
Abstract
Background
There is limited information on indocyanine green (ICG) fluorescence and blue dye for detecting sentinel lymph node (SLN) in early breast cancer. A retrospective study was conducted to assess the feasibility of an SLN biopsy using the combination of ICG fluorescence and the blue dye method.
Methods
Seven hundred and fourteen patients with clinically node-negative breast cancer were included in this study. They underwent SLN biopsy using a combination of ICG fluorescence and the blue dye method from March 2007 to February 2014. The ICG (a fluorescence-emitting source) and patent blue (the blue dye) were injected into the patients’ subareolar region. The removed lymph nodes that had ICG fluorescence and/or blue dye uptake were defined as SLNs. The results of the SLN biopsies and follow-up results of patients who underwent SLN biopsy alone were investigated.
Results
In 711 out of 714 patients, SLNs were identified by a combination of ICG fluorescence and the blue dye method (detection rate, 99.6 %). The average number of SLNs was 2.4 (range 1–7), and the average number of resected swollen para-SLNs was 0.4 (range 0–5). Ninety-nine patients with an SLN and/or para-SLN involvement during the intraoperative pathological diagnosis underwent axillary lymph node resection (ALND). In addition, two of three patients whose SLN was not identified also underwent ALND. In 46 of 101 patients with an ALND, non-SLN involvement was not found. Follow-up results were analyzed in 464 patients with invasive carcinoma excluding those with ductal carcinoma in situ (n = 148) and those who underwent ALND (n = 101). During the follow-up period (range 4.4–87.7 months; median, 38 months), two patients (0.4 %) developed axillary lymph node recurrence. They were successfully salvaged, and to date, no further locoregional recurrence has been observed.
Conclusions
A high rate of SLN detection and low rate of axillary lymph node recurrence were confirmed by an SLN biopsy using a combination of ICG fluorescence and the blue dye method. Therefore, it is suggested that this method may replace the combination of dye and radioisotope methods.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Sentinel lymph node (SLN) biopsy has become a standard procedure in early breast cancer detection, not only in western countries but also in Japan [1], and large-scale studies have not shown the efficiency of axillary lymph node dissection (ALND) on the outcomes of patients with SLN-negative breast cancer [2]. Moreover, the American College of Surgeons Oncology Group’s (ACOSOG) Z0011 trial suggested that avoidance of an ALND may be permitted even for SLN-positive patients [3]. The American Society of Clinical Oncology’s (ASCO) guideline recommendations published in 2014 stated that women without SLN metastases should not receive an ALND and that women with one to two metastatic SLNs planning to undergo breast-conserving surgery with whole-breast radiation should not undergo ALND, in most cases [4]. Breast cancer clinical practice guidelines currently available in Japan recommended an SLN biopsy using a combination of dye and radioisotope (RI) methods based on several reports [5–7].However, RI has the disadvantages of requiring a radioactive facility, causing exposure to radiation, and a high cost. In contrast, the blue dye method is easy to perform, even though SLN identification rate is reported to be lower when compared to the RI method, and some patients experience an allergic reaction [8].
Indocyanine green (ICG) in plasma emits light at the wavelength of 760 nm and produces fluorescence at 830 nm, which are visualized as a real-time image with a photodynamic eye (PDE) camera. Therefore, the ICG fluorescence method is suited for intraoperative SLN biopsy [9–13]. Since ICG alone is not as sensitive a dye for color perception [14], we have occasionally had difficulty in identifying an SLN using a dye method without fluorescence. Moreover, fluorescence is more sensitive than RI [15], and the ICG can spread further within the lymphatic basin because of its low molecular weight [12]. Therefore, the ICG fluorescence method has led to too many SLNs or difficulty in identifying SLNs due to frequent leaks in the ICG. To solve these problems, the patent blue was used in combination with the ICG as a dye. The patent blue seems to be better as a dye for color perception than ICG alone [12, 15]. The present study was performed to demonstrate the efficiency of ICG fluorescence and the blue dye method, and we describe the follow-up results of patients who underwent SLN biopsy alone using this method.
Patients and methods
We have performed SLN biopsy using the combination of ICG fluorescence and the blue dye (patent blue) method in primary breast cancer patients with a T1–3 tumor without clinical axillary lymph node metastasis (N0) and distant metastasis (M0) at the Kaizuka City Hospital from March 2007 to February 2014. Patients who had preoperative systemic therapy (e.g., chemotherapy or endocrine therapy) were excluded. Administration of the patent blue was approved by the local ethics committees at our hospital. Well-trained surgeons performed the SLN biopsy according to the standard procedure.
Sentinel lymph node (SLNs) were defined as: axillary lymph nodes, which are blue-stained and/or have positive ICG fluorescence, as detected with a PDE. Para-SLNs were defined as surgically removed swollen axillary lymph nodes that contained neither ICG fluorescence nor blue dye inside. Since swollen nodes other than blue nodes may be considered similar to SLNs in a wide sense of the sentinel node concept, we resected the swollen para-SLNs, if any.
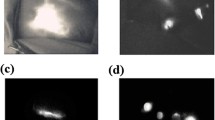
During the procedure an agent, which was a mixture of 1.0 mL of 0.5 % ICG as a source of fluorescence and 2.0 mL of 1 % patent blue as a blue dye, was injected into the subareolar area after administering general anesthesia and sterilizing the operation site. After 3.5–5.0 min of breast massage, the lymphatic flow pathway was traced with a PDE camera (a charge-coupled device; Hamamatsu Photonics Co., Hamamatsu, Japan) (Fig. 1a). An appropriate skin incision was made at the point where the lymphatic flow drained into the axillary area, and then the patent blue and/or ICG stained lymph nodes were removed (Fig. 1b). The resected lymph nodes were examined with a PDE and were classified as SLNs or para-SLNs according to ICG fluorescence and/or blue dye detection (Fig. 1c). SLN metastasis was detected with intraoperative hematoxylin and eosin-based histopathologic examination of sliced 2 mm sections of frozen tissues.

a The lymphatic flow pathway of the indocyanine green (ICG) fluorescence is traced with a photodynamic eye (PDE) camera. b After an appropriate skin incision is made at the point where the lymphatic flow drained into the axilla, the patent blue and/or ICG stained lymph nodes are removed. c The resected lymph nodes are examined with a PDE and are classified according to the ICG fluorescence and/or blue dye detection. The sentinel lymph node (SLN) have ICG fluorescence and/or blue dye. The para-SLNs have no ICG fluorescence or blue dye inside, even if ICG fluorescence and/or blue dye in the surrounding tissue are observed
The estrogen receptor (ER) and progesterone receptor (PgR) of the main breast tumor were evaluated with immunohistochemistry (IHC), and tumors with ≥1 % positively stained tumor cells were classed as positive. The HER2 status was considered positive if the IHC was 3+ or if the fluorescence in situ hybridization (HER2 to chromosome 17) was >2.2.
Results
From March 2007 to February 2014, we performed SLN biopsy in 714 patients with early breast cancer using a combination of ICG fluorescence and the blue dye method. By using this combination method, SLNs were identified in 711 of 714 patients (detection rate, 99.6 %). One of three patients who were not identified with an SLN had a history of previous surgery in the axillary area. The average number of SLNs was 2.4 (range 1–7 nodes), and the average of para-SLNs was 0.4 (range 0–5 nodes). No adverse reactions because of hypersensitivity were found.
Among 711 patients, 107 had SLN involvement in the final pathological reports. Of those, 94 patients had macrometastases of SLNs, 9 had micrometastases of SLNs, and 4 patients had isolated tumor cells (ITCs) of SLNs.
Ninety-nine patients had SLN and/or para-SLN involvement according to intraoperative pathological examination; thus, they underwent complete ALND. Of 99 patients with ALND, 46 had only SLN involvement, 50 had both SLN and non-SLN involvement, and 3 had only non-SLN involvement including para-SLN (Table 1). Two of three patients whose SLNs were not identified underwent ALND. One patient preferred not to undergo ALND.
In 612 patients with negative SLNs and para-SLNs, according to intraoperative pathological examination, 148 were diagnosed with ductal carcinoma in situ (DCIS) based on the resected specimen. Patients who underwent ALND, those with DCIS, and those whose SLNs were unidentified were excluded. Finally, 464 patients with invasive carcinoma who did not undergo ALND were included in the follow-up analysis. The patient’s characteristics are shown in Table 2. These patients had negative SLN metastasis according to intraoperative pathological reports, but two had macrometastases of SLNs, seven had micrometastases of SLNs, and two had ITCs of SLNs according to the final reports (Table 3). Adjuvant therapy was given according to St. Gallen’s recommendations or the ASCO guidelines (Table 2).
During a median follow-up of 38 months (range 4.4–87.7), 2 of 464 patients (0.4 %) developed axillary lymph node (ALN) recurrence and 11 of 464 patients (2.4 %) developed distant recurrences. However, no patient had ipsilateral breast tumor recurrence or both ALN and distant recurrences.
One patient with ALN recurrence was 45 years old at the time of the primary surgical treatment. She had a T2 tumor and underwent mastectomy; tamoxifen was administered as adjuvant therapy. The pathological reports were as follow: invasive ductal carcinoma, pT2, no involvement of 1 SLN and 2 para-SLNs, grade 2, ER positive, PgR positive, and lymphovascular invasion (LVI) positive. After a disease-free interval of 50 months, ALN recurrence occurred. Another patient with an ALN recurrence was 67 years old at the time of the primary surgical treatment. She had a T1 tumor and underwent mastectomy; letrozole was administered as adjuvant therapy. The pathological reports were as follows: invasive ductal carcinoma, pT1, no involvement of three SLNs, grade 3, ER positive, PgR positive, and LVI positive. After a disease-free interval of 24 months, ALN recurrence occurred. Both patients were successfully treated with salvage axillary dissection, and they have had no locoregional or distant recurrence after ALND (Table 4).
Discussion
Although the RI method for SLN biopsy has a high SLN detection rate, it requires a radioactive facility, stringent safety controls, and has a high cost [8]. In contrast, the ICG fluorescence method requires little skill, and the cost of the agent and device is much lower than in the RI method [12, 14]. Therefore, the use of this method has been increasing recently, especially in community hospitals in Japan.
The ICG fluorescence method is advantageous for determining the skin incision line in the axilla area of the SLN biopsy, because fluorescence of the lymphatic flow is traced with a PDE camera simultaneously. When the lymphatic flow is traced with a PDE camera, the lighting is decreased to visualize the ICG fluorescence clearly, but it is difficult to perform the SLN biopsy simultaneously in dim light [9]. Additionally, SLN detection is awkward without fluorescence under surgical light, because ICG is less sensitive than other blue dyes with regards to color perception. In former studies, the SLN biopsy using ICG without fluorescence had a low detection rate. Motomura et al. [14, 16] reported that the SLN detection rate was 73.8 % with ICG alone without fluorescence. In our experience of performing SLN biopsy with ICG alone without fluorescence between January 2003 and July 2007, the detection rate was 65.8 % (25/38 patients). We also performed SLN biopsies with dye (the patent blue) alone from August 2006 to March 2007, and the detection rate was 80.8 % (21/26 patients). Therefore, a high identification rate may be achieved by combining the patent blue with ICG which is excellent for color perception. Hojo et al. [17] showed a high identification rate with a combination of ICG fluorescence and the patent blue method. Wishart et al. [18] demonstrated that the combination of ICG and the blue dye method had the highest nodal sensitivity in a study using a three tracer (RI, blue dye, and ICG). The SLN detection rate in our study is consistent with these reports. However, we could not distinguish ICG fluorescence only-positive SLNs from both ICG fluorescence and blue dye-positive SLNs because of contamination. It was not proven that the combination method is superior to ICG fluorescence only. In fact, we had an elevated detection rate when using the combination method. This may easily detect deep SLN because of the advantages of ICG fluorescence and blue dye.
However, the prognosis after performing SLN biopsies using a combination of ICG fluorescence and the blue dye (patent blue) method is not yet clear. ACOSOG’s Z0010 trial was a large multicenter study that evaluated locoregional recurrence after a negative SLN biopsy with RI and/or blue dye method. The study demonstrated that the 5-year incident rate for local recurrence, regional recurrence, and distant recurrence were 2.4, 0.5, and 2.8 %, respectively [19]. In the current study, we observed the outcome of patients undergoing SLN biopsy using the combination method. At a median follow-up of 38 months (range 4.4–87.7), there were only 2 (0.4 %) ALN recurrences, 11 (2.4 %) distant recurrences, no local recurrence, and no patient among the SLN-negative patients with both ALN and distant recurrences.
It appears to be meaningless to statistically analyze the predictive factors related to the ALN recurrences, because the numbers of these events were too small. However, it may be noteworthy that both the patients with ALN recurrences received mastectomy, endocrine therapy, and no radiation therapy as adjuvant therapy; LVI positive in the pathological examinations was common. Schlembach et al. [20] noted that radiation therapy associated with breast-conserving surgery irradiated the entire axillary dissection field site in nearly all patients. ACOSOG’s Z0011 trial suggested that no axillary-specific irradiation is likely for treating a significant portion of the axilla [3]. Thus, no radiation therapy and LVI may be associated with ALN recurrence.
Compared with ACOSOG’s Z0011 trial, a limitation of our study was that the follow-up period was short. Considering that cases undergoing breast conservative surgery following radiation therapy were fewer in comparison with ACOSOG’s Z0010 trial (56.7 vs. 92.2 %), the results of our study may be similar to that of ACOSOG’s Z0010 trial [3, 19].
However, there may be a possible disadvantage to using ICG fluorescence and the blue dye method, because the two kinds of dye may increase shock. Fortunately, no adverse reactions due to hypersensitivity were observed in this study.
In conclusion, it is suggested that a combination of ICG fluorescence and the blue dye (patent blue) method can be substituted for a combination of RI and the blue dye method; therefore, it may be possible to avoid using RI. However, a large prospective study is needed to confirm this efficacy.
References
Saji S, Hiraoka M, Tokuda Y, Fukui N, Ikeda T. Trends in local therapy application for early breast cancer patients in the Japanese Breast Cancer Society Breast Cancer Registry during 2004–2009. Breast Cancer. 2012;19:1–3.
Rutgers EJ. Sentinel node biopsy: interpretation and management of patients with immunohistochemistry-positive sentinel nodes and those with micrometastases. J Clin Oncol. 2008;26:698–702.
Giuliano AE, Hunt KK, Ballman KV, Beitsch PD, Whiworth PW, Blumencranz P, et al. Axillary dissection vs no axillary dissection in women with invasive breast cancer and sentinel node metastasis: a randomized clinical trial. JAMA. 2011;305(6):569–75.
Lyman GH, Temin S, Edge SB, Newman LA, Turner RR, Weaver DL, et al. Sentinel lymph node biopsy for patients with early-stage breast cancer: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol. 2014;32:1365–83.
Noguchi M, Motomura K, Imoto S, Miyauchi M, Sato K, Iwata H, et al. A multicenter validation study of sentinel lymph node biopsy by the Japanese Breast Cancer Society. Breast Cancer Res Treat. 2000;63:31–40.
Cody HS 3rd, Fey J, Akhurst T, Fazzari M, Mazumdar M, Yeung H, et al. Complementarity of blue dye and isotope in sentinel node localization for breast cancer: univariate and multivariate analysis of 966 procedures. Ann Surg Oncol. 2001;8:13–9.
Goyal A, Newcomb RG, Chhabra A, Mansel RE, ALMANAC Trialists Group. Factors affecting failed localisation and false-negative rates of sentinel node biopsy in breast cancer–results of the ALMANAC validation phase. Breast Cancer Res Treat. 2006;99:203–8.
Kim T, Giuliano AE, Lyman GH. Lymphatic mapping and sentinel lymph node biopsy in early-stage breast carcinoma: a metaanalysis. Cancer. 2006;106:4–16.
Kitai T, Inomoto T, Miwa M, Shikayama T. Fluorescence navigation with indocyanine green for detecting sentinel lymph nodes in breast cancer. Breast Cancer. 2005;12:211–5.
Hirano A, Kamimura M, Ogura K, Kim N, Hattori A, Setoguchi Y, et al. A comparison of indocyanine green fluorescence imaging plus blue dye and blue dye alone for sentinel node navigation surgery in breast cancer patients. Ann Surg Oncol. 2012;19:4112–6.
Schaafsma BE, Verbeek FP, Rietbergen DD, van der Hiel B, van der Vorst JR, Liefers GJ, et al. Clinical trial of combined radio- and fluorescence-guided sentinel lymph node biopsy in breast cancer. Br J Surg. 2013;100:1037–44.
Sugie T, Sawada T, Tagaya N, Kinoshita T, Yamagami K, Toi M, et al. Comparison of the indocyanine green fluorescence and blue dye methods in detection of sentinel lymph nodes in early-stage breast cancer. Ann Surg Oncol. 2013;20:2213–8.
Jung SY, Kim SK, Kim SW, Kwon Y, Lee ES, Kang HS, et al. Comparison of sentinel lymph node biopsy guided by the multimodal method of indocyanine green fluorescence, radioisotope, and blue dye versus the radioisotope method in breast cancer: a randomized controlled trial. Ann Surg Oncol. 2014;21:1254–9.
Motomura K, Inaji H, Komoike Y, Kasugai T, Noguchi S, Koyama H. Sentinel node biopsy guided by indocyanin green dye in breast cancer patients. Jpn J Clin Oncol. 1999;29:604–7.
Ballardini B, Santoro L, Sangalli C, Gentilini O, Renne G, Lissidini G, et al. The indocyanine green method is equivalent to the 99mTc-labeled radiotracer method for identifying the sentinel node in breast cancer: a concordance and validation study. Eur J Surg Oncol. 2013;39:1332–6.
Motomura K, Inaji H, Komoike Y, Hasegawa Y, Noguchi S, Koyama H, et al. Combination technique is superior to dye alone in identification of the sentinel node in breast cancer patients. J Surg Oncol. 2001;76:95–9.
Hojo T, Nagao T, Kikuyama M, Akashi S, Kinoshita T. Evaluation of sentinel node biopsy by combined fluorescent and dye method and lymph flow for breast cancer. Breast. 2010;19:210–3.
Wishart GC, Loh SW, Jones L, Benson JR. A feasibility study (ICG-10) of indocyanine green (ICG) fluorescence mapping for sentinel lymph node detection in early breast cancer. Eur J Surg Oncol. 2012;38:651–6.
Hunt KK, Ballman KV, McCall LM, Boughey JC, Mittendorf EA, Cox CE, et al. Factors associated with local-regional recurrence after a negative sentinel node dissection: result of the ACOSOG Z0010 trial. Ann Surg. 2012;256:428–36.
Schlembach PJ, Buchholz TA, Ross MI, Kirsner SM, Salas GJ, Strom EA. Relationship of sentinel and axillary level I-II lymph nodes to tangential fields used in breast irradiation. Int J Radiat Oncol Biol Phys. 2001;51:671–8.
Conflicts of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
About this article

Cite this article
Inoue, T., Nishi, T., Nakano, Y. et al. Axillary lymph node recurrence after sentinel lymph node biopsy performed using a combination of indocyanine green fluorescence and the blue dye method in early breast cancer. Breast Cancer 23, 295–300 (2016). https://doi.org/10.1007/s12282-014-0573-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12282-014-0573-8