/s12403-018-0278-x
Maithani P, Gurjar R, Banerjee R, Balaji B, Ramachandran S, Singh R (1998) Anomalous fluoride in groundwater from western part of Sirohi district, Rajasthan and its crippling effects on human health. Curr Sci 74(9):773–777
Marya CM, Ashokkumar B, Dhingra S, Dahiya V, Gupta A (2014) Exposure to high-fluoride drinking water and risk of dental caries and dental fluorosis in Haryana, India. Asia Pac J Public Health 26:295–303
Miller G, Egyed M, Shupe J (1977) Alkaline phosphatase activity, fluoride citric acid, calcium, and phosphorus content in bones of cows with osteoporosis. Fluoride 10:76
Miri M, Allahabadi A, Ghaffari HR, Fathabadi ZA, Raisi Z, Rezai M, Aval MY (2016) Ecological risk assessment of heavy metal (HM) pollution in the ambient air using a new bio-indicator. Environ Sci Pollut Res 23:14210–14220
Narsimha A, Sudarshan V (2017) Contamination of fluoride in groundwater and its effect on human health: a case study in hard rock aquifers of Siddipet, Telangana State, India. Appl Water Sci 7:2501–2512
NAS (1971) Fluorides, committee on biological effects of atmospheric pollutants. National Academy of Sciences, Washington, DC. p 295
Ozsvath DL (2009) Fluoride and environmental health: a review. Rev Environ Sci Biotechnol 8:59–79
Petersen PE (2004) Challenges to improvement of oral health in the 21st century: the approach of the WHO Global Oral Health Programme. Int Dent J 54:329–343
Podgorny PC, McLaren L (2015) Public perceptions and scientific evidence for perceived harms/risks of community water fluoridation: an examination of online comments pertaining to fluoridation cessation in Calgary in 2011. Can J Pub Health 106:e413–e425
Riggs BL et al (1990) Effect of fluoride treatment on the fracture rate in postmenopausal women with osteoporosis. N Engl J Med 322:802–809
Rostamia I, Mahvib AH, Dehghanib MH, Baghania AN, Marandid R (2017) Application of nano aluminum oxide and multi-walled carbon nanotube in fluoride removal. Desalination 1:6
Saltelli A, Tarantola S, Chan K-S (1999) A quantitative model-independent method for global sensitivity analysis of model output. Technometrics 41:39–56
Samal AC, Bhattacharya P, Mallick A, Ali MM, Pyne J, Santra SC (2015) A study to investigate fluoride contamination and fluoride exposure dose assessment in lateritic zones of West Bengal, India. Environ Sci Pollut Res 22:6220–6229
Saxena V, Ahmed S (2001) Dissolution of fluoride in groundwater: a water-rock interaction study. Environ Geol 40:1084–1087
Singh A, Jolly S, Bansal B, Mathur C (1963) Endemic fluorosis: epidemiological, clinical and biochemical study of chronic fluorine intoxication In Panjaei (India). Medicine 42:229–246
Sobol IM (1993) Sensitivity estimates for nonlinear mathematical models. Math Model Comput Exp 1:407–414
Staff E (2001) Supplemental guidance for developing soil screening levels for superfund sites, Peer review Draft Washington, DC: US Environmental Protection Agency Office of Solid Waste and Emergency Response, OSWER:9355.9354–9324
Subba Rao N, Prakasa Rao J, Nagamalleswara Rao B, Niranjan Babu P, Madusudhana Reddy P, Devadas DJ (1998) A preliminary report on fluoride content in groundwaters of Guntur area, Andhra Pradesh, India. Curr Sci 75:887–888
Tang Q-q DuJ, H-h Ma, S-j Jiang, X-j Zhou (2008) Fluoride and children’s intelligence: a meta-analysis. Biol Trace Elem Res 126:115–120
USEPA (1992) Guidelines for exposure assessment. Fed Reg 57:22888–22938
WHO (2004) IPCS risk assessment terminology. World Health Organization, Geneva
WHO (2011) Guidelines for drinking-water quality. WHO Chron 38:104–108
Wu J, Sun Z (2016) Evaluation of shallow groundwater contamination and associated human health risk in an alluvial plain impacted by agricultural and industrial activities, mid-west China. Expo Health 8:311–329
Wu J, Li P, Qian H (2015) Hydrochemical characterization of drinking groundwater with special reference to fluoride in an arid area of China and the control of aquifer leakage on its concentrations. Environ Earth Sci 73:8575–8588
Yadav AK, Abbassi R, Gupta A, Dadashzadeh M (2013) Removal of fluoride from aqueous solution and groundwater by wheat straw, sawdust and activated bagasse carbon of sugarcane. Ecol Eng 52:211–218
Yang K, Liang X (2011) Fluoride in drinking water: effect on liver and kidney function. In: Nriagu Jerome O (ed) Encyclopedia of Environmental Health. Elsevier, Amsterdam, pp 769–775
Zhang XY, Trame M, Lesko L, Schmidt S (2015) Sobol sensitivity analysis: a tool to guide the development and evaluation of systems pharmacology models. CPT Pharmacometrics Syst Pharmacol 4:69–79
Zhang S et al (2016) Excessive apoptosis and defective autophagy contribute to developmental testicular toxicity induced by fluoride. Environ Pollut 212:97–104
Acknowledgements
This work was supported by the Board of Research and Nuclear Sciences through the Department of Atomic Energy, India for providing financial assistance under the National Uranium project (NUP) (BRNS Project Ref. No.: 36(4)/14/10/2014-BRNS). The authors are also profoundly grateful to the reviewers and the associate editor for the careful examination of the draft of the manuscript and their many valuable comments and suggestions to help improve the manuscript.
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the Board of Research and Nuclear Sciences under Department of Atomic Energy, India.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Kumar, D., Singh, A., Jha, R.K. et al. A Variance Decomposition Approach for Risk Assessment of Groundwater Quality. Expo Health 11, 139–151 (2019). https://doi.org/10.1007/s12403-018-00293-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12403-018-00293-6