
Abstract
Background
Physical limitations prior to cancer diagnosis may lead to suboptimal health outcomes. Our objective was to evaluate the impacts of poor physical health-related quality of life (HRQOL) and physical functioning (PF) on the risk of contralateral breast cancer (CBC).
Methods
We performed a nested case–control study of women with invasive unilateral breast cancer (UBC) who did not receive prophylactic contralateral mastectomy using the Surveillance, Epidemiology and End Results Medicare Health Outcomes Survey data resource. Among 2938 women aged ≥ 65 years diagnosed with first stage I–III UBC between 1997 and 2011, we identified 100 subsequent CBC cases and 915 matched controls without CBC using incidence density sampling without replacement. Pre-diagnosis physical HRQOL and PF were determined using Medical Outcomes Trust Short Form-36 (SF-36)/Veterans Rand 12-Item Health Survey (VR-12) responses within 2 years prior to first UBC diagnosis. We estimated adjusted odds ratios (OR) and 95% confidence intervals (CI) using conditional logistic regression models.
Results
Cases and controls were similar with respect to comorbidities, stage, surgery, and radiation treatments, but differed by hormone receptor status (ER/PR-negative, 23% and 11%, respectively) of first UBC. Cases had modestly lower mean pre-diagnosis physical HRQOL (− 1.8) and PF (− 2.2) scores. In multivariable models, we observed an increased CBC risk associated with low physical HRQOL (lowest vs. highest quartile, OR = 1.8; 95% CI 0.8–4.3), but CIs included 1.0. Low PF was associated with a 2.7-fold (95% CI 1.1–6.7) increased CBC risk.
Conclusions
Findings indicate that low physical HRQOL, specifically poor PF, is associated with CBC risk. Efforts to understand and minimize declines in PF post-breast cancer are well motivated.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
There are more than 3.8 million women in the United States with a history of breast cancer [1], and contralateral breast cancer (CBC)—cancer in the breast opposite to a previous or synchronous breast cancer—is the most common second cancer among breast cancer survivors [2]. Asynchronous CBC, which is diagnosed more than a year after the first primary breast cancer, accounts for more than 60% of CBC cases in the US [3]. CBC is a serious adverse outcome; 36% of deaths are cancer-related in women with CBC, compared to 28% in women with unilateral breast cancer over a 24-year study period [4]. Among women diagnosed with CBC between 1992 and 2010, almost half were ages 65–80 [5]. The high proportion of cases among older women underscores the need to elucidate risk factors, especially modifiable ones, in the growing population of aging breast cancer survivors.
Multiple risk factors for developing a second primary CBC have been identified. CBC is associated with both moderate and high penetrance breast cancer susceptibility genes; a first-degree relative with a history of breast cancer; a first primary estrogen receptor negative breast cancer [6]; age less than 40 years at diagnosis of a first primary [4]; and being Black, Hispanic, or Asian or Pacific Islander—regardless of hormone receptor status [7, 8]. Modifiable risk factors have also been implicated; women with a BMI greater than 30 kg/m2 [6], type II diabetes [9], any drinking history [6, 10], and a combination of smoking and drinking [11] are also at elevated risk for CBC. Comparatively little is known about the effects physical health-related quality of life (HRQOL) and physical functioning (PF), on the risk of CBC [12].
The impact of post-breast cancer diagnosis physical functioning and activity on survival and recurrence is well understood [13,14,15,16,17,18,19]. The role of pre-diagnosis physical functioning in shaping the risk of CBC is less so. This relationship warrants further study to support a life course-oriented approach to preventing CBC. Our objective was to evaluate the risk of CBC greater than 12 months after initial unilateral breast cancer (UBC) diagnosis among older women based on their pre-diagnosis self-reported physical HRQOL.
Methods
We conducted our study using the linked Surveillance, Epidemiology and End Results-Medicare Health Outcomes Survey (SEER-MHOS) data resource. The SEER Program aggregates cancer incidence data from 18 population-based registries, and includes patient demographics, tumor site, morphology, stage, first treatment course, and vital status [20]. MHOS is a self-administered survey sent to randomly selected Medicare managed-care beneficiaries to assess functional health and health-related quality of life [21]. Registries included in the SEER-MHOS data resource include: Connecticut, Detroit, Greater California, Greater and Rural Georgia, Hawaii, Iowa, Kentucky, Louisiana, New Jersey, New Mexico, and Seattle-Puget Sound [22]. Between 1998 and 2017, approximately 6% of MHOS participants have been linked to SEER [23]. Response rates to MHOS Surveys ranged between 50 and 73% between 1998 and 2011 and were similar between those who were and were not linked to SEER [24]. This study was reviewed and approved by the institutional review board of the University of Illinois at Chicago.
In this study, we included women ages 65 years and older diagnosed with a first primary invasive unilateral breast cancer between 1997 and 2011 who received cancer-directed surgery. Women who received prophylactic contralateral mastectomy were excluded. Women must have completed the MHOS within 2 years before primary breast cancer diagnosis. CBC was defined as a second breast cancer on the contralateral side, diagnosed more than 2 months after the initial unilateral breast cancer. We further described these CBC outcomes as having occurred within 2–12 months post-diagnosis (synchronous) and > 12 months post-diagnosis (asynchronous). Women were excluded in cases of unknown laterality, paired sites, bilateral breast cancer, or survival times that were unknown. Women were excluded from the analysis if the CBC was diagnosed within 2 months of the UBC, the survival time after CBC diagnosis was unknown and in cases of missing health-related quality of life component and subscale scores. If patients completed multiple surveys within the study period, only the most recent survey prior to diagnosis was used for analysis.
Among 2938 women with stages I–III UBC between 1997 and 2011, we identified 100 subsequent CBC cases and 915 controls using incidence density sampling without replacement [25] (Fig. 1); CBC cases were matched to up to ten female Medicare beneficiaries on age (65–69, 70–74, 75–79, 80–84, 85+ years), race (White, non-White), SEER reporting region of residence, and quarter year of primary breast cancer diagnosis. Information on demographics, clinical characteristics, and physical health-related quality of life was collected from SEER records and MHOS survey responses. Hormone receptor status was categorized as either estrogen and/or progesterone receptor positive or estrogen and progesterone receptor negative. We collected information on presence and number of comorbidities including arthritis, coronary artery disease, chronic obstructive pulmonary disease, depression, diabetes, heart failure, hypertension, inflammatory bowel disease, myocardial infarction, and stroke.

Flowchart for inclusion of breast cancer patients from the SEER-MHOS Data Resource
Physical HRQOL was determined from survey responses to the Medical Outcomes Trust Short Form-36 (SF-36)/Veterans Rand 12-Item Health Survey (VR-12). Higher scores on these measures indicate better physical HRQOL. Details of the SF-36 and VR-12 have been described elsewhere [26, 27]. From 1998 to 2005, MHOS ascertained physical and emotional functioning using the SF-36 [28]. In 2006, VR-12 replaced the SF-36. Algorithms developed by Boston University School of Public Health for the conversion of SF-36 to VR-12 scores were used in the SEER-MHOS data resource to account for changes in the survey instrument over time [29]. The VR-12 is a brief, generic health survey comprised of 12 items that correspond to eight principal physical and mental health domains including physical functioning (PF), role limitations due to physical problems (RP), bodily pain (BP), general health perceptions (GH), general mental health (MH), role limitations due to emotional problems (RE), social functioning [30], and vitality (VT) [32]. The items can be summarized into two scores, a mental component summary (MCS) score and physical component summary (PCS) score. In this study, physical HRQOL refers to the PCS, which includes PF. The PCS and MCS scores utilize all eight scales in their calculation and are computed from weights derived from the 1999 Veterans Health Study [31]. In this study, we used T-scores, a linear transformation of the scoring range for the SF-36/VR-12 that yields a population mean of 50 and standard deviation of 10, based on 1990 population norms [29].
Statistical analysis
We estimated relative risks of CBC using conditional logistic regression models with adjusted odds ratios (OR) and 95% confidence intervals (CI) in analyses of (i) all CBC cases and their matched non-CBC controls and (ii) of asynchronous CBC cases occurring > 12 months after the index primary breast cancer diagnosis. Under these risk set-based sampling conditions, these models provide an unbiased approximation of the hazard ratio [32]. Patients were matched on age, race, SEER region, and quarter year of diagnosis. In a multivariable-adjusted model, we additionally controlled for AJCC stage (I, II, III), surgery type (breast-conserving, mastectomy), receipt of any radiation (yes/no), hormone receptor status (ER- and/or PR-positive, ER- and PR-negative), and number of comorbid conditions (0–2, 3–4, 5+). We used Wilcoxon rank-sum tests to compare medians, Chi-square tests for categorical variables, and independent samples t test for continuous scores on a linear transformed scale. All tests were two-sided, with a significance level of P < 0.5. Statistical analyses were conducted using Stata Statistical Software: Release 16 (College Station, TX: StataCorp LLC).
Results
Descriptive characteristics of the 100 identified CBC cases and 915 incidence density sampled controls are reported in Table 1. The median (interquartile range) age at primary breast cancer diagnosis was 73 (70–79) years among cases and 74 (70–78) years among controls. The majority of patients were White (cases: 84.5%; controls: 82%). Compared with controls, CBC cases had a higher proportion of women that were diagnosed with stage I breast cancer (69 vs. 63%, P = 0.47) and received breast-conserving surgery (65 vs. 59%, P = 0.19), and a lower proportion that were treated with radiotherapy (47 vs. 54%, P = 0.18), but these differences were not statistically significant. A significantly higher proportion of cases were ER-/PR-negative (23 vs. 11%, P < 0.01) compared with controls. Cases and controls were similar with respect to prevalence of common comorbidities, including hypertension, arthritis, depression, diabetes, and chronic obstructive pulmonary disease.
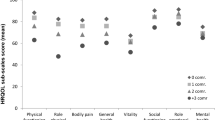
In Table 2, mean physical HRQOL component and subscale scores are reported. Overall, cases had lower mean physical HRQOL (− 1.8; 95% CI − 4.3, 0.7; P = 0.16) and PF (− 2.2; 95% CI − 4.9, 0.5; P = 0.11) component scores, but these differences were not statistically significant. Additionally, cases had lower role limitation-physical, pain, general health, and energy/fatigue scores, but these differences were not statistically significant.
Results from multivariable conditional logistic regression models for all cases are reported in Table 3. Multivariable models with adjustment for AJCC stage, surgery type, radiation, hormone receptor status, and comorbidities suggested increased CBC risk with lower physical HRQOL and PF scores. Compared with women in the upper quartile of physical HRQOL, women in the first quartile had a 1.70-fold (95% CI 0.78, 3.69; P = 0.18) increased risk of CBC. Compared with women in the upper quartile of PF, those in the first quartile had a more than twofold (OR 2.26; 95% CI 1.02, 4.99; P = 0.04) increased risk of CBC.
Results from conditional logistic regression models restricted to cases with asynchronous CBC and their matched controls are reported in Table 4. Compared with women in the upper quartile of physical HRQOL, women in the first quartile had a 1.8-fold (95% CI 0.78, 4.30; P = 0.17) increased risk of asynchronous CBC, but confidence intervals included 1.0. Compared with women in the upper quartile of PF, those in the first quartile had a more than twofold (OR 2.72; 95% CI 1.10, 6.71; P = 0.03) increased risk of asynchronous CBC.
Discussion
In this population-based cohort of older women with invasive UBC, we observed an association between lower physical functioning scores and increased risk of CBC. Analyses that were restricted to asynchronous CBC that occurred > 12 months after primary breast cancer were also consistent with an increased risk associated with low physical functioning scores.
Differences in initial UBC treatment among older women with poor physical functioning may also contribute to the differential risk of subsequent CBC. The interplay between factors leading to undertreatment of older, comorbid women is complex. In a SEER Medicare study of adjuvant chemotherapy use from 1991 to 1999 in women over 65 with stage-III breast cancer, increasing age was associated with a significantly lower odds of receiving chemotherapy. Compared with women 65–69 years old, the odds of receiving chemotherapy among women 70–75 was 0.48 and 0.23 among those 75–79. In a National Health Service study of chemotherapy use among women over 70 years old diagnosed with early breast cancer, multivariable models found that older age and worse performance status were significantly associated with not being offered chemotherapy [33]. Commonly cited reasons for not offering chemotherapy in that study included minimal benefits, comorbidities, and patient frailty. Physical functioning plays an important role in treatment decisions. Women with functional limitations are more likely to be older, overweight or obese, less physically active, and less likely to receive chemotherapy and radiotherapy [34]. Frailty or prefrailty in women over age 65 is also associated with a reduced likelihood of initiating adjuvant hormonal therapy with tamoxifen or an aromatase inhibitor, and discontinuation of these treatments is significantly associated with older age and perceived age-related factors [35]. The WECARE study of risk factors for CBC found that adjuvant chemotherapy was associated with a 40% reduction in the risk of developing CBC [36], and tamoxifen use was associated with a 27% reduction in the risk of CBC. Thus, our finding of increased risk of CBC in women with elderly women with lower PF may be due, at least in part, to less use of systemic adjuvant therapies in those women.
Another possible explanation for our findings is related to the dysregulation of physiologic processes that accompany frailty in older adults. For example, Marcos-Perez found that serum levels of soluble TNFα receptor II (sTNF-RII), a downstream marker of activity of the pro-inflammatory cytokine TNF-alpha, progressively increase with increasing degree of frailty in elderly individuals [37]. In one nested case–control study [38], elevated serum sTNF-RII was associated with the development of breast cancer in postmenopausal women (OR 2.44; 95% CI: 1.30–4.58 for comparison of highest to lowest tertile). These data suggest that our observed association of frailty with CBC may have a biologic basis.
Our study has several strengths, including sampling from SEER-MHOS data, a large population-based registry that included surgery type, receipt of radiation, and common comorbidities such as diabetes. These registry data provide considerable detail on multiple dimensions of health-related QOL for nearly 20 years of Medicare Advantage enrollees. Our analysis utilized both composite and subscale scores from the SF-36/VR-12, which allowed us to identify that only the physical functioning subscale was associated with increased CBC risk. Also, to account for potential survivor bias, we used risk set-based incidence density sampling to obtain estimates that are an unbiased approximation of the hazard ratio [32]. This study also fills an important gap created by the lack of clinical trial data on the impact of premorbid physical limitations on breast cancer outcomes [39].
This study also has limitations. The generalizability of our findings is restricted to women aged 65 years and older. The SEER-MHOS linked data resource is limited to Medicare managed-care enrollees, and thus lacks information on Medicare fee-for-service enrollees who constitute the majority of Medicare enrollees [40], and who may systematically differ from managed-care enrollees [41]. Our data are also limited to SEER registries, which lack information on managed-care enrollees in states with high managed-care penetration [40]. The SEER registry does not include cancers diagnosed after an individual migrates out of a registry, leading to under ascertainment of second cancers [2]. While collected in the MHOS survey [40], we did not include information on lifestyle factors which we hypothesize is part of the causal pathway between poor physical functioning and CBC risk due to extensive missing information. This paper is also limited by its observational nature and possible residual confounding due to unmeasured covariates, including primary breast treatment with adjuvant chemotherapy and endocrine therapy. Therefore, we are not able to determine causality.
In conclusion, our findings indicate that lower physical functioning is related to the risk of CBC in older breast cancer patients. Poor physical functioning is prevalent but understudied among older women with a history of breast cancer. Further study of this factor and its possible role in CBC prevention would be well motivated. Efforts to understand, minimize, and treat declines in physical functioning across the life course may reduce the risk of this adverse outcome.
References
American Cancer Society Breast Cancer Facts & Figures 2019–2020. Atlanta: American Cancer Society, Inc. 2019.
Curtis Re Fd, Ron E, Ries Lag, Hacker Dg, Edwards Bk, Tucker Ma, Fraumeni Jf Jr. (Eds) (2006) New Malignancies Among Cancer Survivors: Seer Cancer Registries, 1973–2000. Vol Nih Publ. No. 05-5302. National Cancer Institute Bethesda, Md.
Sakai T, Ozkurt E, Desantis S, Sm W, Rosenbaum L, Zheng H, Golshan M. National trends of synchronous bilateral breast cancer incidence in the United States. Breast Cancer Res Treat. 2019;178(1):161–7. https://doi.org/10.1007/S10549-019-05363-0.
Xiong Z, Yang L, Deng G, Huang X, Li X, Xie X, Wang J, Shuang Z, Wang X. Patterns of occurrence and outcomes of contralateral breast cancer: analysis of seer data. J Clin Med. 2018. https://doi.org/10.3390/Jcm7060133.
Marmor S, Portschy PR, Burke EE, Virnig BA, Tuttle TM. Prognostic factors for metachronous contralateral breast cancer: implications for management of the contralateral breast. Breast J. 2017;23(3):299–306. https://doi.org/10.1111/Tbj.12732.
Akdeniz D, Schmidt MK, Seynaeve CM, Mccool D, Giardiello D, Van Den Broek AJ, Hauptmann M, Steyerberg EW, Hooning MJ. Risk factors for metachronous contralateral breast cancer: a systematic review and meta-analysis. Breast. 2019;44:1–14. https://doi.org/10.1016/J.Breast.2018.11.005.
Kurian AW, Mcclure LA, John EM, Horn-Ross PI, Ford JM, Clarke CA. Second primary breast cancer occurrence according to hormone receptor status. J Natl Cancer Inst. 2009;101(15):1058–65. https://doi.org/10.1093/Jnci/Djp181.
Bessonova L, Taylor TH, Mehta RS, Zell JA, Anton-Culver H. Risk of a second breast cancer associated with hormone-receptor and Her2/Neu status of the first breast cancer. Cancer Epidemiol Biomarkers Prev. 2011;20(2):389–96. https://doi.org/10.1158/1055-9965.Epi-10-1016.
Li CI, Daling JR, Tang MT, Malone KE. Relationship between diabetes and risk of second primary contralateral breast cancer. Breast Cancer Res Treat. 2011;125(2):545–51. https://doi.org/10.1007/S10549-010-1035-4.
Knight JA, Bernstein L, Largent J, Capanu M, Begg CB, Mellemkjaer L, Lynch CF, Malone KE, Reiner AS, Liang X, Haile RW, Boice JD Jr, JL B. Alcohol intake and cigarette smoking and risk of a contralateral breast cancer: the women’s environmental cancer and radiation epidemiology study. Am J Epidemiol. 2009;169(8):962–8. https://doi.org/10.1093/Aje/Kwn422.
Knight JA, Fan J, Malone KE, John EM, Lynch CF, Langballe R, Bernstein L, Shore RE, Brooks JD, Reiner AS, Woods M, Liang X, Bernstein JL. Alcohol consumption and cigarette smoking in combination: a predictor of contralateral breast cancer risk in the wecare study. Int J Cancer. 2017;141(5):916–24. https://doi.org/10.1002/Ijc.30791.
Saquib N, Pierce JP, Saquib J, Flatt SW, Natarajan L, Bardwell WA, Patterson RE, Stefanick MI, Thomson CA, Rock CI, Jones LA, Gold EB, Karanja N, Parker BA. Poor physical health predicts time to additional breast cancer events and mortality in breast cancer survivors. Psychooncology. 2011;20(3):252–9. https://doi.org/10.1002/Pon.1742.
Holmes MD, Chen WY, Feskanich D, Kroenke CH, Coldits GA. Physical activity and survival after breast cancer diagnosis. JAMA. 2005;293(20):2479–86. https://doi.org/10.1001/Jama.293.20.2479.
Lahart IM, Metsios GS, Nevil AM, Carmichael AR. Physical activity, risk of death and recurrence in breast cancer survivors: a systematic review and meta-analysis of epidemiological studies. Acta Oncol. 2015;54(5):635–54. https://doi.org/10.3109/0284186x.2014.998275.
Cannioto RA, Hutson A, Dighe S, Mccann W, Mccann SE, Zirpoli GR, Barlow W, Kelly KM, Denysschen CA, Dl H, Unger JM, Moore HCF, Stewart JA, Isaacs C, Hobday TJ, Salim M, Hortobagyi GN, Gralow J, Albain KS, Budd GT, Ambrosone CB. Physical activity before during and after chemotherapy for high-risk breast cancer relationships with survival. J Natl Cancer Inst. 2020. https://doi.org/10.1093/Jnci/Djaa046.
Courneya KS, Segal RJ, McKenzie DC, Dong H, Gelmon K, Friedenreich CM, Yasui Y, Reid RD, Crawforf JJ, Mackey JR. Effects of exercise during adjuvant chemotherapy on breast cancer outcomes. Med Sci Sports Exerc. 2014;46(9):1744–51. https://doi.org/10.1249/Mss.0000000000000297.
Ibrahim EM, Al-Homaidh A. Physical activity and survival after breast cancer diagnosis: meta-analysis of published studies. Med Oncol. 2011;28(3):753–65. https://doi.org/10.1007/S12032-010-9536-X.
Sweeney C, Schmitz KH, Lazovich D, Virnig BA, Wallace RB, Folsom AR. Functional limitations in elderly female cancer survivors. J Natl Cancer Inst. 2006;98(8):521–9. https://doi.org/10.1093/Jnci/Djj130.
Holick CN, Newcomb PA, Trentham-Dietz A, Titus-Ernstoff L, Bersch AJ, Stampfer MJ, Baron JA, Egan KM, Willett WC. Physical activity and survival after diagnosis of invasive breast cancer. Cancer Epidemiol Biomarkers Prev. 2008;17(2):379–86. https://doi.org/10.1158/1055-9965.Epi-07-0771.
Mandelblatt JS, Cai L, Luta G, Kimmick G, Clapp J, Isaacs C, Pitcher B, Barry W, Winer E, Sugarman S, Hudis C, Muss H, Cohen HJ, Hurria A. Frailty and long-term mortality of older breast cancer patients: Calgb 369901 (Alliance). Breast Cancer Res Treat. 2017;164(1):107–17. https://doi.org/10.1007/S10549-017-4222-8.
Kent EE, Malinoff R, Rozjabek HM, Ambs A, Clauser SB, Topor MA, Yuan G, Burroughs J, Rodgers AB, Demichele K. Revisiting the surveillance epidemiology and end results cancer registry and medicare health outcomes survey (Seer-Mhos) linked data resource for patient-reported outcomes research in older adults with cancer. J Am Geriatr Soc. 2016;64(1):186–92. https://doi.org/10.1111/Jgs.13888E.
Program Ncihdr The Seer Mhos Data File: Seer prorgram data and overview https://healthcaredelivery.cancer.gov/Seer-Mhos/Aboutdata/Overview.html. Accessed 10 Aug 2021.
Program Ncihdr total number of Seer-Mhos participants. https://Healthcaredelivery.Cancer.Gov/Seer-Mhos/Aboutdata/Num_Patients.html. Accessed 10 Aug 2021.
Program Ncihdr response rates to Mhos baseline survey. https://Healthcaredelivery.Cancer.Gov/Seer-Mhos/Aboutdata/Table.Response.Rates-Baseline.html. Accessed 10 Aug 2021.
Suissa S. The Quasi-Cohort approach in pharmacoepidemiology: upgrading the nested case-control. Epidemiology. 2015;26(2):242–6. https://doi.org/10.1097/Ede.0000000000000221.
Ware JE Jr, Sherbourne CD. The Mos 36-item short-form health survey (Sf-36). I. Conceptual framework and item selection. Med Care. 1992;30(6):473–83.
Iqbal SRW, Selim A, Quian S, Lee A, Ren X, Rothendler J, Miller D, Kazis L. The Veterans Rand 12 Item Health Survey (Vr-12): what it is and how it is used, 2007.
Hays RD, Cathy DS, Rebecca M. User's manual for the medical outcomes study (Mos) core measures of health-related quality of life, 1995.
Selim A, Rogers W, Qian S, Rothendler JA, Kent EE, Kazis LE. A new algorithm to build bridges between two patient-reported health outcome instruments: The Mos Sf-36(R) and the Vr-12 health survey. Qual Life Res. 2018;27(8):2195–206. https://doi.org/10.1007/S11136-018-1850-3.
Zhou J, Asfaw AA, Nabulsi NA, Mukand NA, Lee I, Ko NY, Boudreau DM, Calip GS. Hsr20–113: diabetes complications and risks of breast cancer recurrence among older women. JNCCN. 2020;18(3.5):Hsr20-113. https://doi.org/10.6004/Jnccn.2019.7475.
Chen L, Chubak J, Boudreau DM, Barlow WE, Weiss NS, Li CI. Diabetes treatments and risks of adverse breast cancer outcomes among early-stage breast cancer patients: a seer-medicare analysis. Cancer Res. 2017;77(21):6033–41. https://doi.org/10.1158/0008-5472.Can-17-0687.
Essebag V, Platt RW, Abrahamowicz M, Pilote L. Comparison of nested case-control and survival analysis methodologies for analysis of time-dependent exposure. BMC Med Res Methodol. 2005;5(1):5. https://doi.org/10.1186/1471-2288-5-5.
Ring A, Harder H, Langridge C, Ballinger RS, Fallowfield LJ. Adjuvant chemotherapy in elderly women with breast cancer (Achew): an observational study identifying Mdt perceptions and barriers to decision making. Ann Oncol. 2013;24(5):1211–9. https://doi.org/10.1093/Annonc/Mds642.
Braithwaite D, Satariano WA, Sternfeld B, Hiatt RA, Ganz PA, Kerlikowske K, Moore DH, Slattery MI, Tammemagi M, Castillo A, Melisko M, Esserman L, Weltzien EK, Caan BJ. Long-term prognostic role of functional limitations among women with breast cancer. J Natl Cancer Inst. 2010;102(19):1468–77. https://doi.org/10.1093/Jnci/Djq344.
Sheppard VB, Faul LA, Luta G, Clapp JD, Rl Y, Wang JH, Kimmick G, Isaacs C, Tallarico M, Barry WT, Pitcher BN, Hudis C, Winer EP, Cohen HJ, Muss HB, Hurria A, Mandelblatt JS. Frailty and adherence to adjuvant hormonal therapy in older women with breast cancer: Calgb Protocol 369901. J Clin Oncol. 2014;32(22):2318–27. https://doi.org/10.1200/Jco.2013.51.7367.
Langballe R, Mellemkjaer L, Malone KE, Lynch CF, John EM, Knight JA, Bernstein L, Brooks J, Andersson M, Reiner AS, Liang X, Woods M, Concannon PJ, Bernstein JL. Systemic therapy for breast cancer and risk of subsequent contralateral breast cancer in the wecare study. Breast Cancer Research : Bcr. 2016;18(1):65. https://doi.org/10.1186/S13058-016-0726-0.
Marcos-Perez D, Sanchez-Flores M, Maseda A, Lorenzo-Lopez L, Millan-Calenti JC, Gostner JM, Fuchs D, Pasaro E, Laffon B, Valdiglesias V. Frailty in older adults is associated with plasma concentrations of inflammatory mediators but not with lymphocyte subpopulations. Front Immunol. 2018;9:1056. https://doi.org/10.3389/Fimmu.2018.01056.
Gross AL, Newschaffer CJ, Hoffman-Bolton J, Rifai N, Visvanathan K. Adipocytokines, inflammation, and breast cancer risk in postmenopausal women: a prospective study. Cancer Epidemiol Biomarkers Prev. 2013;22(7):1319–24. https://doi.org/10.1158/1055-9965.Epi-12-1444.
De Glas NA, Hamaker ME, Kiderlen M, De Craen AJ, Mooijaart SP, Van De Velde CJ, Van Munster BC, Portielje JE, Liefers GJ, Bastiaannet E. Choosing relevant endpoints for older breast cancer patients in clinical trials: an overview of all current clinical trials on breast cancer treatment. Breast Cancer Res Treat. 2014;146(3):591–7. https://doi.org/10.1007/S10549-014-3038-Z.
Ambs A, Warren JL, Bellizzi KM, Topor M, Haffer SC, Clauser SB. Overview of the seer-medicare health outcomes survey linked dataset. Health Care Financ Rev. 2008;29(4):5–21.
Riley G. Two-year changes in health and functional status among elderly medicare beneficiaries in Hmos and fee-for-service. Health Serv Res. 2000;35(5 Pt 3):44–59.
Acknowledgements
This study used data from the Surveillance, Epidemiology, and End Results (SEER)—Medicare Health Outcomes Survey (MHOS) linked data resource. The authors acknowledge the role of the National Cancer Institute; the Centers for Medicare and Medicaid Services; MHOS; Information Management Services, Inc; and the SEER Program tumor registries in the creation of the SEER-MHOS database. The National Cancer Institute provided suggested edits and approval of the manuscript before final journal submission.
Funding
NHM was supported by the University of Illinois Cancer Center Pfizer Fellowship. Research reported in this publication was supported, in part, by the National Institutes of Health’s National Cancer Institute, Grant Numbers U54CA202995, U54CA202997, and U54CA203000. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Dr. Calip reports current employment with Flatiron Health, Inc., which is an independent subsidiary of the Roche group; stock ownership in Roche; and research funding from Pfizer, Inc. unrelated to this study awarded to the University of Illinois at Chicago.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
About this article

Cite this article
Mukand, N.H., Ko, N.Y., Nabulsi, N.A. et al. The association between physical health-related quality of life, physical functioning, and risk of contralateral breast cancer among older women. Breast Cancer 29, 287–295 (2022). https://doi.org/10.1007/s12282-021-01309-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12282-021-01309-x