
Abstract
Background
This study aimed to validate the reproducibility of quantitative analysis using time-of-flight (TOF) and conventional PET with 13N-ammonia (13N-NH3).
Methods and Results
Phantom images were reconstructed with and without TOF, and recovery coefficients (RCs) and the percent contrast of each sphere over the percent background variability were assessed. In the clinical study, 21 subjects underwent dynamic 13N-NH3 PET scanning under stress and rest conditions. The dynamic acquisition images and intra- and inter-observer reproducibility of myocardial blood flow (MBF) and coronary flow reserve (CFR) were compared between reconstructions (with and without TOF). In the phantom study, RCs and the percent contrast of each sphere over the percent background variability was improved with TOF. In the clinical study, the noise of blood pool and myocardial images with TOF was less than that without TOF. Territorial and global intra- and inter-observer reproducibility of MBF and CFR values was excellent. Although segmental intra- and inter-observer reproducibility was excellent, there were larger variations in apex and the segment near the right ventricle (RV) without TOF. These variations became inconspicuous with TOF.
Conclusion
Visual image quality, RCs, and percent contrast over percent background variability with TOF were better than that without TOF. Excellent correlations and good agreements in quantitative values were observed. TOF improved the variation of segmental values.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Non-invasive regional quantification of myocardial blood flow (MBF) and coronary flow reserve (CFR) is obtained by myocardial perfusion imaging using PET/CT with 13N-ammonia (13N-NH3).1 13N-NH3 PET was set as class I of evidence level by the American College of Cardiology (ACC), American Heart Association (AHA), American Society of Nuclear Cardiology (ASNC), and the Japanese Circulation Society (JCS) for the diagnosis of coronary artery disease and the assessment of its severity.2,3 Absolute quantification of MBF and CFR has incremental values in the evaluation of the prognosis for patients with cardiovascular disease. In comparison to SPECT, PET offers better accuracy and sensitivity by higher spatial resolution, and more accurate attenuation and scatter correction.4 Recently, as clinical use of 13N-NH3 PET studies has increased, quantitative analysis of MBF and CFR adding to visual assessment is required.
There has been a growing interest in the use of the 3-dimensional (3D) mode acquisition and time-of-flight (TOF) technology that has also gained popularity in clinical oncology PET studies.5 TOF comprises the difference in arrival times between a pair of coincident photons, thus narrowing the probability distribution of the location of the annihilation event along the line of response (LOR). Compared with conventional PET, TOF-PET improves the signal-to-noise ratio.6,7 There are few reports of 13N-NH3 myocardial PET using TOF information. In this paper, we evaluated the image quality, recovery coefficients (RCs), and reproducibility of quantitative values in TOF and conventional PET with 13N-NH3.
Materials and Methods
Data Acquisition, Image Reconstruction and Processing
All data were obtained using the GEMINI-TF16 (Philips Healthcare, Cleveland, USA), a fully 3D TOF-PET scanner combined with a 16-slice Brilliance CT scanner. This scanner demonstrates the 12% energy resolution and a timing resolution of 585 ps. The dimensions of the individual LYSO crystals are 4 × 4 × 22 mm3 in size and the measured spatial resolution of the system is 4.8 mm. First, a CT scan (over 180 mm using 120 kV, 115 mAs/slice, 1.5 s/rotation, and a pitch of 0.438) was performed, and then, images were reconstructed to produce 3.0-mm-thick slices at 3.0-mm increments. All emission data were acquired in 3D list-mode. Images were reconstructed using a blob-based, list-mode iterative algorithm with TOF information [TOF-ordered subset expectation maximization (TOF-OSEM)], and without TOF [3-dimmensional raw action maximum likelihood algorithm (3D-RAMLA)]. The reconstruction parameters for TOF-OSEM were three iterations, 33 subsets, and a relaxed (λ = 1) OSEM update equation, and for 3D-RAMLA were two iterations, 33 subsets, and a relaxed (λ = 0.08) OSEM update equation. Data were corrected by normalization with the application of the dead time and the attenuation. Attenuation correction was performed using the CT transmission while scatter was estimated by the single scatter simulation. Random values were estimated by the delayed coincidence window method. All images were reconstructed in a 144 × 144 × 144 image grid of 4 × 4 × 4 mm3.
Phantom Study
Phantom
Two different diameter sizes (30 and 50 cm) of NU2 image quality phantom (Itoi Factory Kobe, Japan) of the National Electrical Manufactures Association (NEMA) were used in this study. Both phantoms had an interior length of 18 cm and contained six spheres of 10, 13, 17, 22, 28, and 37 mm diameters. All spheres were filled with hot solution. The background was filled with 1:4 warm activity concentrations of 5.3 kBq·mL−1 18F.
Data acquisition for the phantom study
Data acquired from 30-min list-mode in a noise-free condition were reconstructed with and without TOF (TOF-OSEM and 3D-RAMLA) in order to measure RCs. The RC for each diameter sphere was calculated as follows:
PET images of 5, 10, 30, and 60 seconds were reconstructed and the image quality was evaluated for each duration time with percent contrast/percent background variability of 10, 13, 17, and 22 mm diameters, respectively. Twelve region-of-interests (ROIs) of the same size to the spheres were drawn over the background. ROIs were drawn on the central slice, and ±1 and ±2 cm on either side of center, resulting in a total of 60 background ROIs, 12 on each of the five slices. The percent contrast for each diameter sphere (Q jmm ) was calculated as follows:
C H,j and C B,j refer to the average measured activity in the ROIs for each diameter sphere and the average measured activity in all the background diameter ROIs; a H/a B refers to the activity concentration ratio for the hot sphere to the background.
The percent background variability N jmm for each diameter sphere was calculated as follows:
SD jmm was the standard deviation (SD) of the background ROIs for each diameter sphere, calculated as follows:
Clinical Study
Subjects
This was a retrospective study of subjects referred for myocardial perfusion imaging with 13N-NH3 PET. The study population consisted of eight healthy volunteers (5 men and 3 women; mean age, 50.6 ± 14.0 years [range, 26-75 years]) and 13 patients with cardiovascular diseases (8 men and 5 women; mean age, 67.1 ± 10.0 years [range, 45-81 years]). All patients were studied at rest and during hyperemia induced by the intravenous injection of adenosine. Patients refrained from caffeine-containing drinks and smoking for 24 hours before the study. Baseline characteristics of the subjects are detailed in Table 1. Rest and peak heart rate, and rest and minimum blood pressure during adenosine infusion are listed in Table 2. The institutional ethics committee approved this study. All patients signed the written informed consent forms before study enrollment.
Data acquisition for the clinical study
PET scanning was performed after a slow intravenous injection of 370 MBq 13N-NH3 followed by a 30 mL saline solution (2.0 mL/s-15 seconds). Twenty-seven dynamic frames were reconstructed (twenty-four 5 seconds, two 30 seconds, and one 1 minute). One hour later after decay, a pharmacologic stress test was performed with the injection of adenosine (120 μg·kg−1·min−1 × 6 minutes). Subjects breathed freely during both the CT and PET acquisitions.
MBF and CFR Analysis
Quantitative values were analyzed with the PMOD software (PMOD Technologies Ltd., Zurich, Switzerland). The images were reoriented to standard short-axis for the definition of myocardial segments and volume-of-interests (VOIs). These VOIs were required for calculations of the time activity curves (TACs) of the right ventricle (RV) and the left ventricle (LV) blood pool and the myocardium. The LV-TACs served as the input curves, while the RV-TACs were applied for spillover correction in the septal segments. Only the first 4 minutes after injection were used for curve fitting. TACs of myocardia were fitted with the kinetic model using the DeGrado’s 1-compartment model, which was recommended to use the only first 4 minutes of data after injection of the tracer to reduce motion effects.8 Results of MBF and CFR were expressed in each territory and segment based on AHA’s 17 segment model. Territorial and global values were summarized by volume-weighted averaging to the vascular territories (RCA, LAD, and LCX) and global LV myocardium.
All frames during 0-40 seconds of blood volume and during 120-240 seconds of myocardium were averaged and smoothed with a 3D Gaussian filter of 6-mm full-width at half maximum (FWHM). In addition, a fraction of the blood volume image was subtracted in order to improve the contrast in myocardial images. For the blood factor, 0.05 was used in this study because the noise characteristics in 3D-PET were superior to conventional 2D-PET.
Intra-observer analyses of MBF and CFR were performed at intervals of a few months. Inter-observer analyses by two observers were operated after independent reviews. Both observers had enough experience about using the PMOD software.
Analysis of Dynamic PET Images
A comparison of the variability of the dynamic data between with and without TOF was conducted. ROIs of RV and LV blood pool were set in 5-seconds images from injection to 60 seconds, while septal, apical, and lateral myocardial walls of LV were set in 5-s images from 60 to 115 seconds. SD of ROIs was compared between with and without TOF.
Statistical Analysis
The results were expressed as mean ± SD. A paired Student’s t test was used to compare the quantitative data with and without TOF in intra- and inter-observer analyses. A Pearson’s product moment correlation coefficient and Bland-Altman plots were used to validate correlation and agreement of quantitative values in intra- and inter-observer analyses. A P value of <.01 was considered as statistically significant.
Results
Phantom Study
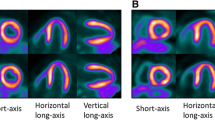
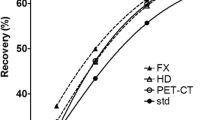
The image quality of NEMA NU2 phantoms of the 30 and 50 cm diameter with and without TOF reconstruction is shown in Figure 1. Reconstructed images with TOF had less noise compared to those without TOF. The smaller sphere’s accumulation was underestimated with both reconstructions. Moreover, the decrease of accumulation in small spheres was more noticeable in the 50-cm-diameter phantom. Figure 2 shows the RC curves against the sphere diameter measured in both sizes of phantoms with and without TOF reconstructions. The maximum measured radioactivity concentration decreased as the sphere’s size became smaller. RCs ranged from 1.06 to 0.45 depending on the diameter of the spheres in the standard size (30 cm) phantom with TOF, while from 1.03 to 0.38 without TOF. RCs were 0.43 (with TOF) and 0.26 (without TOF) on 10-mm-diameter spheres in the large (50 cm) phantom. RCs were strongly dependent on the use of TOF reconstruction. RCs of the large phantom were smaller than those of standard size phantom. Additionally, there was higher percent contrast/percent background variability of all spheres with TOF in each duration time (Figure 3).

Representative images of standard (30 cm) and large (50 cm) NEMA phantoms with and without TOF

Recovery coefficients for hot spheres of various diameters with TOF (red) and without TOF (blue) obtained from noise-free scans in standard φ: 30-cm (top) and larger φ: 50-cm (bottom) phantoms

Percent contrast/percent background variability of 10, 13, 17, and 22 mm diameters of various duration times
Clinical Study
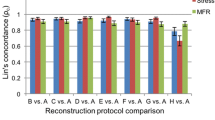
Representative trans-axial images with and without TOF of every three frames from the 2nd frame (10 seconds) are shown in Figure 4. The noise of blood pool and myocardial images with TOF was less than that without TOF in all frames. Tables 3 and 4 show SD of ROIs with and without TOF under stress and rest conditions. The less variation was observed with TOF images than that without TOF images. Mean and SD for territorial and global values with and without TOF in intra- and inter-observer analyses are shown in Table 5. Global stress and rest MBF and CFR in intra- and inter-observer analyses were statistically similar (all p = ns). When compared with and without TOF, the measured MBF was significantly larger with TOF, especially at rest condition. Consequently, CFR values with TOF were lower than those without TOF. In intra-observer analysis, a Pearson’s product moment correlation coefficient for territorial MBF values and CFR values under stress (n = 60) and rest (n = 63) tests with and without TOF indicated excellent correlations (stress MBF: r = 0.99 and 0.99, rest MBF: r = 0.97 and 0.97, and CFR: r = 0.99 and 0.98, all P < .0001). Excellent correlations were also observed with and without TOF in inter-observer analyses (stress MBF: r = 0.99 and 0.99, rest MBF: r = 0.98 and 0.97, and CFR: r = 0.98 and 0.99, all P < .0001). Figures 5, 6, 7, and 8 show segmental correlation coefficient analyses and Bland-Altman plots for intra- and inter-observer with and without TOF. Correlations and agreements of quantitative values were almost excellent, except in some segments without TOF reconstruction in intra- and inter-observer analyses; TOF improved the difference and agreement. Figures 9 and 10 show the differences of MBF and CFR values for each segment with and without TOF in intra- and inter-observer analyses. There were some cases that have poor agreement in particular segments both in intra- and inter-observer analyses. Specifically, there were larger variation in segment 17 (apex) and the segments near the RV, such as segment 2, 3, 4, 8, 14, and 15. This variation became inconspicuous with TOF.

Representative dynamic trans-axial images without TOF (top) and with TOF (bottom) under rest condition

Intra-observer Pearson’s product moment correlation coefficient (left) and Bland-Altman plots (right) for segmental stress MBF (top), rest MBF (middle), and CFR (bottom) without TOF

Intra-observer Pearson’s product moment correlation coefficient (left) and Bland-Altman plots (right) for segmental stress MBF (top), rest MBF (middle), and CFR (bottom) with TOF

Inter-observer Pearson’s product moment correlation coefficient (left) and Bland-Altman plots (right) for segmental stress MBF (top), rest MBF (middle), and CFR (bottom) without TOF

Inter-observer Pearson’s product moment correlation coefficient (left) and Bland-Altman plots (right) for segmental stress MBF (top), rest MBF (middle), and CFR (bottom) with TOF

Difference plots without TOF (left) and with TOF (right) for stress MBF (top), rest MBF (middle), CFR (bottom) for each segment in intra-observer analyses

Difference plots without TOF (left) and with TOF (right) for stress MBF (top), rest MBF (middle), CFR (bottom) for each segment in inter-observer analyses
Discussion
The NEMA phantom study showed higher image contrast for small spheres using TOF than that using non-TOF because TOF technology was able to localize the coincidence and reduce the propagation of noise along LOR (Figure 1, 2, and 3). It has been shown in previous studies that the image contrast gain with TOF is proportional to the system timing resolution and object size as defined by the relation D/Δχ, where D is object diameter and Δχ = c·Δt/2, c is speed of light, and Δt is timing resolution FWHM.6 This gain of our PET/CT system with timing resolution of 575 ps became 3.5 with 30 cm diameter and 5.8 with 50 cm diameter, respectively. These results were particularly more crucial for cardiac imaging than brain one.
The RC was overestimated for 22-mm-diameter hot spot in 30-cm-diameter phantom with TOF (Figure 2). This bias at the voxel level is due to so-called Gibbs Ringing and is frequently observed in the images reconstructed using point spread function algorithm. The RC values larger than 1.0 were observed for 17- and/or 22-mm spheres (sphere size over 3-4 times as large as the crystal size of PET/CT system).9 This bias is not taken in consideration for absolute quantification of MBF and CFR because normal thickness of myocardial wall is about 10 mm. However, some attention may be paid to cardiac hypertrophy.
In 13N-NH3 PET imaging, the reproducibility of intra- and inter-observer variation with TOF was better than that without TOF, respectively. Because 13N-NH3 PET can measure MBF and CFR with good linearity of tracer, and provide excellent perfusion and ECG-gated images, this multi-direction study will be further widespread in the future.10 Highly reproducible measurement of the MBF and CFR is essential for a clinical routine. Schepis et al11 reported a high rate of concordance between the measurements of the MBF and CFR in 13N-NH3 PET acquired using the 2D and the 3D PET scanners. In general, the infused activity should be adjusted according to a body size. However, for acquisition in the 3D PET scanner, infused activity must be limited to defuse count saturation related to the detector dead time. When the patient’s build is enough big, the gain of benefit using TOF-PET is also significant (Figure 1), and will offset the disadvantage about the administration limit (500 MBq) in 3D PET. We examined the reproducibility of MBF and CFR values with only 370 MBq administration of 13N-NH3 using TOF and convention 3D PET, and confirmed that TOF improved the reproducibility under this low dose situation.
Grace et al12 studied the effect of reconstruction parameters and reconstruction algorithms for MBF measurement. They reported that reconstruction algorithms significantly affected the estimation of quantitative blood flow data and should not be assumed to be interchangeable. Although aggressive smoothing may produce visually appealing images with reduced noise levels, this may cause an underestimation of the absolute MBF. Because TOF-PET does not equip an aggressive smoothing process, TOF-PET can provide accurate quantitative values under achieving good signal-to-noise condition. Table 5 indicates that rest MBF and CFR were higher and lower with TOF than those without TOF, respectively. These differences of the quantitative values were probably due to smaller partial volume effects and higher contrast.
To the best of our knowledge, reproducibility with TOF acquisition technique for the absolute quantification of MBF and CFR with 13N-NH3 PET has not yet been reported. Slomka et al13 compared several kinds of software for MBF and CFR using 13N-NH3 myocardial perfusion PET data. Similar to the present study, high reproducibility of the territorial quantitative values with the PMOD software was demonstrated. Although the reproducibility of the 17 segments was generally similar to that of the coronary territories, some segments showed the considerable intra- and inter-observer differences (Figure 9, 10). In the specific locations of apex (segment 17) and the segment near the RV (segment 2, 3, 4, 8, 14, and 15), the reproducibility was relatively low without TOF images. This impaired reproducibility was improved with TOF technique. To detect various coronary perfusion deficits clinically, the accurate measurement of MBF and CFR not only by territory but also by segment could be essential. These results revealed that MBF and CFR measurements by segment were able to show better reproducibility with TOF.
The calculation in the apex was difficult because of so-called apical thinning due to motion artifacts by both cardiac motion and breathing in addition to small myocardial thickness.14 Moreover, the spillover from RV blood pool into the myocardial wall was introduced as an extra parameter in kinetic model analysis, and RV-TACs were used for the correction of the spillover. However, it was often difficult to place the VOIs at RV blood pool accurately, yielding a variation of the absolute values of segments adjacent to the RV. TOF-PET enabled to place the VOIs at RV and LV blood pool, and myocardium in quantitative analysis without bothering an operator because of better image quality. Nesterov et al15 described the basal segments of the septal wall as the most difficult to place the VOIs in the heart. Mitigation of partial volume effects using TOF made improved the reproducibility of these segments.
In the quantification of myocardial perfusion not only with 13N-NH3 but also with 82Rb or 15O-labeled water, signal-to-noise performance and partial volume effects are major problems. TOF technology could mitigate these intrinsic nuisances, contributing to reliable quantification and reproducibility of MBF and CFR.
New Knowledge Gained
TOF-PET improved partial volume effects and noise characteristics, producing higher intra- or inter-observer reproducibility of MBF and CFR in 13N-NH3 PET.
Conclusion
Visual image quality with TOF was better than that without TOF in the phantom study. RCs and percent contrast of each sphere over percent background variability were improved with TOF, especially of small sphere and in the large phantom.
In the clinical study, intra- or inter-observer reproducibility of measuring quantitative values was compared between with and without TOF. Excellent correlations and good agreements in quantitative values were observed both with and without TOF reconstruction. Larger variation in the apex and the segments near the RV without TOF was improved with TOF reconstruction because TOF-PET is superior at the point of partial volume effects and noise characteristics.
References
Schelbert HR, Phelps ME, Huang SC, MacDonald NS, Selin C, Kuhl DE. N-13 ammonia as an indicator of myocardial blood flow. Circulation 1981;63:1259-72.
Klocke FJ, Baird MG, Lorell BH, Bateman TM, Messer JV, Berman DS, et al. ACC/AHA/ASNC guidelines for the clinical use of cardiac radionuclide imaging-executive summary: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/ASNC Committee to Revise the 1995 Guidelines for the Clinical Use of Cardiac Radionuclide Imaging). J Am Coll Cardiol 2003;42:1318-33.
Tamaki N, Kumita S, Kiyoko K, Matsuzaki M, Nishimura T, Senda S, et al. Guidelines for clinical use of cardiac nuclear medicine (JCS 2010)—digest version. Circ J 2012;76:761-7.
Di Carli MF, Hachamovitch R. Should PET replace SPECT for evaluating CAD? The end of the beginning. J Nucl Cardiol 2006;13:2-7.
Allemand R, Gresset C, Vacher J. Potential advantages of a cesium fluoride scintillator for a time-of-flight positron camera. J Nucl Med 1980;21:153-5.
Budinger TF. Time-of-flight positron emission tomography: Status relative to conventional PET. J Nucl Med 1983;24:73-8.
Karp JS, Surti S, Daube-Witherspoon M, Muehllehner G. Benefit of time-of-flight in PET: Experimental and clinical results. J Nucl Med 2008;49:462-70.
DeGrado TR, Hanson M, Turkington T, Delong D, Brezinski D, Vallee J. Estimation of myocardial blood flow for longitudinal studies with 13N-labeled ammonia and positron emission tomography. J Nucl Cardiol 1996;3:494-507.
Rapisarda E, Bettinardi V, Thielemans K, Gilardi MC. Image-based point spread function implementation in a fully 3D OSEM reconstruction algorithm for PET. Phys Med Biol 2010;55:4131-51.
Okazawa H, Takahashi M, Hata T, Sugimoto K, Kishibe Y, Tsuji T. Quantitative evaluation of myocardial blood flow and ejection fraction with a single dose of 13NH3 and gated gated PET. J Nucl Med 2002;43:999-1005.
Schepis T, Gaemperli O, Treyer V, Valenta I, Burger C, Koepfli P, et al. Absolute quantification of myocardial blood flow with 13N-ammonia and 3-dimensional PET. J Nucl Med 2007;48:1783-9.
Grace P, Kelley R, Adam M, Pham P, Tabibiazar R, Kinahan P, et al. Effect of reconstruction algorithms on myocardial blood flow measurement with 13N-ammonia PET. J Nucl Med 2007;48:1259-65.
Slomka P, Alexanderson E, Jacome R, Jiménez M, Romero E, Meave A, et al. Comparison of clinical tools for measurements of regional stress and rest myocardial blood flow assessed with 13N-ammonia PET/CT. J Nucl Med 2012;53:1-11.
Klein R, Beanlands R, Dekemp R. Quantification of myocardila blood flow and flow reserve: Technical aspects. J Nucl Cardiol 2010;17:555-70.
Nestrov SV, Han C, Maki M, Kajander S, Naum AG, Helenius H, et al. Myocardial perfusion quantification with 15O-labe;ed water PET: High reproducibility of the new cardiac analysis software (Carimas). Eur J Nucl Med Mol Imaging 2009;36:1594-602.
Conflict of interest
The authors have no conflict of interest to disclose with respect to this paper.
Author information
Authors and Affiliations
Corresponding authors
Additional information
See related editorial, doi:10.1007/s12350-015-0098-3.
Rights and permissions
About this article

Cite this article
Suda, M., Onoguchi, M., Tomiyama, T. et al. The reproducibility of time-of-flight PET and conventional PET for the quantification of myocardial blood flow and coronary flow reserve with 13N-ammonia. J. Nucl. Cardiol. 23, 457–472 (2016). https://doi.org/10.1007/s12350-015-0074-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12350-015-0074-y