
Abstract
Background
18F-florbetapir PET is emerging as an excellent quantitative tool to quantify cardiac light chain (AL) amyloidosis burden. The primary aim of this study was to determine interobserver reproducibility and intraobserver repeatability, defined per the recommendations of the Quantitative Imaging Biomarker Alliance technical performance group, of PET 18F-florbetapir retention index (RI) in patients with cardiac AL amyloidosis.
Methods
The study cohort comprised 37 subjects with systemic AL amyloidosis enrolled in the prospective study: Molecular Imaging of Primary Amyloid Cardiomyopathy (clinical trials.gov NCT: 02641145). Using 10 mCi of 18F-florbetapir, a 60-minute dynamic cardiac scan was acquired. Global and segmental left ventricular estimates of retention index (RI) of 18F-florbetapir were calculated (Carimas 2.9 software, Turku, Finland). RI was analyzed twice, at least 24 hours apart, by two independent observers. Intraobserver repeatability and interobserver reproducibility were evaluated using Bland–Altman plots and scatter plots with fitted linear regression curves.
Results
All reproducibility (interobserver, r = 0.98) and repeatability (intraobserver, R=0.99 for each observer) measures of 18F-florbetapir RI are excellent. On the Bland–Altman plots, the agreement limits for global 18F-florbetapir RI were high and ranged for reproducibility (interobserver) from − 9.3 to + 9.4% (Fig. 1), and for repeatability (observer 1 from − 10.8 to + 10.7% and from − 9.2 to + 11.4%, for observer 2).
Conclusions
The present study showed excellent interobserver reproducibility and intraobserver repeatability of 18F-florbetapir PET retention index in patients with cardiac AL amyloidosis.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Amyloidoses are a group of disorders characterized by the localized or systematic deposition of misfolded extracellular proteins into organs or tissues in the form of beta-pleated sheets of insoluble amyloid fibrils. Cardiac light chain (AL) amyloidosis is marked by amyloid fibril deposition in the heart, frequently leading to highly fatal AL amyloid cardiomyopathy (AL-CMP).1 The gravity of this illness has motivated a surge in clinical trials of novel therapies for AL-CMP.2,3,4,5 There has been substantial improvement in the diagnosis and imaging of cardiac amyloidosis in recent years. Despite these positive steps, evaluation of therapeutic breakthroughs for this disease is currently limited because imaging advances have lagged behind drug development.5 In fact, the lack of reproducible, validated and quantitative in vivo imaging tools has become a major obstacle to the development of novel anti-amyloid therapies for the heart.
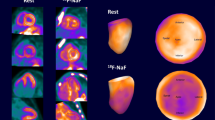
18F-florbetapir, a radiotracer originally developed for detection of beta amyloid imaging in the brain, has been shown to specifically bind to myocardial AL deposits in vitro and in vivo.6,718F-florbetapir positron emission tomography (PET)/CT is a promising technique to quantify cardiac AL burden and measure changes in myocardial amyloid load in response to therapy. Repeatability and reproducibility are critical aspects of performance of a quantitative imaging biomarker8; however, no previous studies have examined the reproducibility and repeatability of quantitative 18F-florbetapir PET/CT in cardiac AL amyloidosis.
The primary aim of this study was to determine interobserver reproducibility and intraobserver repeatability of cardiac PET 18F-florbetapir retention index (RI)9 in patients with systemic AL amyloidosis using the Carimas 2.9 analysis software. Our definitions comply with the recommendations of the QIBA (Quantitative Imaging Biomarker Alliance) technical performance group, which is defining standard performance analysis methods for imaging biomarkers.8
Methods
Patient Selection
We studied 37 subjects with systemic AL amyloidosis diagnosed by fat pad, bone marrow, renal or endomyocardial biopsy. All subjects were enrolled in the prospective study, Molecular Imaging of Primary Amyloid Cardiomyopathy (clinical trials.gov NCT: 02641145). Inclusion criteria for the study were: age > 18 years, elevated free light chains or abnormal Kappa/Lambda ratio, an eGFR greater than 30 mL/min/m2 within 14 days of study enrollment, and no contraindications to cardiac magnetic resonance (CMR) imaging, and enrolled intro three groups (1) Active AL Cardiac: elevated age-adjusted NT-ProBNP or a cTnT greater than or equal to 0.01 ng/mL; (2) Remission AL Cardiac: documented active systemic AL amyloidosis with cardiac involvement and hematological remission or very good partial remission for > 1 year prior; and (3) Active AL Non-cardiac: active systemic AL with normal cardiac biomarkers and normal left ventricular wall thickness. This study was approved by Partners Human Research Committee. All participants provided written, informed consent.
PET/CT Scan Protocol
All subjects underwent a low-dose CT transmission scan (10 mA, 120 kVp, free tidal breathing), followed by a 60-minute dynamic list-mode cardiac PET/CT scan. PET image acquisition began one minute before intravenous tracer injection of 18F-florbetapir (mean 9.19 mCi, range 5.84-13.24 mCi); cardiac imaging was performed with arms raised above the head. Emission data were constructed into 38 or 47 dynamic frames (12 × 5, 6 × 10, 4 × 30, 6 × 60, 10 × 300 seconds or 20 × 5, 8 × 10, 6 × 30, 4 × 60, 8 × 300, 1 × 600 seconds).
Image Analysis
De-identified 18F-florbetapir PET cardiac images were analyzed using the semi-automatic Carimas software package (version 2.9, Turku PET Centre, Finland), an open access software that can be downloaded at no charge. Each image was analyzed twice, at least 24 hours apart, by each of two independent observers. Observers were both novices to nuclear cardiology and 18F-florbetapir image analysis and received the same training. Images for each patient were de-identified and uploaded into the software for reorientation and definition of long and short axes. Software generated left ventricular (LV) myocardial contours were manually adjusted, and the blood pool input function was obtained from a region in the left atrium to avoid myocardial spillover. Global and 17-segment left ventricular18F-florbetapir RI, as defined in Dorbala et al.,9 were calculated.
Statistical Analysis
Interobserver reproducibility was determined using the average of analyses 1 and 2 for each observer. Intraobserver repeatability and interobserver reproducibility were quantified using the percent differences between measurements. Bland–Altman plots and scatter plots with fitted linear regression curves were created for intraobserver and interobserver measurements. Pearson’s correlation coefficients (r) were calculated for intraobserver and interobserver measurements. Reliability of inter and intraobserver measures were calculated using intraclass correlation coefficients (ICC).
Results
The mean age of the study cohort was 62 ± 6 years; 46% were female (N = 17). The mean body mass index was 26.80 ± 3.8 kg/m2 and the mean estimated glomerular filtration rate was 55.5 ± 11.5 mL/min/1.73 m2.
Intraobserver Repeatability
Correlation between each observer’s initial and repeated measurements of 18F-florbetapir RI was excellent (r > 0.95), as shown in Table 1.
Interobserver Reproducibility
Correlation between segmental and global 18F-florbetapir RI measurements of observer 1 and observer 2 was excellent (r > 0.92), as shown in Table 1.
Inter- and Intraobserver Agreement
All reproducibility (interobserver) and repeatability (intraobserver) measures of 18F-florbetapir RI are very high. Correlation of interobserver global 18F-florbetapir RI values is high (r = 0.98, Figure 1) while the correlation for observers 1 and 2 are also high (r = 0.99, Figures 2 and 3). On the Bland–Altman plots, the agreement limits for global 18F-florbetapir RI were high and ranged for reproducibility (interobserver) from − 9.3 to + 9.4 % (Figure 1), and for repeatability (observer 1 from − 10.8 to + 10.7%, Figure 2 and for observer 2 from − 9.2 to + 11.4%, Figure 3). Differences for segmental 18F-florbetapir RI reproducibility (interobserver) and repeatability (intraobserver) measurements were minimal and shown in Figure 4A–C.

A, B Interobserver reproducibility of global 18F-florbetapir retention index. Reproducibility (interobserver variability) of global 18F-florbetapir retention indexes was assessed by Bland–Altman plot (A) and scatter plot with fitted linear regression (B). 95% confidence intervals (dotted lines) and mean (solid line) are shown. Markers represent Active AL Non-cardiac (open circles), Remission AL Cardiac (solid circles) and Active AL Cardiac (solid squares)

A, B Repeatability of global 18F-florbetapir retention index: Observer 1. Repeatability (intraobserver variability) of global 18F-florbetapir retention indexes was assessed by Bland–Altman plot (A) and scatter plot with fitted linear regression (B). 95% confidence intervals (dotted lines) and mean (solid line) are shown. Markers represent Active AL Non-cardiac (open circles), Remission AL Cardiac (solid circles) and Active AL Cardiac (solid squares)

A, B Repeatability of global 18F-florbetapir retention index: Observer 2. Repeatability (intraobserver variability) of global 18F-florbetapir retention indexes was assessed by Bland–Altman plot (A) and scatter plot with fitted linear regression (B). 95% confidence intervals (dotted lines) and mean (solid line) are shown. Markers represent Active AL Non-cardiac (open circles), Remission AL Cardiac (solid circles) and Active AL Cardiac (solid squares)

A-C Repeatability and reproducibility of segmental 18F-florbetapir retention indexes. Repeatability (intraobserver, A) and reproducibility (interobserver, B. Observer 1, C. Observer 2) of 17 segmental 18F-florbetapir retention indexes showed no systematic bias for any specific myocardial segments (1-17 as defined by the American Heart Association)
Reliability of Measurements
Inter and intraobserver measurements of global 18F-florbetapir RI were highly reliable with intraclass correlation coefficient (ICC) of > 0.99 (Figure 5A–C).

A-C Reliability of global of segmental 18F-florbetapir retention indexes. These figures show that the reliability, estimated by intraclass correlation coefficient (ICC), of interobserver (A) and intraobserver (B, Observer 1, and C, Observer 2) measures of global 18F-florbetapir retention indexes is excellent
Discussion
This study, the first to the best of our knowledge, aimed to assess the intraobserver repeatability, interobserver reproducibility of left ventricular myocardial 18F-florbetapir RI in cardiac AL amyloidosis at a global and segment level. Intraobserver repeatability- and interobserver reproducibility of 18F-florbetapir RI in cardiac AL amyloidosis assessed using Carimas software was excellent at both global and segmental levels. Moreover, Pearson’s correlation coefficients were all above 0.92, indicating high correlation between intraobserver and interobserver repeat measurements. Graphical analysis similarly indicated excellent agreement. Bland–Altman coefficients of reproducibility were small, indicating the minimum absolute difference between 2 measurements is similarly small. Quantifying the repeatability and reproducibility of measurement of myocardial retention of 18F-florbetapir by a single or by two different observers is important to assess changes in disease burden following therapy. Global as well as segmental measurements are important as early changes in response to therapy may be more evident at a segmental level than at a global level.
With this software-based approach, minimal manual editing of the myocardial contours was required, and all parameters studied showed excellent agreement within and between observers both at the global and segmental levels. These findings are promising for clinical application because through using this freely available software, the quantification of amyloid burden is minimally affected by intra- and interobserver variability and can be identified by either one or more observers with minimal training.
Comparing the results of this study to previous studies shows the robustness of PET repeatability analysis. A 2015 study conducted by Nesterov et al. aimed to analyze C-11 acetate inter- and intraobserver reproducibility using Carimas. High inter- and intraobserver repeatability measures were similarly found at the global and segmental levels.10 While there has been little research done using the radiotracer 18F-florbetapir, the repeatability of other radiotracers for cardiac amyloidosis has been tested. For example, Kero et al. used 11C-PIB to measure the left ventricular RI in patients with cardiac amyloidosis. Intraobserver reproducibility was similarly determined to be very good and it was concluded that Carimas is an effective software to analyze the 11C-PIB retention index in amyloidosis patients.11 The results of the current study show a comparable repeatability using 18F-florbetapir as the radiotracer.
Strengths and Limitations
Patients were enrolled in this prospective study based on previously defined study criteria, reducing patient selection bias. We performed a quantitative imaging test using 18F-florbetapir as a radiotracer to determine left ventricular myocardial amyloid burden in subjects with AL cardiac amyloidosis. The software used to quantify amyloid burden, Carimas, has been previously validated. However, it is difficult to account for partial volume and spillover effects of radiotracer using this software. Our study attempted to minimize the effects of spillover by placing the blood pool input in the left atrium rather than the left ventricle. Other limitations are that image-derived whole blood, rather than plasma, input functions were used, and that metabolite corrections were not performed. Additionally, inter-study variability to measure physiological variability within subjects is critical to define thresholds to assess response to therapy, and they were not assessed in this cohort.
Conclusion
The present study showed excellent intraobserver repeatability and interobserver reproducibility in measurement of myocardial 18F-florbetapir PET retention index in patients with cardiac AL amyloidosis using Carimas software. Further analysis of inter-study variability is needed to define the magnitude of RI change that can be considered clinically significant. Once this value is determined, physicians will be able to better assess patient response to therapy in patients with AL cardiomyopathy.
New Knowledge Gained
This study demonstrated excellent intraobserver repeatability and interobserver reproducibility in measurement of myocardial 18F-florbetapir PET retention index using Carimas software in patients with cardiac AL amyloidosis.
Abbreviations
- AL:
-
Light chain
- AL-CMP:
-
Light chain amyloidosis with cardiomyopathy
- PET:
-
Positron imaging tomography
- RI:
-
Retention index
- LV:
-
Left ventricle
- NT-ProBNP:
-
N-terminal pro b-type natriuretic peptide
- CTnT:
-
Cardiac troponin T
- eGFR:
-
Estimated glomerular filtration rate
- MICA:
-
Molecular Imaging of Primary Amyloid Cardiomyopathy
References
Falk RH, Alexander KM, Liao R, Dorbala S. AL (light-chain) cardiac amyloidosis: A review of diagnosis and therapy. J Am Coll Cardiol. 2016;68:1323–41.
Ruberg FL, Berk JL. Transthyretin (TTR) cardiac amyloidosis. Circulation. 2012;126:1286–300.
Richards DB, Cookson LM, Berges AC, Barton SV, Lane T, Ritter JM, et al. Therapeutic clearance of amyloid by antibodies to serum amyloid P component. N Engl J Med. 2015;373:1106–14.
Gertz MA, Landau H, Comenzo RL, Seldin D, Weiss B, Zonder J, et al. First-in-human phase I/II study of NEOD001 in patients with light chain amyloidosis and persistent organ dysfunction. J Clin Oncol. 2016;34:1097–103.
Dorbala S, Kijewski MF, Park MA. Quantitative molecular imaging of cardiac amyloidosis: The journey has begun. J Nucl Cardiol. 2016;23:751–3.
Park MA, Padera RF, Belanger A, Dubey S, Hwang DH, Veeranna V, et al. 18F-florbetapir binds specifically to myocardial light chain and transthyretin amyloid deposits: Autoradiography study. Circ Cardiovasc Imaging. 2015;8:e002954.
Dorbala S. Imaging cardiac amyloidosis: An opportunity for nuclear cardiology. J Nucl Cardiol. 2014;21:1043–4.
Raunig DL, Mcshane LM, Pennello G, Gatsonis C, Carson PL, Voyvodic JT, et al. Quantitative imaging biomarkers: A review of statistical methods for technical performance assessment. Stat Methods Med Res. 2014;24:27–67.
Dorbala S, Vangala D, Semer J, Strader C, Bruyere JR Jr, Di Carli MF, et al. Imaging cardiac amyloidosis: A pilot study using (18)F-florbetapir positron emission tomography. Eur J Nucl Med Mol Imaging. 2014;41:1652–62.
Nesterov SV, Turta O, Han C, Maki M, Lisinen I, Tuunanen H, et al. C-11 acetate has excellent reproducibility for quantification of myocardial oxidative metabolism. Eur Heart J Cardiovasc Imaging. 2015;16:500–6.
Kero T, Lindsjo L, Sorensen J, Lubberink M. Accurate analysis and visualization of cardiac (11)C-PIB uptake in amyloidosis with semiautomatic software. J Nucl Cardiol. 2016;23:741–50.
Disclosure
RHF has received consulting fees from Ionis Pharmaceuticals and Alnylam Pharmaceuticals and research funding from GlaxoSmithKline. SD serves as a consultant for Proclara, Pfizer, AAA, and GEHC and has received research funds from Pfizer. The other authors do not have any conflicts to disclose.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The authors of this article have provided a PowerPoint file, available for download at SpringerLink, which summarizes the contents of the paper and is free for re-use at meetings and presentations. Search for the article DOI on SpringerLink.com.
The authors have also provided an audio summary of the article, which is available to download as ESM, or to listen to via the JNC/ASNC Podcast.
Funding
SD and RF are supported by NIH RO1 Grant (RO1 HL 130563); SD is supported by American Heart Association Grant (AHA 16 CSA 2888 0004).
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Nodoushani, A., El-Sady, M.S., Park, MA. et al. Reproducibility and Repeatability of Assessment of Myocardial Light Chain Amyloidosis Burden Using 18F-Florbetapir PET/CT. J. Nucl. Cardiol. 28, 2004–2010 (2021). https://doi.org/10.1007/s12350-019-01961-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12350-019-01961-z