
Abstract
It is well accepted that the cerebellum plays a crucial role in the prediction of the sensory consequences of movements. Recent findings of altered error processing in patients with selective cerebellar lesions led to the hypothesis that feedback processing and feedback-based learning might be affected by cerebellar damage as well. Thus, the present study investigated learning from and processing of positive and negative feedback in 12 patients with selective cerebellar lesions and healthy control subjects. Participants performed a monetary feedback learning task. The processing of positive and negative feedback was assessed by means of event-related potentials (ERPs) during the learning task and during a separate task in which the frequencies of positive and negative feedback were balanced. Patients did not show a general learning deficit compared to controls. Relative to the control group, however, patients with cerebellar lesions showed significantly higher ERP difference wave amplitudes (rewards–losses) in a time window between 250 and 450 ms after feedback presentation, possibly indicating impaired outcome prediction. The analysis of the original waveforms suggested that patients and controls primarily differed in their pattern of feedback-related negativity and P300 amplitudes. Our results add to recent findings on altered performance monitoring associated with cerebellar damage and demonstrate, for the first time, alterations of feedback processing in patients with cerebellar damage. Unaffected learning performance appears to suggest that chronic cerebellar lesions can be compensated in behaviour.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Traditionally, the cerebellum was associated solely with motor functions, such as motor coordination and motor learning (for reviews, see [1–3]). More than 25 years ago, Leiner and colleagues [4] proposed a cerebellar contribution to higher cognitive functions (for reviews, see [5, 6]) which was supported by findings of pathways connecting the cerebellum not only with motor but also with non-motor regions of the cerebral cortex (e.g. [7]).
In the motor domain, the cerebellum is supposed to predict the sensory consequences of motor actions and to learn from expectation violations, that is, the occurrence of a mismatch between prediction and sensory feedback [8, 9] (for reviews, see [10–12]). For example, impairments in saccadic adaptation seen in cerebellar dysfunction [13–15] are in accordance with a deficit in predicting the sensory consequences of movements.
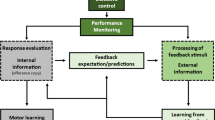
The cerebellum’s uniform anatomy and the regular loop structure of its connections with different cerebral cortical areas such as the prefrontal cortex have raised the idea of a “universal cerebellar transform,” meaning that the cerebellum has comparable functions in different behavioural domains (for reviews, see [16–20]). Given the cerebellum’s role in motor control, its core function may relate to prediction.
Predictions are known to play a fundamental role in error and feedback processing and feedback-based learning. Dopaminergic (DA) neurons of the midbrain which project both to the basal ganglia (BG) and the anterior cingulate cortex (ACC) [21, 22] (for reviews on anatomical connections, see [23, 24]) code a prediction error (for reviews, see [25, 26]). In both monkeys and humans, DA neurons’ activity increases for better than expected outcomes and decreases for worse than expected events [27] (for reviews, see [25, 26]). In accordance with the projection sites of the DA neurons, functional magnetic resonance imaging (fMRI) studies revealed prediction error-related signals in both the striatum and ACC in healthy humans [28–32].
Event-related potentials (ERPs) are frequently applied to examine the temporal dynamics of feedback processing and performance monitoring in humans. Two ERP components are typically associated with the processing of performance feedback: the feedback-related negativity (FRN) and the P300. The FRN, which is seen in the time window between 200 and 300 ms after performance feedback, is usually more pronounced for negative feedback (e.g. [33]). This early ERP component is not only supposed to reflect DA input to the ACC (for a review, see [34, 35]), but also appears to reflect a negative reward prediction error (e.g. [36, 37]). A close functional link between the FRN, on the one hand, and the error negativity [38] or error-related negativity (ERN) [39], on the other hand, has been proposed, both being linked to the DA system (for a review, see [34]). The P300 is an ERP component which follows the FRN. It peaks between 300 and 500 ms after presentation of performance feedback and has been described to be also modulated by feedback valence or magnitude. In addition, both the FRN and the P300 are strongly affected by feedback expectation (e.g. [36, 37, 40]). However, the findings regarding the types of modulations are more contradictory for the P300 than for the FRN [36, 37, 41–45] and the origin of the P300 is also less clear than the neural source of the FRN (e.g. [46, 47]; for a review, see [48]). Besides, there is evidence that the P300 can be divided into two functionally and topographically distinct sub-components, the more frontal P3a and the more parietal P3b, which are supposed to reflect different processes in feedback evaluation and decision-making (e.g. [49]; for a review, see [50]). While the P3b amplitude predicts outcome maximization, the frontal P3a seems to be associated with attentional processes and to indicate subsequent behavioural adjustment in the sense of strategy changes in decision-making tasks (e.g. [49, 51, 52]). A third component involved in feedback processing is the P200, which precedes the FRN [53]. Together with the FRN and the P300, it has recently been proposed to constitute a feedback processing complex which is sensitive to feedback valence and magnitude and has its neural sources, among other structures, in the medial frontal cortex, the ACC and posterior cingulate cortex [54].
The anatomical basis for a potential cerebellar influence on performance monitoring may be a recently detected direct cerebellar projection to the BG [55, 56] (for a review, see [57]). Moreover, both the BG and the cerebellum are connected to cortical areas such as the anterior midcingulate cortex via the thalamus (for reviews, see [5, 58–61]), possibly providing action information for online behavioural control [62, 63]. Accordingly, altered error processing as reflected in reduced ERN amplitudes was seen in BG and cerebellar lesion patients [62, 63]. Concerning feedback processing, some imaging studies have reported activations in the cerebellum (e.g. [64, 65]), although cerebellar activation is not a common finding for such tasks (see [66]). Studies on feedback learning in patients with cerebellar lesions are sparse. In one study, the reward-based acquisition of stimulus–outcome associations was spared, while a deficit in reversal learning emerged, resembling a pattern described in patients with BG lesions [67, 68]. To the best of our knowledge, feedback processing has not been assessed in cerebellar lesion patients to date. The concomitant assessment of feedback learning and feedback processing in these patients is particularly interesting, as dissociations between altered processing and spared performance are a frequent finding in cerebellar dysfunction and in the context of performance monitoring in general [62, 63], probably reflecting compensation and/or functional reorganization.
Thus, the present study aimed to examine learning from and processing of positive and negative feedback in patients with selective cerebellar lesions. It was hypothesized that lesions to the cerebellum lead to altered feedback processing and potentially also feedback learning, as the cerebellum, together with the BG, provides action-related information to the ACC in order to generate adequate predictions on action consequences. The feedback learning task that we applied assessed the ability to learn probabilistic stimulus–reward contingencies [45, 69, 70]. During the feedback learning task and also during a separate task with balanced frequencies of positive and negative outcomes, feedback processing was assessed by means of ERPs. Differences in feedback processing between patients and controls were primarily expected in the P200–FRN–P300 complex and in the ACC-driven FRN in particular.
Material and Methods
Participants
Thirty-seven subjects participated in the present study: a group of 12 patients with focal vascular cerebellar lesions caused by stroke (mean age = 49.42 years, SD = 11.02, age range = 35–69 years; seven females) and 25 healthy control subjects (mean age = 48.76 years, SD = 12.88, age range = 32–71 years; 17 females). Patients had completed 10.82 years of formal education on average (SD = 1.66; data of one patient missing) and controls 11.64 years (SD = 1.85). The subtests “picture completion” and “similarities” of a German short version of the Wechsler Adult Intelligence Scale [71] were administered to further compare the groups on intellectual abilities. Patients had a mean IQ score of 115.00 (SD = 9.58), while controls’ scores amounted to 120.57 on average (SD = 8.37; data of three controls missing). Groups were comparable with respect to mean age, general intellectual abilities and the duration of formal education (all p > 0.087 for group comparisons on the measures of interest). Participants over 60 years of age were screened for cognitive impairments (i.e. symptoms of dementia) with the Mini Mental State Examination [72]. All subjects reached at least 27 points (out of 30 points) which is the cut-off score for dementia. Exclusion criteria for study participation were current or former neurological disorders (except lesions in the cerebellum for the patients) as well as a history of severe psychiatric disorders. Five patients did, however, report depressive episodes; two patients were under antidepressive medication at the time of testing. One control subject also mentioned a former depressive episode.
Patients participated in the study, on average, 68.25 months (SD = 64.43) after the lesion event (range, 10–238 months). In the acute stage after the lesion, all (but one) patients had been treated at the Department of Neurology at the Klinikum Dortmund, Germany. Cerebellar lesions were documented with magnetic resonance imaging (3 T) by means of a standard axial T1- and T2-weighted sequences (1 × 1 × 1-mm voxel size). Lesion assessment took place during a follow-up examination at the Department of Neurology at the Klinikum Dortmund, Germany, with close temporal proximity to study participation (M = 3.71 months, SD = 1.64; range, 1–7 months). The affected brain regions were determined by visual inspection and in accordance with the classifications for cerebellar infarcts proposed by Amarenco and colleagues [73]. One patient had a cerebellar infarction in both hemispheres. All other patients showed unilateral left-sided or right-sided lesions. More detailed information on the cerebellar lesions is presented in Table 1. MR images are shown in Fig. 1. Only patients who did not report residual motor symptoms, which might have affected task performance, participated in our investigation.

Structural transversal T2-weighted MR images of cerebellar lesion locations in individual patients (for patient 7, a coronal T1-weighted MR image is added for better visualization of the lesion location)
The examination took place at the Institute of Cognitive Neuroscience, Department of Neuropsychology, Ruhr University Bochum, Germany, and took approximately 2–2.5 h. All subjects gave written informed consent before the examination started. The study was approved by the Ethics Committee of the Medical Faculty of the Ruhr University Bochum, Germany.
Cognitive Screening
Computer-Based Visual One-Back Task
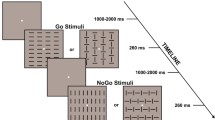
A computer-based visual one-back task was applied to guarantee that participants were able to differentiate between the Asian symbols used in the probabilistic feedback-based learning task (see “Probabilistic Feedback Learning Task” section for details of the learning task). Six Asian symbols which resembled those used in the feedback learning task served as stimuli. On each trial, one Asian symbol appeared on the computer screen for 1500 ms. Participants had to press a button within 2500 ms if the stimuli of the current and the preceding trial were identical (12 trials out of 72). We applied two different sets of six Asian symbols for each subject, one set in the one-back task and the second one in the learning task described in “Probabilistic Feedback Learning Task” section.
Visual and Verbal Short-Term and Working Memory Tasks
Visual and verbal short-term memory and working memory were investigated with the subtests “digit span” and “block span” (forward and backward) of the Wechsler Memory Scale [74].
Declarative Associative Learning Task
The verbal paired associate subtest of the Wechsler Memory Scale [74] assesses declarative associative leaning. It measures the general ability to learn associations between two stimuli. Eight word pairs are read to the subject in successive blocks. Half of the word pairs are semantically related, and four are not (referred to as “easy” and “hard” pairs, respectively). After each learning block, the first word of each pair is read and participants are asked to reproduce the corresponding second word. Learning is successful when all word pairs are correctly reproduced (at least three learning blocks; maximum six learning blocks). A delayed recall test is performed approximately 30 min after initial learning. The first word of each pair is read again, and subjects are asked to give the corresponding second word.
Probabilistic Feedback Learning Task
To assess the ability for feedback learning, participants performed a modified version of the probabilistic selection task which was introduced by Frank and colleagues [45, 69, 70]. This task consists of a learning and a transfer phase, which are described in detail below. While subjects performed the feedback learning task, ERPs were recorded to assess the processing of positive and negative feedback.
Learning Phase
In the learning phase, all participants performed at least three and a maximum of six blocks of trials, before they reached a transfer phase (see description below). Each block consisted of 60 trials. On each trial, participants had to choose one of two stimuli shown on the left and right sides of a computer monitor within 3500 ms by pressing a left or right response button. Afterwards, the chosen stimulus was surrounded by a circle and stayed on the computer screen for another 300 ms. After a short delay of 500 ms, subjects were given feedback on selection accuracy. Their choice was either rewarded (+50 cent) or punished (−20 cent). The feedback stimulus (reward or loss) was shown for 800 ms (see Fig. 2a for details of the task). We used six unfamiliar Asian symbols as stimuli (referred to as A–F) [69]. Always the same three pairs of two Asian symbols (stimuli A and B, stimuli C and D, stimuli E and F) were presented. The three stimulus pairs varied with respect to the distribution of feedback probabilities (see Fig. 2b). For stimulus pair AB, the probabilities for positive vs. negative feedback were 80/20; that is, choosing A led to positive feedback in 80 % of the choices and negative feedback followed in 20 % of the choices, while for stimulus B, the frequencies were reversed. The probabilities for positive vs. negative feedback for stimulus pairs CD and EF were 70/30 and 60/40, respectively. Each stimulus pair appeared 20 times per learning block. If subjects entered the transfer phase before the sixth block depended on whether they reached a learning criterion or not (at least 70 % correct responses for the AB pair).

Set-up of the feedback-based learning task and the fractal task (a) with stimulus pairs and reward probabilities (b for the learning task, c for the fractal task)
Transfer Phase
Latest after six blocks of learning trials, subjects entered the transfer phase, in which stimuli A and B were recombined with all other stimuli (24 trials with stimulus A, involving the pairings AC, AD, AE and AF and 24 trials with stimulus B involving BC, BD, BE and BF). Subjects did not receive feedback for their choices and were asked to choose those stimuli providing the best outcome. The analysis of transfer trials reveals the ability to learn from positive and negative feedback, which is assessed by the number of correct A choices and B avoidances in the trials involving stimuli A or B, respectively (see [69]). In addition to the new combinations, the stimulus pair AB was also presented in the transfer phase (ten trials) to control, if participants continued to favour stimulus A over B also in the absence of feedback.
Separate Task with Balanced Outcome Frequencies
As the processing of performance feedback, reflected by the ERP components FRN, P200 and P300, is strongly affected by feedback expectation (e.g. [36, 37, 40]), a different task involving different stimuli and fixed reward probabilities of 50 % for each stimulus was applied to assess the processing of positive and negative feedback without a confounding influence of the frequency of different feedback types. In order to avoid interference with the feedback learning task, we used six unfamiliar fractals as stimuli, which did not resemble the stimuli used in the feedback learning task (referred to as A–F; see Fig. 2c). Thus, the task will be referred to as fractal task in the following. Apart from the stimuli and reward probabilities, the procedures with respect to the sequence of events on a single trial and stimulus timing were identical in the fractal task and the learning task. Participants performed two blocks in the fractal task, each consisting of 60 trials. Fractals were created with the software ChaosPro (http://www.chaospro.de).
Procedure
Subjects were informed about the objective of the study and gave written informed consent according to the declaration of Helsinki. The examination started with the IQ tests, followed by the learning phases of the verbal paired associate subtest. Afterwards, electrodes were attached, the fractal task was started, and brain activity was assessed by means of electroencephalography (EEG). Then, subjects performed the delayed recall test of the verbal paired associate subtest, followed by the learning task, during which EEG was also recorded. Thereafter, the computer-based one-back task was presented and subjects performed the tests digit span and block span.
Electroencephalography Recording
EEG was recorded from 30 scalp sites with silver–silver chloride electrodes which mounted in an elastic cap: F7, F3, Fz, F4, F8, FT7, FC3, FCz, FC4, FT8, T7, C3, Cz, C4, T8, TP7, CP3, CPz, CP4, TP8, P7, P3, Pz, P4, P8, PO7, PO3, POz, PO4 and PO8, according to the International 10–20 system. A Brain Products BrainAmp Standard Amplifier (Brain Products, Munich, Germany) and the appropriate software at a sample rate of 500 Hz were used. Two electrodes were placed on the left and right mastoids. Their average served as reference for EEG recordings. At FPz, a ground electrode was positioned. Stimulus timing was controlled by Presentation Software (Neurobehavioral Systems; http://www.neuro-bs.com). Electrode impedance was kept below 10 kΩ.
Data Analysis
Electroencephalography Data Analysis
The Brain Vision Analyzer Software Package (Brain Products, Munich, Germany) and MATLAB (Mathworks, Natick, Massachusetts, USA) were applied to analyze EEG data off-line. First, band-pass filters with cutoffs of 0.5 and 40 Hz were used. To remove vertical eye movement and blink artefacts, we performed an independent component analysis (ICA) on the EEG data of each individual [75]. ICA results in an unmixing matrix separating the EEG signal into a sum of temporally independent and spatially fixed components. The number of components fits the number of channels. Each participant’s 30 components were screened for maps with a topography that might indicate artefacts caused by eye movements and blinks. Candidate components were characterized by a symmetric, frontally positive topography. Components which reflect blink artefacts typically explain a large proportion of the variance. By performing an ICA back transformation, one candidate component was then removed from the raw data. We checked back-transformed data via visual inspection for remaining artefacts. A second component was only removed, if numerous artefacts were still seen.
Feedback processing was primarily analyzed by means of ERPs obtained during the fractal task. In a second step, data from the learning task were also considered (see Supplementary Material). For analysis of feedback-related ERPs in both tasks, segments were created from 200 ms before up to 600 ms after the positive or negative feedback stimulus, followed by a baseline correction relative to the 200 ms preceding the feedback stimulus. Afterwards, trials with data points exceeding an absolute amplitude value of +/−150 μV were excluded by an automatic artefact detection algorithm. Finally, single-subject averages for positive and negative feedback were created.
Data from electrode positions FC3, FCz, FC4, P3, Pz and P4 were considered in order to explore potential group differences in the topography of ERP components. In a first step, the feedback-locked components P200, FRN and P300 in the original waveforms were analyzed for the fractal task. In accordance with previous studies (e.g. [76]), the FRN was defined as the largest negative peak amplitude in the time window between 200 and 350 ms after feedback presentation, relative to the preceding positive peak amplitude, which was scored as P200 amplitude (maximum positivity between 150 ms after feedback onset and the latency of the negative peak). For the P300, the largest positive peak in the time window between 350 and 450 ms after feedback presentation was examined. For all components, peak latencies were also considered as an indicator of the timing of feedback processing. Then, the data were also analyzed with a difference wave approach by subtracting the ERPs after positive feedback from those after negative feedback to assess between-group differences in feedback processing in the P200–FRN–P300 complex not directly related to one of the three components. Mean amplitudes in the P200–FRN–P300 complex consistently yield differences between positive and negative feedback valence [54]. Finally, the same analyses were conducted for the ERPs obtained during the learning task to explore, if the pattern of results was comparable between both tasks. Here, analyses were restricted to the first three blocks of trials because these were conducted by all subjects.
Statistical Design and Analysis
Behavioural data of the background and experimental tasks as well as EEG data were analyzed with analyses of variance (ANOVAs). Greenhouse–Geisser corrections were applied, if sphericity was violated. We only report main effects and interactions involving the between-subjects factor GROUP (patients vs. controls) for ANOVA results. T tests for paired samples and independent samples were also applied, where appropriate. EEG findings for the fractal task are reported in the “Results” section, those for the probabilistic feedback learning task in the Supplementary Material section. For the analysis of the ERPs in the fractal task, we had to exclude one patient due to technical data acquisition problems.
Results
Cognitive Screening
Computer-Based Visual One-Back Task
Analyses with t tests for independent samples did not reveal any significant differences between patients and controls concerning the reaction times and the number of misses and errors (all p > 0.327; see Table 2 for means and standard deviations of the respective measures).
Visual and Verbal Short-Term and Working Memory Tasks
Patients and controls did not differ in any of the visual and verbal short-term memory and working memory tasks (block span and digit span, forward and backward; all p > 0.209; see Table 2).
Declarative Associative Learning Task
Table 2 also provides descriptive data for the immediate and delayed recall performance in the declarative associative learning task of patients and controls. ANOVA for the immediate recall performance with the between-subjects factor GROUP (patients vs. controls) and the within-subjects factors BLOCK (1 to 3) and DIFFICULTY (easy vs. hard) did not reveal a significant main effect of GROUP or significant interactions with the factor GROUP (all p > 0.066). Only the interaction GROUP × BLOCK was marginally significant, indicating a stronger increase of the scores for patients (p = 0.066). ANOVA of the delayed recall performance with the between-subjects factor GROUP and the within-subjects factor DIFFICULTY showed a marginally significant effect of GROUP, with higher scores for controls (p = 0.055). The interaction GROUP × DIFFICULTY did not reach significance (p = 0.178).
Probabilistic Feedback Learning Task: Behavioural Data
Learning Phase
Figure 3 shows the learning performance of patients and controls in the probabilistic learning task. An ANOVA with the between-subjects factor GROUP and the within-subjects factors BLOCK (1 to 3) and PAIR (AB vs. CD vs. EF) was performed. The main effect of GROUP and interactions with the factor GROUP did all not reach significance (all p > 0.198).

Behavioural data: learning performance for stimulus pairs AB, CD and EF for patients (a) and healthy control subjects (b). Error bars represent standard errors
Transfer Phase
As transfer phase performance can only be interpreted, if subjects learned to prefer stimulus A over B in the learning phase (see [69]), only those subjects entered transfer phase analysis who reached at least 70 % correct responses for stimulus pair AB latest in block 6. Nine patients and 22 controls reached this criterion.
ANOVA on transfer phase performance with the between-subjects factor GROUP and the within-subjects factor LEARNING TENDENCY (learning from positive vs. negative feedback) did not reveal a significant main effect of GROUP or an interaction with GROUP (patients’ choices of stimulus A in percent: M = 86, SD = 13; avoidance of stimulus B: M = 58, SD = 35.08; controls’ choices of stimulus: M = 73, SD = 21; avoidance of stimulus B: M = 68, SD = 21) (both p > 0.108).
Event-Related Potential Data
As outlined in the “Material and Methods” section, ERP data from the fractal task were primarily analyzed. Figure 4 shows the original waveforms after positive and negative feedback in the fractal task at electrodes FC3, FCz, FC4, P3, Pz and P4 for patients and healthy controls. Topographies of two of the analyzed components can be found in Fig. 5. Figure 6 depicts the punishment–reward difference waves at six electrodes for patients and controls and the respective topographies. ERP data obtained in the feedback learning task are reported in the Supplementary Material section.

ERP data: grand average feedback-locked ERPs for positive and negative feedback processing in the fractal task for patients and healthy control subjects at six electrode sites (FC3, FCz, FC4, P3, Pz, P4)

Topographic maps: topographies of a the FRN peak following negative feedback in patients and controls (amplitude relative to preceding positive peak) and b the P300 peak after positive and negative feedback in patients and controls

Difference waves: a Punishment–reward difference waves from the fractal task for patients and controls at six electrode sites. Horizontal lines above the waveforms indicate time windows of significant amplitude differences between groups as revealed by t tests in consecutive 10-ms time frames. b Topographies of the mean difference signal between 250 and 450 ms after feedback in patients and controls
Fractal Task: Original Waveforms
P200
Both ANOVAs on P200 amplitudes and latencies with the within-subjects factors FEEDBACK TYPE (positive vs. negative), LATERALITY (left vs. right) and ROW (frontal vs. parietal) and the between-subjects factor GROUP did not reveal any significant main effects or interactions with the factor GROUP (all p > 0.175).
Feedback-Related Negativity
For FRN amplitudes, the interaction FEEDBACK TYPE × GROUP reached significance (F(1.000, 34.000) = 5.420, p = 0.026; see above for factors involved in the ANOVA). Patients showed higher FRN amplitudes after negative (M = −5.10, SD = 2.36) than positive (M = −3.52, SD = 2.00) feedback (t(10) = 2.871, p = 0.017), while controls’ FRN amplitudes after positive (M = −3.97, SD = 1.92) vs. negative feedback (M = −4.15, SD = 1.94) did not differ significantly (p = 0.580). All other interactions with the factor group did not reach significance (p > 0.085). Topographic maps of the FRN following negative feedback (see Fig. 5a) indicate that the negativity is most pronounced at frontocentral electrode sites in controls, whereas it is more diffusely distributed in the patients. The analysis of FRN latencies (by means of an ANOVA with the same factors as reported above) did not yield any significant GROUP effects (all p > 0.101 for the main effect and the interactions).
P300
Also for P300 amplitude, the interaction GROUP × FEEDBACK TYPE reached significance (F(1.000,34.000) = 4.160, p = 0.049). Cerebellar patients had larger P300 amplitudes after positive (M = 11.95, SD = 2.57) than negative feedback (M = 9.80, SD = 3.56; t(10) = 3.728, p = 0.004). For controls, the comparison of P300 amplitudes after negative (M = 10.43, SD = 4.67) vs. positive (M = 11.17, SD = 4.22) feedback failed to reach significance (p = 0.065). As can be seen in the topographic maps in Fig. 5b, P300 amplitudes are similar at frontal and parietal sites in controls. In the patients, the P300 for both positive and negative feedback is, however, slightly more pronounced at frontal sites. Finally, P300 latencies were not significantly affected by whether subjects belonged to the group of patients or healthy controls (all p > 0.121).
Fractal Task: Difference Waves
Visual inspection of the difference waves (punishment–reward; see Fig. 6a) suggests that the differences between negative and positive feedback processing as well as the between-group differences in this measure span the whole P200–FRN–P300 complex. For each of the six electrodes analyzed, mean amplitudes of the punishment–reward difference waves were compared between patients and controls by means of t tests in consecutive 10-ms time windows, starting from 200 up to 500 ms after feedback presentation. This approach aimed to (a) identify time windows in which reliable differences between groups occurred across different electrode sites and (b) yield information on the onset of processing differences between patients and controls at different scalp locations. The horizontal lines above the difference waveforms in Fig. 6 indicate time windows of significant amplitude difference for each single electrode. Comparable patterns of amplitude differences were found at frontal and parietal electrode sites, with the earliest significant differences between 240 and 260 ms after feedback presentation: Patients showed generally higher amplitudes than controls. At parietal sites, however, the time window of significant differences between patients and controls is longer compared to frontal electrode sites, extending beyond 450 ms. No obvious laterality effects were seen for the strength, onset or offset time of the between-group amplitude differences.
Overall, difference wave amplitudes differed most strongly between groups between 250 and 450 ms. An analysis of mean amplitudes in this time window with the factors, ROW, LATERALITY and GROUP showed significantly enhanced difference wave amplitudes for cerebellar lesion patients compared to controls (main effect of GROUP: F(1,34) = 6.639, p = 0.014). No interactions involving the GROUP factor were seen (all p > 0.261). The topography of the difference wave in this time window (Fig. 6b) clearly shows that the amplitude difference between negative and positive feedback processing is pronounced over the whole scalp for the patients. In comparison, the topographic map in controls reflects the overall reduced amplitude of the difference wave.
Discussion
The present study analyzed learning from and processing of positive and negative monetary feedback in patients with selective cerebellar lesions and healthy controls. Patients and controls did not differ regarding their general learning performance. Feedback processing was assessed by means of ERPs. The first analysis focused on the three components P200, FRN and P300, which have previously been related to performance feedback. For both the FRN and the P300, amplitude differences between negative and positive feedback were seen in cerebellar lesion patients but not controls. This was also reflected in an additional analysis on punishment–reward difference waves, for which significant group effects emerged in the P200–FRN–P300 complex between 250 and 450 ms after feedback presentation. Cerebellar lesion patients showed higher difference wave amplitudes than controls in this time window, indicating more pronounced differences in the processing of negative and positive feedback than in controls. Furthermore, the result pattern on the descriptive level suggested that ERPs following reward were particularly altered in the patients. These results were obtained in an experiment with balanced probabilities for positive and negative feedback (“fractal task”), but a similar pattern also emerged for the ERPs of the feedback learning task (see Supplementary Material). While the analysis of the original waveforms did not yield the same effects, pronounced differences between patients and controls were indeed also seen in the difference wave analysis of the learning task, albeit somewhat weaker and with a later onset than in the fractal task.
The ERP differences between patients and controls can thus not clearly be ascribed to a particular ERP component. They rather appear to span a time window which has recently been described as the P200–FRN–P300 complex and in which processing has frequently been linked to performance feedback (e.g. [33, 37]). It is likely, however, that the neural processes underlying the FRN significantly contributed to the processing differences between patients and controls. On the one hand, analysis of the fractal task data did reveal FRN differences between patients and controls. Moreover, many researchers define the FRN based on the non-reward–reward difference wave in a broad time window comparable to or even longer than the one for which we found group effects in the difference wave analysis in the present study (250 to 450 ms) (e.g. [37, 77]). This definition of the FRN is based on the consistent finding that mean amplitudes between 200 and 300 ms after feedback presentation, but also earlier and later, are valence dependent, being more negative for negative feedback (e.g. [33, 34]). At first sight, the results of the present investigation where healthy controls did not show differences between positive and negative feedback processing appear to contradict this. Interestingly, however, processing in the mentioned time window has also been related to feedback expectation [36, 37, 77]. The valence effect itself was ascribed to systematic differences in the expectation of positive and negative feedback. In many studies, negative feedback is less frequent than positive feedback and thus more unexpected. In designs with balanced feedback probabilities, an “overoptimistic bias,” that is, subjectively higher expectations for positive outcomes, has been made responsible for the valence effect [78]. In fact, Ferdinand and colleagues [76] found positive and negative feedback to generate FRNs of comparable size if both feedback types were equally (un)expected (cf. also [78, 79]), suggesting that the FRN and, thus, feedback processing by the ACC are mainly driven by feedback expectancy. This finding is in line with a recent model proposed by Alexander and Brown [80] which assumes that the medial prefrontal cortex, especially the ACC, works as a general action–outcome predictor, by taking into account the (un)expectedness of the delivered feedback, irrespective of its valence. In the fractal task of the present investigation, positive and negative feedback were equally likely to occur and could not be predicted. Furthermore, the use of six different and not-easy-to-remember fractal stimuli may have prevented an overoptimistic bias in study participants. Following the reasoning of the model by Alexander and Brown [80], both types of feedback were thus similarly (un)expected with a prediction error of about 50 % for each outcome and should elicit similar ERPs. Exactly, this was observed in healthy controls of the present study.
In contrast to the control group, the patient group showed processing differences between feedback types. ERPs were overall more negative for negative than for positive feedback. This modified ERP pattern could be explained by altered feedback prediction and is thus in line with our assumption that the cerebellum is critically involved in generating action–outcome predictions. Hence, cerebellar patients seemed—on average—more surprised by both positive and negative feedback than controls.
The cerebellum may exert its role in feedback prediction via anatomical connections with structures of the so-called reward system, with interactions between the cerebellum and the BG being of particular interest [55, 56] (for a review, see [57]). The cerebellum and the BG are linked to the cortex via the thalamus (for reviews, see [5, 58–61]), e.g. with the anterior midcingulate cortex [81]. Importantly, in both BG and cerebellar lesion patients, error processing is altered: The ERN for errors compared to correct responses is reduced. Both structures thus appear to provide action information for online performance monitoring [62, 63]. At the same time, these findings are highly compatible with the interpretation of impaired outcome prediction in the cerebellar lesion patients of the present study. The cerebellum would thus be involved in predicting the outcomes of actions and would have a comparable role in motor control and in performance monitoring, as was suggested by recent reviews on cerebellar anatomy and function [5, 17].
As was described above, the processing differences between patients and controls extended into the P300 period. Contrary to the FRN, the P300 is regarded as an indicator of conscious cognitive processes [82–84]. The longer latency of the P300 compared to the FRN and potential hippocampal and neocortical contributions (for a review, see [48]) allow the assumption that the P300 reflects more declarative stages of feedback processing. Accordingly, the patients may have made more use of declarative strategies compared to controls to compensate for feedback prediction deficits and reach normal feedback learning performance. This assumption is somewhat corroborated by the topographic maps of the P300. While the P300 in controls was quite evenly distributed across the scalp for both feedback types, a stronger frontal than parietal signal was seen in the patients, suggesting the use of strategies mediated by the prefrontal cortex.
The P300 consists of two sub-components, P3a and P3b (e.g. [49]). In the present investigation, the P300 differences between patients and controls emerged in a time window up to 450 ms after feedback presentation and thus in the typical time window of the P3a, which is frontally more pronounced (for a review, see [50]). The P3a is associated with stimulus-driven attentional processes and allocation [50, 51] and is therefore also in line with other interpretations in the context of reward processing, which link the P300 to expectancy [36, 37, 40], as unexpected stimuli automatically catch attention. The P300 finding therefore adds to the results in the earlier FRN time window, suggesting that reward expectancy and, thus, prediction differed between patients and controls. The frontally pronounced topography of the P300 in the patients also supports an interpretation as P3a and might indicate a compensatory process.
Neuroimaging evidence for a cerebellar role in feedback processing is sparse to date. Some studies did report cerebellar activations [64, 65, 85], but a recent meta-analysis on reward processing did not report cerebellar activations [66]. One reason for this finding may be that often not the whole cerebellum is scanned in functional imaging studies, so that the involvement of the cerebellum in this process is underestimated. For error processing which is tightly linked to feedback learning and feedback evaluation, the cerebellum was found to be important in neuroimaging studies (e.g. [86]).
Conclusion
Overall, the present study provides first evidence for alterations of feedback processing in patients with selective cerebellar lesions. Compared to healthy controls, the feedback-locked ERPs of cerebellar lesion patients more clearly distinguished between negative and positive feedback, as was reflected in both the FRN and the P300. Group differences were most pronounced, however, when the P200–FRN–P300 complex was considered as a whole in a difference wave approach. The results extend our current knowledge of cerebellar functions and support the assumption of a cerebellar contribution to prediction also in the context of performance feedback. Largely intact learning accompanied by modified feedback processing hints at a compensatory mechanism which could be related to different learning strategies and a stronger involvement of the frontal cortex. This interpretation is, however, speculative at the moment and needs to be investigated further.
References
Thach WT, Goodkin HP, Keating JG. The cerebellum and the adaptive coordination of movement. Annu Rev Neurosci. 1992;15:403–42.
Llinas R, Welsh JP. On the cerebellum and motor learning. Curr Opin Neurobiol. 1993;3:958–65.
Glickstein M, Yeo C. The cerebellum and motor learning. J Cogn Neurosci. 1990;2:69–80.
Leiner HC, Leiner AL, Dow RS. Does the cerebellum contribute to mental skills? Behav Neurosci. 1986;100:443–54.
Strick PL, Dum RP, Fiez JA. Cerebellum and nonmotor function. Annu Rev Neurosci. 2009;32:413–34.
Timmann D, Daum I. Cerebellar contributions to cognitive functions: a progress report after two decades of research. Cerebellum. 2007;6:159–62.
Middleton FA, Strick PL. Anatomical evidence for cerebellar and basal ganglia involvement in higher cognitive function. Science. 1994;266:458–61.
Popa LS, Hewitt AL, Ebner TJ. Predictive and feedback performance errors are signaled in the simple spike discharge of individual Purkinje cells. J Neurosci. 2012;32:15345–58.
Ramnani N, Toni I, Josephs O, Ashburner J, Passingham RE. Learning- and expectation-related changes in the human brain during motor learning. J Neurophysiol. 2000;84:3026–35.
Blakemore SJ, Sirigu A. Action prediction in the cerebellum and in the parietal lobe. Exp Brain Res. 2003;153:239–45.
Shadmehr R, Smith MA, Krakauer JW. Error correction, sensory prediction, and adaptation in motor control. Annu Rev Neurosci. 2010;33:89–108.
Bellebaum C, Daum I. Mechanisms of cerebellar involvement in associative learning. Cortex. 2011;47:128–36.
Xu-Wilson M, Chen-Harris H, Zee DS, Shadmehr R. Cerebellar contributions to adaptive control of saccades in humans. J Neurosci. 2009;29:12930–9.
Golla H, Tziridis K, Haarmeier T, Catz N, Barash S, Thier P. Reduced saccadic resilience and impaired saccadic adaptation due to cerebellar disease. Eur J Neurosci. 2008;27:132–44.
Barash S, Melikyan A, Sivakov A, Zhang M, Glickstein M, Thier P. Saccadic dysmetria and adaptation after lesions of the cerebellar cortex. J Neurosci. 1999;19:10931–9.
Ramnani N. Frontal lobe and posterior parietal contributions to the cortico-cerebellar system. Cerebellum. 2012;11:366–83.
Ramnani N. The primate cortico-cerebellar system: anatomy and function. Nat Rev Neurosci. 2006;7:511–22.
Schmahmann JD. Disorders of the cerebellum: ataxia, dysmetria of thought, and the cerebellar cognitive affective syndrome. J Neuropsychiatry Clin Neurosci. 2004;16:367–78.
Ito M. Control of mental activities by internal models in the cerebellum. Nat Rev Neurosci. 2008;9:304–13.
Ito M. Movement and thought: identical control mechanisms by the cerebellum. Trends Neurosci. 1993;16:448–50.
Williams SM, Goldman-Rakic PS. Characterization of the dopaminergic innervation of the primate frontal cortex using a dopamine-specific antibody. Cereb Cortex. 1993;3:199–222.
Gaspar P, Berger B, Febvret A, Vigny A, Henry JP. Catecholamine innervation of the human cerebral cortex as revealed by comparative immunohistochemistry of tyrosine hydroxylase and dopamine-beta-hydroxylase. J Comp Neurol. 1989;279:249–71.
Smith AD, Bolam JP. The neural network of the basal ganglia as revealed by the study of synaptic connections of identified neurones. Trends Neurosci. 1990;13:259–65.
Berger B, Gaspar P, Verney C. Dopaminergic innervation of the cerebral cortex: unexpected differences between rodents and primates. Trends Neurosci. 1991;14:21–7.
Schultz W, Dickinson A. Neuronal coding of prediction errors. Annu Rev Neurosci. 2000;23:473–500.
Schultz W, Dayan P, Montague PR. A neural substrate of prediction and reward. Science. 1997;275:1593–9.
Zaghloul KA, Blanco JA, Weidemann CT, McGill K, Jaggi JL, Baltuch GH, et al. Human substantia nigra neurons encode unexpected financial rewards. Science. 2009;323:1496–9.
Orr C, Hester R. Error-related anterior cingulate cortex activity and the prediction of conscious error awareness. Front Hum Neurosci. 2012;6:177. doi:10.3389/fnhum.2012.00177.
Amiez C, Sallet J, Procyk E, Petrides M. Modulation of feedback related activity in the rostral anterior cingulate cortex during trial and error exploration. Neuroimage. 2012;63:1078–90.
Jocham G, Klein TA, Ullsperger M. Dopamine-mediated reinforcement learning signals in the striatum and ventromedial prefrontal cortex underlie value-based choices. J Neurosci. 2011;31:1606–13.
Seymour B, Daw N, Dayan P, Singer T, Dolan R. Differential encoding of losses and gains in the human striatum. J Neurosci. 2007;27:4826–31.
Robinson OJ, Frank MJ, Sahakian BJ, Cools R. Dissociable responses to punishment in distinct striatal regions during reversal learning. Neuroimage. 2010;51:1459–67.
Miltner WH, Braun CH, Coles MGH. Event-related brain potentials following incorrect feedback in a time-estimation task: evidence for a generic neural system for error detection. J Cogn Neurosci. 1997;9:788–98.
Holroyd CB, Coles MG. The neural basis of human error processing: reinforcement learning, dopamine, and the error-related negativity. Psychol Rev. 2002;109:679–709.
Gehring WJ, Willoughby AR. The medial frontal cortex and the rapid processing of monetary gains and losses. Science. 2002;295:2279–82.
Bellebaum C, Daum I. Learning-related changes in reward expectancy are reflected in the feedback-related negativity. Eur J Neurosci. 2008;27:1823–35.
Hajcak G, Moser JS, Holroyd CB, Simons RF. It’s worse than you thought: the feedback negativity and violations of reward prediction in gambling tasks. Psychophysiology. 2007;44:905–12.
Falkenstein M, Hohnsbein J, Hoormann J, Blanke L. Effects of errors in choice reaction tasks on the ERP under focused and divided attention. In: Brunia CHM, Gaillard AWK, Kok A, editors. Psychophysiological brain research. Tilburg: Tilburg University Press; 1990. p. 192–5.
Gehring WJ, Goss B, Coles MGH, Meyer DE, Donchin E. A neural system for error detection and compensation. Psychol Sci. 1993;4:385–90.
Pfabigan DM, Alexopoulos J, Bauer H, Sailer U. Manipulation of feedback expectancy and valence induces negative and positive reward prediction error signals manifest in event-related brain potentials. Psychophysiology. 2011;48:656–64.
Bellebaum C, Kobza S, Thiele S, Daum I. Processing of expected and unexpected monetary performance outcomes in healthy older subjects. Behav Neurosci. 2011;125:241–51.
Bellebaum C, Polezzi D, Daum I. It is less than you expected: the feedback-related negativity reflects violations of reward magnitude expectations. Neuropsychologia. 2010;48:3343–50.
Sato A, Yasuda A, Ohira H, Miyawaki K, Nishikawa M, Kumano H, et al. Effects of value and reward magnitude on feedback negativity and P300. Neuroreport. 2005;16:407–11.
Yeung N, Sanfey AG. Independent coding of reward magnitude and valence in the human brain. J Neurosci. 2004;24:6258–64.
Frank MJ, Woroch BS, Curran T. Error-related negativity predicts reinforcement learning and conflict biases. Neuron. 2005;47:495–501.
Fushimi M, Matsubuchi N, Sekine A. Progression of P300 in a patient with bilateral hippocampal lesions. Clin Neurophysiol. 2005;116:625–31.
Ludowig E, Bien CG, Elger CE, Rosburg T. Two P300 generators in the hippocampal formation. Hippocampus. 2010;20:186–95.
Linden DE. The P300: where in the brain is it produced and what does it tell us? Neuroscientist. 2005;11:563–76.
Kopp B, Lange F. Electrophysiological indicators of surprise and entropy in dynamic task-switching environments. Front Hum Neurosci. 2013;7:300. doi:10.3389/fnhum.2013.00300.
Polich J. Updating P300: an integrative theory of P3a and P3b. Clin Neurophysiol. 2007;118:2128–48.
Zhang DD, Gu RL, Wu TT, Broster LS, Luo Y, Jiang Y, et al. An electrophysiological index of changes in risk decision-making strategies. Neuropsychologia. 2013;51:1397–407.
San Martin R, Appelbaum LG, Pearson JM, Huettel SA, Woldorff MG. Rapid brain responses independently predict gain maximization and loss minimization during economic decision making. J Neurosci. 2013;33:7011–9.
Potts GF, Martin LE, Burton P, Montague PR. When things are better or worse than expected: the medial frontal cortex and the allocation of processing resources. J Cogn Neurosci. 2006;18:1112–9.
West R, Bailey K, Anderson S, Kieffaber PD. Beyond the FN: a spatio-temporal analysis of the neural correlates of feedback processing in a virtual Blackjack game. Brain Cogn. 2014;86:104–15.
Bostan AC, Dum RP, Strick PL. The basal ganglia communicate with the cerebellum. Proc Natl Acad Sci U S A. 2010;107:8452–6.
Hoshi E, Tremblay L, Feger J, Carras PL, Strick PL. The cerebellum communicates with the basal ganglia. Nat Neurosci. 2005;8:1491–3.
Bostan AC, Strick PL. The cerebellum and basal ganglia are interconnected. Neuropsychol Rev. 2010;20:261–70.
Haber SN, Calzavara R. The cortico-basal ganglia integrative network: the role of the thalamus. Brain Res Bull. 2009;78:69–74.
Alexander GE, DeLong MR, Strick PL. Parallel organization of functionally segregated circuits linking basal ganglia and cortex. Annu Rev Neurosci. 1986;9:357–81.
McHaffie JG, Stanford TR, Stein BE, Coizet V, Redgrave P. Subcortical loops through the basal ganglia. Trends Neurosci. 2005;28:401–7.
Middleton FA, Strick PL. Basal ganglia and cerebellar loops: motor and cognitive circuits. Brain Res Brain Res Rev. 2000;31:236–50.
Peterburs J, Gajda K, Koch B, Schwarz M, Hoffmann KP, Daum I, et al. Cerebellar lesions alter performance monitoring on the antisaccade task—an event-related potentials study. Neuropsychologia. 2012;50:379–89.
Ullsperger M, von Cramon DY. The role of intact frontostriatal circuits in error processing. J Cogn Neurosci. 2006;18:651–64.
Berns GS, McClure SM, Pagnoni G, Montague PR. Predictability modulates human brain response to reward. J Neurosci. 2001;21:2793–8.
Ramnani N, Elliott R, Athwal BS, Passingham RE. Prediction error for free monetary reward in the human prefrontal cortex. Neuroimage. 2004;23:777–86.
Liu X, Hairston J, Schrier M, Fan J. Common and distinct networks underlying reward valence and processing stages: a meta-analysis of functional neuroimaging studies. Neurosci Biobehav Rev. 2011;35:1219–36.
Bellebaum C, Koch B, Schwarz M, Daum I. Focal basal ganglia lesions are associated with impairments in reward-based reversal learning. Brain. 2008;131:829–41.
Thoma P, Bellebaum C, Koch B, Schwarz M, Daum I. The cerebellum is involved in reward-based reversal learning. Cerebellum. 2008;7:433–43.
Frank MJ, Seeberger LC, O’reilly RC. By carrot or by stick: cognitive reinforcement learning in parkinsonism. Science. 2004;306:1940–3.
Frank MJ, Kong L. Learning to avoid in older age. Psychol Aging. 2008;23:392–8.
Dahl G. WIP—Reduzierter Wechsler Intelligenztest: Anwendung, Auswertung, statistische Analysen, Normwerte. Meisenheim: Hain; 1986.
Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12:189–98.
Amarenco P, Kase CS, Rosengart A, Pessin MS, Bousser MG, Caplan LR. Very small (border zone) cerebellar infarcts. Distribution, causes, mechanisms and clinical features. Brain. 1993;116:161–86.
Wechsler D. Wechsler Memory scale—revised. London: Psychological Corporation; 1987.
Lee TW, Girolami M, Sejnowski TJ. Independent component analysis using an extended infomax algorithm for mixed subgaussian and supergaussian sources. Neural Comput. 1999;11:417–41.
Ferdinand NK, Mecklinger A, Kray J, Gehring WJ. The processing of unexpected positive response outcomes in the mediofrontal cortex. J Neurosci. 2012;32:12087–92.
Holroyd CB, Krigolson OE, Baker R, Lee S, Gibson J. When is an error not a prediction error? An electrophysiological investigation. Cogn Affect Behav Neurosci. 2009;9:59–70.
Oliveira FTP, McDonald JJ, Goodman D. Performance monitoring in the anterior Cingulate is not all error related: expectancy deviation and the representation of action-outcome associations. J Cogn Neurosci. 2007;19:1994–2004.
Jessup RK, Busemeyer JR, Brown JW. Error effects in anterior cingulate cortex reverse when error likelihood is high. J Neurosci. 2010;30:3467–72.
Alexander WH, Brown JW. Medial prefrontal cortex as an action-outcome predictor. Nat Neurosci. 2011;14:1338–44.
Seifert S, von Cramon DY, Imperati D, Tittgemeyer M, Ullsperger M. Thalamocingulate interactions in performance monitoring. J Neurosci. 2011;31:3375–83.
Ridderinkhof KR, Ramautar JR, Wijnen JG. To P(E) or not to P(E): a P3-like ERP component reflecting the processing of response errors. Psychophysiology. 2009;46:531–8.
Sommer W, Matt J. Awareness of P300-related cognitive processes: a signal detection approach. Psychophysiology. 1990;27:575–85.
Sommer W, Matt J, Leuthold H. Consciousness of attention and expectancy as reflected in event-related potentials and reaction times. J Exp Psychol Learn Mem Cogn. 1990;16:902–15.
Kobza S, Bellebaum C. Processing of action- but not stimulus-related prediction errors differs between active and observational feedback learning. Neuropsychologia. 2015;66:75–87.
Ide JS, Li CSR. A cerebellar thalamic cortical circuit for error-related cognitive control. Neuroimage. 2011;54:455–64.
Acknowledgments
This work was supported by the Ministry of Innovation, Science and Research of the federal state of Nordrhein-Westfalen, Germany (Ministerium für Innovation, Wissenschaft und Forschung des Landes Nordrhein-Westfalen; MIWF [grant number 334-4]).
Compliance with Ethical Standards
ᅟ
Conflict of Interest
The authors declare that they have no conflict of interest.
Research Involving Human Participants: Statement of Human Rights
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Rustemeier, M., Koch, B., Schwarz, M. et al. Processing of Positive and Negative Feedback in Patients with Cerebellar Lesions. Cerebellum 15, 425–438 (2016). https://doi.org/10.1007/s12311-015-0702-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12311-015-0702-8