
Abstract
Esophageal cancer is the eighth most common type of cancer worldwide and constitutes the sixth leading cause of cancer deaths. It is characterized by its high mortality rate, poor prognosis at time of diagnosis and variability based on geographic location. Present day, the prevalence of esophageal cancer is in transition. Although esophageal squamous cell carcinoma continues to be the most prevalent type worldwide, esophageal adenocarcinoma is quickly becoming the most prevalent type in developed countries. Risk factors for the development of esophageal squamous cell carcinoma include low socioeconomic status, consumption of tobacco, alcohol, hot beverages, and nitrosamines. Additionally, micronutrient deficiencies have also been linked to the development of esophageal squamous cell cancer. These include vitamin C, vitamin E, and folate. With respect to esophageal adenocarcinoma, risk factors include Barrett's esophagus, gastroesophageal reflux disease, obesity, and tobacco consumption. Screening for esophageal cancer will likely play an essential role in prevention, and consequently, mortality in the future. Present day, there are no established guidelines for esophageal squamous cell cancer screening. Guidelines for esophageal adenocarcinoma are more well established but lack concrete evidence in the form of randomized controlled trials. This review will discuss the epidemiology, risk factors, and current prevention strategies for esophageal cancer in depth. It is our aim to raise awareness on the aforementioned topics to increase public health efforts in eradicating this disease.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Cancers of the esophagus account for over 500,000 cancer deaths annually, which is 5.3% of all global cancer deaths and have significant varying distributions worldwide [1]. Esophageal squamous cell carcinoma (ESCC) is the most prevalent histological type worldwide, while the United States (US) and other Western countries have predominantly esophageal adenocarcinoma (EAC) [2, 3]. The US distribution of esophageal cancers includes 64% adenocarcinoma, 31% squamous cell carcinoma, and 5% basal, transitional, and other unspecified carcinomas [4]. EAC typically has a better overall median survival than ESCC, particularly in early stage disease [5, 73,74,75]. EAC is thought to be related to Barrett’s esophagus and typically occurs in the distal third of the esophagus and at the gastroesophageal junction (GEJ) though the exact mechanism of malignant transformation is not fully understood. Barrett’s esophagus increases a patient’s risk for EAC 30- to 40-fold [6]. Reciprocally, ESCC is typically found in the proximal two-thirds of the esophagus [3].
According to GLOBOCAN 2018 data, esophageal cancer has the 8th highest incident but is the 6th most deadly cancer worldwide [1, 2]. Esophageal cancer has disproportionately higher mortality, because it is rarely found before it has advanced or metastasized. In fact, in the US, only 18% of esophageal cancers are still confined to the primary site at time of diagnosis [4]. Distant metastasis has been demonstrated in 40% of cases which portends a significantly worse prognosis [4]. In 1975, less than 5% of patients survived 5 years but 5-year survival now exceeds 20% in some parts of the world [3, 4]. The complex anatomy of the mediastinum and GEJ, coupled with the high rates of recurrence, have traditionally led to poor outcomes with surgical intervention alone [3]. A better understanding of the etiology and risk factors of these cancers will allow patients to make risk modifying lifestyle choices and clinicians to target and diagnose populations at higher risk for these deadly carcinomas. We present an update from recent data on the incidence, mortality, and etiological factors of esophageal cancer.
Epidemiology
Incidence
The incidence of esophageal cancer varies across regions and populations. In 2018, approximately 570,000 people were estimated to have been diagnosed with cancer of the esophagus, which constituted 3.2% of all cancer diagnoses [1]. Globally, roughly 87% of all esophageal cancers are ESCC with 11% constituting EAC [7].
The age-standardized incidence rate was highest in Eastern Asia (12.2 per 100,000 people), followed by Eastern and Southern Africa (8.3 and 7.4 per 100,000 people, respectively), and Northern Europe (5.5 per 100,000) (see Fig. 1). The lowest rate was observed in Central America (0.98 per 100,000). Differences in incidence rates were 56-fold between the country with the highest rate (Malawi, Southeastern Africa: 18.7), and the country with the lowest rate that reports data on both sexes (Guinea, West Africa: 0.42) [1, 8]. Notably, esophageal carcinoma is the most common cancer diagnosis in Malawi [9]. Asia, as a continent, accounted for about 78% of all esophageal cancer cases [1, 8]; 49% of all cases occurred in China [8].

Map showing estimated age-standardized incidence rates (ASR) in 2018 for esophageal cancer, both sexes, all ages. Created with mapchart.net. Data obtained from Globocan 2018 [13]
The incidence of esophageal cancer in the US (5.6 per 100,000) is lower when compared to the world (9.3 per 100,000) [1] and within the US was highest among Caucasians, accounting for 85% of the total 27,340 histology confirmed cases from 2012–2016 [4]. In the US, Caucasians accounted for 94% of all EACS but 66% of all ESCCs. Esophageal cancer in Blacks and Asian/Pacific Islanders tended to be ESCC (76% of 2621 cases and 69% of 1208 cases respectively over the same period), while Hispanics had a tendency toward EAC (56% of 2067 cases) [4].
Like most digestive system cancers (except for gallbladder cancer), there is a higher incidence in men than women with men accounting for 70% off all esophageal cancers worldwide. The cumulative risk of esophageal cancer, from birth to age 74, is 1.15% for men and 0.43% for women [1]. Men are at three to four times higher risk than women for developing ESCC and seven to ten times higher risk for developing EAC [6]. The incidence rate for both sexes increases with age. Esophageal cancer affects the elderly predominately, as 60% of cases are reported in people greater than 65 years old, with 12% of cases diagnosed before age 55 [1, 10].
Within China, rates of esophageal cancer vary widely and these abrupt differences can be seen over short geographic distances [76]. It is possible that the environment and/or exposure to certain risk factors account for the variations observed between the esophageal cancer histological subtypes. The tendency to classify cancers of the GEJ as EAC rather than cancers of the gastric cardia may also be influencing trends [11].
Mortality
Esophageal cancer continues a general trend among gastrointestinal cancers presenting with a greater proportion of cancer mortality than incidence. While the incidence accounts for 3.2% of all cancer diagnoses worldwide, esophageal cancer mortality accounts for 5.3% of all cancer deaths. Liver, pancreas, stomach, and gallbladder cancers also follow this trend, with colorectal cancer being the exception. Estimated age-standardized mortality rates (per 100,000) of esophageal cancer is 5.5. Other gastrointestinal cancers are colorectum (8.9), liver (8.5), stomach (8.2), pancreas (4.4), and gallbladder (1.7) (see Fig. 2). About 508,000 people died of esophageal cancer in 2018 worldwide. Of them, about 357,000 were male and 151,000 were female. The gender disparity is on par with the disparity in incidence. The age-standardized mortality was 8.3 per 100,000 for men and 3.0 for women. The cumulative risk of dying from esophageal cancer stands at 1.00% for men and 0.36% for women [1, 8].

reproduced from https://globocan.iarc.fr/ [13])
Bar chart showing the estimated age-standardized cancer mortality rates (world) in 2018, worldwide, both sexes, all ages (
Roughly 16,000 people die annually in the US from esophageal cancer [1, 4]. This constitutes a rate of 7.1 per 100,000 among men and 1.5 per 100,000 for women based on National Cancer Institute data. As with incidence, mortality in the US was highest among Caucasians. However, American Indian/Alaska Natives where the sole race/ethnicity where the age-adjusted mortality was higher than the incidence (6.2 per 100,000 mortality vs 5.9 incidence) [4].
Around the world, esophageal cancer age-standardized mortality rates for both sexes (per 100,000) were highest in Eastern Asia (10.7), Eastern Africa (8.2), and Southern Africa (7.2) followed by Southcentral Asia (4.6) and Northern Europe (4.3) (see Fig. 3). Kenya had the highest mortality (18.4). Asia, as a continent, accounted for 78% of all esophageal cancer deaths; 56% of these deaths occurred in China. Higher mortality rates in females than males were demonstrated in Nepal, certain central/western African countries (Cameroon, Central African Republic, Liberia, and Côte d’Ivoire) and several countries with proximity to the Arabian Sea (Djibouti, Eritrea, Ethiopia, Oman, Qatar, Sudan, and Yemen) [8]. In 2018, esophageal carcinoma was estimated to be the most common cause of cancer related death in Kenya, Botswana, and Bangladesh [8].

Map showing estimated age-standardized mortality rates (ASR) in 2018 for esophageal cancer, both sexes, all ages. Created with mapchart.net. Data obtained from Globocan 2018 [13]
Trends
Within the US, esophageal cancer incidence has been declining since 1986 (see Fig. 4). The annual percentage change (APC) in incidence of esophageal cancer was − 1.5% per year from 2007 to 2016 [3]. Blacks had the largest change in APC at − 4.4%. American Indian/Alaskan Native females were the only race/ethnicity that demonstrated an increase in incidence during this timeframe (APC + 0.8%) [3]. Histologically, ESCC incidence APC was − 3.6% per year while EAC incidence APC was + 2.1% per year from 1998 to 2003. It is predicted that the US will have 15,000 new cases of EAC annually by 2030 [12].

Trends in esophageal cancer incidence (1975–2017) rates by sex, US [3]
Worldwide, incident cases of esophageal cancers are expected to increase by roughly 35% from 2018 to 2030. Estimated number of deaths are expected to increase by roughly 37% during this same timeframe [13]. China has seen a 3.3% decrease in the annual standardized incidence rate from 1989 to 2008 [76]. In contrast to most of the world, incidence rates in Africa are uptrending with some of the highest incidence rates found in East Africa [77]. Incidence of ESCC are declining worldwide among men, however, this decline is offset by increasing incidence of EAC, particularly by the Caucasian population [12]. Incidence of EAC has remained low in many Asian populations but there has been increasing trend noted in Singapore and Israel [78].
Survival
Esophageal cancer has historically had a poor prognosis due to its late diagnosis. In the US, 40% of esophageal cancers were found after spreading to distant organs or lymph nodes while another 32% were found to have regional spread to nearby organs and lymph nodes. Survival based on cancer stage follows a predictable pattern, though survival is still < 50% at 5 years with localized disease (46.7% expected 5-year survival). Esophageal cancer with regional and distant metastasis demonstrate 5-year survivals of 25.1 and 4.8%, respectively (see Fig. 5) [4].

Esophageal cancer 5-year SEER relative survival rates, 2010–2016 by sex and stage at diagnosis [3]
The average 5-year survival rate in the US for esophageal cancer is 19.9%. Caucasians demonstrate a 21% 5-year survival rate, with Blacks having a rate of 13%. Survival disparity between races needs further explanation with future research. Though incidence rates are quite different between sexes, 5-year survival is similar, with survival rates of 19.4% for males and 21.5% for females [4].
Median survival for all esophageal cancers in the US is 9 months. Localized, regional, and distant metastatic disease demonstrate a median survival of 30, 13, and 6 months, respectively. The median survival for patients with EAC in the US is 11 months while the median survival for ESCC is 8 months [5].
China has demonstrated similar 5-year survival rates to US for esophageal cancer at 20.9% [79]. European survival rates are lower with 1- and 5-year survival rates at 33.4 and 9.8%, respectively. Similar to other regions worldwide, male sex, older age, and late stage of disease portend a poorer relative survival. ESCC was noted to have a poorer 1-year relative survival [14].
Like most cancers, esophageal carcinoma mortality demonstrates a negative association with the human development index (HDI). Nations with higher HDI tend to have lower mortality rates (see Fig. 6) [1, 8].

reproduced from https://globocan.iarc.fr/ [13])
Mortality—age-standardized rates (world) versus Human Development Index, esophageal cancer, in 2018, both sexes, all ages (
Etiology and risk factors
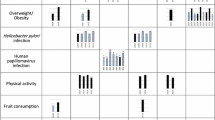
Esophageal carcinoma is often preceded by chronic inflammation in the esophagus that disrupts normal cell signaling and growth. For example, heavy alcohol use has been shown to increase risk for ESCC [11, 15]. Barrett’s esophagus is considered the most important factor in EAC [11]. Tobacco use (smoking or chewing) increases rates of either type [11, 15]. Multiple studies have demonstrated an increased risk of EAC with obesity but reduced risk of ESCC [16,17,18,19]. Low income, Vitamins A and C, zinc deficiencies, hot drinks, and infections (such as human papillomavirus) as well as intrinsic esophageal diseases have been demonstrated to increase incidence of ESCC (see Table 1) [6, 11]. Studies from Africa, China, Europe, Iran, Japan, and the United States demonstrate considerable esophageal cancer etiologic heterogeneity suggesting major risks factors for one population may by not be as significant in other populations [80].
Age and sex
Esophageal cancer rates become more common with age, likely because this carcinoma takes decades to develop. The average age of diagnosis in the US is 68. Esophageal cancer is common after the age of 55 when 88% of all cases occur. The Surveillance, Epidemiology, and End Results (SEER) database in the US reveals that age-adjusted incidence rates (per 100,000) in 2016 rose from 0.3 for those aged 20–49 years, to 8.0 for those aged 50–64, to 20.3 for those aged 65–74 years, and to 24.9 for individuals aged 75 years or older. This corresponded with mortality rates (per 100,000), which increased from 0.3 for those aged 20–49, to 6.9 for those aged 50–64, and to 17.5 for those aged 65–74 years. The highest mortality rate was 25.0 per 100,000 for individuals aged 75 years and older [4].
In the United Kingdom, a country with predominantly EAC, the average age of diagnosis is 65 for males and 74 for females [81]. The average age of diagnosis in Malaysia is 63 and China demonstrates an even younger average age of diagnosis at 61 years [81, 83]. Africa, a continent with predominantly ESCC, has shown a disproportionate number of patients (approximately 20%) diagnosed before age 40 [80].
Esophageal cancer is more common in males than females. Men are two to eight times more affected than women [1, 20]. However, there are several areas within west/central Africa, the Horn of Africa as well as the Arabian Peninsula where esophageal cancer is more common in women. In Yemen, the incidence ratio of women to men is highest at 1.8 [8].
The large sex disparities in esophageal cancer is a well-known phenomenon, but the reasons for this pattern are not fully understood. The higher rates of EAC seen in males are thought to be partially explained by higher prevalence of abdominal obesity and gastroesophageal reflux disease (GERD) and the associations of testosterone in males; estrogen appears to have a protective effect in females [21]. Breastfeeding has also been demonstrated to decrease risk of EAC [22]. These findings suggest a possible hormonal component to esophageal cancer.
Genetics and family history
Reports regarding the familial risk of esophageal cancer have been contradictory. Studies in the United States, Italy, and Switzerland have not identified an association [23, 24]. However, studies in China (a country with much higher rates of ESCC) demonstrated a nearly doubled risk of ESCC in individuals with a familial history of ESCC in a first degree relative; these individuals also tend to have poorer survival [25,26,27]. Shared environmental factors among family members, such as diet, obesity, and tobacco use, may account for these discordant findings.
Family history of several other cancers have been associated with increased risks of esophageal cancer: lung, prostate, breast, cervical, oral, and pharyngeal cancers have shown association [23, 28, 29]. Family history of hiatal hernia has also been associated with EAC [28]. The rare autosomal recessive genetic syndrome, Fanconi anemia, has shown a several hundred- to several thousand-fold higher risk for esophageal cancer, due to their astonishing elevated risk of developing solid tumors [30].
Multiple genetic mutations have been implicated among esophageal cancer cases. TP53 mutations can be seen in more than 83% of ESCC. Overexpression of EGFR (seen in up to 76% of cases), CCND1 (46% of cases), CDK4/CDK6 (24% of cases), and MDM2 (6% of cases) are also common in ESCC [15]. Amplification of CCNE1 (19% of cases), cyclin E (17%), and mutations in MGST1 have been implicated in EAC [15, 31]. Individuals with higher levels of VEGF-C expression typically experience shorter periods of event-free survival, while those with variant alleles of the FLT1 gene have a 45–60% increased risk of mortality [15].
ALDH2 mutations are thought to be protective against esophageal cancer. Inactivation of this protein makes an individual unable to metabolize acetaldehyde, a byproduct of alcohol metabolism. It is thought that the adverse reactions from consuming alcohol in these individuals decreases alcohol consumption and thus lowers risk [32].
Obesity and gastroesophageal reflux disease
Obesity has been a well-researched and long understood risk factor in developing EAC [1, 16,17,18,19, 33]. There appears to be a dose-dependent response between risk of EAC and increasing BMI or increasing waist circumference [15, 19]. A meta-analysis of 221 data sets from 141 articles showed a significant increase in risk for EAC for each 5 kg/m2 increase in BMI (RR 1.5) [34]. Individuals with a BMI > 40 have a twofold increased risk in developing EAC, and this association remains strong regardless of GERD symptoms when compared to those with BMI < 25 [16]. This is potentially explained by higher rates of GERD and Barrett’s esophagus seen with obesity, particularly those with large amounts of abdominal fat [18, 19, 21]. Associations between GERD and EAC have been well demonstrated with estimated odds ratios (ORs) ranging from 2.5 to 40 based on severity or time with disease [35]. Obesity has also been shown to have an inverse relationship with ESCC (relative risk (RR) 0.38) [18, 19]. Variations in obesity prevalence worldwide, as well as differences in central obesity seen across sexes and age, could explain the different incidence patterns seen between EAC and ESCC [16, 18, 21].
To provide prospective, the absolute risk of EAC to an individual patient with GERD is quite low. Up to 44% of adults in the US experience reflux symptoms at least monthly; however, the incidence of EAC in these individuals older than 50 is 65/100,000. Additionally, 40% of EAC cases report no history of reflux [35].
Alcohol
Alcohol consumption and smoking are well established risk factors for ESCC, and several studies have demonstrated a synergistic effect [33, 36,37,38]. The population-attributable fraction of ESCC due to alcohol consumption can vary widely geographically. In the US, 72.4% of ESCC cases are attributed to alcohol while only 10.9% of cases are attributable in China, which is likely a reflection in the levels of exposure [86]. The increase in risk appears to be dependent on the amount of alcohol consumed and the beverage type [36, 37, 39, 84]. Relative risks range from 1.8 to 7.4, depending on weekly alcohol consumption [39]. One cohort study in South Korea demonstrated light drinking (≤ 5 drinks per week) as having a significant adverse effect, when traditionally the risk was thought to apply to moderate/heavy alcohol consumption [36]. The authors hypothesized that the increased risk with light alcohol intake was related to the high prevalence of abnormal ALDH2 enzyme activity seen in Asian populations [36].
Beer intake appears to have a linear relationship with ESCC, with higher intake signifying increased risk (OR 1.05). However, those with modest intake of wine (3.5–6.4 drinks per week) or spirits (0.7–1.4 drinks per week) demonstrated significantly lower risk for ESCC than nondrinkers but demonstrate the same increased risk of ESCC when consumed in higher amounts [37]. Alcohol consumption has not been demonstrated to significantly increase risk of EAC in population-based studies [40].
Tobacco
Prospective epidemiological data have consistently shown smoking as a major risk factor for ESCC, and this risk appears to be dose dependent. Studies in Africa, Asia, Europe, and the US have demonstrated this to varying degrees suggesting this risk factor is not a geographical phenomenon [76, 77, 82, 85, 86]. In an Australian population-based case–controlled study, greater than 75% of ESCC cases could be attributed to smokers with heavy alcohol consumption [41]. Another study from Australia found an OR of 21.9 for ESCC with combined tobacco and alcohol use [42]. Even 10 years after cessation of smoking, former smokers are at twice the risk of ESCC compared to non-smokers [43].
Similar trends in EAC risk are seen with smoking, especially if Barrett’s esophagus is present, but not to the degree seen with ESCC [44, 76]. This risk is reduced with smoking cessation but does not return to the level of one who has never smoked [45].
Diet
A meta-analysis of 32 studies regarding fruit and vegetables indicated that high intake has a protective effect against ESCC. The authors suggest significant thresholds of 160 g/day of non-starchy vegetables and 20 g/day of fruits provided a protective benefit but cautioned against overemphasis on specific consumption requirements [46]. Case–control studies worldwide have demonstrated this finding with both ESCC and EAC [47]. The protective benefits are thought to derive from the antioxidant properties of fruits and vegetables helping reduce oxidative stress and inflammation. Folate and Vitamin C, which are readily obtained from these foods, have been shown to reduce risk of esophageal cancer in some studies [48, 87]. There is also evidence that diets high in fiber may reduce the risk of esophageal cancer [47, 78] Beta-carotene, vitamin E, and selenium have not shown reduced ESCC incidence or mortality in high-incidence ESCC populations in China [76]. Vitamin D has not demonstrated any consistent associations with esophageal cancer [49].
There is convincing evidence that the consumption of maté, consumed in the traditional South American manner (scalding hot liquid through a metal straw) increases the risk for esophageal cancer in a consistent dose-dependent manner. This finding may be secondary to the epithelial damage from the heat, rather than the maté itself [47]. Additional studies have demonstrated that individuals who consume very hot foods/beverages are almost twice as likely to develop esophageal cancer, particularly in Asian and South American populations [47, 50]. Meta-analysis of coffee, specifically, did not establish a protective or detrimental association with esophageal cancer; of note, temperature was not adequately evaluated in the analysis [51]. When targeting prevention strategies for esophageal cancer, very hot foods/drinks may be an important target for behavioral modification.
Consumption of red, salted, or processed meat can increase risk for ESCC by as much as 57%, with a nonsignificant increase in risk noted for EAC [47, 52, 85]. However, population studies have shown an increase in Barrett’s esophagus, a precursor for EAC, in those that consume a diet high in meat [53]. One study in China demonstrated risk reductions in esophageal precancerous lesions with consumption of animal livers and deep well water [54].
Helicobacter pylori
Helicobacter pylori (H. pylori) was famously discovered as a cause of peptic ulcer disease in 1983 and is now considered a well-established cause of gastric cancer [55]. In 1994, the World Health Organization classified H. pylori as a class I (definite) carcinogen. This process occurs through chronic inflammation resulting in atrophic gastritis that leads to intestinal metaplasia followed by dysplasia [56]. In 2015, 4.4 billion individuals were estimated to have H. pylori worldwide. The prevalence range of H. pylori is quite large with highest prevalence estimates occurring in Africa (70.1%; 95% CI 62.6 − 77.7) and lowest in Oceania (24.4%; 95% CI 18.5–30.4); in comparison, the US prevalence is estimated to be 35.6% (95% CI 30.0–41.1) of the population [57].
Current evidence tends to support a reduced risk of EAC in those with H. pylori infection (OR 0.50–0.57) [58, 59]. H. pylori may reduce risk for EAC through atrophic gastritis by reducing acid production and reflux. The prominent decline in H. pylori colonization in Western countries may partially explain the increase in EAC rates seen in those areas. The effects of H. pylori on ESCC risk are less clear with study results differing substantially, likely due to the wide heterogeneity seen between studies, which makes determining any association difficult [58].
Medications and additional risk factors
Several medications have been implicated in lowering one’s risk of esophageal cancer, largely with respect to EAC. Aspirin, nonsteroidal anti-inflammatory drugs (NSAIDs), and statins have been implicated in multiple studies at reducing risk, possibly due to their anti-inflammatory effects. The all-Ireland FINBAR study evaluating aspirin and NSAIDs showed an OR of 0.57 and 0.58, respectively, in reducing EAC risk [60]. Another study out of the Netherlands showed HR 0.46 for NSAIDs and HR 0.46 for statins but did not demonstrate a benefit with aspirin; the combined use of NSAIDs and statins had a synergistic protective effect (HR 0.22) [61]. An observational study from the Department of Veterans’ Affairs showed similar trends suggesting greater risk reduction in EAC with longer duration of statin use [62]. Proton pump inhibitors have demonstrated a 71% decrease in risk of progression from Barrett’s esophagus to EAC in previous studies when used for greater than 2–3 years; this appears to be independent from the use of aspirin/NSAIDs/statins [63].
A large Belgian cohort study showed that in patients with stage I–III esophageal cancer, post-diagnosis use of statins was associated with decreased overall and cancer-specific mortality (adjusted HR = 0.84 and 0.87, respectively) [64]. A recent meta-analysis out of China was significant for three reasons as it demonstrated that statin use after diagnosis of esophageal cancer was significantly correlated to decreased all-cause (HR = 0.81) and cancer-specific mortality (HR = 0.84), that this protective effect was observed regardless of histologic subtype of cancer, and that statin use prior to diagnosis also confirmed favorable survival benefit [88]. These studies suggest a potential importance of statin use in esophageal cancer treatment, as well as prevention.
There is some evidence that decreased lower esophageal sphincter tone may contribute to the development of Barrett’s esophagus and thus EAC. A case–control study from Sweden implicated medications such as anticholinergics, benzodiazepines, beta agonists, and nitroglycerin as increasing EAC risk when used for more than 5 years [65].
An additional risk factor for ESCC includes betel quid chewing, most commonly seen in India and southeast Asia. When combining alcohol, tobacco, and betel quid chewing, risk for ESCC increases by more than 41-fold [66]. Occupational exposures of asbestos, pesticides, concrete/masonry work, and combustion products from biofuels, coal/oil, and wildfires have been associated with esophageal cancer in a dose dependent manner [67,68,69].
Prevention
Esophageal cancer remains an important public health challenge and significant cause of cancer-related death worldwide. The significant differences between ESCC and EAC result in major variances in incidence, geography, and etiological characteristics, which makes fully understanding and preventing esophageal cancer difficult.
There are currently no screening guidelines for ESCC [70]. Current recommendations for screening of EAC in those with precancerous conditions is derived from low levels of evidence. As of 2017, there have been no randomized controlled trials to compare screening versus no screening [71].
Significant survival improvements with esophageal cancer have been occurring since 1973, largely due to earlier detection and the utilization of surgery in treatment; however, both types continue to carry a high mortality rate, though EAC has slightly better long-term survival outcomes [4, 5]. The poor overall prognosis of esophageal cancer is due to the advanced nature of the disease at diagnosis, with a 1-year survival rate of 42% in the US [4]. Dysplasia is the preneoplastic lesion associated with ESCC and Barrett’s esophagus is the most important risk factor for EAC. Conventional white light endoscopy with biopsy remains the standard for identifying esophageal premalignant lesions; however, many studies from Asian countries elucidate the effectiveness of narrow-band imaging without biopsy procedure for the detection of ESCC in endoscopic surveillance [83]. In studies out of Japan and Taiwan, the sensitivities and specificities of detecting synchronous and metachronous ESCC have ranged 88.9–97.3 and 88.9–97.2%, respectively [83]. Early-stage detection of esophageal cancer remains the best way to improve cure rates and survival [2, 70]. Treatment of early-stage ESCC restricted to the first one-third of the submucosa (Sm1), without lymph node involvement, utilizing surgery or endoscopic resection have demonstrated 5-year survival rates greater than 90% [70].
Various biochemical markers, optic-based chromoendoscopic techniques, and balloon cytology have been evaluated for esophageal cancer screening but currently no single technique has obtained a sensitivity and specificity, or an economic feasibility appropriate for broad population-based application [70, 89]. The psychological and economic implications must be considered for such a program. Any future ESCC screening recommendations will likely rely heavily on risk factor models to identify those at highest risk who should undergo screening. One study on Japanese men utilized health risk appraisal models that incorporated ALDH2 genotype, alcohol, tobacco, and diet and referred those identified to be in the top 10% risk group for endoscopy with iodine staining. Their models were able to detect up to 3.13% of ESCCs (eight times the national average); notably, these cancers were diagnosed at earlier stages [72].
When targeting prevention strategies for esophageal cancer, the elimination of very hot foods/drinks in the diet combined with alcohol/tobacco cessation likely will provide the most behavioral modification benefit. The addition of fruits and vegetables to one’s diet would likely be of benefit, but may be difficult in developing countries, where more than 80% of ESCC deaths occur [70].
Conclusion
Esophageal cancer continues to be a significant cause of cancer-related death worldwide. Survival has been slowly improving since the 1970s, but 5-year survival rates are generally still less than 20% [4]. Esophageal cancers are not typically diagnosed until advanced stages, when very few options are available to extend life expectancy beyond several months. Less than one in five esophageal cancers in the US are diagnosed in an early stage and the median survival for those with advanced cases is only 6–13 months [5].
In the US, GERD, obesity, smoking, and low fruit/vegetable intake account for 80% of EAC cases, the type of esophageal cancer most common in the US [65]. Tobacco, alcohol, and low fruit and vegetable intake account for nearly 90% of ESCC cases in the US [65]. Reliable biomarkers to predict outcomes are still limited and current screening guidelines are derived from low levels of evidence. This highlights the need for randomized controlled trials of the eighth most common cancer worldwide. The significant clinical, histological, and etiological differences between EAC and ESCC justify different therapeutic approaches. Earlier diagnosis, likely with improved screening measures, is key in obtaining better outcomes as significant survival benefit has been demonstrated in small studies where esophageal cancer was discovered at earlier stages.
References
Bray F, Ferlay J, Soerjomataram I, Siegel RL, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424.
Umar S, Fleischer D. Esophageal cancer: epidemiology, pathogenesis and prevention. Nat Rev GastroenterolHepatol. 2008;5:517–26.
Ilson DH, van Hillegersberg R. Management of patients with adenocarcinoma or squamous cancer of the esophagus. Gastroenterology. 2018;154:437–51.
Howlader N, Noone AM, Krapcho M, et al. SEER Cancer Statistics Review, 1975–2016, National Cancer Institute. Bethesda, MD, https://seer.cancer.gov/csr/1975_2016/, based on November 2018 SEER data submission, posted to the SEER web site, April 2019. Accessed 23 February 2020.
Njei B, McCarty TR, Birk JW. Trends in esophageal cancer survival in United States adults from 1973 to 2009: a SEER database analysis. J GastroenterolHepatol. 2016;31:1141–6.
Pickens A, Orringer MB. Geographical distribution and racial disparity in esophageal cancer. Ann ThoracSurg. 2003;76:S1367–S13691369.
Arnold M, Soerjomataram I, Ferlay J, Forman D. Global incidence of oesophageal cancer by histological subtype in 2012. Gut. 2015;64:381–7.
Ferlay J, Ervik M, Lam F, et al. Global cancer observatory: cancer today. International Agency for Research on Cancer, Lyon, France. Available from: https://gco.iarc.fr/today. Accessed 05 March 2020.
Global Burden of Disease Cancer Collaboration. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 32 cancer groups, 1990 to 2015: a systematic analysis for the global burden of disease study. JAMA Oncol. 2017;3:524–48.
Montgomery EA (2014) Oesophageal Cancer. In: Stewart BW, Wild CP (Eds) World Cancer Report 2014. World Health Organization. p 374–82.
Chen W, Zheng R, Zeng H, et al. Annual report on status of cancer in China, 2011. Chin J Cancer Res. 2015;27:2–12.
Arnold M, Laversanne M, Brown LM, et al. Predicting the future burden of esophageal cancer by histological subtype: international trends in incidence up to 2030. Am J Gastroenterol. 2017;112:1247–55.
Ferlay J, Ervik M, Lam F, et al. Global Cancer Observatory: Cancer Tomorrow. Lyon, France: International Agency for Research on Cancer. 2018. Available from: https://gco.iarc.fr/tomorrow, accessed 15 March 2020.
Gavin AT, Francisci S, Foschi R, et al. EUROCARE-4 Working Group. Oesophageal cancer survival in Europe: a EUROCARE-4 study. Cancer Epidemiol. 2012;36:505–12.
Huang FL, Yu SJ. Esophageal cancer: Risk factors, genetic association, and treatment. Asian J Surg. 2018;41:210–5.
Hoyo C, Cook MB, Kamangar F, et al. Body mass index in relation to oesophageal and oesophagogastric junction adenocarcinomas: a pooled analysis from the International BEACON Consortium. Int J Epidemiol. 2012;41:1706–18.
Corley DA, Kubo A, Zhao W. Abdominal obesity and the risk of esophageal and gastric cardia carcinomas. Cancer Epidemiol Biomarkers Prev. 2008;17:352–8.
Lindkvist B, Johansen D, Stocks T, et al. Metabolic risk factors for esophageal squamous cell carcinoma and adenocarcinoma: a prospective study of 580,000 subjects within the Me-Can project. BMC Cancer. 2014;14:103.
Steffen A, Schulze MB, Pischon T, et al. Anthropometry and esophageal cancer risk in the European prospective investigation into cancer and nutrition. Cancer Epidemiol Biomarkers Prev. 2009;18:2079–89.
Siewert JR, Ott K. Are squamous and adenocarcinomas of the esophagus the same disease? SeminRadiat Oncol. 2007;17:38–44.
Arnold M, Colquhoun A, Cook MB, et al. Obesity and the incidence of upper gastrointestinal cancers: an ecological approach to examine differences across age and sex. Cancer Epidemiol Biomarkers Prev. 2016;25:90–7.
Cronin-Fenton DP, Murray LJ, Whiteman DC, et al. Reproductive and sex hormonal factors and oesophageal and gastric junction adenocarcinoma: a pooled analysis. Eur J Cancer. 2010;46:2067–76.
Dhillon PK, Farrow DC, Vaughan TL, et al. Family history of cancer and risk of esophageal and gastric cancers in the United States. Int J Cancer. 2001;93:148–52.
Turati F, Edefonti V, Bosetti C, et al. Family history of cancer and the risk of cancer: a network of case-control studies. Ann Oncol. 2013;24:2651–6.
Chen T, Cheng H, Chen X, et al. Family history of esophageal cancer increases the risk of esophageal squamous cell carcinoma. Sci Rep. 2015;5:16038.
Su Z, Zou GR, Mao YP, et al. Prognostic impact of family history of cancer in Southern Chinese patients with esophageal squamous cell cancer. J Cancer. 2019;10:1349–57.
Jia N, Wen X, Zhang N, et al. Younger age of onset and multiple primary lesions associated with esophageal squamous cell carcinoma cases with a positive family history of the cancer suggests genetic predisposition. Chin Med J (Engl). 2014;127:2779–833.
Jiang X, Tseng CC, Bernstein L, et al. Family history of cancer and gastroesophageal disorders and risk of esophageal and gastric adenocarcinomas: a case-control study. BMC Cancer. 2014;14:60.
Turati F, Negri E, La Vecchia C. Family history and the risk of cancer: genetic factors influencing multiple cancer sites. Expert Rev Anticancer Ther. 2014;14:1–4.
Rosenberg PS, Greene MH, Alter BP. Cancer incidence in persons with Fanconi anemia. Blood. 2003;101:822–6.
Buas MF, He Q, Johnson LG, et al. Germline variation in inflammation-related pathways and risk of Barrett's oesophagus and oesophageal adenocarcinoma. Gut. 2017;66:1739–47.
Lewis SJ, Smith GD. Alcohol, ALDH2, and esophageal cancer: a meta-analysis which illustrates the potentials and limitations of a Mendelian randomization approach. Cancer Epidemiol Biomarkers Prev. 2005;14:1967–71.
Blot WJ, Tarone RE. Esophageal cancer. In: Thun MJ, Linet MS, Cerhan JR, Haiman CA, Schottenfeld D, editors. Cancer epidemiology and prevention. 4th ed. New York: Oxford University Press; 2018. p. 579–592.
Renehan AG, Tyson M, Egger M, et al. Body-mass index and incidence of cancer: a systematic review and meta-analysis of prospective observational studies. Lancet. 2008;371:569–78.
Holmes RS, Vaughan TL. Epidemiology and pathogenesis of esophageal cancer. SeminRadiat Oncol. 2007;17:2–9.
Choi YJ, Lee DH, Han K-D, et al. The relationship between drinking alcohol and esophageal, gastric or colorectal cancer: a nationwide population-based cohort study of South Korea. PLoS ONE. 2017;12:e0185778.
Pandeya N, Williams G, Green AC, et al. Alcohol consumption and the risks of adenocarcinoma and squamous cell carcinoma of the esophagus. Gastroenterology. 2009;136:1215–24.
Toh Y, Oki E, Ohgaki K, et al. Alcohol drinking, cigarette smoking, and the development of squamous cell carcinoma of the esophagus: molecular mechanisms of carcinogenesis. Int J Clin Oncol. 2010;15:135–44.
DomperArnal MJ, Arenas F, Arbeloa L. Esophageal cancer: Risk factors, screening and endoscopic treatment in Western and Eastern countries. World J Gastroenterol. 2015;21:7933–43.
Anderson LA, Cantwell MM, Watson RG, et al. The association between alcohol and reflux esophagitis, Barrett's esophagus, and esophageal adenocarcinoma. Gastroenterology. 2009;136:799–805.
Pandeya N, Olsen CM, Whiteman DC. Sex differences in the proportion of esophageal squamous cell carcinoma cases attributable to tobacco smoking and alcohol consumption. Cancer Epidemiol. 2013;37:579–84.
Dong J, Thrift AP. Alcohol, smoking and risk of oesophago-gastric cancer. Best Pract Res ClinGastroenterol. 2017;31:509–17.
Bosetti C, Gallus S, Garavello W, et al. Smoking cessation and the risk of oesophageal cancer: an overview of published studies. Oral Oncol. 2006;42:957–64.
Hardikar S, Onstad L, Blount PL, et al (2013) The role of tobacco, alcohol, and obesity in neoplastic progression to esophageal adenocarcinoma: a prospective study of Barrett's esophagus. PloS one. 8.
Cook MB, Kamangar F, Whiteman DC, Freedman ND, Gammon MD, Bernstein L, Brown LM, Risch HA, Ye W, Sharp L, Pandeya N, Webb PM, Wu AH, et al. Cigarette smoking and adenocarcinomas of the esophagus and esophagogastric junction: a pooled analysis from the international BEACON consortium. JNCI J Natl Cancer Inst. 2010;102:1344–53. https://doi.org/10.1093/jnci/djq289.
Liu J, Wang J, Leng Y, et al. Intake of fruit and vegetables and risk of esophageal squamous cell carcinoma: a meta-analysis of observational studies. Int J Cancer. 2013;133:473–85.
World Cancer Research Fund/American Institute for Cancer Research. Diet, Nutrition, Physical Activity and Cancer: a Global Perspective. Continuous Update Project Expert Report 2018. Available at https://dietandcancerreport.org. Accessed 24 Aug 2020.
Zhao Y, Guo C, Hu H, et al. Folate intake, serum folate levels and esophageal cancer risk: an overall and dose-response meta-analysis. Oncotarget. 2017;8:10458–69.
Zgaga L, O'Sullivan F, Cantwell MM, et al. Markers of Vitamin D exposure and esophageal cancer risk: a systematic review and meta-analysis. Cancer Epidemiol Biomarkers Prev. 2016;25:877–86.
Chen Y, Tong Y, Yang C, et al. Consumption of hot beverages and foods and the risk of esophageal cancer: a meta-analysis of observational studies. BMC cancer. 2015;15:449.
Zhang J, Zhou B, Hao C. Coffee consumption and risk of esophageal cancer incidence: a meta-analysis of epidemiologic studies. Medicine (Baltimore). 2018;97:e0514.
Qu X, Ben Q, Jiang Y. Consumption of red and processed meat and risk for esophageal squamous cell carcinoma based on a meta-analysis. Ann Epidemiol. 2013;23:762–70.
Kubo A, Levin TR, Block G, et al. Dietary patterns and the risk of Barrett's esophagus. Am J Epidemiol. 2008;167:839–46.
Pan D, Su M, Zhang T, et al. A distinct epidemiologic pattern of precancerous lesions of esophageal squamous cell carcinoma in a high-risk area of Huai'an, Jiangsu Province, China. Cancer Prev Res (Phila). 2019;12:449–62.
Marshall B, Warren JR. Unidentified curved bacilli in the stomach of patients with gastritis and peptic ulceration. Lancet. 1984;323(8390):1311–5.
Ahn HJ, Lee DS. Helicobacter pylori in gastric carcinogenesis. World J Gastrointest Oncol. 2015;7:455–65.
Hooi JKY, Lai WY, Ng WK, et al. Global prevalence of helicobacter pylori infection: systematic review and meta-analysis. Gastroenterology. 2017;153:420–9.
Islami F, Kamangar F. Helicobacter pylori and esophageal cancer risk: a meta-analysis. Cancer Prev Res (Phila). 2008;1:329–38.
Nie S, Chen T, Yang X, et al. Association of helicobacter pylori infection with esophageal adenocarcinoma and squamous cell carcinoma: a meta-analysis. Dis Esophagus. 2014;27:645–53.
Anderson LA, Johnston BT, Watson RG, et al. Nonsteroidal anti-inflammatory drugs and the esophageal inflammation-metaplasia-adenocarcinoma sequence. Cancer Res. 2006;66:4975–82.
Kastelein F, Spaander MC, Biermann K, et al. Probar-study Group. Nonsteroidal anti-inflammatory drugs and statins have chemopreventative effects in patients with Barrett's esophagus. Gastroenterology. 2011;141:2000–8.
Nguyen DM, Richardson P, El-Serag HB. Medications (NSAIDs, statins, proton pump inhibitors) and the risk of esophageal adenocarcinoma in patients with Barrett's esophagus. Gastroenterology. 2010;138:2260–6.
Singh S, Garg SK, Singh PP, et al. Acid-suppressive medications and risk of oesophageal adenocarcinoma in patients with Barrett's oesophagus: a systematic review and meta-analysis. Gut. 2014;63:1229–377.
Lacroix O, Couttenier A, Vaes E, et al. Statin use after diagnosis is associated with an increased survival in esophageal cancer patients: a Belgian population-based study. Cancer Causes Control. 2019;30:385–93.
Wheeler JB, Reed CE. Epidemiology of esophageal cancer. SurgClin North Am. 2012;92:1077–87.
Lee CH, Lee JM, Wu DC, et al. Independent and combined effects of alcohol intake, tobacco smoking and betel quid chewing on the risk of esophageal cancer in Taiwan. Int J Cancer. 2005;113:475–82.
Offermans NS, Vermeulen R, Burdorf A, et al. Occupational asbestos exposure and risk of esophageal, gastric and colorectal cancer in the prospective Netherlands Cohort Study. Int J Cancer. 2014;135:1970–7.
Roshandel G, Semnani S, Malekzadeh R, et al. Polycyclic aromatic hydrocarbons and esophageal squamous cell carcinoma. Arch Iran Med. 2012;15:713–22.
Jansson C, Plato N, Johansson AL, et al. Airborne occupational exposures and risk of oesophageal and cardia adenocarcinoma. Occup Environ Med. 2006;63:107–12.
Lopes AB, Fagundes RB. Esophageal squamous cell carcinoma—precursor lesions and early diagnosis. World J GastrointestEndosc. 2012;4:9–16.
Hamel C, Ahmadzai N, Beck A, et al. (2020) Screening for esophageal adenocarcinoma and precancerous conditions (dysplasia and Barrett’s esophagus) in patients with chronic gastroesophageal reflux disease with or without other risk factors: two systematic reviews and one overview of reviews to inform a guideline of the Canadian Task Force on Preventive Health Care (CTFPHC). Syst Rev. 9.
Yokoyama T, Yokoyama A, Kumagai Y, et al. Health risk appraisal models for mass screening of esophageal cancer in Japanese men. Cancer Epidemiol Biomarkers Prev. 2008;17(10):2846–54. https://doi.org/10.1158/1055-9965.EPI-08-0397.
Gavin AT, Francisci S, Foschi R, et al. Oesophageal cancer survival in Europe: a EUROCARE-4 study. Cancer Epidemiol. 2012;36:505–12.
Hou H, Meng Z, Zhao X, et al. Survival of esophageal cancer in China: a pooled analysis on hospital-based studies From 2000 to 2018. Front Oncol. 2019;9:548.
Qin J, Zhu HD, Guo JH, et al. Factors associated with overall survival and relief of dysphagia in advanced esophageal cancer patients after 125I seed-loaded stent placement: a multicenter retrospective analysis. Dis Esophagus. 2019;32:doz012.
Smyth EC, Lagergren J, Fitzgerald RC, et al. Oesophageal cancer. Nat Rev Dis Primers. 2017;3:17048.
Asombang AW, Chishinga N, Nkhoma A, et al. Systematic review and meta-analysis of esophageal cancer in Africa: epidemiology, risk factors, management and outcomes. World J Gastroenterol. 2019;25:4512–33.
Coleman HG, Xie SH, Lagergren J. The epidemiology of esophageal adenocarcinoma. Gastroenterology. 2018;154:390–405.
Zeng H, Zheng R, Guo Y, et al. Cancer survival in China, 2003–2005: a population-based study. Int J Cancer. 2015;136:1921–30.
Van Loon K, Mwachiro MM, Abnet CC, et al. The African esophageal cancer consortium: a call to action. J Glob Oncol. 2018;4:1–9.
Chung CS, Lee YC, Wu MS. Prevention strategies for esophageal cancer: perspectives of the East vs West. Best Pract Res ClinGastroenterol. 2015;29:869–83.
Siti-Azrin AH, Wan-Nor-Asyikeen WA, Norsa'adah B. Review of the burden of esophageal cancer in Malaysia. Asian Pac J Cancer Prev. 2016;17:3705–9.
Guo LW, Huang HY, Shi JF, et al. Medical expenditure for esophageal cancer in China: a 10-year multicenter retrospective survey (2002–2011). Chin J Cancer. 2017;36:73.
Abnet CC, Arnold M, Wei WQ. Epidemiology of esophageal squamous cell carcinoma. Gastroenterology. 2018;154:360–73.
Lin Y, Totsuka Y, Shan B, et al. Esophageal cancer in high-risk areas of China: research progress and challenges. Ann Epidemiol. 2017;27:215–21.
Kitagawa Y, Uno T, Oyama T, et al. Esophageal cancer practice guidelines 2017 edited by the Japan Esophageal Society: part 1. Esophagus. 2019;16:1–24.
Bo Y, Lu Y, Zhao Y, et al. Association between dietary vitamin C intake and risk of esophageal cancer: a dose-response meta-analysis. Int J Cancer. 2016;138:1843–50.
Deng HY, Lan X, Zheng X, et al. The association between statin use and survival of esophageal cancer patients: a systematic review and meta-analysis. Medicine (Baltimore). 2019;98:e16480.
Yang W, Han Y, Zhao X, et al. Advances in prognostic biomarkers for esophageal cancer. Expert Rev MolDiagn. 2019;19:109–19.
Acknowledgements
The authors would like to recognize the contribution of cancer registry staff who collected the data used in this review.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that there is no conflict of interest regarding the publication of this paper.
Human and animal rights
This article does not contain any studies directly involving human participants, as it is a review of data already collected in multiple cancer databases.
Informed consent
For this type of study/review, formal consent is not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Uhlenhopp, D.J., Then, E.O., Sunkara, T. et al. Epidemiology of esophageal cancer: update in global trends, etiology and risk factors. Clin J Gastroenterol 13, 1010–1021 (2020). https://doi.org/10.1007/s12328-020-01237-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12328-020-01237-x