
Abstract
Multi-nodular goiter (MNG) is one of the commonest thyroid gland disease. Surgery is an important treatment option in the presence of indications. There are several alternative procedures for thyroid gland operation such as subtotal thyroidectomy (STT), near-total thyroidectomy (NTT), hemi-thyroidectomy plus subtotal resection (Dunhill procedure), and total thyroidectomy (TT), but the surgical procedure of choice is still under discussion. In this study, 173 consecutive patients with multi-nodular goiter underwent thyroid operation in the department of surgery of Pursina Hospital in Rasht-Iran, using two different methods: Dunhill operation and total thyroidectomy. Outcome assessment was performed 4 days after surgery, 2 weeks, 1, 2, 10, and 20 month after surgery. Preoperative assessment, seroma, recurrent laryngeal nerve palsy, hypocalcaemia rates, and rates of other postoperative complications, final pathology, and recurrence were compared in two methods. Due to the high incidence of malignancy in this survey, TT can be the method of choice for MNG surgery. Also, TT will be more beneficial in the surgical treatment of benign thyroid disorders, especially those which are bilateral or extended to substernal space or which presented with compression symptoms.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Multi-nodular goiter (MNG) is one of the commonest thyroid gland disease [1] which sometimes presents with shortness of breath and dysphasia due to compression of the trachea and esophagus, as well as obstruction of venous flow in the head and neck. Surgery is an important treatment option in the presence of indications (compressive symptoms, high suspicion of malignancy, hyperthyroidism, cosmetic preference, etc.) [2]. There are several alternative procedures for thyroid gland operation such as subtotal thyroidectomy (STT), near-total thyroidectomy (NTT), hemi-thyroidectomy plus subtotal resection (Dunhill procedure), and total thyroidectomy (TT). But the surgical procedure of choice is still under discussion [1–3]. There are some studies which prefer TT method because of the lower incidence of goiter recurrence and less frequent need for completion thyroidectomy, especially when there is a bilateral gland involvement posterior to middle thyroid veins [4, 5].
On the other hand, there are some other investigations which avoided the TT method, because of its complications of persistent or temporary recurrent laryngeal nerve palsy and parathyroid damage [6, 7]. These surgeons declare that BST or NTT methods are better because of presuming lower incidence of postoperative complications and the attempt to achieve postoperative euthyroid status earlier. They also state that unfortunately, in these methods, there is a high recurrence rate owing to gland remnants, even under suppression hormonal treatment with l-thyroxine [8].
There are increasing numbers of publications which state that hemi-thyroidectomy plus subtotal resection (Dunhill operation) overcomes some disadvantages of bilateral subtotal or total resection. In Dunhill method, only one side has to be explored in case of reoperation, and in case of papillary microcarcinoma in the resected lobe, hemi-thyroidectomy is sufficient and a completion thyroidectomy can be avoided. The aim of this study was to compare long-term results of TT method and Dunhill operation in patients undergoing thyroid surgery for MNG.
Material and Methods
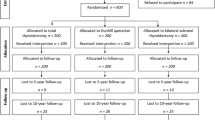
In a longitudinal prospective-descriptive study, from January 2009 to January 2011, 173 consecutive patients with multi-nodular goiter underwent thyroid operation in the department of surgery of Pursina Hospital in Rasht (a city in north of Iran), using two different method: Dunhill operation (83 cases) and total thyroidectomy (90 cases). No other treatment modalities were used in these cases.
Exclusion Criteria
Exclusion criteria were as follows: suspicion of malignancy, positive family history of thyroid malignancy, Grave’s disease, thyroiditis, previous thyroid surgery, and disturbed calcium metabolism.
Preoperation Management
Clinical assessments in all patients included measurements of serum thyrotropin, thyroxine, triiodothyroxine, thyroid antibodies and calcium, fine needle aspiration (negative, suspicious, indeterminate), and ultrasound estimation of thyroid volume and morphology.
Surgery was performed under general anesthesia by an experienced surgeon. Written informed consent was obtained from all patients; patient information included detailed explanation of the two treatment alternatives under investigation and of the concept of randomization for treatment allocation.
Surgical Methods
TT method
Surgical dissection of the thyroid took place after the identification and preservation of both laryngeal nerves and superior and inferior parathyroid glands. In all patients, we identified 3–4 parathyroid glands and left them in situ with their own vascularization. If we inadvertently removed or devascularized a parathyroid gland, we autotransplanted the gland into the ipsilateral sternocleidomastoid muscle.
Dunhill Operation
A small (less than 5 g) homogeneous remnant was left unilaterally at either the superior pole or posterior depending on the location of the sonographically or intraoperatively detected nodules.
Postoperation Management
At the time of extubation, the anesthesiologist evaluated vocal cord motility in all patients. Because unilateral recurrent laryngeal nerve palsy sometimes can be clinically difficult to detect, an otolaryngologist performed a laryngoscopy in all patients before they were discharged. We defined recurrent laryngeal nerve palsy as hoarseness associated with vocal cord paralysis at laryngoscopy within 6 months postoperatively. After 6 months, we considered recurrent laryngeal nerve palsy to be permanent. Hormonal treatment with l-thyroxine began within 5 days after surgery in all patients. We drained the neck with bilateral suction drains for 48 h, and patients were usually discharged within 4 days after surgery. Calcium levels were obtained on the first and second postoperative days and at a 6-month follow-up appointment. Hypocalcemia was defined as less than 2.00 mmol/L and permanent if requiring ongoing oral calcium supplementation beyond 3 months.
Follow-up Planning
Outcome assessment was performed 4 days after surgery, two weeks, 1, 2, 10, and 20 months after surgery for each patient. All clinical variables were assessed by unbiased observer (a research surgeon who was not involved in the surgery or clinical decisions and who was blinded to the treatment group). We extracted data on sex, age, and WHO classification of goiter:
-
Grade I: palpable but visible with the neck extended
-
Grade II: visible with the neck in normal position
-
Grade III: visible from a considerable distance
Preoperative assessment (operative time, intraoperative blood loss, hematoma, mortality), seroma (a collection of fluid under the skin at the site of the surgical incision), recurrent laryngeal nerve palsy (temporary, Permanent) and hypocalcemia rates (temporary, permanent), rates of other postoperative complications, final pathology and recurrence were assessed.
We diagnosed recurrence if one of the following criteria showed up:
-
1)
Volume of one lobe more than 9 ml for women and more than 12 ml for men or volume of both lobes more than 18 ml for women and more than 24 ml for men
-
2)
Presence of a nodule more than 9 mm
-
3)
Presence of an autonomous adenoma
Statistical Analysis
Statistical analyses involved the ANOVA test for repetitive measures over time and the Mann–Whitney U test or unpaired two-tailed Student’s t test for comparisons at each group. P < 0.0001 was considered statistically significant.
Results
One hundred seventy-three patients (83 cases with Dunhill method (DO) and 90 cases with total thyroidectomy (TT)) were evaluated. There were 28 men (65 %) and 145 women (83.81 %). Their age ranged from 16 to 79 years with a mean of 45.2 ± 11.4 years. Seventy-five percent of all cases aged below 60 years. Ultrasonography of thyroid showed MNG in all patients. The minimum and maximum time between beginning of symptoms and operation time were 2 months and 40 years. More than 50 % of cases referred after 6 years of beginning manifestations. Bilateral gland involvement showed in 37.5 % (n = 65) of patients. The FNA result in 56 % of cases was negative for malignancy and was indeterminate and suspicious in 37 and 7 % of all cases. Chart 1 shows the frequency of different FNA results in all patients before surgery performed.

The frequency of different FNA results in all patients before surgery performed
The distribution of demographic features and intraoperative characteristics between the two study groups are showed in Table 1 and Chart 2. According to these data, there were no significant differences in mean age, primary presentations, bilateral involvements, and FNA results between two operation groups. The average of operative time showed no significant difference between the two approaches (43 ± 12 min versus 48 ± 11 min). The mean amount of intraoperative blood loss for DO method was 183 ± 11 ml whereas that for the TT approach was 261 ± 21 ml (P < 0.0001). No mortality happened during this survey, and postoperative hematoma requiring repeat surgery occurred in no patients. Table 2 compares the complications in the 2 groups. Transient RLN palsy was observed in only 2 from DO group and 5 from TT group (P = 0.652). There was a direct relationship between bilateral involvement and the incidence of RLN palsy (P < 0.0001). This indicates a relative risk increase of 4.38 in patients with bilateral involvement (CI95% 0.94–20.4). Other demographic features had no relation to this complication. No patients showed permanent RLN palsy. The majority of patients in both groups, however, have no disturbance in RLN function (DO group, 97.5 %; TT group, 94.4 %).

Clinical manifestations of patients at the time of presentation in 2 groups of surgery
Transient hypocalcemia was observed in 21.54 % of DO group patients and 23.33 % of TT group patients (P = 0.851). Of these 39 patients, just 2 cases showed clinical presentations of tetany and other hypocalcemia found on laboratory exams. Again, there was a statistically significant effect of bilateral involvement on the development of transient hypocalcemia and correlates with a relative risk increase of 3.14 (CI95% 1.09–9.59). Of note, postoperative normocalcemia was evident in 65 and 69 of patients from DO group and TT group, respectively.
Incidental malignancy within the pathology specimen was determined in 16 patients (1 patient with medullary carcinoma, 2 cases with follicular carcinoma, and 13 patients with papillary carcinoma). There was an equitable distribution within the two groups, with 6 cases in DO group and 10 cases in TT group. All these patients were female (P < 0.0001) and had been referred to our department due to compression problems (P < 0.0001). The majority of these patients (68.75 %) were in the group of patients with bilateral involvement with a relative risk increase of 3.58 (CI95% 1.18–10.87). The preoperative FNA results of these patients were 2 cases (with follicular carcinoma) as suspicious, 4 cases (1 case with medullary carcinoma and 3 cases with papillary carcinoma) as negative, and 10 cases (with papillary carcinoma) as indeterminate. No recurrence of MNG showed up during our follow-up.
Discussion
Goiters (from the Latin gutter, throat), which are defined as an enlargement of the thyroid, have been a cognized medical condition since 2700 B.C. [9]. A multi-nodular goiter is simply a thyroid gland that is usually enlarged and contains multiple thyroid nodules. The risk of malignancy in dominant nodules within multi-nodular goiters is approximately 10 % [10]. Surgical excision can immediately resolve local symptoms. The surgical method of benign thyroid disease treatment is still controversial. Here, we managed to compare two different methods for this surgery. The three main complications following thyroid surgery include voice hoarseness due to RLN palsy, hypocalcaemia, and postoperative hemorrhage. Due to a ligation of the all branches of vessels on superior and inferior pole, there were no patients in this study who required re-operation for hematoma. The mean amount of intraoperative blood loss for DO method was less than TT method. Also, the incidence of postoperative transient hypocalcemia (23.33 %) and transient RLN palsy (5.55 %) in patients of TT group were more. There are some other studies which showed the same results. Barczynski et al. [11] compared the results of DO, TT, and BST methods and showed that the lower incidence of postoperative transient hypocalcemia and transient RLN palsy belonged to TT group. On the other hand, on 2011, Pelei et al. [12] performed a meta-analysis on different surgery methods of MNG and concluded that there was no significant difference of postoperative complications between patients. In a study of Veyseller et al. [13] on TT method, the incidence of postoperative permanent hypocalcemia and permanent RLN palsy were 0.6 and 1.86 % whereas we had no cases of these complications. Similar to ours results, no MNG recurrence was presented in their study. Also, Bauer et al. [14] showed that although the rate of total complications is higher for patients undergoing TT procedure, the rate of permanent complications in these patients is similar to those undergoing unilateral resection. The usefulness of FNA in multi-nodular goiter is controversial. Recently, Antonio Rios et al. [15] reported that FNA is not useful for differentiating MNG with malignant degeneration from benign MNG, as more than 80 % of carcinomas go unnoticed. Al-Yaarubi et al. [16] mentioned that sensibility and specificity of FNA in determination of malignancy in MNG cases are 16 and 97 %. So, in our survey, incidental malignancy within the pathology specimen was determined in 16 patients (6 cases in DO group and 10 cases in TT group). The preoperative FNA results of these patients were 2 cases (with follicular carcinoma) as suspicious, 4 cases (1case with medullary carcinoma and 3 cases with papillary carcinoma) as negative, and 10 cases (with papillary carcinoma) as indeterminate. Patients with malignancy in DO group needed re-surgery for completion thyroidectomy, but no re-surgery performed on cases of TT group. Due to the small remnant tissue, re-operation is difficult and carries a significant risk of damage to both RLNs and the parathyroid glands, and during completion thyroidectomy, there is a 10-fold increase in iatrogenic injuries [17]. So, due to the high incidence of malignancy in this survey (10 %), TT can be the method of choice for MNG surgery. On the other hand, our results showed a direct relationship between bilateral involvement and compression symptoms with incidence of malignancy. So, when the frequency of complications in recurrent operations and the malignity possibility of the thyroid tissue left behind are taken into consideration, we believe that, despite the higher rate of post-operative complications, TT will be more beneficial in the surgical treatment of benign thyroid disorders, especially those which are bilateral or extended to substernal space or which presented with compression symptoms.
References
Unnikrishnan AG, Kalra S, Baruah M, Nair G, Nair V, Bantwal G et al (2011) Endocrine society of India management guidelines for patients with thyroid nodules: a position statement. Indian J Endocrinol Metab 15:2–8
Moalem J, Suh I, Duh QY (2008) Treatment and prevention of recurrence of multinodular goiter: an evidence-based review of the literature. World J Surg 32:1301
Ho TW, Shaheen AA, Dixon E, Harvey A (2011) Utilization of thyroidectomy for benign disease in the United States: a 15-year population-based study. Am J Surg 201(5):201–570
Sheikh EA, Saadat SH, Waleem U, Heidar IZ, Haroon A, Ashfaq M (2009) Total thyroidectomy as primary elective procedure in multinodular thyroid disease. J Ayub Med Coll Abbottabad 21(4):57–59
Vassiliou J, Tympa A, Arkadopoulos N, Nikolakopoulos F, Petropoulou T, Smyrniotis V (2013) Total thyroidectomy as the single surgical option for benign and malignant thyroid disease: a surgical challenge. Arch Med Sci 9(1):74–78
Acun Z, Comert M, Cihan A, Ulukent SC, Ucan B, Cakmak GK (2004) Near-total thyroidectomy could be the best treatment for thyroid disease in endemic regions. Arch Surg 139:444–447
Olson SE, Starling J, Chen H (2007) Symptomatic benign multinodular goiter: unilateral or bilateral thyroidectomy? Surgery: 142–458
Agarwal G, Aggarwal V (2008) Is total thyroidectomy the surgical procedure of choice for benign multinodular goiter? An evidence-based review. World J Surg 32(7):1313–1324
Clark OH, Lal G (2007) Thyroid, parathyroid, and adrenal. In: Brunicardi FC, Anderson DK, Billiar TR, Dunn DL, Hunter JG, Poliock RE (eds). Schwartz’s Principles of Surgery. 8th edn. Vol. 2. The McGraw-Hill Companies. (p 37)
Harrison BJ, Maddox PR, Smith DM (2002) Disorders of the thyroid gland. In: Cuschieri A, Steel RJC, Mossa AR (eds). Essential Surgical Practice. 4th edn. Arnold
Barczyński M, Konturek A, Hubalewska-Dydejczyk A, Gołkowski F, Cichoń S, Nowak W (2010) Five-year follow-up of a randomized clinical trial of total thyroidectomy versus Dunhill operation versus bilateral subtotal thyroidectomy for multinodular nontoxic goiter. World J Surg 34(6):1203–1213
Si P, Yulin X, Yi T, Guo Y, Sun S (2012) Compare the postoperative complications incidence of benign multi-nodular goiter: a meta-analysis. Chin-Ger J Clin Oncol 11(10):575–580
Veyseller B, Aksoy F, Demirhan H, Yildirim YS, Ertaş B, Açikalin RM et al (2009) Total thyroidectomy in benign thyroid diseases. Kulak Burun Bogaz Ihtis Derg 19(6):299–303
Bauer P, Murray S, Clark N, Pontes DS, Sippel RS, Chen H (2013) Unilateral thyroidectomy for the treatment of benign multinodular goiter. J Surg Res 184(1):514–518
Ríos A, Rodríguez JM, Galindo PJ, Montoya M, Tebar FJ, Sola J et al (2004) Utility of fine-needle aspiration for diagnosis of carcinoma associated with multinodular goiter. Clin Endocrinol 61:732–737
Al-Yaarubi S, Farhan H, Al-Futaisi A, Al-Qassabi S, Al-Rasadi KH, Al-Riyami SH et al (2011) Accuracy of ultrasound-guided fine-needle aspiration cytology for diagnosis of carcinoma in patients with multinodular goiter. Indian J Endocrinol Metab 15:132–135
Reeve TS, Delbringe L, Crummer P, Smyth C (1988) Secondary thyroidectomy: a twenty-year experience. World J Surg 12:449–453
Source of Funding
Funding for this study was provided by Guilan University of Medical science.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Mobayen, M., Baghi, I., Farzan, R. et al. Comparison of the results of total thyroidectomy and Dunhill operation in surgical treatment of multinodular goiter. Indian J Surg 77 (Suppl 3), 1137–1141 (2015). https://doi.org/10.1007/s12262-015-1213-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12262-015-1213-z