
Abstract
Faecal carriage of Carbapenem-resistant Enterobacteriaceae (CRE) is being observed as an important risk factor for bacteremia among patients with hematological malignancies. A prospective surveillance study was conducted among these patients to determine the gut colonization of CRE. Rectal/perianal swabs were collected to isolate CRE. Carbapenem resistance was detected by disk diffusion, modified-Hodge, Carba-NP test, and PCR for blaNDM-1, blaKPC, blaOXA-48, blaVIM, blaIMP genes. A total of 209 CRE isolates were identified from 151 patients. E. coli was the most common (83.2%) CRE identified, followed by Klebsiella spp. (9.6%). The majority of CRE were observed resistant to ertapenem (86%). blaNDM-1 was the most common gene (57.3%), followed by blaOXA-48 (37.8%). 26.8% isolates found to carry both blaNDM-1 and blaOXA-48 genes. CRE is increasingly observed to cause bacteremia among hematological malignancy patients due to increased colonization. Screening for gut CRE colonization is necessary to guide empirical therapy and apply infection control measures among these patients.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Emergences of the Carbapenem-resistant Enterobacteriaceae (CRE) group of microorganisms in the last few decades are becoming a serious problem worldwide. It complicates the disease pathogenesis, adversely affects the outcome and economy of the patient. According to the 2013 Centre for Diseases Control and Prevention (CDC) report, CRE is considered an urgent threat in the United States and included in the list of priority-resistant organisms by World Health Organisation (WHO) [1]. Early detection and treatment of CRE infection is a big challenge in the health sector. Gut colonization with CRE is an important risk factor for bloodstream infection, especially in malignanat conditions. Patients diagnosed with hematologic malignancies develop severe mucositis during chemotherapy and are at higher risk of developing bacteremia due to the translocation of enteric colonized bacteria into the bloodstream. Although there are limited data, mortality due to CRE infection has been reported as 60–100% among these patients [2, 3]. As per the CDC report, there is increased CRE infections in different parts of the world [2, 4]. Developing countries, including India, are observed to be affected the worst due to this emergence of multidrug-resistant bacteria [5]. Since most gut flora belongs to Enterobacteriaceae, screening for CRE fecal carriage is highly crucial, particularly in patients with immunocompromised conditions, admitted in ICU set up or having hematological malignancies [6, 7]. The mechanism of resistance in CRE is predominantly due to the presence of carbapenemase enzyme encoded on chromosome or plasmid. The other less common mechanisms are mutation in the porin channels, alteration in the efflux pumps, etc. [8]. These carbapenem hydrolyzing genes are transferred horizontally from one bacteria to another or may cause point mutation of efflux pumps resulted in its overexpression and finally resulted in carbapenem resistance. Important carbapenemase genes carried by CRE are New Delhi Metallo-β-lactamase (blaNDM 1–12), Klebsiella pneumoniae Carbapenemase (blaKPC), Oxacillinase-48 type (blaOXA-48), (blaOXA-56), Verona Integron-encoded Metallo-β-lactamase (blaVIM), Imipenemase Metallo-β-lactamase(blaIMP) etc. Patients with hematological malignancies and the recipients of hematopoietic stem cell transplantation (HSCT) are highly vulnerable to infections with CRE due to prolonged neutropenic conditions and gastrointestinal mucositis [9]. Treatment of bacteremia caused due to CRE is complicated. Although drugs such as colistin, tigecycline, and the newer beta-lactam/beta-lactamase inhibitor such as Ceftazidime–avibactam, Meropenem–vaborbactam, Ceftalozane–tazobactam, etc. are available for the treatment of CRE, growing resistance of colistin and tigecycline is also a reason for concern. Early detection of these patients with intestinal colonization of CRE may help take antibiotic stewardship measures and infection control preventive actions. This will reduce the incidence of endogenous infection and prevent CRE transmission in health care settings.
Materials and Methods
This was a cross-sectional study conducted in the Department of Microbiology with the collaboration of the Department of Medical Oncology and Department of Haematology of a tertiary health care center in North India. It was carried out over 2 years (2016–2017). The ethical clearance was obtained from the Institute Ethics Committee. The study aimed to determine the prevalence of intestinal colonization due to CRE in patients with hematological malignancy. The study's objectives were to characterize the CRE isolates by phenotypic tests, Modified Hodge's test, and Carba-NP test and detection of carbapenemase gene blaNDM blaKPC, blaOXA-48, blaIMP, and blaVIM by PCR.
Consecutive patients with a clinical diagnosis of hematological malignancy (including both newly diagnosed and relapse cases) admitted for chemotherapy to either of the department were included in the study. Both adult and pediatric age groups of the patient were recruited in the study. During cytotoxic therapy, patients who developed neutropenia (< 500 neutrophils/µl of blood) were noted for further analysis to compare the prevalence of CRE in different groups. Patients with fever and neutropenia due to underlying conditions other than hematological malignancy were excluded from the study. Patient demographic data and the risk factors associated with malignancy conditions such as neutropenia, previous hospital stay, previous antibiotic therapy, steroid therapy, and comorbid conditions were collected.
Phenotypic Tests
Rectal/perianal swabs were collected from these patients and processed further to isolate CRE following the Centre for Disease Control and Prevention (CDC) protocol [10].
The rectal swabs were processed as follows.
Two Rectal/perianal swabs were collected from every patient and inoculated in 5 ml of Trypticase Soy Broth (TSB) transport media. 10 µg strength of ertapenem or meropenem disk was added in each tube along with two rectal swabs and were incubated at 35 ± 2 °C for overnight. A loopful of incubated broth was subcultured on MacConkey agar with intermittent heating of the loop and incubated in ambient air at 35 ± 2 °C for overnight. Isolated colonies on MacConkey agar were further processed for the final identification of organisms.
Identification of Organisms
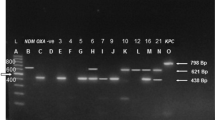
The lactose fermenting isolated colony from MacConkey agar were tested for the biochemical tests such as catalase, oxidase, triple sugar iron, indole, mannitol motility agar, Christensen urea agar medium, and Simon's citrate media as per the standard operative protocol. All the identified isolates were tested for carbapenem resistance by disk diffusion by Kirby–Bauer method on Muller–Hinton agar (MHA) using four carbapenem disks (imipenem, meropenem, ertapenem, and doripenem, HiMedia, Mumbai). Interpretation of the result was made as per the Clinical and Laboratory Standards of Institute (CLSI) 2016 guideline [11]. CRE was defined as an isolate resistant to either of the carbapenem disks. All the isolates were further tested for carbapenemase-producing CRE (CPCRE) using the modified Hodge test (MHT) and RAPIDEC ® Carba NP test (BioMeriux, France). The MHT test was performed as per the standard protocol of CLSI 2014 [10]. The indicator strain Escherichia coli ATCC 25922 strain was used for lawn culture. Klebsiella pneumoniae ATCC BAA 1705 and ATCC BAA 1706 were used as the positive and negative control, respectively. Enhanced growth of the indicator strain towards the antibiotic disk was considered as positive for carbapenemase production. Carba-NP test (RAPIDECw CARBA NP) was performed and interpreted as per the manufacturer's instruction. All the CRE strains were subjected to PCR analysis. PCR for blaNDM, blaKPC, blaOXA-48, blaIMP, and blaVIM gene had been carried out using primers from the published literature [11].
Data were analyzed using SPSS software v.20.0 (SPSS Inc., Chicago, IL) by Chi-square test, except where the data was less than 5, Fisher's exact test was used. Significance was set at P < 0.05 using two-sided comparisons. Cohen's Kappa coefficient was calculated to check the inter-rater agreement between all the assays.
Results
Rectal/perianal swabs were collected from 200 patients diagnosed with hematological malignancy and processed following the CDC protocol. One hundred fifty-one patients out of 200 (75.5%) were confirmed to carry CRE in their gut as colonizers. A total of 209 CRE isolates were identified from 151 patients (93 patients had a single CRE isolate, and fifty-eight patients had two different types of CRE isolates). Among the rest 49 patients, Gram-positive cocci were isolated in six patients. Acinetobacter spp. was from three patients, and Pseudomonas spp. and Citrobacter spp. were found in one patient without any CRE in their gut. No growth was observed among the rest of the thirty-nine patients.
Demographic Results
On comparing the demographic data, the male was the predominant group (75%, [150/200]) followed by females (25%, [50/200]). The ratio of adult vs. pediatrics patients was found as 2.6:1. Mean age distribution among adult and pediatrics patients were 36.5 years (18–62 years) and 5 years (10 months–17 years), respectively (Table 1) Among the total patients recruited in the study, 77% from the pediatric group, and 74.6% from the adult group were found to carry CRE in their gut. The current study was done only on the admitted patients, among which Acute myeloid leukemia was observed as the commonest underlying condition (78%, [156/200]). One hundred sixty-three patients had a history of antibiotic intake (includes cefoperazone–sulbactam and amikacin) within the past 30 days of admission. Fever was observed among 14.5% (29/200) of the total patients during the hospital stay when rectal swab was taken. Approximately 79% of febrile patients were observed to have absolute neutropenia. However, absolute neutropenia in patients with a history of antibiotic intake and steroid intake within the last 30 days were observed less, i.e., 28% and 33%, respectively. Patients with acute leukemias (especially myeloid leukemias; AML) had functional neutropenia in addition to occasionally observed low absolute neutrophil count (ANC) numbers at the time of presentation/diagnosis. Hence, the relation of ANC with CRE colonization among these patients was questionable.
Fifty-two (33%, 52/200) patients were neutropenic, of which 42 carried CRE. Comorbidity was observed in only one patient in the non-CRE category.
Microbiology Results
Escherichia coli was the most common CRE isolate (83.2%, [174/209]), followed by Klebsiella spp. (9.6%, [20/209]) and Enterobacter spp. (2.87%, [6/209]). Six isolates of Enterococcus spp. were isolated from various patients during the study period. When we compare the four different carbapenem disk susceptibility testing results, the majority of CRE isolates (86%) were found resistant to ertapenem disk, followed by meropenem (75%), doripenem (65%), and imipenem (41%) disk. Comparing the carbapenemase production by the CRE isolates, the Carba-NP test was more sensitive than MHT (Table 2). Carba-NP was tested for 164 CRE isolates, whereas MHT was carried out on 71 CRE isolates. Tests detected indeterminate by either Carba-NP or MHT were considered as negative to avoid subjective variation. Out of 164 CRE isolates, 82.9% (136/164) of isolates were positive for carbapenemase production using the Carba-NP test. MHT was done on 71 isolates of CRE, of which only 56.3% (40/71) were found positive for carbapenemase production. Among the different carbapenemase genes, most isolates were observed positive for the blaNDM-1 gene alone (94/164, 57.3%), followed by the blaOXA-48 gene (62/164, 37.8%). Forty-four out of 164 (26.8%) CRE isolates were found to carry both blaNDM and blaOXA-48 genes. Only 3 out of 164 (1.8%) Enterobacteriaceae isolates were positive for blaIMP gene conferring them Carbapenem resistance. No isolates were found to contain the blaKPC or blaVIM gene.
Statistical Analysis
Proportions between the CRE and non-CRE groups were compared using the Chi-square test and Fisher's exact test. No significant difference was found between CRE and non-CRE groups comparing the risk factors, e.g., age, sex, diagnosis, fever, absolute neutropenia, history of intake of antibiotic or steroid (P < 0.05) (Table 1) Carba-NP was observed more sensitive for the detection of CP-CRE in comparison to MHT. The Cohen's Kappa coefficient between Carba-NP and MHT tests was observed to be 9% only. This indicates a poor agreement of the result between Carba-NP and MHT. The level of agreement of meropenem with the Carba-NP test was observed to be highest (75%), followed by others. Nine CRE isolates negative by Carba-NP and MHT were observed resistant by ertapenem.
Discussion
Febrile neutropenia is a common complication among patients with hematological malignancies following chemotherapy causing significant morbidity and mortality [12,13,14]. Bloodstream infection (BSI) is the most common cause of morbidity and mortality among febrile neutropenic patients [14]. The infection is mostly caused due to translocation of colonized bacteria in the gut [13, 15]. Colonization of multidrug-resistant bacteria in the gut increases the rate of BSI, thereby increasing the mortality rate [15,16,17]. In a retrospective study on stem cell transplant by The Gruppo Italiano Trapianto Midollo Osseo (GITMO) group observed carbapenem resistant K. pneumoniae colonization followed by infection in 30% of the total cases [18]. Incidence of BSI among these patients ranges from 11 to 38% with a mortality rate of 40%, particularly infected with CRE [19]. The emergence of CRE as a pathogen and gut colonizer is of great concern among these patients. The increased gut colonization with the resistant bacteria resulted from increased carbapenem utilization such as Meropenem and Imipenem in clinical treatments [20]. In the current study, most of our patients had a history of intake of aminoglycoside and beta-lactam/beta-lactamase inhibitor combination of antibiotics within the last 30 days before the sampling. The high incidence of CRE carriage in our study probably occurred due to increased antibiotic use among these patients during the neutropenic period to prevent infection acquisition. Gaind et al. had shown a significant increase in the CRE colonization with an increase in the length of stay in the hospital [6]. Early identification and prompt treatment were observed as helpful to tackle this condition and showed a reduction of mortality by 2–10% [21].
In our study, a total of 209 isolates were identified out of 200 samples. The prevalence of CRE was 78.46% (164/209) among isolates collected. A total of 75.5% (151/200) patients had been found with CRE as fecal colonizers in their gut, which is unfortunately very high and alarming in this study population. Salomao et al. observed that 18% of the total patients exposed to healthcare settings within the last 1 year and use antibiotics in the previous 1 month carry CRE in their gut [22]. There were also reports of a high rate of fecal carriage of ESBL producing Enterobacteriaceae among people from both hospital and community settings [23]. The earlier studies from various hospitals in India showed a varied incidence of CRE ranges from 1.8 to 51% in different patient populations [14]. The first Indian study among pediatric cancer patients had reported the prevalence of CRE colonization as 20.2% [14]. Such a high percentage of CRE prevalence in our study is alarming and needs immediate action to control its spread. This study highlights the high incidence of fecal carriage of CRE in hospitalized patients with hematological malignancy. In the current study, patients with AML were found the predominant group, followed by others. This study was carried out only on admitted patients. As per the hospital protocol, the majority of patients with a diagnosis of AML were referred for in-patient treatment, and patients with a diagnosis of ALL were referred for outpatient treatment. This might be the reason for a high number of AML cases in our study. Although patients diagnosed with ALL do receive steroids compared to AML patients, neutropenia in AML is more protracted than ALL; hence, infection related death due to induction in AML are higher than ALL. A further study from the different geographical locations can be done to look for the association of gut colonization with CRE along with the underlying conditions.
The chance of infection by CRE is increased due to increased colonization of resistant bacteria in the GIT [16]. The common risk factors associated with CRE acquisition among the patients in healthcare settings include exposure to antimicrobials, recent stay in a long term acute care facility (LTCF), recent invasive procedures, immunosuppression due to long term steroid intake, cancer chemotherapy, HIV, autoimmune diseases, etc. [2, 24, 25]. CRE infections can spread in the healthcare settings by health care providers during patient care, sharing the beds, toilets, and surroundings of the patient as in other infections [26, 27]. In this way, the risk of infection of hospitalized patients is increased many folds with the increase in the prevalence of gut colonization by CRE microorganisms, and therefore, there is an increase in the risk of endogenous infection [14, 16, 17].
There was no significant difference in the prevalence of CRE in the current study with respect to age or sex. However, its prevalence was observed highest among AML patients. Most of the CRE isolates (141/164, 86%) were resistant to ertapenem, followed by meropenem (75%) and doripenem (65%). The least number of CRE isolates were found resistant imipenem. In earlier studies, Ertapenem was the most sensitive disk for detecting CRE compared to others [28].
In the current study, Carba-NP and MHT were used to detect CP-CRE isolates. Carba-NP was found more sensitive for detection of CP-CRE in comparison to MHT. All the isolates found positive by the Carba-NP test were also observed resistant to ertapenem disk. However, few isolates were observed resistant by ertapenem disk but negative or indeterminate by the Carba-NP test. It may be due to the presence of different carbapenemase genes or due to the presence of noncarbapenemase mechanisms such as loss of porin channels, mutation of the efflux pumps or AmpC over expression, etc. As per the CLSI 2016, the sensitivity and specificity of the Carba-NP test vary with the presence of different carbapenemase genes. The sensitivity was observed to be more than 90% in KPC, NDM, IMP, VIM, and SME carbapenemase. However, it may be as low as 11% in OXA-48 carbapenemases [11]. Similarly, the sensitivity and specificity of MHT were derived primarily based on the USA isolates, which suggest it has a very high level of sensitivity (> 90%) and specificity (> 90%) in detecting KPC type of carbapenemase. In contrast, its sensitivity and specificity may be as low as 11% in detecting the NDM type of carbapenemase [29].
In developing countries, blaNDM and blaOXA types are most commonly reported, followed by blaVIM, blaIMP, whereas blaKPC is frequently reported from developed countries [30]. Among the 164 isolates in the current study, blaNDM was the predominant carbapenemase gene (57.3%), followed by blaOXA-48 (37.8%). A total of 26.8% isolates were observed to contain both NDM-1 and OXA-48 genes. Gaind et al. also observed similar results [6]. A total of 86 out of 136 isolates positive for Carba-NP were found to carry blaNDM-1gene. The blaNDM-1 gene was first recognized in an isolate of K. pneumoniae of a Swedish citizen treated in India [31]. Subsequently, it was increasingly reported from the majority of the Indian CRE isolates. A study done by Kumarasamy et al. showed that the prevalence of the blaNDM-1 gene was variable between 31 and 55% [32]. The CRE isolates with the NDM-1 gene are potentially hazardous as plasmids mostly mediate the resistance. It is easily transferable among various bacterial populations resulting in the conversion of sensitive strains into resistant ones. In our study, a very high number of patients carry both blaNDM and blaOXA-48, which increases the risk of morbidity and mortality among these patients.
Gut colonization by resistant bacteria has been described by many researchers and varies in different geographical regions. In the current study, there was a very high prevalence of CRE colonization, which might be because of antibiotics' frequent usage among these patients. Apart from antibiotic usage, environmental factors like the presence of resistant bacteria in the water bodies, open defaecation, irrational use of antibiotics in livestock animals, poultry, and agriculture are also contributing to this rise of antimicrobial resistance [33]. So, a multidisciplinary approach targeting different levels is required to combat this problem.
In summary, CREs are increasingly becoming common pathogens among hematological malignancy patients, causing bloodstream infections. Outcomes of these infected patients are poor due to high morbidity and mortality. Developing research data to guide the use of new antimicrobial agents to treat these CRE pathogens in this population is paramount. The formulation of optimal infection prevention strategies and strict adherence to these protocols is also an urgent need. A very high incidence of CRE colonization was observed in the hematological malignancy patients in the current study. Screening for gut colonization is necessary to guide empirical therapy and apply infection control measures to prevent transmission in healthcare settings.
References
World Health Organization (2014) Antimicrobial resistance global report on surveillance. World Health Organization, Geneva. http://apps.who.int/iris/bitstream/10665/112642/1/9789241564748_eng.pdf?ua1. (Accepted 12 Oct 2019)
Satlin MJ, Jenkins SG, Walsh TJ (2014) The global challenge of carbapenem-resistant Enterobacteriaceae in transplant recipients and patients with hematologic malignancies. Clin Infect Dis 58:1274–1283
Trecarichi EM, Pagano L, Martino B, Candoni A, Di Blasi R, Nadali G et al (2016) Bloodstream infections caused by Klebsiella pneumoniae in onco-hematological patients: clinical impact of carbapenem resistance in a multicentre prospective survey. Am J Hematol 91:1076–1081
Montagnani C, Prato M, Scolfaro C, Colombo S, Esposito S, Tagliabue C et al (2016) Carbapenem-resistant Enterobacteriaceae infections in children: an Italian retrospective multicenter study. Pediatr Infect Dis J 35:862–868
Zhang R, Liu L, Zhou H, Chan EW, Li J, Fang Y et al (2017) Nationwide surveillance of Clinical Carbapenem-resistant Enterobacteriaceae (CRE) Strains in China. EbioMedicine 19:98–106
Mittal G, Gaind R, Kumar D, Kaushik G, Gupta KB, Verma PK et al (2016) Risk factors for fecal carriage of carbapenemase producing Enterobacteriaceae among intensive care unit patients from a tertiary care center in India. BMC Microbiol 16:138
Das P, Singh AK, Pal T, Dasgupta S, Ramamurthy T, Basu S (2011) Colonization of the gut with Gram-negative bacilli, its association with neonatal sepsis and its clinical relevance in a developing country. J Med Microbiol 60:1651–1660
Queenan AM, Bush K (2007) Carbapenemases: the versatile beta-lactamases. Clin Microbiol Rev 20:440–458
Satlin MJ, Walsh TJ (2017) Multidrug-resistant Enterobacteriaceae, Pseudomonas aeruginosa, and vancomycin-resistant Enterococcus: three major threats to hematopoietic stem cell transplant recipients. Transplant Infect Dis. https://doi.org/10.1111/tid.12762
CDC 2012 CRE Toolkit: Guidance for Control of Carbapenem‐Resistant Enterobacteriaceae (CRE). http://www.cdc.gov/hai/organisms/cre/cre‐toolkit/index.html. (Accepted 25 Oct 2019)
Clinical and Laboratory Standards Institute, 26 ed. Wayne: CLSI supplement M100S.2016
Asthana S, Mathur P, Tak V (2014) Detection of Carbapenemase production in gram-negative bacteria. J Lab Phys 6:69–75
Lustberg MB (2012) Management of neutropenia in cancer patients. Clin Adv Hematol Oncol 10(12):825–826
Kokkayil P, Agarwal R, Mohapatra S, Bakshi S, Das B, Sood S et al (2018) Bacterial profile and antibiogram of blood stream infections in febrile neutropenic patients with hematological malignancies. J Infect Dev Ctries 12:442–447
Gopalakrishnan V, Jenq RR (2018) Implicating or exonerating the gut microbiome in blood–borne infection. Nat Med 24(12):1788–1789
Aklilu A, Manilal A, Ameya G, Woldemariam M, Siraj M (2020) Gastrointestinal tract colonization rate of extended-spectrum beta-Lactamase- and Carbapenemase-producing Enterobacteriaceae and associated factors among hospitalized patients in Arba Minch General Hospital, Arba Minch, Ethiopia. Infect Drug Resist 13:1517–1526
Montassier E, Al-Ghalith GA, Ward T, Corvec S, Gastinne T, Potel G, Moreau P, de la Cochetiere MF, Batard E, Knights D (2016) Pretreatment gut microbiome predicts chemotherapy-related bloodstream infection. Genome Med 8(1):49
Girmenia C, Viscoli C, Pichiocchi A, Cudillo L, Botti S, Errico A et al (2015) Management of carbapenem resistant Klebsiella pneumoniae infections in stem cell transplant recipients: an Italian multidiciplinary consensus statement. Hematologia 100:e373
Satlin MJ, Chen L, Patel G, Gomez-Simmonds A, Weston G, Kim AC et al (2017) Multicenter clinical and molecular epidemiological analysis of Bacteremia due to Carbapenem-Resistant Enterobacteriaceae (CRE) in the CRE epicenter of the United States. Antimicrob Agents Chemother 61:e02349-e2416
Zilberberg MD, Shorr AF (2013) Prevalence of multidrug-resistant Pseudomonas aeruginosa and carbapenem-resistant Enterobacteriaceae among specimens from hospitalized patients with pneumonia and bloodstream infections in the United States from 2000 to 2009. J Hosp Med 8:559–563
Baljin B, Baldan G, Chimeddorj B, Tulgaa K, Gunchin B, Sandag T et al (2016) Faecal carriage of gram-negative multidrug-resistant bacteria among patients hospitalized in two centres in Ulaanbaatar, Mongolia. PLoS ONE 11:e0168146
Salomão MC, Guimarães T, Duailibi DF, Perondi M, Letaif L, Montal AC et al (2017) Carbapenem-resistant Enterobacteriaceae in patients admitted to the emergency department: prevalence, risk factors, and acquisition rate. J Hosp Infect 97:241–246
Ouchar Mahamat O, Tidjani A, Lounnas M, Hide M, Benavides J, Somasse C et al (2019) Fecal carriage of extended-spectrum β-lactamase-producing Enterobacteriaceae in hospital and community settings in Chad. Antimicrob Resist Infect Control 8:169
Nicolas-Chanoine MH, Vigan M, Laouénan C, Robert J, E-carb Study Group (2019) Risk factors for carbapenem-resistant Enterobacteriaceae infections: a French case–control–control study. Eur J Clin Microbiol Infect Dis. 38(2):383–393
Torio RO, Paras DNT, Abad CLR (2019) 495 Risk factors of Carbapenem-resistant Enterobacteriaceae (CRE) infections among intensive care unit (ICU) patients in a Tertiary Hospital in the Philippines. Open Forum Infect Dis 6(2):S241–S242
Chemaly RF, Simmons S, Dale C Jr et al (2014) The role of the healthcare environment in the spread of multidrug-resistant organisms: update on current best practices for containment. Ther Adv Infect Dis 2(3–4):79–90
Magiorakos AP, Burns K, Rodríguez Baño J et al (2017) Infection prevention and control measures and tools for the prevention of entry of Carbapenem-resistant Enterobacteriaceae into healthcare settings: guidance from the European Centre for Disease Prevention and Control. Antimicrob Resist Infect Control 6:113
Chung HS, Yong D, Lee M (2016) Mechanisms of Ertapenem resistance in Enterobacteriaceae isolates in a tertiary university hospital. J Investig Med 64:1042–1049
Bir R, Mohapatra S, Kumar A, Tyagi S, Sood S, Das BK et al (2019) Comparative evaluation of in-house Carba NP test with other phenotypic tests for rapid detection of Carbapenem-resistant Enterobacteriaceae. J Clin Lab Anal 33:e22652
Nordmann P, Naas T, Poirel L (2011) Global spread of Carbapenemase-producing Enterobacteriaceae. Emerg Infect Dis 17:1791–1798
Yong D, Toleman MA, Giske CG, Cho HS, Sundman K, Lee K et al (2009) Characterization of a new metallo-beta-lactamase gene, bla(NDM-1), and a novel erythromycin esterase gene carried on a unique genetic structure in Klebsiella pneumoniae sequence type 14 from India. Antimicrob Agents Chemother 53:5046–5054
Kumarasamy KK, Toleman MA, Walsh TR, Bagaria J, Butt F, Balakrishnan R, Chaudhary U et al (2010) the emergence of a new antibiotic resistance mechanism in India, Pakistan, and the U.K.: a molecular, biological, and epidemiological study. Lancet Infect Dis 10:597–602
Taneja N, Sharma M (2019) Antimicrobial resistance in the environment: Indian scenario. Ind J Med Res 149:119–128
Author information
Authors and Affiliations
Contributions
Dr. A.K. had done the laboratory work and drafting of the manuscript. Dr. S.M. was the chief investigator, gave the concept, design of the study, and drafting of the manuscript. Dr. R.B. helped in the analysis of data. Mr. S.T. had helped in the molecular work. Dr. S.B. and Dr. M.M. had revised the manuscript critically for intellectual content. H.G. had contributed to writing the manuscript. Dr. S.S. had helped in the analysis of data. Dr. B.K.D. had revised it critically for intellectual content. Dr. A.K. had given the final approval of the version.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethics Approval
Ethics approval had been taken for this study by the institutional ethical committee, and all the protocols were followed as per the ethical standards.
Consent to Participate
Informed consent had been taken from the participants.
Consent of Publication
Consent had been taken from all the contributing authors for publication.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Kumar, A., Mohapatra, S., Bir, R. et al. Intestinal Colonization Due to Carbapenem-Resistant Enterobacteriaceae Among Hematological Malignancy Patients in India: Prevalence and Molecular Charecterisation. Indian J Hematol Blood Transfus 38, 1–7 (2022). https://doi.org/10.1007/s12288-021-01415-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12288-021-01415-y