
Abstract
Cardiac markers are used to evaluate functions of heart. However, there are no satisfactory cardiac biomarkers for the diagnosis of acute myocardial infarction (AMI) within 4 h of onset of chest pain. Among novel cardiac markers, glycogen phosphorylase BB (GPBB) is of particular interest as it is increased in the early hours after AMI. The present study was conducted with the objective to find out the sensitivity and specificity of GPBB over other cardiac markers i.e. myoglobin and CKMB in patients of AMI within 4 h after the onset of chest pain. The study includes 100 AMI patients and 100 normal healthy individuals as controls. In all the cases and controls, serum GPBB and myoglobin concentrations were measured by ELISA where as CK-MB was measured by diagnostic kit supplied by ERBA. The sensitivity and specificity of glycogen phosphorylase BB (GPBB) were greater than CK-MB and myoglobin in patients of AMI within 4 h after the onset of chest pain. Hence, glycogen phosphorylase BB (GPBB) can be used as additional biomarker for the early diagnosis of AMI.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Acute myocardial infarction (AMI) is the significant cause of morbidity and mortality worldwide [1]. It is more commonly known as heart attack, is a common presentation of ischemic heart disease or coronary artery disease. It is a medical condition that occurs when a coronary artery is severely blocked by vulnerable plaque and as a result of that, there is a significant reduction in the blood supply [2]. The mortality rate of myocardial infarction is approximately 30% and for every 1 in 25 patients who survive the initial hospitalization, dies in the first year after AMI. Indians are four time more prone to AMI as compared to the people of other countries due to a combination of the genetic and lifestyle factors that promote metabolic dysfunction [3].
Chest pain is one of the commonest complaints among patients presenting to cardiology department [4]. By accurately ruling out chest pain of cardiac origin, 40% of patients presenting with acute chest pain could be spared from the risks and costs of unnecessary hospital admission and more invasive cardiac testing [5]. Early accurate diagnosis and treatment of acute myocardial infarction can reduce the mortality and morbidity. Majority of deaths due to AMI occur during the first hour after the onset of symptoms. If AMI cases are diagnosed and treated effectively during the first hour after the onset of symptoms, the mortality can be reduced from 9 to 3% but if delayed, mortality can be 5 times higher [6]. However, there are no reliable tests available for the diagnosis of AMI in the early hours after the onset of symptoms. Electrocardiographic (ECG) has only 50–60% sensitivity for the diagnosis of myocardial necrosis [7]. Myoglobin which appears in the blood within 2 h after myocardial infarction lacks specificity [5]. Similarly, CKMB starts to rise within 3–5 h after onset of AMI and lack sensitivity [8].
Glycogen phosphorylase BB, a new cardiac marker has been discussed in recent year as a potentially useful biomarker in the early detection of ischemia [9, 10]. GPBB is a fundamental enzyme in the regulation of carbohydrate metabolism by mobilization of glycogen. Three different isoenzymes of glycogen phosphorylase (GP) exist; GPMM (present in muscles), GPLL (liver) and GPBB (brain and heart muscles) [11]. Glycogen phosphorylase-BB appears to be released into the circulation 2–4 h after myocardial injury [12]. Hence, this study has been aimed to find out the sensitivity and specificity of GPBB over other cardiac markers i.e. myoglobin and CKMB in patients of AMI within 4 h after the onset of severe chest pain.
Materials and Methods
This study has been conducted in the Department of Biochemistry and Department of Cardiology, G.R. Medical College and J.A. Group of Hospitals, Gwalior. The study included 200 subjects (both sex) of age group 35–75 years. Out of them, 100 were normal healthy individuals as controls and 100 of them were patients of AMI admitted to the Cardiology Department of J.A. Group of Hospitals. Each patient undergone clinical and laboratory evaluation, which included the detailed clinical history, clinical examination, ECG, chest X-ray, routine blood investigations and cardiac biomarkers (CK-MB and cTnT [card test]) as a part of routine assessment and diagnosis of AMI was made after review of all the above information by cardiologist.
Inclusion Criteria
The patients arriving to the Cardiology Department within 4 h of onset of chest pain.
Exclusion Criteria
The patients arriving to hospital after 4 h of onset of chest pain, those with diabetes mellitus, chronic muscle disease, renal disease, liver disease, recent surgery, implanted pacemaker, autoimmune disease and arthritis.
This study has been approved by the Institutional Ethical Clearance Committee and written informed consent was obtained from all the study participants.
About 5 ml of venous blood sample was taken from AMI cases (within 4 h of chest pain) and controls under all aseptic precautions. Serum was separated and kept at −200 C until the analysis was carried out. GPBB and myoglobin were measured by ELISA whereas CKMB was measured by the diagnostic kit supplied by ERBA.
Statistical Analysis
Data are presented as mean ± standard deviation. The statistical differences between cases and controls were determined by student independent sample t test. Data analyses were performed with the Statistical Package for the Social Sciences, version 21.0 (SPSS, Chicago, Illinois, USA). Sensitivity, specificity, positive and negative predictive values were calculated and receiver operating characteristic (ROC) curve analysis was performed with the help of StatsDirect 3.
Results
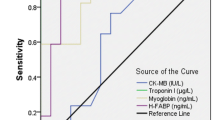
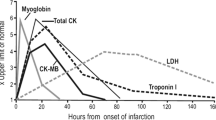
A total of 200 subjects were included in this study. Of these, 100 were cases of AMI and rest 100 were controls. Figure 1 shows the mean levels of GPBB and myoglobin in AMI and control subjects. Figure 2 shows the mean levels of CKMB in AMI and control subjects. The mean levels of cardiac markers GPBB, myoglobin and CKMB activity were higher in AMI cases when compared to that of controls and were statistically significant at p < 0.001. Table 1 shows sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) of GPBB which were greater than myoglobin and CKMB. Figures 3, 4, 5 show ROC curve analysis of GPBB, myoglobin, CKMB having area under the curve (AUC) 0.993, 0.964 and 0.691 respectively.

Shows the mean levels of GPBB and myoglobin in AMI and control subjects

Shows the mean levels of CKMB in AMI and control subjects

The ROC curve analysis of GPBB within 4 h of onset of acute myocardial infarction

The ROC curve analysis of myoglobin within 4 h of onset of acute myocardial infarction

The ROC curve analysis of CKMB within 4 h of onset of acute myocardial infarction
Discussion
AMI is the major cause of mortality and long-term morbidity in the modern world [13]. Myocardial ischemia results from the reduction of coronary flow to such an extent that supply of oxygen to the myocardium does not meet the oxygen demand of myocardial tissue. When this ischemia is prolonged and irreversible, then myocardial cell death and necrosis occur which is defined as myocardial infarction [14]. Early and correct diagnosis of AMI is of utmost important to enable the immediate and intensified treatment which consequently reduces the mortality [13]. Although CKMB, myoglobin and cardiac troponin start to rise early after the onset of AMI, lacks sensitivity and specificity.
In the recent years, several alternative markers like ischemia modified albumin [15], heart fatty acid binding protein [16] and GPBB [17] have been analyzed for the early diagnosis of myocardial ischemia. GPBB, which is bound to glycogen in sarcoplasmic reticulum, catalyzes the first step of glycogenolysis after activation, which involves the separation of glucose-1-phosphate from glycogen [18]. During myocardial ischemia, GPBB is activated and causes increase in glycogen degradation. GPBB isoenzyme is released into bloodstream via the T-tubules system with the peak value within the first 4 h after the onset of chest pain [10, 18]. The early release of GPBB into the blood is a common result of the combination of escalated glycogenolysis and increased permeability of cell membranes which is typical for myocardial ischemia and necrosis [19,20,21].
In our study, mean levels of cardiac markers GPBB, myoglobin and CKMB were higher in AMI cases when compared to that of healthy controls and were statistically significant at p < 0.001 (Figs. 1 and 2). In this study, we also found that GPBB was the most sensitive and specific biomarker to detect myocardial infarction when compared to myoglobin and CKMB at the first 4 h (Table 1). Rabitzsch et al. [12] and Cubranic et al. [22] also reported the highest sensitivity of GPBB in the early hours of chest pain. Myoglobin which appears in the blood early after AMI lacks specificity because it also increases in other muscular disorders and cannot be distinguished from that released from heart [4]. Moreover, the sensitivity and specificity of myoglobin in our study found to be less than GPBB (Table 1). CKMB though increased in AMI within 4 h of chest pain, had low sensitivity and specificity (Table 1) as compared to GPBB and myoglobin. Also, ROC curve analysis showed GPBB had the highest area under curve followed by myoglobin and CKMB. This study has been conducted for the first time in Madhya Pradesh of India. Hence, further studies with adequate sample size are needed to accept the concept.
Conclusion
Glycogen phosphorylase BB was the more sensitive and specific cardiac marker than other cardiac markers i.e. myoglobin and CKMB and shows better diagnostic efficiency for the early diagnosis of myocardial infarction within 4 h of chest pain. Glycogen phosphorylase BB can be used as an additional biomarker for the early diagnosis of acute myocardial infarction.
References
Sesani S, Vijayabhaskar M, Madhulatha MI, Lokary V. Assessment of C-reactive protein in cases of acute myocardial infarction and its correlation with risk factors. Int J Sci Study. 2016;4(7):140–3.
Rathish R, Gunalan G, Sumathi P. Current biomarkers for myocardial infarction. Int J Pharm Biol Sci. 2013;4(1):434–42.
Sathisha TG, Manjunatha GBK, Avinash SS, Shetty J, Devi OS, Devaki RN. Microalbunuria in non diabetic, non hypertensive myocardial infarction in south Indian patients with relation to lipid profile and cardiac markers. J clin Diagn Res. 2011;5(6):1158–60.
Bozkurt S, Kaya EB, Okutucu S, Aytemir K, Coskun F, Oto A. The diagnostic and prognostic value of first hour glycogen phosphorylase isoenzyme BB level in acute coronary syndrome. Cardiol J. 2011;18(5):496–502.
Pyati AK, Devaranavadagi BB, Sajjannar SL, Nikam SV, Shannawaz M, Sudharani. Heart-type fatty acid binding protein: a better cardiac biomarker than CK-MB and myoglobin in the early diagnosis of acute myocardial infarction. J Clin Diagn Res. 2015;9(10):8–11.
Alhashemi JA. Diagnostic accuracy of a bedside qualitative immunochromatographic test for acute myocardial infarction. Am J Emerg Med. 2006;24(2):149–55.
Adams J, Trent R, Rawles J. Earliest electrocardiographic evidence of myocardial infarction: implications for thrombolytic treatment. The GREAT Group. BMJ. 1993;307:409–13.
Nigam PK. Biochemical markers of myocardial injury. Indian J Clin Biochem. 2007;22(1):10–7.
Apple FS, Wu AH, Mair J, Ravkilde J, Panteghini M, Tate J, et al. Committee on standardization of markers of cardiac damage of the IFCC. Future biomarkers for detection of ischemia and risk stratification in acute coronary syndrome. Clin Chem. 2005;5(1):810–24.
Krause EG, Rabitzsch G, Noll F, Mair J, Puschendorf B. Glycogen phosphorylase isoenzyme BB in diagnosis of myocardial ischaemic injury and infarction. Mol Cell Biochem. 1996;60:289–95.
Lippi G, Mattiuzzi C, Comelli I, Cervellin G. Glycogen phosphorylase isoenzyme BB in the diagnosis of acute myocardial infarction: a meta-analysis. Biochem Med (Zagreb). 2013;23(1):78–82.
Rabitzsch G, Mair J, Leichleitner P, Noll F, Hofmann U, Krause EG. Isoenzyme BB of glycogen phosphorylase b and myocardial infarction. Lancet. 1993;34:1032–3.
Gravning J, Kjekshus J. The perfect biomarker in acute coronary syndrome: a challenge for diagnosis, prognosis, and treatment. Eur Heart J. 2008;29(23):2827–8.
Alam GK, Lieb DB. Biochemical markers of myocardial ischemia in renal failure. Hosp Physician. 2002;1:27–31.
Christenson RH, Duh SH, Sanhai WR, Wu AH, Holtman V, Painter P, et al. Characteristics of an albumin cobalt binding test for assessment of acute coronary syndrome patients: a multicenter study. Clin Chem. 2001;47(3):464–70.
Alhadi HA, Fox KA. Do we need additional markers of myocyte necrosis: the potential value of heart fatty-acid-binding protein. QJM. 2004;97(4):187–98.
Rabitzsch G, Mair J, Lechleitner P, Noll F, Hofmann U, Krause EG, et al. Immunoenzymometric assay of human glycogen phosphorylase isoenzyme BB in diagnosis of ischemic myocardial injury. Clin Chem. 1995;41:966–78.
Peetz D, Post F, Schinzel H, Schweigert R, Schollmayer C, Steinbach K, et al. Glycogen phosphorylase BB in acute coronary syndromes. Clin Chem Lab Med. 2005;43(12):1351–8.
Lacnák B, Stejskal D, Jedelský L, Karpísek M, Sprongl L. Utilization of glycogen phosphorylase BB measurement in the diagnosis of acute coronary syndromes in the event of chest pain. Vnitr Lek. 2007;53:1164–9.
Stejskal D, Lacnak B, Jedelsky L, Stepanova L, Proskova J, Solichova P, et al. Use of glycogen phosphorylase BB measurement with POCT in the diagnosis of acute coronary syndromes. A comparison with the ELISA method. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2007;151(2):247–9.
Hofmann U, Rabitzsch G, Löster K, Handschack W, Noll F, Krause EG. Immunenzymometric assay for the heart specific glycogen phosphorylase BB in human serum using monoclonal antibodies. Biomed Biochim Acta. 1989;48(2–3):S132–6.
Cubranic Z, Madzar Z, Matijevic S, Dvornik S, Fisic E, Tomulic V, et al. Diagnostic accuracy of heart fatty acid binding protein (H-FABP) and glycogen phosphorylase isoenzyme BB (GPBB) in diagnosis of acute myocardial infarction in patients with acute coronary syndrome. Biochem Med (Zagreb). 2012;22(2):225–36.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Singh, N., Rathore, V., Mahat, R.K. et al. Glycogen Phosphorylase BB: A more Sensitive and Specific Marker than Other Cardiac Markers for Early Diagnosis of Acute Myocardial Infarction. Ind J Clin Biochem 33, 356–360 (2018). https://doi.org/10.1007/s12291-017-0685-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12291-017-0685-y