
Abstract
We evaluated the effects of the oral nutritional supplement containing arginine, glutamine, and hydroxymethylbutyrate (Abound®) on healing of colonic anastomoses in experimental rat model. Seventy Wistar-Albino male rats were divided into seven groups. Colon transection and anastomosis were performed in all groups except for the sham group. In groups 2 and 5, rats were fed with standard rat chow after the operation. Oral nutritional supplement was added to standard nutrition for 3 days postoperatively in group 3 and 7 days in group 6 and preoperative 7 days plus postoperative 3 days in group 4 and preoperative 7 days plus postoperative 7 days in group 7. Bursting pressures were measured, adhesions were evaluated, and tissue samples were taken for measurement of tissue hydroxyproline levels and for histopathological examination. The usage of oral nutritional supplement had positive effects on bursting pressures, tissue hydroxyproline levels, and histopathological findings of anastomoses, but feeding with oral nutritional supplement both preoperatively and postoperatively had no additive effect on these parameters when compared with the groups that were fed only postoperatively. The mixture of arginine, glutamine, and hydroxymethylbutyrate may be safely used for achieving better healing results after colonic anastomoses.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Anastomotic leakage following colorectal resection and primary anastomosis is a major clinical problem. The increased morbidity and mortality following anastomotic leakage are considerable and lead to prolonged hospital stay. Despite vast improvements in surgical technique and devices, anastomotic leakage continues to be a clinical problem. Factors that were known to correlate with an increased leakage rate were older age, anemia, prior radiation therapy, intraperitoneal infection, level of anastomosis, low anastomoses in obese patients, malnutrition, weight loss, alcohol intake, long operative times, peritoneal contamination, and blood transfusions [1].
Nutritional state is an important factor for adequate anastomotic healing. There is a correlation between low albumin levels and an increased incidence of anastomotic leaks. Patients who undergo gastrointestinal surgery are at risk of nutritional depletion from inadequate nutritional intake, both preoperatively and postoperatively, the stress of surgery and the subsequent increase in metabolic rate. Nutritional support leads to improved nutritional status and clinical outcome in severely depleted patients. It also reduces the morbidity and length of hospital stay. Enteral feeding results in specific clinical benefits including reduced incidence of postoperative infectious complications, and improved wound healing response [2, 3].
The leucine metabolite β-hydroxy-β-methylbutyrate (HMB) has anticatabolic, anabolic, and lipolytic effects. HMB has been extensively used as an ergogenic aid; particularly among bodybuilders and athletes. The nutrient combined by arginine, glutamine, and HMB (Abound®) had been used safely in patients with cancer-cachexia and acquired immune deficiency syndrome and elderly. It reversed lean tissue loss, enhanced collagen synthesis, improved wound healing, and decreased diabetic foot ulcer duration [4–7].
According to these beneficial effects, we evaluated the effects of this oral nutritional supplement on healing of colonic anastomoses in an experimental rat model.
Materials and Methods
Animals
Seventy Wistar-Albino male rats, weighing 200–250 g, were included in the study. The rats were kept in the same laboratory conditions, fed with commercial rat chow and normal tap water. All animals were deprived of food for a period of 12 h before and after the operation, but had free access to water 2 h before anesthesia. No enteral or parenteral antibiotics were administered at any time. Rats that died during the experimental period were excluded from the study and no new rat was included in the experiment. The procedures in this experimental study were performed in accordance with the National Guidelines for the Use and Care of Laboratory Animals and approved by the Animal Ethics Committee of Ankara Research and Training Hospital.
Experimental Groups
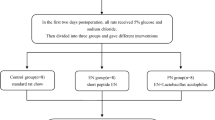
Seventy rats were randomly divided into seven groups each including ten animals. Colon transection and anastomosis were performed in all groups except for the sham group (group 1) in which laparotomy and mobilization of colon was performed and rats were fed with standard rat chow. In this group, bursting pressures were measured and tissue samples were taken for measurement of tissue hydroxyproline levels and for histopathological examination on postoperative day 7.
In group 2, rats were fed with standard rat chow after the operation. Oral nutritional supplement (including 300 mg/kg/day HMB for each rat) was added to standard nutrition for 3 days postoperatively in group 3 and preoperative 7 days plus postoperative 3 days in group 4. In these groups (groups 2, 3, 4), bursting pressures were measured and tissue samples were taken for measurement of tissue hydroxyproline levels and for histopathological examination on postoperative day 3.
In group 5, rats were fed with standard rat chow for 7 days after the operation. Oral nutritional supplement (including 300 mg/kg/day HMB for each rat) was added to standard nutrition for 7 days postoperatively in group 6 and preoperative 7 days plus postoperative 7 days in group 7. In these groups (groups 5, 6, 7), bursting pressures were measured and tissue samples were taken for measurement of tissue hydroxyproline levels and for histopathological examination on postoperative day 7.
The oral nutritional supplement that was used in this study (Abound®, Abbott, USA) is composed of glutamine (30.8 g/100 g), arginine (30.8 g/100 g), and HMB (5.4 g/100 g). There is no standard dose for this product for experimental wound healing studies. We gave the nutrient at the dose of 300 mg/kg/day HMB for each rat. This dose was given in two equal doses by orogastric tube and then the tube was taken off.
Surgical Procedure
Animals were anesthetized by intramuscular injection of 30 mg/kg ketamine hydrochloride (Ketalar®; Parke-Davis, Istanbul, Turkey) and 5 mg/kg xylasine (Rompun®; Bayer, Istanbul, Turkey). Under aseptic conditions, midline laparotomy was performed. The left colon was transected 3 cm proximal to the peritoneal reflection. Then, end-to-end anastomosis was performed by one-layer, inverting, interrupted sutures by using 6-0 polydioxanone (Ethicon, UK). The same surgeon, who was unaware of the grouping of each rat, performed all anastomoses. The fascia and skin layers of the abdomen were closed separately with continuous 3-0 silk sutures. Animals were allowed to feed 12 h after the operation. All rats were sacrificed on postoperative day 3 or 7, according to the groups, by high-dose diethyl ether inhalation. The abdominal cavity was inspected through a U-shaped incision. Colonic bursting pressures were measured and tissue samples were taken for histopathological examination and measurement of tissue hydroxyproline levels.
Evaluation of Adhesions
Adhesions were classified by another surgeon who was unaware of the groups, according to a classification system based on the resistance against stretching forces. Scores were classified as follows: 0, no resistance; 1, separated easily; 2, separated by traction; and 3, separated by sharp dissection.
Measurement of Bursting Pressure
The anastomotic segment was separated from the surrounding organs. The tissues that adhered to the anastomosis too tightly were not forced away. The colon 2.5 cm proximal and distal to the anastomosis was removed. One end of the segment was tied by 3-0 silk. The cannula was inserted into the proximal colonic segment. A catheter was inserted into the other end and tied by 3-0 silk to avoid air leaks; it was connected to an infusion pump connected to a barometer. The segment was put into a container that was filled with the water and the pressure was increased gradually. The pressure, at which the air bubbles were seen, was recorded as the bursting pressure in millimeter of mercury.
Measurement of Hydroxyproline Levels
After measurement of bursting pressures, the colonic tissues including the anastomotic segment were taken for measurement of hydroxyproline and placed into eppendorf tubes that were frozen in liquid nitrogen and stored in a deep-freezer at −80 °C. The tissue samples were weighted and 50 mg of tissues were placed into tubes, and 1 mL of 6 M HCl was added. These mixtures were hydrolyzed by autoclaving at 150 °C for 1 h. Ten microliters of these hydrolyzed samples were taken into other tubes and were allowed to dry at room temperature. Chloramine-T solution (0.2 mL) was added to the tubes. After 10 min, 1 mL of Ehrlich reagent was added and mixed. The tubes were stored at 50 °C for 90 min. After incubation, the absorbances of these solutions were measured spectrophotometrically [8].
Histological Examination
The colonic segment that was including the anastomosis was removed from each rat and the specimens were fixed in 10 % formalin, embedded in paraffin, sectioned at 4 μm, stained with hematoxylin and eosin, and examined under the light microscope with a magnification of ×100 by a pathologist blinded to the study design. The perianastomotic leucocyte, monocyte, capillary, fibroblast, and collagen contents were scored according to Ehrlich and Hunt numerical scale [9]. According to the scale, 0 meant no evidence, 1 occasional evidence, 2 light scattering, 3 abundant evidence, and 4 confluent cells or fibers.
Statistical Analysis
Hydroxyproline levels, histopathological scores, adhesion scores, and bursting pressures were compared by Kruskal-Wallis variance analysis. If the p values of the variance analyses were statistically significant, differences between groups were analyzed with the Mann-Whitney U test. Statistical analyses were performed with the SPSS 15.0 for Windows (SPSS Inc., Chicago). Values of p < 0.05 were considered to be significant.
Results
One rat from each groups of 1, 2, 3, 5, and 7 died in the postoperative period. At necropsy, the rat in group 3 had findings of ileus. Anastomotic dehiscence and peritonitis were recorded in rats in groups 2, 5, and 7. The cause of death of the rat in group 1 was thought to be due to complication of anesthesia because there was no finding of hemorrhage, peritonitis, or ileus at necropsy. Thus, since five animals were lost, the data of 65 rats were included in the final analysis.
Evaluation of Adhesion Scores
There was no significant difference between the adhesion scores of the groups (p > 0.05, Table 1).
Colonic Bursting Pressures
Mean colonic bursting pressures of groups were given in Table 1. Groups 6 and 7 had the highest levels of bursting pressures. No significant difference was found among these groups (p > 0.05). Significant difference was found between the colonic bursting pressures of group 5 against groups 6 and 7 (p < 0.05). Bursting pressures were higher in groups 6 and 7 than in group 5.
Group 2 had the lowest colonic bursting pressure values. There was no significant difference between group 3 and group 4 (p > 0.05). There was a statistically significant difference between the colonic bursting pressures of group 2 against groups 3 and 4 (p < 0.05). Bursting pressures were higher in groups 3 and 4 than in group 2.
Tissue Hydroxyproline Concentrations
The mean tissue hydroxyproline levels of the groups are given in Table 2. The highest mean hydroxyproline level was detected in group 6, and the lowest was found in group 2.
There was no significant difference between groups 6 and 7 (p > 0.05). A significant difference was found between the tissue hydroxyproline levels of group 5 against groups 6 and 7 (p < 0.05). Hydroxypyroline levels were higher in groups 6 and 7 than in group 5.
Group 2 had the lowest tissue hydroxyproline levels. There was no significant difference between group 3 and group 4 (p > 0.05). There was a statistically significant difference between the tissue hydroxyproline levels of group 2 against groups 3 and 4 (p < 0.05). Hydroxyproline levels were higher in groups 3 and 4 than in group 2.
Histopathological Evaluation
The Ehrlich-Hunter mean histopathological scores of groups were given in Table 3. There was a significant difference between the monocyte and collagen scores of group 3 and group 4 (p < 0.05). The scores of group 3 were higher than those of group 4. There was no statistically significant difference between the leukocyte, capillary, and fibroblast scores of groups 3 and 4 (p > 0.05).
A significant difference was found between all histopathological scores of group 2 against group 3 and group 4 (p < 0.05) except for the monocyte scores of groups 2 and 4 (p > 0.05). The scores of groups 3 and 4 were higher than those of group 2.
There was a significant difference between the leukocyte and capillary scores of group 6 and group 7 (p < 0.05). The scores of group 6 was higher than those of group 7, but there was no statistically significant difference between the other histopathological scores of these groups (p > 0.05).
A significant difference was found between the leukocyte and collagen scores of group 5 and group 6 (p < 0.05). There was also a significant difference between the leukocyte, capillary, and collagen scores of group 5 and group 7 (p < 0.05). These scores of groups 6 and 7 were higher than those of group 5.
The usage of oral nutritional supplement had positive effects on bursting pressures, tissue hydroxyproline levels, and histopathological findings of anastomoses, but feeding with oral nutritional supplement both pre- and postoperatively had no additive effect on these parameters when compared with the groups that were fed with oral nutritional supplement only postoperatively.
Discussion
Healing of full-thickness injury to the gastrointestinal tract remains an unresolved clinical issue. Failure of healing results in dehiscence, leaks, and fistulas, which carry significant morbidity and mortality [10, 11]. Anastomotic dehiscence is one of the most dreaded complications of operations of the large intestine. Reported rates of anastomotic dehiscence vary between 1 and 30 %, although experienced colorectal surgeons often quote 3 to 6 % as an acceptable overall leakage rate [1, 2].
Nutritional state is an important factor in contributing to anastomotic leaks. Poor nutritional intake or lack of individual nutrients significantly alters many aspects of wound healing. The possible role of single amino acids in enhanced wound healing has been studied for the last several decades. Arginine appears most active in terms of enhancing wound fibroplasia. Arginine deficiency results in decreased wound-breaking strength and wound-collagen accumulation. Oral arginine supplementation significantly increases collagen accumulation. The main effect of arginine on wound healing is to enhance wound collagen deposition. As increases in breaking strength during the first weeks of healing are directly related to new collagen synthesis, arginine supplementation may result in an improvement in wound strength as a consequence of enhanced collagen deposition. Supplementation of parenteral glutamine decreased the postoperative complications and hospital stay and in the patients undergoing the colorectal surgery for cancer. Recently, a dietary supplemental regimen of arginine, HMB, and glutamine was found to significantly and specifically enhance collagen deposition in elderly, healthy human volunteers when compared to an isocaloric, isonitrogenous [2, 10, 12].
Combining the amino acids arginine and glutamine with HMB has been shown to reverse lean tissue loss in cancer and acquired immunodeficiency syndrome patients. This supplementation improved the emotional status, decreased feeling of weakness, and increased red blood cells, hemoglobin, hematocrit, lymphocytes, and eosinophils when compared with placebo-supplemented subjects [4].
Williams et al. [5] examined the effect of arginine, HMB, and glutamine supplementation on wound collagen accumulation in 35 human volunteers 70 years or older. Collagen synthesis was significantly enhanced in healthy elderly volunteers by the oral administration of this mixture. The absence of side effects or complications within the study population indicated that oral administration of this mixture provided a safe and effective nutritional means for increasing wound repair in this age group [5]. According to these data, we thought that this mixture might have positive effects on anastomotic healing since collagen is the single most important molecule for determining intestinal wall strength. As we thought the collagen scores of the groups that were fed with oral nutritional supplement were higher than the groups that were fed only with standard rat diet (Table 3). Hydroxyproline is a major component of the protein collagen. Hydroxyproline and proline play key roles for collagen stability. In our study, the levels of hydroxyproline were also higher in study groups when compared with the control groups. These levels were also correlated with the bursting pressures.
Tatti et al. [7] found that supplementation with combination of HMB, glutamine, and arginine significantly decreased the ulcer duration. They suggested that this combination had potential clinical usefulness in treatment of diabetic foot ulcers.
Several studies indicated no adverse effects from HMB supplementation. It appears to be safe when taken over several months, with 3–6-g dosages in humans. It has no adverse effects on the hepatic enzyme function, lipid profile, renal function, or immune system. In summary, available evidence suggests that HMB supplementation is safe and may potentially improve several markers of health [6, 13–16].
Despite these studies about the benefits of the mixture of arginine, HMB, and glutamine, there is not any study about the effects of this nutrient on healing of intestinal anastomoses. In the present study, we evaluated the effects of this mixture on the healing of intestinal anastomoses. The usage of this oral nutritional supplement had positive effects on bursting pressures, tissue hydroxyproline levels, and histopathological findings of anastomoses, but feeding with oral nutritional supplement both pre- and postoperatively had no additive effect on these parameters when compared with the groups that were fed with oral nutritional supplement only postoperatively. There are a lot of studies which investigated the effects of perioperative nutritional support on patient outcomes. The role of preoperative nutritional support is to improve undernutrition before surgery, while postoperative nutrition aims at maintaining nutritional status in the catabolic period after surgery. The timing of nutritional support is widely debated [17]. Regarding perioperative nutrition support, the ESPEN guidelines on enteral nutrition in surgery and organ transplantation recommend that patients with severe nutritional risk should receive nutritional support 10–14 days prior to major surgery even if it means delaying surgery. Patients who do not meet their requirements from a normal diet should be encouraged to take oral supplements or enteral nutrition should be administered prior to hospital admission [18]. In one study, Smedley et al. [19] found that perioperative oral nutritional supplementation started before hospital admission for lower gastrointestinal tract surgery significantly diminished the degree of weight loss and incidence of minor complications and was cost-effective. In another study, van Bokhorst-De Van Der Schueren et al. [20] demonstrated that 9 days of preoperative tube feeding, with or without arginine, did not significantly improve nutritional status, reduce the surgery-induced immune suppression, or affect clinical outcome in severely malnourished head and neck cancer patients. However, the effect of preoperative nutrition on wound healing was not studied widely. In our study, we found conflicting results about perioperative nutritional support. Feeding with oral nutritional supplement both pre- and postoperatively had no additive effect on wound healing parameters. We thought that the duration of preoperative oral supplementatiom might be inadequate. So, forthcoming studies should examine the effect of preoperative supplementation on wound healing for different durations.
In conclusion, the mixture of arginine, HMB, and glutamine may be safely used for achieving better healing results after intestinal anastomoses. Control groups did not have any other caloric supplementation. Although the difference of calories has influence on the improvement of anastomotic strength, we think that ingredients of the oral supplement such as arginine, glutamine, and HMB have further positive effects on anastomotic healing rather than caloric supplementation. The positive effects of arginine and glutamine on wound healing have been known for years, but we did not determine whether HMB had an additive effect on wound healing or not. So, further studies, which will compare the oral nutritional supplements including arginine and glutamine against the mixture used in this study, are needed for evaluating the additive effects of HMB on wound healing.
References
Nasirkhan MU, Abir F, Longo W et al (2006) Anastomotic disruption after large bowel resection. World J Gastroenterol 12:2497–2504
Kingham TP, Pachter HL (2009) Colonic anastomotic leak: risk factors, diagnosis, and treatment. J Am Coll Surg 208:269–278
Ward N (2003) Nutrition support to patients undergoing gastrointestinal surgery. Nutr J 2:18
Rathmacher JA, Nissen S, Panton L et al (2004) Supplementation with a combination of beta-hydroxy-beta-methylbutyrate (HMB), arginine, and glutamine is safe and could improve hematological parameters. J Parenter Enteral Nutr 28:65–75
Williams JZ, Abumrad N, Barbul A (2002) Effect of a specialized amino acid mixture on human collagen deposition. Ann Surg 236:369–374
Wilson GJ, Wilson JM, Manninen AH (2008) Effects of beta-hydroxy-beta-methylbutyrate (HMB) on exercise performance and body composition across varying levels of age, sex, and training experience: a review. Nutr Metab 5:1
Tatti P, Barber AE, Masselli PML (2010) Nutritional supplement is associated with a reduction in healing time and improvement of fat free body mass in patients with diabetic foot ulcers. EWMA J 10:13–17
Jamall IS, Finelli VN, Que Hee SS (1981) A simple method to determine nanogram levels of 4-hydroxyproline in biological tissues. Anal Biochem 112:70–75
Ehrlich HP, Tarver H, Hunt TK (1973) Effects of vitamin A and glucocorticoids upon inflammation and collagen synthesis. Ann Surg 177:222–227
Barbul A (2005) Wound healing. In: Brunicardi FC (ed) Schwartz’s principles of surgery, 8th edn. McGraw-Hill Medical Publishing Division, USA, pp 223–248
Ho YH, Ashour MA (2010) Techniques for colorectal anastomosis. World J Gastroenterol 16:1610–1621
Oguz M, Kerem M, Bedirli A et al (2007) L-Alanin-L-glutamine supplementation improves the outcome after colorectal surgery for cancer. Colorectal Dis 9:515–520
Nissen S, Sharp R, Ray M et al (1996) Effect of leucine metabolite beta-hydroxy-beta-methylbutyrate on muscle metabolism during resistance-exercise training. J Appl Physiol 81:2095–2104
Vukovich MD, Stubbs NB, Bohlken RM (2001) Body composition in 70-year-old adults responds to dietary beta-hydroxy-beta-methylbutyrate similarly to that of young adults. J Nutr 131:2049–2052
Nissen S, Sharp RL, Panton L et al (2000) Beta-hydroxy-beta methylbutyrate (HMB) supplementation in humans is safe and may decrease cardiovascular risk factors. J Nutr 130:1937–1945
Gallagher PM, Carrithers JA, Godard MP et al (2000) Beta-hydroxy-beta-methylbutyrate ingestion, part II: effects on hematology, hepatic and renal function. Med Sci Sports Exerc 32:2116–2119
Cerantola Y, Grass F, Cristaudi A et al. (2011) Perioperative nutrition in abdominal surgery: recommendations and reality. Gastroenterol Res Pract 2011:739347
Kotze V (2011) Perioperative nutrition: what do we know? S Afr J Clin Nutr 24:S19–S22
Smedley F, Bowling T, James M et al. (2004) Randomized clinical trial of the effects of preoperative and postoperative oral nutritional supplements on clinical course and cost of care. Br J Surg 91:983–990
van Bokhorst-De Van Der Schueren MA, Quak JJ, von Blomberg-van der Flier BM et al. (2001) Effect of perioperative nutrition, with and without arginine supplementation, on nutritional status, immune function, postoperative morbidity, and survival in severely malnourished head and neck cancer patients. Am J Clin Nutr 73:323–332
Conflict of Interest
We have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
The procedures in this experimental study were performed in accordance with the National Guidelines for the Use and Care of Laboratory Animals and approved by the Animal Ethics Committee of Ankara Research and Training Hospital.
Rights and permissions
About this article

Cite this article
Kusabbi, R., Kismet, K., Kuru, S. et al. Effects of the Oral Nutritional Supplement Containing Arginine, Glutamine, and Hydroxymethylbutyrate (Abound®) on Healing of Colonic Anastomoses in Rats. Indian J Surg 77 (Suppl 3), 1242–1247 (2015). https://doi.org/10.1007/s12262-015-1268-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12262-015-1268-x