
Abstract
Liver abscess is a rare complication associated with the ingestion of foreign bodies such as fish bone, which migrates to the liver through gastrointestinal tract. Here, we are reporting one such case of fish bone induced liver abscess that presented with acute small intestinal obstruction. On preoperative imaging, there was evidence of left lobe liver abscess with distal ileal transition point for obstruction and ascites. However, intraoperatively to our surprise, a foreign body, i.e., fish bone, was retrieved from liver abscess cavity, apart from ruptured liver abscess, and adhesive small bowel obstruction in distal ileum. This foreign body was identified later on revisiting the contrast-enhanced computed tomography abdomen post-operatively. We are reporting rare incidence to discuss presentation and adequate management.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Liver abscess caused by fish bone has been seldom reported in the literature. This case report spotlights a fish bone causing liver abscess and presenting as intestinal obstruction.
Case Summary
A 63-year-old lady presented to the emergency with 4 days history of fever, pain abdomen, obstipation, abdominal distension, and bilious vomiting. Patient had undergone treatment for acid peptic disease for pain upper abdomen prior to this visit. On examination, patient had tachycardia, abdominal distension, diffuse, tenderness, and bowel sounds were sluggish. On digital rectal examination, there was no significant abnormality detected.
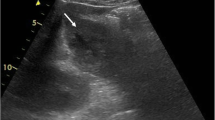
On X-ray abdomen, multiple air fluid levels with dilated small-bowel loops were seen. Ultrasonography abdomen showed a relatively ill-defined anechoic to hyperechoic lesion with hyperechoic foci measuring approximately 5.2 × 4.8 × 4.2 cm noted in segment III of liver in subcapsular location, suggestive of liver abscess with prominent bowel loops of 3 cm with sluggish peristalsis and mild ascites. CECT (contrast-enhanced computed tomography) abdomen showed 5 × 5 cm abscess in left lobe of liver with impending rupture, transition point seen distal to ileum. Proximal bowel loop dilated with mild ascites. The total leukocyte counts were slightly raised, 12,000. Liver function test panel was normal. Renal function test was deranged on admission, which became normal subsequently after fluid resuscitation.
Patient underwent exploratory laparotomy with peritoneal lavage, release of adhesive kink of terminal ileum, left lobe liver abscess cavity drainage, and abdominal drain placement. Intraoperatively, there was pyoperitoneum with pus flakes over abdominal viscera. The distal ileum was kinked due to flimsy inter-bowel adhesions, and the proximal bowel loops were dilatated with collapsed distal ileal loops. There was a ruptured left lobe liver abscess with a linear pointed foreign body retrieved from the abscess cavity as shown in Fig. 1. In the postoperative period, the preoperative CECT was reviewed and there was a linear hyperdense area amidst the left liver lobe abscess shown in Figs. 2 and 3 which was missed previously. Subsequently, on histopathologic examination, the foreign body was suggestive of a calcified bone. However, there was no evidence of any perforation in the stomach or any other part of the gut, probably due to healing of fistula tract. The patient was monitored and subsequently discharged on day 5 postoperatively after recovery.

Fish bone retrieved from the liver abscess cavity intraoperatively

CECT abdomen showing left liver lobe abscess with foreign body in situ. Red arrow tip pointing at it

CECT showing left liver lobe abscess with foreign body in situ. Red arrow tip pointing at it
Discussion
Liver abscess is a rare complication associated with the ingestion of foreign bodies, such as fish bone. The fish bone migrates from luminal GIT (gastrointestinal tract) to liver. There are about 53 cases reported in English literature [1]. Out of which 36 of them had left lobe liver abscess probably due to migration from stomach. The most common presenting symptom was epigastric pain and fever [1]. Our patient presented with features of intestinal obstruction with liver abscess. All the cases were diagnosed preoperatively on imaging for fish bone induced liver abscess. Most of the patients underwent either surgery or image-guided drainage, while few patients received conservative treatment and the fish bone were left in situ. Among these patients, eight of them had duodenal perforation and 17 had stomach perforation. In the rest, site of perforation was not available, similar to our case. Probably the fish bone ingestion incident was old enough for the healing of the fistula tract. Upper gastrointestinal endoscopy was not performed as our patient presented with intestinal obstruction.
Patients who underwent formal laparotomy and lavage had short-term hospital stay than those who underwent image-guided laparotomy [2]. For patients, undergoing percutaneous drainage of the abscess, the foreign body persisted, thus endoscopic removal of the foreign body done to avoid recurrence [3]. Migrated foreign bodies from the GIT cause other intra-abdominal abscess as well [4]. The fistula tracts between stomach and the left lobe of liver were identified as a fibrous tract along with fish bone or regional phlegmon with embedded foreign body in stomach [2, 5]. The foreign body which causes liver abscess are associated with normal oral flora, with streptococcus being the most common [6], unlike the other pyogenic liver abscess which are usually caused by E. coli and Klebsiella spp.
Conclusion
This is the first case reporting small-bowel obstruction associated with liver abscess probably due to migration of ingested fish bone from gastrointestinal tract. A history of foreign body ingestion in the past and any episode of choking may raise suspicion preoperatively. The imaging may or may not be able to identify foreign bodies in all such cases of liver abscess. However, the presence of fistulization from gastrointestinal tract to liver should raise suspicion and any connection should be searched for during surgery and managed accordingly. It is important to identify and retrieve all remnants of any foreign body from liver abscess cavity that may cause recurrence. Thus, definitive management of the fish bone-associated liver abscess should involve drainage of liver abscess cavity with removal of the fish bone and management of gastrointestinal fistula whenever present, to control the source of infection and to prevent future recurrence.
References
Grayson N, Shanti H, Patel AG (2022) Liver abscess secondary to fishbone ingestion: case report and review of the literature. J Surg Case Rep 2:1–5 https://doi.org/10.1093/jscr/rjac026
Chong LW, Sun CK, Wu CC, Sun CK (2014) Successful treatment of liver abscess secondary to foreign body penetration of the alimentary tract: a case report and literature review. World J Gastroenterol 20(13):3703–3711
Horii K, Yamazaki O, Matsuyama M, Higaki I, Kawai S, Sakaue Y (1999) Successful treatment of a hepatic abscess that formed secondary to fish bone penetration by percutaneous transhepatic removal of the foreign body: report of a case. Surg Today 29(9):922–926
Zambrana JL, García-Gutiérrez JA, Díez F (1998) Subphrenic abscess related to the ingestion of a toothpick. N Engl J Med 338(2):133–135. https://doi.org/10.1056/NEJM199801083380216
Abel RM, Fischer JE, Hendren WH (1971) Penetration of the alimentary tract by a foreign body with migration to the liver. Arch Surg 102(3):227–228
Sim GG, Sheth SK (2019) Retained foreign body causing a liver abscess. Case Rep Emerg Med 2019:4259646. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6942747/
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation and data collection were performed by Dr. Catherine Halam, Dr. Ankita Singh, and Dr. Devender Singh. The first draft of the manuscript was written by Dr. Catherine Halam, and all authors commented on previous versions of manuscript. All authors read and approved the final manuscript. Conceptualizations: Dr. Ankita Singh. Methodology: Dr. Devender Singh. Formal analysis and investigation: Dr. Catherine Halam. Writing — original draft preparation: Dr. Catherine Halam. Review and editing: Dr. Ankita Singh. Supervision: Prof. Sunil Chumber.
Corresponding author
Ethics declarations
Ethics Approval
Not applicable.
Consent
Taken.
Data
Patient history and references.
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Halam, C., Singh, A., Singh, D. et al. A Fish Bone in the Liver Abscess with Intestinal Obstruction. Indian J Surg (2024). https://doi.org/10.1007/s12262-024-04111-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s12262-024-04111-z