
Abstract
Purpose of Review
Globally, a change has been noticed in the epidemiology of fungal infections in the intensive care units (ICUs). The current review provides an insight into the current epidemiology of emerging fungal infections with special reference to their prevalence, spectrum of pathogen, outbreaks, and emergence of antifungal resistance reported from different ICUs of the world.
Recent Findings
The ICUs across the world are witnessing multiple changes in the epidemiology of fungal infections including change in prevalence and spectrum of etiological agents, new susceptible risk groups, geographical variations, emergence of novel multi-drug resistant Candida auris, outbreak due to rare fungal species, emergence of antifungal resistance, etc. An understanding of the contemporary local epidemiology of fungal agents in ICU is essential for optimal patient management.
Summary
Invasive candidiasis and invasive aspergillosis continue to haunt as major pathogens in the ICU, and several new risk factors associated with these infections have surfaced up. There is a contrasting picture for the species distribution of Candida among the different countries of the world. C. auris, the yeast behaving like bacteria, has emerged as a potential threat to ICUs across the five continents. Other mycelial agents like Mucorales, Paecilomyces spp., Fusarium spp., and Cladosporium spp., although encountered infrequently, continue to be reported as serious infections in ICU. The ICUs are also vulnerable sites for fungal infection outbreaks due to several fungi including rare ones like Cryptococcus spp., Pichia anomala, and Kodamaea ohmeri.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Patients admitted to the intensive care units (ICU) are at increased risk of dying from systemic infections. A growing proportion of those cases are due to fungi, which have high mortality compared to bacterial infections and a considerable economic impact due to prolonged ICU stay [1,2,3,4]. With the advancement of medicine and supportive therapy in critically ill patients, increased number of elderly subjects is being admitted to the ICU, thereby substantially increasing the cumulative pool of patients at-risk for fungal infections over the past decade [3]. The severity of the acute illness, use of broad-spectrum antimicrobials, status of infection prevention, and control practices are few important factors that contribute to the emergence of fungal infections in ICU patients. Although diagnostic competency for fungal infections has improved, the critical status and the non-specific presentation of the invasive disease in ICU patients often delay confirmation of etiology and appropriate management [4]. It, thus, becomes imperative that the ICU team is well versed with the epidemiology of emerging fungal infections in their healthcare setting. Invasive candidiasis (IC) and invasive aspergillosis (IA) are the most important fungal diseases in terms of occurrence rates [5]; however, the spectrum of fungi causing infection is broadening over the years. The current review aims to present a comprehensive picture of the epidemiology of emerging fungal infections in the ICU. Specifically, the areas updated in this review are as follows:
-
a)
Change in prevalence and spectrum of agent highlighting the importance of local epidemiology
-
b)
Emergence of Candida auris in ICU
-
c)
Change in host factor—new susceptible risk groups for fungal infections in ICU
-
d)
Emergence of rare fungal agents causing infections and outbreaks
-
e)
Emergence of antifungal resistance
Change in Prevalence and Spectrum of Agent Highlighting the Importance of Local Epidemiology
Clinical presentations of fungal diseases in ICU
Recently, an early occurrence of invasive candidiasis (IC) has been noted where majority of the cases occur between five to 12 days of ICU admission [6]. The prevalent types of IC in ICU patients are candidemia and Candida peritonitis. The differentiation between candidemia originating from skin flora or gastrointestinal tract colonized with Candida species helps in planning intervention strategies, as vascular catheter related candidemia is of exogenous origin compared to endogenous origin of candidemia from gut [7, 8]. Though majority of ICU patients are mechanically ventilated and Candida spp. can be isolated from respiratory tract of every one out of four such patients [9], Candida pneumonia is extremely rare [7]. Other forms of IC, meningitis, endocarditis, and endophthalmitis are witnessed infrequently in ICU.
IA can have several manifestations in the ICU and vary with the host–pathogen interactions from mere colonization and chronic colonization in pre-existing cavity to acute invasive disease. Majority of such infections involve the lungs and sinuses. The aggressive angio-invasive form is seen in neutropenic patients while chronic lesions are frequent in patients of chronic obstructive pulmonary disease (COPD) and those receiving steroids. Other manifestations include endocarditis, mediastinitis, infection of vascular graft, and osteomyelitis, which occur as sporadic cases or in outbreak settings. Involvement of central nervous system may occur by hematogenous seeding from the lungs, direct spread from sinuses or during neurosurgery [8].
Global trends in yeast and mycelial infections in ICU
-
a.
Changes in prevalence rates: Candida spp. ranked fourth (15.5%) among bloodstream infections in Australian ICUs [10] while 3.2% patients had microbiologically proven fungal blood infections in French ICUs [11]. A positive impact has been observed in 3474 ICUs of the United States of America (USA) where, the incidence of catheter-related candidemia decreased from 0.5 to 0.3/103 catheter days. This favorable decline was largely due to the empiric use of fluconazole in high-risk patients especially of surgical ICUs [12]. The rates of IC in ICU during contemporary times are depicted in Table 1. The disparity in the results of different studies is not surprising as they differ in their demographical features, healthcare practices, presence of co-morbidities, and other ICU-related interventions. Nevertheless, the true incidence of IC is expected to be much higher, as only 30–50% cases are diagnosed by a positive blood culture [32].
Table 1 Prevalence of invasive candidiasis among ICUs of different countries The recognition of IA in new susceptible groups admitted in ICU is of recent occurrence. In an Italian study covering 18 ICUs, incidence of IA was 0.2% (12 cases in 5561 patients) [33]. In another multi-centric study involving 30 ICUs from 8 countries, proven IA was seen in 17% patients (94 of 563 cohort) and another 36% had putative IA [34]. Baddley et al. [35] in their retrospective compilation of ICUs from > 600 USA hospitals over 4 years (2005–2008) reported 412/6424 (6.4%) ICU patients with IA. Among 1850 hospitalized patients in Belgium ICU, incidence of IA was 6.9% [36]. Prior studies based on autopsy findings suggest that IA is the most common missed diagnosis in ICU patients [37]. Among patients of severe hospital-acquired pneumonia admitted in Spanish ICU, the incidence of proven IA was 19% over 7 years [38]. Uncommon yet devastating, mucormycosis has been increasingly reported from ICU patients especially in India over the past half a decade [39•]. Epidemiological data specific for mucormycosis in ICU settings is largely inadequate and is derived from individual case reports or small case series [40,41,42]. Taj-Aldeen et al. [14] in their analysis of fungal disease burden in Qatar reported an incidence of 0.37 per 105 populations for mucormycosis in their ICUs. Tortorano et al. [30] reported four cases of mucormycosis in their 38-ICU study. There were two cases of Lichtheimia spp. in poly-trauma patients: one case of Rhizopus oryzae in diabetic ketoacidosis patient, and another case was diagnosed as mucormycosis after post-mortem examination of a lymphoma patient. Three cases of cutaneous mucormycosis by Lichtheimia spp. were reported as possible cross-contamination in French ICU [40]. Goncalves et al. [43] recently analyzed the fungal spores present in the ICU air of their Brazilian hospital. They isolated Penicillium spp. (15.2%) followed by Aspergillus spp., Cladosporium spp., Fusarium spp., Paecilomyces spp., Curvularia spp., Alternaria spp., Zygomycetes, and sterile mycelium. The most common species isolated in morning hours was Aspergillus spp. (14%) and in the afternoon was Cladosporium spp. (14%). Rudramurthy et al. also reported high fungal spore burden in Indian ICUs, with predominance of A. flavus and A. fumigatus [44]. The fact that these fungi are present in the ICU environment, they are potential etiologies for emerging fungal infections in the ICU given the vulnerabilities of critically ill ICU patients. Though Cryptococcal meningitis is primarily a disease of AIDS patients, such patients when admitted to ICU are prone to develop Cryptococcal bloodstream infection. In a multi-centric study involving 38 Italian ICUs [30] out of 384 fungal infections over 2 years, three were due to cryptococcosis. The clinical profile of these patients was agranulocytopenia in first, AIDS in second, and chronic renal failure in the third patient. All three succumbed to death. Owing to lack of ICU-specific data, the incidence of other fungal infections in ICU settings is difficult to estimate.
-
b.
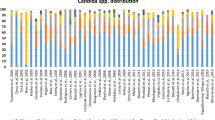
Changes in species distribution: The last two decades have witnessed a shift from C. albicans to non-albicans Candida species (NAC). Predominant species of Candida causing candidemia in ICU are depicted in Table 2. The International Surveillance Program, ARTEMIS DISK, reported a 10% fall in incidence of C. albicans over 6 years, though it was still the most commonly isolated species [50]. Broadly, in all multi-centric European studies pertaining to ICU candidemia, more than 50% cases (range 54–84%) are attributable to C. albicans, followed by C. glabrata as the second most common species in Northern Europe and C. parapsilosis in Southern Europe [30, 39•]. Prevalence of C. glabrata was double in USA as compared to Europe, predominantly at the cost of C. albicans [51]. Colombia recently reported a C. albicans to NAC ratio of 48:52 with C. tropicalis being the second most common species (38.6%) followed by C. parapsilosis (28.5%) [52]. Among other Latin American countries, C. albicans ranged from 19 to 66%, C. parapsilosis from 5 to 49%, and C. tropicalis from 9 to 39% [52]. In Argentina, Brazil, and Colombia, an increase in frequency of C. glabrata candidemia was observed in recent years [53]. In Australia, C. glabrata increased from 16% in 2004 to 26.7% in 2014 [45]. There is some fluctuation and no drastic change in the species distribution on a long-term global scale, though individual centers may experience vast variations in their Candida spectrum. Davis et al. [51], in their non-neutropenic ICU patients, observed an increase in C. glabrata from 0 to 30% over 3 years with C. tropicalis nearly disappearing during the same time in Detroit, USA.
-
c.
Range of mortality—According to Extended Prevalence of Infection in the ICU study (EPIC-II), candidemia had the highest crude ICU mortality (42.6%) compared to gram-negative (29.1%) and gram-positive (25.3%) bacteremia [54]. Two Italian studies have reported crude mortality at 30 days ranging from 39.3% [54] to 46.2% [30] for IC in their ICUs. The same was 44.7% among Indian ICUs [31•]. Attributable mortality is considered a better index though it is difficult to calculate as the demarcation between mortality due to candidemia and that due to severe underlying disease is difficult to establish. Nonetheless, Indian ICUs have reported an attributable mortality of 19.6% [31•] to candidemia while Falagas et al. [55], in their review of six studies, have reported the attributable mortality to range from 5 to 71%. With respect to different species, Dimopoulos et al. [56] documented a multivariate odds ratio of 6.7 for lethal outcome in NAC as compared to C. albicans candidemia. USA-based survey reported higher mortality (> 50%) associated with C. glabrata and C. krusei and lower mortality (28%) associated with C. parapsilosis, in comparison to C. albicans [57].
In Italian ICUs, the crude mortality rate of IA was 63% [30]. The mortality was significantly higher in medical ICUs (56%) than surgical ones (23%) (p = 0.008). In one of the earliest studies by Janssen et al. in 1996, the reported mortality rate of proven or probable IA in ICU was as high as 92% in the Netherlands despite antifungal therapy and adequate supportive care [58]. Similar high mortality of 90% was reported by Meersseman et al. in 2004 from Belgian ICUs [56]. Other studies reported crude mortalities of 80% in Spanish [59] and 76% in Belgian ICUs for IA [60]. Blot et al. [61], in their international multi-centric evaluation of European Organization for Research and Treatment of Cancer/Mycoses Study Group (EORTC/MSG) guidelines on 524 ICU patients with IA, reported a non-significant difference in mortality among proven (77%), probable (72%) and putative (67%) cases (p = 0.3). Trof et al. [62] reported that isolation of Aspergillus spp. was associated with increased mortality in critically ill patients, irrespective of invasion or colonization.
Emergence of C. auris in ICU
C. auris infection has emerged as a serious problem in ICUs of many countries, as the organism is developing antifungal resistance very fast, is easily transmitted among patients in ICU, is not easily identified by phenotypic identification system practiced in majority of the clinical laboratories, and causes severe infection with high mortality. Ever since its debut in 2009 [53], C. auris has spread to over 25 countries of five continents [63•]. In one of the largest ICU-acquired candidemia study from India, a total of 5.3% cases from 19 of 27 ICUs were due to C. auris. Significant risk factors associated with C. auris infection were admission in public-sector hospitals, longer duration of ICU stay and central venous catheter, and prior antifungal exposure. Thirty-day crude mortality of C. auris infection was 42%, and attributable mortality was 27% [64•]. Whole genome sequencing of 47 isolates identified four clades of the organism with little variation of organisms in a single clade [65].
It is not clear where from C. auris has emerged. In a hospital of the UK, only one patient was found to be colonized with C. auris while screening 2246 patients at admission [66]. In a prospective study, it was observed that after the entry of a C. auris infected patient in ICU, the organism rapidly (within 4 days) colonizes all patients. It was difficult to get rid of the colonized organism without twice daily chlorhexidine body wash. The organism can persist even on dry linen for 7 days [67]. In a systematic study from the UK, reusable skin-attached thermometers and systemic fluconazole exposure were found to be significantly associated with C. auris infection [68]. The guidelines provided by the Centre for Disease Control and Prevention (CDC), Atlanta, USA for the control of C. auris recommend (a) speciation of all Candida isolates obtained from sterile body sites like blood and cerebrospinal fluid to initiate appropriate therapy and (b) speciation of all Candida isolates obtained from non-sterile sites so as to initiate infection control practices while handling colonized patients and continue the same for at least 1 month till no evidence of transmission of C. auris exists.
Change in Host Factor—New Susceptible Risk Groups for Fungal Infections in ICU
Among the host factors, critical physiology like higher age, high Acute Physiology and Chronic Health Evaluation (APACHE-II) score, neutropenia (> 10 days), Candida colonization index (> 0.5), and critical pathology like gastrointestinal perforation, necrotizing pancreatitis, severe bacterial sepsis, and diabetes mellitus are associated with an increased risk of IC. Among the iatrogenic factors, administration of corticosteroids, broad-spectrum antimicrobials, and total parenteral nutrition; invasive procedures like central venous catheters, mechanical ventilation, and hemodialysis; and major surgeries like those of gastrointestinal system contribute to increased risk of IC [69]. Several authors have tried to elucidate the individual risk factors for IC caused by C. albicans vs NAC in the ICU. While few observed no differences in risk factors [70], majority have documented certain differences. Montagna et al. [54], in their review, have analyzed several risk factors and reported that abdominal surgery and diabetes mellitus present increased risk of C. albicans infections while antifungal prophylaxis with fluconazole decreases it. Increased age, female gender, use of corticosteroids, parenteral nutrition, neutropenia, and central venous catheters increased the risk of NAC infections. C. parapsilosis was significantly associated with parenteral nutrition as the yeast has selective growth advantage at higher glucose concentrations [71]. Use of antimicrobial agents like piperacillin–tazobactam and vancomycin increased risk of C. glabrata and C. krusei candidemia [6], and use of prior caspofungin increased breakthrough C. parapsilosis candidemia [41] while no increased risk was observed for C. glabrata on fluconazole-treated patients [72].
Any patient in ICU may acquire IC as the risk factors are commonly present in those patients. However, the IA story in ICU is still evolving. It is challenging to delineate colonization from infection in cultures growing Aspergillus spp. from non-sterile site. The diagnosis of IA is difficult as the patients do not have specific clinical features, imaging seldom help in non-neutropenic patients, and invasive sample collection is difficult in critically ill patient [73]. The clinical guideline proposed by EORTC/MSG does not help in majority of the patients due to different host factors in ICU patients [74]. In recent years, non-cancer, non-transplant patients admitted in the ICU are forming a discrete pool of population vulnerable to IA [60, 75]. Among non-neutropenic, apparently immunocompetent patients admitted in the ICU, the risk of IA is attributed to the biphasic response in sepsis wherein the initial hyper-inflammation phase is followed by the phase of immune-paralysis. The neutrophil deactivation during this latter phase puts those patients at increased risk of IA [76]. Another subset of non-neutropenic patients at particular risk of IA in ICU are those of COPD. Structural and functional alterations in the lung, frequent hospitalizations and exposure to invasive procedures, rampant administration of broad-spectrum antimicrobials, and steroid therapy contribute in predisposing a COPD lung to IA [77]. Cirrhosis, both compensated and decompensated, puts these patients at heightened risk of IA due to impaired phagocytosis [68, 78]. Environmental factors, especially the concentration of Aspergillus spores in the air, have been implicated in sporadic cases and outbreaks of IA in ICUs [79].
Among the risk factors for mucormycosis, immune-deficient patients especially those with hematological or solid organ malignancy are at increased risk. With respect to other ICU patients, increased risk is seen with patients of diabetic ketoacidosis and use of contaminated dressings in trauma patients [39•].
Emergence of Rare Fungal Agents Causing Infections and Outbreaks
Fungal agents have been threatening the already critical environment of the ICUs by appearing as outbreaks caused by uncommon species. The 1996–1998 outbreak of Pichia anomala (C. pelliculosa) at a leading tertiary care center in India involved patients of three ICUs (neonatal, neurosurgical and pediatric) with a mortality of 42%. The possible source were the contaminated hands of the healthcare workers, and the outbreak could be controlled only after improved hand-washing practices and nystatin–fluconazole prophylaxis to all ICU admitted patients [80]. Another outbreak involving a rare fungus, Kodamaea ohmeri, was reported from the same center involving 38 patients of pediatric surgery ICU in the year 2007–2008. The risk factors significantly associated with fungemia were prematurity and use of piperacillin–tazobactam and endotracheal tube, and the mortality was 50% [81]. An outbreak of C. tropicalis, involving 16 neonates between 28 and 36 weeks of gestation, was reported from North India, the fungus being isolated from the blankets and mattresses of the neonates [82]. A cluster of six cases of Cryptococcal bloodstream infection and respiratory infection was reported from USA-based ICU in 2013. No environmental source could be identified, and short-term steroid course was the only identified risk factor [83]. An outbreak consisting of five cases of gastrointestinal mucormycosis due to Rhizopus microsporus was reported in 2004 in Spanish ICU subsequent to use of contaminated wooden tongue depressors and had an attributable mortality of 40% [84]. Similarly, outbreaks and pseudo-outbreaks by contaminated bronchoscopes and other devices have been reported for Fusarium solani, Penicillium spp. and Sporothrix cyanescens [85]. Outbreaks, implicating bronchoscopes used in the ICU, have been reported for other yeast infections like Trichosporon cutaneum, Rhodotorula rubra, and Trichosporon mucoides as well [86, 87].
There are several challenges unique to emergence of such rare species in the ICU. Their epidemiology, with respect to reservoirs and modes of transmission, is not well understood, making their detection difficult. The identification of these rare agents is challenging for the microbiology laboratory as they require molecular expertise and even the specific guidelines for performing and interpreting their antifungal susceptibility are lacking. Finally, the facilities of reference laboratories are not available in all regions and countries.
Emergence of Antifungal Resistance
The ICUs bear the dual brunt of antifungal resistance. On one hand, the colonization of patients with multiple fungal agents along with administration of several antifungal agents as empiric therapy favors emergence of acquired resistance among fungal pathogens. On the other, the critically ill patient along with any breach in infection control practices causes emergence of intrinsically resistant species to outgrow others, often leading to an outbreak.
The antifungal susceptibility data for candidemia from various ICUs of the world is summarized in Table 3. Globally, C. albicans has maintained good susceptibility to nearly all antifungal agents in the ICU with the highest resistance being shown to azole group (fluconazole and voriconazole) being less than 10%, followed by echinocandins (being less than 5%). Resistance to antifungals is a major concern in C. glabrata-associated candidemia in nearly all ICUs across the world. While resistance rates range from 4% to over 50% for fluconazole and voriconazole, rates for echinocandins vary from 0% to over 30%. Resistance to amphotericin B lies within 10% in contemporary times. C. parapsilosis has shown resistance up to 20% for fluconazole in countries like China [94] and Slovakia (69) and up to 6% for echinocandins in Europe [54]. C. tropicalis has maintained high susceptibility to antifungal agents in most countries except a resistance of 6% to fluconazole reported from China [94] and 5% reported from SENTRY surveillance study (encompassing Europe, Latin America and North America) [91]. The Indian ICUs [31•], wherein C. tropicalis is the predominant species, have reported resistance to all antifungal agents ranging from 1 to 8%. Among the C. auris isolates reported from two ICU-based studies, contrasting susceptibilities have been reported. While the resistance rates to fluconazole, voriconazole, amphotericin B, and echinocandins were reported as 31%, 4%, 13.5%, and 7.7% (for caspofungin), respectively from Indian ICUs (2012, n = 52) [31•], those reported from British ICUs (2017, n = 79) [95] were 100%, 98%, 18%, and 0% (for micafungin), respectively.
Among the mycelial fungi, the susceptibility data from ICU-based studies is limited to A. fumigatus. Montagna et al. [33] isolated 12 cases of A. fumigatus infection from 18 ICUs of Italy over one and a half year. The susceptibility of five of them was performed, and all were susceptible to amphotericin B, voriconazole, posaconazole, caspofungin, and anidulafungin. In another study from ICU in the Netherlands [96], 5 out of 20 A. fumigatus strains isolated were resistant to azoles antifungals. Other studies, though not dedicated to ICU settings, have reported a prevalence of 3.2% for azole resistance in A. fumigatus isolates across 19 European countries [97] and a 100% 90-day mortality for IA by azole-resistant A. fumigatus [98].
Conclusions
The prevalence of invasive fungal infections in ICUs is on the rise especially in developing countries. Not only neutropenic patients but also non-neutropenic hosts are found to be susceptible to invasive mold infections. The spectrum of fungal agents causing those infections has broadened across the world, and the spectrum varies with geographical location of ICU. It is important to have surveillance study to know local epidemiology of invasive fungal infections. Outbreaks due to fungi have been reported in many ICUs even due to rare fungal species. Identification of those agents is a challenge in routine clinical mycology laboratory with the standard phenotypic methods. The globally emerging agent, C. auris, thrives in ICU environment, but the source of agent is still not clearly known. Recent emergence of antifungal resistance in both yeast and mycelial fungi has complicated the management of these patients. Routine antifungal susceptibility testing of fungi causing invasive infections may be important, but the breakpoints are not known for majority of emerging fungal agents. Awareness campaign and development of diagnostic mycology laboratories at every corner of globe are the need of the hour.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance
Bajwa S, Kulshrestha A. Fungal infections in intensive care unit: challenges in diagnosis and management. Ann Med Health Sci Res [Internet]. 2013;3(2):238 Available from: http://www.amhsr.org/text.asp?2013/3/2/238/113669. Accessed 9 Nov 2018.
Limper AH, Knox KS, Sarosi GA, Ampel NM, Bennett JE, Catanzaro A, et al. An official American Thoracic Society statement: treatment of fungal infections in adult pulmonary and critical care patients. Am J Respir Crit Care Med. 2011;183(1):96–128.
Blot S, Cankurtaran M, Petrovic M, Vandijck D, Lizy C, Decruyenaere J, et al. Epidemiology and outcome of nosocomial bloodstream infection in elderly critically ill patients: a comparison between middle-aged, old, and very old patients. Crit Care Med. 2009;37(5):1634–41.
Blot S, Charles P. Fungal sepsis in the ICU: are we doing better? Trends in incidence, diagnosis, and outcome. Minerva Anestesiol. 2013;79(12):1396–405.
Vincent J, Marshall J, Anzueto A, Martin CD, Gomersall C. International study of the prevalence and outcomes of infection in intensive care units. JAMA. 2009;302(21):2323–9.
Hankovszky P, Társy D, Öveges N, Molnár Z. Invasive Candida infections in the ICU: diagnosis and therapy. J Crit Care Med [Internet]. 2015;1(4):129–39 Available from:http://content.sciendo.com/view/journals/jccm/1/4/article-p129.xml. Accessed 9 Nov 2018.
Blot S, Vandewoude K. Management of invasive Candidiasis in the critically ill patients. Drugs [Internet]. 2004;64(19):2159–75 Available from:http://springerlink.bibliotecabuap.elogim.com/10.1007/978-3-642-25716-2.
Meersseman W. Invasive aspergillosis in the intensive care unit. Ann N Y Acad Sci. 2012;1272:31–9. Accessed 9 Nov 2018.
Azoulay E, Timsit JF, Tafflet M, De Lassence A, Darmon M, Zahar JR, et al. Candida colonization of the respiratory tract and subsequent Pseudomonas ventilator-associated pneumonia. Chest. 2006;129(1):110–7.
Prowle JR, Echeverri JE, Ligabo EV, Sherry N, Taori GC, Crozier TM, et al. Acquired bloodstream infection in the intensive care unit: incidence and attributable mortality. Crit Care. 2011;15(2):R100.
Quenot JP, Binquet C, Kara F, Martinet O, Ganster F, Navellou JC, et al. The epidemiology of septic shock in French intensive care units: the prospective multicenter cohort EPISS study. Crit Care. 2013;17(2):R65.
Fagan RP, Edwards JR, Park BJ, Fridkin SK, Magill SS. Incidence trends in pathogen-specific central line-associated bloodstream infections in US intensive care units, 1990–2010. Infect Control Hosp Epidemiol [Internet]. 2013;34(09):893–9 Available from:https://www.cambridge.org/core/product/identifier/S0195941700033683/type/journal_article.
Lagrou K, Maertens J, Van Even E, Denning DW. Burden of serious fungal infections in Belgium. Mycoses. 2015;58(Suppl S5):1–5.
Taj-Aldeen SJ, Chandra P, Denning DW. Burden of fungal infections in Qatar. Mycoses. 2015;58:51–7.
Rodriguez-Tudela J, Alastruey-Izquierdo A, Gago S, Cuenca-Estrella M, Leon C, Miro J, et al. Burden of serious fungal infections in Spain. Clin Microbiol Infect. 2015;21(2):183–9.
Arsenijevic V, Denning DW. Estimated burden of serious human fungal diseases in Serbia. J Fungi. 2018;4(76):1–13.
Gugnani HC, Denning DW. Burden of serious fungal infections in the Dominican Republic. J Infect Public Health [Internet]. 2016;9(1):7–12. Available from:. https://doi.org/10.1016/j.jiph.2015.04.026.
Osmanov A, Denning DW. Burden of serious fungal infections in Ukraine. Mycoses. 2015;58(Suppl. S5):94–100.
Mortensen KL, Denning DW, Arendrup MC. The burden of fungal disease in Denmark. Mycoses. 2015;58:15–21.
Ruhnke M, Groll AH, Mayser P, Ullman AJ, Mendling WM, Hof H, et al. Estimated burden of fungal infections in Germany. Mycoses. 2015;58(Suppl S5):22–8.
Sinkó J, Sulyok M, Denning DW. Burden of serious fungal diseases in Hungary. Mycoses. 2015;58:29–33.
Beardsley J, Denning DW, Chau N, Yen N, Crump J, Day J. Estimating the burden of fungal diseases in Vietnam. Mycoses. 2015;58(Suppl. S5):101–6.
Riera F, Caeiro J, Denning DW. Burden of serious fungal infections in Argentina. J Fungi. 2018;4(51):1–11.
Denning DW, Gugnani HC. Burden of serious fungal infections in Trinidad and Tobago. Mycoses. 2015;58:80–4.
Chrdle A, Mallatova N, Vasakova M, Haber J, Denning DW. Burden of serious fungal infections in the Czech Republic. Mycoses. 2015;58(Suppl. S5):6–14.
Velayuthan R, Samudi C, Lakhbeer Singh H, Ng K, Shankar E, Denning D. Estimation of the burden of serious human fungal infections in Malaysia. J Fungi [Internet]. 2018;4(1):38 Available from: http://www.mdpi.com/2309-608X/4/1/38 Accessed 9 Nov 2018.
Gugnani H, Denning DW. Estimated burden of serious fungal infections in Jamaica by literature review and modelling. West Indian Med J. 2015;64(3):245–9. Accessed 9 Nov 2018.
Wadi J, Denning DW. Burden of serious fungal infections in Jordan. J Fungi. 2018;4(15):1–12.
Gangneux JP, Bougnoux ME, Hennequin C, Godet C, Chandenier J, Denning DW, et al. Estimation du poids épidémiologique des infections fongiques graves en France. J Mycol Med [Internet]. 2016;26(4):385–90. Available from:. https://doi.org/10.1016/j.mycmed.2016.11.001.
Tortorano AM, Dho G, Prigitano A, Breda G, Grancini A, Emmi V, et al. Invasive fungal infections in the intensive care unit: a multicentre, prospective, observational study in Italy (2006–2008). Mycoses. 2012;55(1):73–9.
• Chakrabarti A, Sood P, Rudramurthy SM, Chen S, Kaur H, Capoor M, et al. Incidence, characteristics and outcome of ICU-acquired candidemia in India. Intensive Care Med. 2015;48(2):285–95 A first-of-its-kind systematic epidemiological study highlighting the wide variety of Candida spp. and their antifungal susceptibilities among Indian ICUs. Accessed 9 Nov 2018.
Alangaden GJ. Nosocomial fungal infections: epidemiology, infection control, and prevention. Infect Dis Clin North Am [Internet]. 2011;25(1):201–25. Available from:. https://doi.org/10.1016/j.idc.2010.11.003.
Montagna MT, Caggiano G, Lovero G, De Giglio O, Coretti C, Cuna T, et al. Epidemiology of invasive fungal infections in the intensive care unit: results of a multicenter Italian survey (AURORA Project). Infection. 2013;41(3):645–53.
Taccone FS, Van den Abeele AM, Bulpa P, Misset B, Meersseman W, Cardoso T, et al. Epidemiology of invasive aspergillosis in critically ill patients: clinical presentation, underlying conditions, and outcomes. Crit Care. 2015;19(1):1–15.
Baddley JW, Stephens JM, Ji X, Gao X, Schlamm HT, Tarallo M. Aspergillosis in Intensive Care Unit (ICU) patients: epidemiology and economic outcomes. BMC Infect Dis [Internet]. 2013;13(29):1–8 Available from: BMC Infectious Diseases.
Meersseman W, Vandecasteele SJ, Wilmer A, Verbeken E, Peetermans WE, Van Wijngaerdert E. Invasive aspergillosis in critically ill patients without malignancy. Am J Respir Crit Care Med. 2004;170(6):621–5.
Silfvast T, Takkunen O, Kolho E, Andersson LC, Rosenberg P. Characteristics of discrepancies between clinical and autopsy diagnoses in the intensive care unit: a 5-year review. Intensive Care Med. 2003;29(2):321–4. Accessed 9 Nov 2018.
Vallés J, Mesalles E, Mariscal D, Del Mar Fernández M, Peña R, Jiménez JL, et al. A 7-year study of severe hospital-acquired pneumonia requiring ICU admission. Intensive Care Med. 2003;29(11):1981–8.
• Bassetti M, Bouza E. Invasive mould infections in the ICU setting: complexities and solutions. J Antimicrob Chemother. 2017;72(January):i39–47. Elaborate review on mold infections with special reference to newer risk groups identified among ICU patients.
Poirier P, Nourrisson C, Gibold L, Chalus E, Guelon D, Descamp S, et al. Three cases of cutaneous mucormycosis with Lichtheimia spp. (ex Absidia/Mycocladus) in ICU. Possible cross-transmission in an intensive care unit between 2 cases. J Mycol Med [Internet]. 2013;23(4):265–9. Available from:. https://doi.org/10.1016/j.mycmed.2013.09.002.
Sipsas N, Kontoyiannis D. Invasive fungal infections in patients with cancer in the intensive care unit. Int J Antimicrob Agents. 2012;39(6):464–79.
Machicado JD, Younes M, Wolf DS. A rare cause of gastrointestinal bleeding in the intensive care unit. Gastroenterol Int. 2014;146(4):911,1136–7. Available from:. https://doi.org/10.1053/j.gastro.2013.11.038.
Gonçalves CL, Mota FV, Ferreira GF, Mendes JF, Pereira EC, Freitas CH, et al. Airborne fungi in an intensive care unit. Brazilian J Biol [Internet]. 2017;6984(0):265–70 Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1519-69842017005109104&lng=en&tlng=en.
Rudramurthy S, Singh G, Hallur V, Verma S, Chakrabarti A. High fungal spore burden with predominance of Aspergillus in hospital air of a tertiary care hospital in Chandigarh. Indian J Med Microbiol. 2016;34(4):529–32.
Chapman B, Slavin M, Marriott D, Halliday C, Kidd S, Arthur I, et al. Changing epidemiology of candidaemia in Australia. J Antimicrob Chemother. 2017;72(4):1103–8.
Colombo AL, Garnica M, Aranha Camargo LF, Da Cunha CA, Bandeira AC, Borghi D, et al. Candida glabrata: an emerging pathogen in Brazilian tertiary care hospitals. Med Mycol. 2013;51(1):38–44.
Goemaere B, Becker P, Van Wijngaerden E, Maertens J, Spriet I, Hendrickx M, et al. Increasing candidaemia incidence from 2004 to 2015 with a shift in epidemiology in patients preexposed to antifungals. Mycoses. 2018;61(2):127–33.
Lin S, Chen R, Zhu S, Wang H, Wang L, Zou J, et al. Candidemia in adults at a tertiary hospital in China: clinical characteristics, species distribution, resistance, and outcomes. Mycopathologia [Internet]. 2018;183(4):679–89. Available from:. https://doi.org/10.1007/s11046-018-0258-5.
Kreusch A, Karstaedt AS. Candidemia among adults in Soweto, South Africa, 1990–2007. Int J Infect Dis [Internet]. 2013;17(8):e621–3. Available from:. https://doi.org/10.1016/j.ijid.2013.02.010.
Pfaller MA, Diekema DJ, Rinaldi MG, Barnes R, Hu B, Veselov AV, et al. Results from the ARTEMIS DISK Global Antifungal Surveillance Study: a 6.5-year analysis of susceptibilities of Candida and other yeast species to fluconazole and voriconazole by standardized disk diffusion testing results from the ARTEMIS DISK Global Antifungal Surveillance Group. J Clin Microbiol. 2005;43(12):5848–59.
Davis SL, Vazquez JA, McKinnon PS. Epidemiology, risk factors, and outcomes of Candida albicans versus non-albicans candidemia in nonneutropenic patients. Ann Pharmacother. 2007;41(4):568–73.
Motoa G, Muñoz JS, Oñate J, Pallares CJ, Hernández C, Villegas MV. Epidemiología de aislamientos de Candida en unidades de cuidados intensivos en Colombia durante el período 2010–2013. Rev Iberoam Micol. 2017;34(1):17–22.
Satoh K, Makimura K, Hasumi Y, Nishiyama Y, Uchida K, Yamaguchi H. Candida auris sp. nov., a novel ascomycetous yeast isolated from the external ear canal of an inpatient in a Japanese hospital. Microbiol Immunol. 2009;53(1):41–4.
Montagna MT, Lovero G, Borghi E, Amato G, Andreoni S, Campion L, et al. Candidemia in intensive care unit: a nationwide prospective observational survey (GISIA-3 study) and review of the European literature from 2000 through 2013. Eur Rev Med Pharmacol Sci. 2014;18(5):661–74. Accessed 9 Nov 2018.
Falagas ME, Roussos N, Vardakas KZ. Relative frequency of albicans and the various non-albicans Candida spp among candidemia isolates from inpatients in various parts of the world: a systematic review. Int J Infect Dis [Internet]. 2010;14(11):e954–66. Available from:. https://doi.org/10.1016/j.ijid.2010.04.006.
Meersseman W. Invasive aspergillosis in the intensive care unit. Hum Fungal Pathog 2nd Ed. 2014;12:179–89.
Wisplinghoff H, Bischoff T, Tallent SM, Seifert H, Wenzel RP, Edmond MB. Nosocomial bloodstream infections in US hospitals: analysis of 24,179 cases form a prospective mnationwide surveillance study. Clin Infect Dis [Internet]. 2004;39(3):309–17 Available from: https://academic.oup.com/cid/article-lookup/doi/10.1086/421946.http://cid.oxfordjournals.org/content/39/3/309.long Accessed 9 Nov 2018.
Janssen J, van Schijndel RS, Clement E, Ossenkoppele G, Thijs L, Huijgens P. Outcome of ICU treatment in invasive aspergillosis. Intensive Care Med. 1996;22(12):1315–22.
Garnacho-montero J, Olaechea P, Alvarez-lerma F, Alvarez-rocha L, Galván B, Rodriguez A, et al. Epidemiology of fungal respiratory infections in the critically ill patient. Rev Esp Quim. 2013;17426(2):173–88.
Vandewoude KH, Blot SI, Benoit D, Colardyn F, Vogelaers D. Invasive aspergillosis in critically ill patients: attributable mortality and excesses in length of ICU stay and ventilator dependence. J Hosp Infect. 2004;56(4):269–76.
Blot SI, Taccone FS, Van Den Abeele AM, Bulpa P, Meersseman W, Brusselaers N, et al. A clinical algorithm to diagnose invasive pulmonary Aspergillosis in critically ill patients. Am J Respir Crit Care Med. 2012;186(1):56–64.
Trof RJ, Beishuizen A, Debets-Ossenkopp YJ, Girbes ARJ, Groeneveld ABJ. Management of invasive pulmonary aspergillosis in non-neutropenic critically ill patients. Intensive Care Med. 2007;33(10):1694–703.
• Forsberg K, Woodworth K, Walters M, Berkow EL, Jackson B, Chiller T, et al. Candida auris: the recent emergence of a multidrug-resistant fungal pathogen. Med Mycol [Internet]. 2018;57(August):1–12 Available from: https://academic.oup.com/mmy/advance-article/doi/10.1093/mmy/myy054/5062854. An excellent review of published literature on Candida auris with special reference to its epidemiology and rapid emergence across the globe.
• Rudramurthy SM, Chakrabarti A, Paul RA, Sood P, Kaur H, Capoor MR, et al. Candida auris candidaemia in Indian ICUs: analysis of risk factors. J Antimicrob Chemother. 2017;72(6):1794–801. A one-to-one comparison of Candida auris with other Candida spp. with respect to risk factors of the ICU patients.
Lockhart SR, Etienne KA, Vallabhaneni S, Farooqi J, Chowdhary A, Govender NP, et al. Simultaneous emergence of multidrug-resistant candida auris on 3 continents confirmed by whole-genome sequencing and epidemiological analyses. Clin Infect Dis. 2017;64(2):134–40.
Schelenz S, Hagen F, Rhodes JL, Abdolrasouli A, Chowdhary A, Hall A, et al. First hospital outbreak of the globally emerging Candida auris in a European hospital. Antimicrob Resist Infect Control [Internet]. 2016;5(1):1–7. Available from:. https://doi.org/10.1186/s13756-016-0132-5.
Biswal M, Rudramurthy SM, Jain N, Shamanth AS, Sharma D, Jain K, et al. Controlling a possible outbreak of Candida auris infection: lessons learnt from multiple interventions. J Hosp Infect [Internet]. 2017;97(4):363–70. Available from:. https://doi.org/10.1016/j.jhin.2017.09.009.
Lipke AB, Mihas AA. Non-decompensated cirrhosis as a risk factor for invasive aspergillosis: a case report and review of the immune dysfunction of cirrhosis. Am J Med Sci [Internet]. 2007;334(4):314–6. Available from:. https://doi.org/10.1097/MAJ.0b013e318068d79c.
Glöckner A, Karthaus M. Current aspects of invasive candidiasis and aspergillosis in adult intensive care patients. Mycoses. 2011;54(5):420–33.
Shorr AF, Lazarus DR, Sherner JH, Jackson WL, Morrel M, Fraser VJ, et al. Do clinical features allow for accurate prediction of fungal pathogenesis in bloodstream infections? Potential implications of the increasing prevalence of non-albicans candidemia. Crit Care Med. 2007;35(4):1077–83.
Trofa D, Gacser A, Nosanchuk J. Candida parapsilosis: an emerging fungal pathogen. Clin Microbiol Rev. 2008;21:606–25.
Magill SS, Swoboda SM, Shields CE, Colantuoni EA, Fothergill AW, Merz WG, et al. The epidemiology of candida colonization and invasive candidiasis in a surgical intensive care unit where fluconazole prophylaxis is utilized: follow-up to a randomized clinical trial. Ann Surg. 2009;249(4):657–65.
Dimopoulos G, Piagnerelli M, Berré J, Salmon I, Vincent JL. Post mortem examination in the intensive care unit: still useful? Intensive Care Med. 2004;30(11):2080–5.
Ascioglu S, Rex JH, de Pauw B, Bennett JE, Bille J, Crokaert F, et al. Defining Opportunistic invasive fungal infections in immunocompromised patients with cancer and hematopoietic stem cell transplants: an international consensus. Clin Infect Dis [Internet]. 2002;34(1):7–14 Available from: https://academic.oup.com/cid/article-lookup/doi/10.1086/323335.
Garnacho-Montero J, Amaya-Villar R. A validated clinical approach for the management of aspergillosis in critically ill patients: ready, steady, go! Crit Care. 2006;10(2):2–3.
Hartemink KJ, Paul MA, Spijkstra JJ, Girbes ARJ, Polderman KH. Immunoparalysis as a cause for invasive aspergillosis? Intensive Care Med. 2003;29(11):2068–71.
Samarakoon P, Soubani A. Invasive pulmonary aspergillosis in patients with COPD: a report of five cases and systematic review of the literature P. Chronic Resp Dis [Internet]. 2008;5(2):19–27 Available from: http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=2247706.
Prodanovic H, Cracco C, Massard J, Barrault C, Thabut D, Duguet A, et al. Invasive pulmonary aspergillosis in patients with decompensated cirrhosis: case series. BMC Gastroenterol. 2007;7:1–4.
Peláez T, Muñoz P, Guinea J, Valerio M, Giannella M, Klaassen CHW, et al. Outbreak of invasive aspergillosis after major heart surgery caused by spores in the air of the intensive care unit. Clin Infect Dis. 2012;54(3):24–31.
Chakrabarti A, Singh K, Narang A, Singhi S, Batra R, Rao KLN, et al. Outbreak of Pichia anomala infection in the pediatric service of a tertiary-care center in Northern India. J Clin Microbiol. 2001;39(5):1702–6.
Chakrabarti A, Rudramurthy SM, Kale P, Hariprasath P, Dhaliwal M, Singhi S, et al. Epidemiological study of a large cluster of fungaemia cases due to Kodamaea ohmeri in an Indian tertiary care centre. Clin Microbiol Infect. 2014;20(2):83–9.
Chowdhary A, Becker K, Fegeler W, Gugnani H, Kapoor L, Randhawa V, et al. An outbreak of candidemia due to Candida tropicalis in a neonatal intensive care unit. Mycoses. 2003;46(8):287–92.
Vallabhaneni S, Haselow D, Lloyd S, Lockhart S, Moulton-meissner H, Lester L, et al. Cluster of Cryptococcus neoformans infections in intensive care unit, Arkansas, USA, 2013. Emerg Infect Dis. 2015;21(10):1719–24.
Torres-Narbona M, Guinea J, Martínez-Alarcón J, Muñoz P, Gadea I, Bouza E. Impact of zygomycosis on microbiology workload: a survey study in Spain. J Clin Microbiol. 2007;45(6):2051–3.
Schaffer K, FitzGerald S, Commane M, Maguiness A, Fenelon L. A pseudo-outbreak of Fusarium solani in an intensive care unit associated with bronchoscopy. J Hosp Infect. 2008;69(4):398–400.
Singh N, Belen O, Léger MM, Campos JM. Cluster of trichosporon mucoides in children associated with a faulty bronchoscope. Pediatr Infect Dis J. 2003;22(7):609–12.
Jackson L, Klotz SA, Normand RE. A pseudoepidemic of sporothrix cyanescens pneumonia occurring during renovation of a bronchoscopy suite. Med Mycol. 1990;28(6):455–9.
Hrabovský V, Takáčová V, Schréterová E, Pastvová L, Hrabovská Z, Čurová K, et al. Distribution and antifungal susceptibility of yeasts isolates from intensive care unit patients. Folia Microbiol (Praha). 2017;62(6):525–30.
Alimehr S, Shekari Ebrahim Abad H, Fallah F, Rahbar M, Mohammadzadeh M, Vossoghian S, et al. Candida infection in the intensive care unit: a study of antifungal susceptibility pattern of Candida species in Milad hospital, Tehran, Iran. J Mycol Med [Internet]. 2015;25(4):e113–7. Available from:. https://doi.org/10.1016/j.mycmed.2015.09.005.
Sasso M, Roger C, Sasso M, Poujol H, Barbar S, Lefrant JY, et al. Changes in the distribution of colonising and infecting Candida spp. isolates, antifungal drug consumption and susceptibility in a French intensive care unit: a 10-year study. Mycoses. 2017;60(12):770–80.
Pfaller MA, Messer SA, Moet GJ, Jones RN, Castanheira M. Candida bloodstream infections: comparison of species distribution and resistance to echinocandin and azole antifungal agents in Intensive Care Unit (ICU) and non-ICU settings in the SENTRY Antimicrobial Surveillance Program (2008–2009). Int J Antimicrob Agents [Internet]. 2011;38(1):65–9. Available from:. https://doi.org/10.1016/j.ijantimicag.2011.02.016.
Doi AM, Pignatari ACC, Edmond MB, Marra AR, Camargo LFA, Siqueira RA, et al. Epidemiology and microbiologic characterization of nosocomial Candidemia from a Brazilian National Surveillance Program. PLoS One. 2016;11(1):e0146909. Accessed 9 Nov 2018.
• Mencarini J, Mantengoli E, Tofani L, Riccobono E, Fornaini R, Bartalesi F, et al. Evaluation of candidemia and antifungal consumption in a large tertiary care Italian hospital over a 12-year period. Infection [Internet]. 2018;46(4):469–76. https://doi.org/10.1007/s15010-018-1139-z Available from: A compilation of Candida species distribution and their susceptibilities in Italian ICUs over a decade.
Liu W, Tan J, Sun J, Xu Z, Li M, Yang Q, et al. Invasive candidiasis in intensive care units in China: in vitro antifungal susceptibility in the China-SCAN study. J Antimicrob Chemother. 2014;69(1):162–7.
Eyre DW, Sheppard AE, Madder H, Moir I, Moroney R, Quan TP, et al. A Candida auris outbreak and its control in an intensive care setting. N Engl J Med [Internet]. 2018;379(14):1322–31 Available from: http://www.nejm.org/doi/10.1056/NEJMoa1714373.
Fuhren J, Voskuil WS, Boel CHE, Haas PJA, Hagen F, Meis JF, et al. High prevalence of azole resistance in Aspergillus fumigatus isolates from high-risk patients. J Antimicrob Chemother. 2015;70(10):2894–8.
van der Linden JWM, Arendrup MC, Warris A, Lagrou K, Pelloux H, Hauser PM, et al. Prospective multicenter international surveillance of azole resistance in Aspergillus fumigatus. Emerg Infect Dis. 2015;21(6):1041–4.
Van Paassen J, Russcher A, Int’ Veld-Van Wingerden AW, Verweij PE, Kuijper EJ. Emerging aspergillosis by azole-resistant Aspergillus fumigatus at an intensive care unit in the Netherlands, 2010 to 2013. Eur Secur. 2016;21(30):1–9.
Archimedes D, Carolina A, Souza R, Colombo AL. Revisiting species distribution and antifungal susceptibility of Candida bloodstream isolates from Latin American medical centers. J Fungi [Internet]. 2017;3(4):24 Available from:http://www.mdpi.com/2309-608X/3/2/24.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Clinical Pathology
Rights and permissions
About this article

Cite this article
Chakrabarti, A., Sharma, M. Epidemiology of Emerging Fungal Infections in ICU. Curr Fungal Infect Rep 13, 1–10 (2019). https://doi.org/10.1007/s12281-019-0334-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12281-019-0334-4