
Abstract
The incidence of thyroid cancers is increasing worldwide. Some somatic oncogene mutations (BRAF, NRAS, HRAS, KRAS) as well as gene translocations (RET/PTC, PAX8/PPAR-gamma) have been associated with the development of thyroid cancer. In our study, we analyzed these genetic alterations in 394 thyroid tissue samples (197 papillary carcinomas and 197 healthy). The somatic mutations and translocations were detected by Light Cycler melting method and Real-Time Polymerase Chain Reaction techniques, respectively. In tumorous samples, 86 BRAF (44.2 %), 5 NRAS (3.1 %), 2 HRAS (1.0 %) and 1 KRAS (0.5 %) mutations were found, as well as 9 RET/PTC1 (4.6 %) and 1 RET/PTC3 (0.5 %) translocations. No genetic alteration was seen in the non tumorous control thyroid tissues. No correlation was detected between the genetic variants and the pathological subtypes of papillary cancer as well as the severity of the disease. Our results are only partly concordant with the data found in the literature.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Thyroid nodules are very common in clinical practice. Although these nodules are benign in most of the cases, approximately 5 % are malignant. The number of detected thyroid cancers has dramatically increased during the last decades. Their incidence highly depends on the diagnostic methods, as well. In Hungary (population is 10 millions), approximately 750 new thyroid cancer cases are recorded annually by National Cancer Registry.
Thyroid epithelial tumors exhibit a broad spectrum of neoplastic pathology varying from well-differentiated benign tumors to highly malignant anaplastic carcinomas. The geographical differences in the incidence of thyroid carcinomas are partly related to the variation in dietary iodine intake. In iodine-deficient areas, the rate of malignant papillary transformation is higher compared to the follicular ones [1, 2]. The incidence of undifferentiated cancer is also higher in iodine-deficient areas [3, 4] Hungary is generally considered as a heavily iodine-deficient country, such as the UK, Belgium and Poland [3, 5–8].
Papillary cancer (PTC) is the most common histological type of all thyroid malignancies (60–80 %). Somatic mutations are found in more than 40–70 % of papillary carcinoma cases. The frequencies of BRAF (v-raf murine sarcoma viral oncogene homolog B1) mutation are 40–45 %, RAS (rat sarcoma viral oncogene homolog) mutations are 10–20 %, RET/PTC (RET tyrosine-kinase proto-oncogene/papillary thyroid carcinoma) rearrangements are 10–20 % in case of PTC [1, 9–11].
Recent advances in molecular genetics of thyroid cancer can be applied to develop new diagnostic markers for fine needle aspiration (FNA) samples [12]. PTC frequently carries BRAF and/or RAS mutations as well as RET/PTC rearrangements and some of them are associated with unfavorable outcome [12–16]. BRAF mutation has been associated with more aggressive tumor behavior, such as extrathyroidal extension, lymph node involvement, resistance to radioactive iodine, and tumor recurrence [11, 15–19].
In the present study, we planned to investigate the frequency of somatic mutations of BRAF, HRAS, NRAS and KRAS genes and the rearrangements of RET/PTC1, RET/PTC3 and PAX8/PPAR-gamma both in cancerous and tumor free control thyroid tissues of Hungarian subjects. We also aimed to examine the correlation between the genetic variants and the subtypes of PTC as well as the severity of the disease.
Materials and Methods
Thyroid Tissue Samples
We obtained two types of samples: intraoperative fresh frozen and formalin-fixed paraffin-embedded samples. The intraoperative samples were collected from consecutive patients at the 1st Department of Surgery, Semmelweis University, between 2010 and 2014. The paraffin-embedded tissue blocks were received from the archives of the 2nd Department of Pathology, Semmelweis University as well as the Department of Pathology, University of Szeged and the National Institute of Oncology. Altogether, we examined 394 thyroid tissue samples (197 malignant and 197 control of the same subjects). The histological results were confirmed by two independent pathologist, who selected the tumorous and tumor free place in each samples for further analysis for us. The study protocol was reviewed and approved by the Ethic Committee (ETT-TUKEB 1160–0/2010-1018EKU). Patients gave informed consent.
Nucleic Acid Isolation
The thyroid tissues were stored in −72 °C after surgery until processing or were paraffin-embedded. The first step was comminution in phosphate-buffered saline (PBS) with Fisher Scientific PowerGen 125 tissue grinder (Fisher Scientific GmbH, Germany) when processing the intraoperative tissue samples. Genomic DNA was isolated using Roche High Pure PCR template Preparation Kit (Roche, Indianapolis, IN, USA). Total RNA was separated by Roche High Pure RNA Isolation Kit (Roche) from intraoperative tissue samples. From paraffin-embedded tissue samples, genomic DNA was obtained by Roche High Pure PCR template Preparation Kit (Roche), while total RNA was isolated by Roche High Pure RNA Paraffin Kit (Roche, Indianapolis, IN, USA). Quantification of isolated DNA and RNA was assessed by NanoDrop spectrophotometer (Nanodrop Technologies, Montchanin, DE, USA). DNA and RNA isolation was successful from all samples.
Detection of Point Mutations
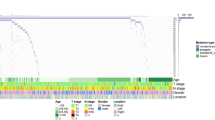
We used a slightly modified protocol described by Nikiforov et al. [12] for the detection of genetic alterations. Briefly, the genomic DNA was tested for BRAF codon 600 (rs113488022), NRAS codon 61 (rs79057879), HRAS codon 61 (rs28933406), KRAS codons 12 and 13 (rs121913535) point mutations using real-time PCR and fluorescence melting curve analysis (Roche Light Cycler 2.0 Instrument, Roche Instrument Center AG, Rotkreuz, Switzerland). Amplification was performed using 20–50 ng of genomic DNA, 40–40 pmol of each primer (TIB MOLBIOL, Berlin, Germany), 2–2 pmol of each hybridization probe (TIB MOLBIOL), 1.5 μl water, 0.5 μl bovine serum albumin (10 mg/ml, Sigma-Aldrich, St. Louis, MO, USA) and 5 μl JumpStartTaq ReadyMix PCR polymerase (Sigma-Aldrich). The reaction mixture was subjected to 60 cycles of PCR amplification consisting of denaturation at 95 °C for 5 s, annealing at 54 °C for 20 s, and extension at 72 °C for 12 s. Post-amplification fluorescence melting curve analysis was performed by gradual heating of samples at a rate of 0.1 °C/s from 45 °C to 95 °C. Fluorescence melting peaks were built by plotting of the negative derivative of fluorescent signal corresponding to the temperature (−dF/dT). The sensitivity of mutation detection by melting curve analysis was 10 % of cells with a mutant allele in the background of normal cells, as established by serial dilutions of the positive controls (Fig. 1).

Melting curve of pathological (a) BRAF mutation (rs113488022), (b) NRAS mutation (rs79057879), (c) HRAS mutation (rs28933406) and mutation negative controls. Expression curves of (d) RET and CCDC6 (RET/PTC1) gene rearrangement in normal and pathological thyroid tissue samples
Detection of Rearrangements
PAX8ex7 and PAX8ex9/PPAR-gamma, RET/PTC1 and RET/PTC3 rearrangements were detected on RNA by RT-PCR ABI Prism 7500 (LT, Foster City, CA, USA) with primers designed to flank the respective point. Reverse transcription was performed using 200 U SuperScriptIII RNase H-reverse transcriptase (Invitrogen Life Technologies, Carlsbad, California, USA), 40 U RNaseOUT Ribonuclease Inhibitor (Invitrogen Life Technologies) and 2 μl random primer (Promega, Madison, WI, USA) and 250–300 ng RNA at 37 °C for 1 h. The PCR reactions were amplified in 20 μl volume using 2 μl cDNA, 10 μl TaqMan 2× Universal PCR Master Mix NoAmpErase UNG (Life Technologies), 40 pmol of each primer, 2 pmol each hybridization TaqMan probe 20× (LT) and 7.5 μl water. Every gene rearrangement was examined in 2–2 parallel measurements in a 96-well plate. The RT-PCR reaction was carried out at 50 °C for 2 min and denaturation at 95 °C for 10 min, followed by 60-cycle PCR amplification: denaturation at 95 °C for 15 s and annealing and extension at 60 °C for 60 s (Fig. 1).
Statistical Analysis
We created three different groups of patients by their clinical and histological data. The relationship between these data and the presence of genetic variants was analyzed. Group A was composed by patients who did not have thyroid cancer metastasis, vascular invasion and the tumor size was 10 mm or less. In group B, tumor metastasis or vascular invasion were not detected and the tumor diameter was more than 10 mm. Group C was composed of patients with metastasis, vascular invasion and the diameter of the nodule was more than 10 mm. We applied Chi-square test with SPSS Statistics 20 program was applied for statistical analysis.
The correlation between the distribution of genetic alterations and the subtypes of PTC was also examined. We applied linear regression test from SPSS Statistic 20 program for statistical evaluation.
Results
The 197 patients with PTC included 63 men (age: 49.9 ± 14.6) and 134 women (age: 47.7 ± 16.2). We found double genetic alterations in 7 cases, and single variants in 92 cancer samples. No genetic alteration of the examined genes was detected in 98 samples. The distribution of genetic variants can be seen in Table 1. The distribution of mutation frequency in subtypes of PTC is shown in Table 2. Altogether, 53.9 % of PTC samples contained one or two genetic alterations (48.8 % mutations and 5.1 % rearrangements). None of the above genetic alterations was identified in the corresponding normal thyroid tissues.
We analyzed mutation and expression changes separately in formalin-fixed paraffin embedded (FFPE) and fresh frozen (FFS) tissues. We could not find significant differences in genetic data in the two sample types.
Correlation was not detected between the genetic data and the severity of the disease in PTC patients. There was a tendency for increased frequency for BRAF mutation in the tall cell variant, however, no significant relationship could be demonstrated between genetic variants and the subtypes of PTC.
Discussion
The most common genetic alterations in PTC are point mutations in the BRAF and RAS genes followed by RET/PTC rearrangements [2]. The demonstration of the occurrence of these changes in PTC has marked conceptual implications for thyroid carcinogenesis as well as clinicopathological significance. These oncogenes might initiate PTC tumorgenesis or, instead, they might occur after the development of a thyroid tumor [20].
The presence of a BRAF mutation may preoperatively predict the behavior of microscopic PTC, suggesting a more aggressive surgical approach [21–23]. The incidence of BRAF mutation in PTC has been reported in 40–45 % of the cases [2, 24, 25]. Reviewing the incidence of genetic alterations in thyroid cancers from different countries, Soares and co-workers [26] reported BRAF mutations in 56 % of the cases. In our study, BRAF mutations were present with similar frequency in PTC tissues while none was seen in the normal thyroid. Similarly to Bernstein and co-workers [27], we found BRAF mutations relatively more frequently (5/7) in tall cell variants of PTC, however, it did not reach significance, perhaps, due to the low number of this subtype present in our study. Two samples of this subtype carried both BRAF and NRAS simultaneously. BRAF mutation frequency found in our microcarcinoma subset is similar to that of shown by Zheng and co-workers [28], who analyzed a large number of cancers and detected BRAF mutations in 40.1 %.
There is evidence that RAS mutations, although more frequent in follicular cancer, are also present in a rather high percentage of PTC, especially in follicular variants and encapsulated forms [2]. The frequency of RAS mutations in PTC is varying, ranging 0–16 % [26, 29]. We could not show high frequency in our Hungarian samples. Our occurrence rate was much lower (4.1 %) than in the US data demonstrating a 10–20 % RAS mutation frequency in PTC samples [11, 12]. In contrast, Di Cristofaro at al. [29, 30] did not find RAS mutations in PTC in a French population.
In our study, we detected RET/PTC rearrangements also with lower frequency than others [25, 26, 31]. While those authors reported a 10–40 % frequency of RET/PTC rearrangements in PTC, we could only show a 5.1 % in our patients. The presence of RET/PTC3 results in a very aggressive growth of papillary cancer [11, 25, 32–34], thus, it carries a prognostic value. Leeman-Neill et al. [35] found higher frequency of RET/PTC (35 %) in 62 post-Chernobyl PTCs samples.
Surprisingly, we did not find PAX8/PPAR-gamma rearrangement in our samples. The frequency of PAX8/PPAR-gamma rearrangement in PTC remains controversial. Armstrong at al. [36] reported PAX8/PPAR-gamma rearrangement in the follicular variant of PTC with low frequency (1–5 %). However, a much higher prevalence of PAX8/PPAR-gamma rearrangement (37 %) was reported in the follicular variant by Castro et al. [37]. Klemke et al. [38] and Soares at al. [26] reported that this type of genetic alteration could not be found in theirs samples. Eszlinger et al. [39] investigated 310 FNA samples and they found PAX8/PPAR-gamma rearrangement in 8 of 310 samples and only 4 were associated with cancer. The observed geographical difference in the occurrence of this rearrangement needs further investigations.
According to some authors, a correlation appears to exist between the genetic alterations, especially BRAF mutations and the severity of the disease in PTC patients [23, 40–44]. However, others could not corroborate these findings, and the BRAF status did not seem to affect the metastatic behavior of PTC and – according to these authors - it should not be considered as a negative determinant in predicting patients outcome [34, 41, 45–50]. Our data support this latter notion since we could show no effect of genetic alterations including BRAF status on disease severity.
The different frequency of genetic variants in our study compared to others might be due to the different iodine intake in Hungary. The US is a high iodine intake area in contrast to Europe including Hungary which is known of low dietary iodine intake of the population [51–53]. Guan et al. [24] reported, that high iodine intake seems to be a significant risk factor for the occurrence of BRAF mutation in the thyroid gland and may therefore be a risk factor for the development of PTC in Chinese population. In Austria, the change in iodine supply over the last 40 years led to a change in histologic type of thyroid cancer, i.e. the ration of papillary cancer increased [54]. The geographic differences in the incidence of thyroid carcinomas are – at least partly - related to the variations in dietary iodine intake [2, 3, 55]. In an earlier study, the relationship between iodine intake and oncogene RAS mutations in thyroid cancer was examined by a Canadian and a Hungarian research group. The comparison between one of the highest (Canada) and lowest (Hungary) dietary iodine intake area could not identify any RAS mutations in 22 specimens with PTC histology [5]. Another study from Serbia [34], also known as a similarly low iodine intake area as Hungary, found similarly low RAS mutation frequency in PTC as we did in our samples.
It is evident that numerous molecular, clinical and pathological features of PTC have changed over the last decades [2], including a range of genetic alterations in various subpopulations and their role in the disease prognosis. The BRAF and RAS mutation panel is expected to determine the therapeutic treatment of papillary thyroid cancer soon. In addition, local differences, such as iodine intake, may also influence the occurrence of genetic variants in PTC which should be taken into account when evaluating their importance. Our Hungarian data add to the variety of knowledge of this area.
Abbreviations
- BRAF :
-
v-raf murine sarcoma viral oncogene homolog B1
- EGFR:
-
Epidermal growth factor receptor
- FNA:
-
Fine needle aspiration
- FNAB:
-
Fine needle aspiration biopsy
- FVPTC:
-
Follicular variant papillary carcinoma
- HRAS :
-
v-Ha-ras Harvey rat sarcoma viral oncogene homolog
- KRAS :
-
v-Ki-ras2 Kirsten rat sarcoma viral oncogene homolog
- MAPK:
-
Mitogen-activated protein kinase
- PAX8/PPAR-gamma:
-
Paired box8/peroxisome proliferator-activated receptor gamma
- PTC:
-
Papillary thyroid carcinoma
- PTMC:
-
Papillary thyroid microcarcinoma
- RAS:
-
Rat sarcoma viral oncogene homolog
- RET/PTC :
-
RET tyrosine-kinase proto-oncogene/papillary thyroid carcinoma
References
Benvenga S (2008) Update on thyroid cancer. Horm Metab Res 40(5):323–328. doi:10.1055/s-2008-1073155
Elisei R (2014) Molecular profiles of papillary thyroid tumors have been changing in the last decades: how could we explain it? J Clin Endocrinol Metab 99(2):412–414. doi:10.1210/jc.2014-1130
Lakatos P, Takacs I (2007) Pajzsmirigybetegsegek: a gyakorlat oldalarol. Budapest
Woodruff SL, Arowolo OA, Akute OO, Afolabi AO, Nwariaku F (2010) Global variation in the pattern of differentiated thyroid cancer. Am J Surg 200(4):462–466. doi:10.1016/j.amjsurg.2010.03.009
Shi YF, Zou MJ, Schmidt H, Juhasz F, Stensky V, Robb D, Farid NR (1991) High rates of ras codon 61 mutation in thyroid tumors in an iodide-deficient area. Cancer Res 51(10):2690–2693
Vanderpump MP, Lazarus JH, Smyth PP, Laurberg P, Holder RL, Boelaert K, Franklyn JA (2011) Iodine status of UK schoolgirls: a cross-sectional survey. Lancet 377(9782):2007–2012. doi:10.1016/S0140-6736(11)60693-4
Szybinski Z (2009) Iodine prophylaxis in Poland in light of the WHO recommendation on reduction of the daily salt intake. Pediatr Endocrinol Diabetes Metab 15(2):103–107
Moreno-Reyes R, Van Oyen H, Vandevijvere S (2011) Optimization of iodine intake in Belgium. Ann Endocrinol (Paris) 72(2):158–161. doi:10.1016/j.ando.2011.03.021
Schlumberger M (2007) Papillary and follicular thyroid carcinoma. Ann Endocrinol (Paris) 68(2–3):120–128. doi:10.1016/j.ando.2007.04.004
Cheng SP, Liu CL, Tzen CY, Yang TL, Jeng KS, Liu TP, Lee JJ (2008) Characteristics of well-differentiated thyroid cancer associated with multinodular goiter. Langenbeck's Arch Surg 393(5):729–732. doi:10.1007/s00423-008-0327-1
Nikiforov YE, Nikiforova MN (2011) Molecular genetics and diagnosis of thyroid cancer. Nat Rev Endocrinol 7(10):569–580. doi:10.1038/nrendo.2011.142
Nikiforov YE, Steward DL, Robinson-Smith TM, Haugen BR, Klopper JP, Zhu Z, Fagin JA, Falciglia M, Weber K, Nikiforova MN (2009) Molecular testing for mutations in improving the fine-needle aspiration diagnosis of thyroid nodules. J Clin Endocrinol Metab 94(6):2092–2098. doi:10.1210/jc.2009-0247
Adeniran AJ, Zhu Z, Gandhi M, Steward DL, Fidler JP, Giordano TJ, Biddinger PW, Nikiforov YE (2006) Correlation between genetic alterations and microscopic features, clinical manifestations, and prognostic characteristics of thyroid papillary carcinomas. Am J Surg Pathol 30(2):216–222
Kimura ET, Nikiforova MN, Zhu Z, Knauf JA, Nikiforov YE, Fagin JA (2003) High prevalence of BRAF mutations in thyroid cancer: genetic evidence for constitutive activation of the RET/PTC-RAS-BRAF signaling pathway in papillary thyroid carcinoma. Cancer Res 63(7):1454–1457
Xing M (2007) BRAF mutation in papillary thyroid cancer: pathogenic role, molecular bases, and clinical implications. Endocr Rev 28(7):742–762. doi:10.1210/er.2007-0007
Paulson L, Shindo M, Schuff K, Corless C (2012) The role of molecular markers and tumor histological type in central lymph node metastasis of papillary thyroid carcinoma. Arch Otolaryngol Head Neck Surg 138(1):44–49. doi:10.1001/archoto.2011.226
Basolo F, Torregrossa L, Giannini R, Miccoli M, Lupi C, Sensi E, Berti P, Elisei R, Vitti P, Baggiani A, Miccoli P (2010) Correlation between the BRAF V600E mutation and tumor invasiveness in papillary thyroid carcinomas smaller than 20 millimeters: analysis of 1060 cases. J Clin Endocrinol Metab 95(9):4197–4205. doi:10.1210/jc.2010-0337
Lee JH, Lee ES, Kim YS (2007) Clinicopathologic significance of BRAF V600E mutation in papillary carcinomas of the thyroid: a meta-analysis. Cancer 110(1):38–46. doi:10.1002/cncr.22754
Adeniran AJ, Theoharis C, Hui P, Prasad ML, Hammers L, Carling T, Udelsman R, Chhieng DC (2011) Reflex BRAF testing in thyroid fine-needle aspiration biopsy with equivocal and positive interpretation: a prospective study. Thyroid 21(7):717–723. doi:10.1089/thy.2011.0021
Guerra A, Zeppa P, Bifulco M, Vitale M (2014) Concomitant BRAF(V600E) mutation and RET/PTC rearrangement is a frequent occurrence in papillary thyroid carcinoma. Thyroid 24(2):254–259. doi:10.1089/thy.2013.0235
Rossi ED, Martini M, Capodimonti S, Lombardi CP, Pontecorvi A, Vellone VG, Zannoni GF, Larocca LM, Fadda G (2013) BRAF (V600E) mutation analysis on liquid-based cytology-processed aspiration biopsies predicts bilaterality and lymph node involvement in papillary thyroid microcarcinoma. Cancer Cytopathology 121(6):291–297. doi:10.1002/cncy.21258
Bellevicine C, Cozzolino I, Malapelle U, Zeppa P, Troncone G (2012) Cytological and molecular features of papillary thyroid carcinoma with prominent hobnail features: a case report. Acta Cytol 56(5):560–564. doi:10.1159/000338395
Xing M, Clark D, Guan H, Ji M, Dackiw A, Carson KA, Kim M, Tufaro A, Ladenson P, Zeiger M, Tufano R (2009) BRAF mutation testing of thyroid fine-needle aspiration biopsy specimens for preoperative risk stratification in papillary thyroid cancer. J Clin Oncol 27(18):2977–2982. doi:10.1200/JCO.2008.20.1426
Guan H, Ji M, Bao R, Yu H, Wang Y, Hou P, Zhang Y, Shan Z, Teng W, Xing M (2009) Association of high iodine intake with the T1799A BRAF mutation in papillary thyroid cancer. J Clin Endocrinol Metab 94(5):1612–1617. doi:10.1210/jc.2008-2390
Gandhi M, Evdokimova V, Nikiforov YE (2010) Mechanisms of chromosomal rearrangements in solid tumors: the model of papillary thyroid carcinoma. Mol Cell Endocrinol 321(1):36–43. doi:10.1016/j.mce.2009.09.013
Soares P, Celestino R, Gaspar da Rocha A, Sobrinho-Simoes M (2014) Papillary thyroid microcarcinoma: how to diagnose and manage this epidemic? Int J Surg Pathol 22(2):113–119. doi:10.1177/1066896913517394
Bernstein J, Virk RK, Hui P, Prasad A, Westra WH, Tallini G, Adeniran AJ, Udelsman R, Sasaki CT, Roman SA, Sosa JA, Prasad ML (2013) Tall cell variant of papillary thyroid microcarcinoma: clinicopathologic features with BRAF(V600E) mutational analysis. Thyroid 23(12):1525–1531. doi:10.1089/thy.2013.0154
Zheng X, Wei S, Han Y, Li Y, Yu Y, Yun X, Ren X, Gao M (2013) Papillary microcarcinoma of the thyroid: clinical characteristics and BRAF(V600E) mutational status of 977 cases. Ann Surg Oncol 20(7):2266–2273. doi:10.1245/s10434-012-2851-z
Zou M, Baitei EY, Alzahrani AS, BinHumaid FS, Alkhafaji D, Al-Rijjal RA, Meyer BF, Shi Y (2014) Concomitant RAS, RET/PTC, or BRAF Mutations in Advanced Stage of Papillary Thyroid Carcinoma. Thyroid 24(8):1256–1266. doi:10.1089/thy.2013.0610
Di Cristofaro J, Marcy M, Vasko V, Sebag F, Fakhry N, Wynford-Thomas D, De Micco C (2006) Molecular genetic study comparing follicular variant versus classic papillary thyroid carcinomas: association of N-ras mutation in codon 61 with follicular variant. Hum Pathol 37(7):824–830. doi:10.1016/j.humpath.2006.01.030
Nikiforov YE (2002) RET/PTC rearrangement in thyroid tumors. Endocr Pathol 13(1):3–16
Szántó Z, Zoltán KI (2008) A pajzsmirigy cancerogenesisében szereplő oncogének, antioncogének és egyéb tumormarkerek diagnosztikai és prognosztikai jelentősége. Orvostudományi Értesítő 81(1):9–12
Nikiforova MN, Nikiforov YE (2008) Molecular genetics of thyroid cancer: implications for diagnosis, treatment and prognosis. Expert Rev Mol Diagn 8(1):83–95. doi:10.1586/14737159.8.1.83
Stanojevic B, Dzodic R, Saenko V, Milovanovic Z, Pupic G, Zivkovic O, Markovic I, Djurisic I, Buta M, Dimitrijevic B, Rogounovitch T, Mitsutake N, Mine M, Shibata Y, Nakashima M, Yamashita S (2011) Mutational and clinico-pathological analysis of papillary thyroid carcinoma in Serbia. Endocr J 58(5):381–393
Leeman-Neill RJ, Brenner AV, Little MP, Bogdanova TI, Hatch M, Zurnadzy LY, Mabuchi K, Tronko MD, Nikiforov YE (2013) RET/PTC and PAX8/PPARgamma chromosomal rearrangements in post-Chernobyl thyroid cancer and their association with iodine-131 radiation dose and other characteristics. Cancer 119(10):1792–1799. doi:10.1002/cncr.27893
Armstrong MJ, Yang H, Yip L, Ohori NP, McCoy KL, Stang MT, Hodak SP, Nikiforova MN, Carty SE, Nikiforov YE (2014) PAX8/PPARgamma Rearrangement in Thyroid Nodules Predicts Follicular-Pattern Carcinomas, in Particular the Encapsulated Follicular Variant of Papillary Carcinoma. Thyroid. doi:10.1089/thy.2014.0067
Castro P, Rebocho AP, Soares RJ, Magalhaes J, Roque L, Trovisco V, Vieira de Castro I, Cardoso-de-Oliveira M, Fonseca E, Soares P, Sobrinho-Simoes M (2006) PAX8-PPARgamma rearrangement is frequently detected in the follicular variant of papillary thyroid carcinoma. J Clin Endocrinol Metab 91(1):213–220. doi:10.1210/jcem.91.1.9999
Klemke M, Drieschner N, Belge G, Burchardt K, Junker K, Bullerdiek J (2012) Detection of PAX8-PPARG fusion transcripts in archival thyroid carcinoma samples by conventional RT-PCR. Genes Chromosom Cancer 51(4):402–408. doi:10.1002/gcc.21925
Eszlinger M, Krogdahl A, Munz S, Rehfeld C, Precht Jensen EM, Ferraz C, Bosenberg E, Drieschner N, Scholz M, Hegedus L, Paschke R (2014) Impact of molecular screening for point mutations and rearrangements in routine air-dried fine-needle aspiration samples of thyroid nodules. Thyroid 24(2):305–313. doi:10.1089/thy.2013.0278
Nikiforova MN, Kimura ET, Gandhi M, Biddinger PW, Knauf JA, Basolo F, Zhu Z, Giannini R, Salvatore G, Fusco A, Santoro M, Fagin JA, Nikiforov YE (2003) BRAF mutations in thyroid tumors are restricted to papillary carcinomas and anaplastic or poorly differentiated carcinomas arising from papillary carcinomas. J Clin Endocrinol Metab 88(11):5399–5404. doi:10.1210/jc.2003-030838
Gandolfi G, Sancisi V, Torricelli F, Ragazzi M, Frasoldati A, Piana S, Ciarrocchi A (2013) Allele percentage of the BRAF V600E mutation in papillary thyroid carcinomas and corresponding lymph node metastases: no evidence for a role in tumor progression. J Clin Endocrinol Metab 98(5):E934–E942. doi:10.1210/jc.2012-3930
Xing M, Haugen BR, Schlumberger M (2013) Progress in molecular-based management of differentiated thyroid cancer. Lancet 381(9871):1058–1069. doi:10.1016/S0140-6736(13)60109-9
Guerra A, Fugazzola L, Marotta V, Cirillo M, Rossi S, Cirello V, Forno I, Moccia T, Budillon A, Vitale M (2012) A high percentage of BRAFV600E alleles in papillary thyroid carcinoma predicts a poorer outcome. J Clin Endocrinol Metab 97(7):2333–2340. doi:10.1210/jc.2011-3106
Fugazzola L, Puxeddu E, Avenia N, Romei C, Cirello V, Cavaliere A, Faviana P, Mannavola D, Moretti S, Rossi S, Sculli M, Bottici V, Beck-Peccoz P, Pacini F, Pinchera A, Santeusanio F, Elisei R (2006) Correlation between B-RAF(V600E) mutation and clinico-pathologic parameters in papillary thyroid carcinoma: data from a multicentric Italian study and review of the literature. Endocr Relat Cancer 13(2):455–464
Trovisco V, Soares P, Preto A, de Castro IV, Lima J, Castro P, Maximo V, Botelho T, Moreira S, Meireles AM, Magalhaes J, Abrosimov A, Cameselle-Teijeiro J, Sobrinho-Simoes M (2005) Type and prevalence of BRAF mutations are closely associated with papillary thyroid carcinoma histotype and patients' age but not with tumour aggressiveness. Virchows Archiv Int J Pathol 446(6):589–595. doi:10.1007/s00428-005-1236-0
Fugazzola L, Puxeddu E, Avenia N, Romei C, Cirello V, Cavaliere A, Faviana P, Mannavola D, Moretti S, Rossi S, Sculli M, Bottici V, Beck-Peccoz P, Pacini F, Pinchera A, Santeusanio F, Elisei R (2006) Correlation between B-RAFV600E mutation and clinico-pathologic parameters in papillary thyroid carcinoma: data from a multicentric Italian study and review of the literature. Endocr Relat Cancer 13(2):455–464. doi:10.1677/erc.1.01086
Eszlinger M, Niedziela M, Typlt E, Jaeschke H, Huth S, Schaarschmidt J, Aigner T, Trejster E, Krohn K, Bosenberg E, Paschke R (2014) Somatic mutations in 33 benign and malignant hot thyroid nodules in children and adolescents. Mol Cell Endocrinol 393(1–2):39–45. doi:10.1016/j.mce.2014.05.023
Czarniecka A, Rusinek D, Stobiecka E, Krajewska J, Kowal M, Kropinska A, Zebracka J, Kowalska M, Wloch J, Maciejewski A, Handkiewicz-Junak D (2010) Occurrence of BRAF mutations in a Polish cohort of PTC patients - preliminary results. Endokrynol Pol 61(5):462–466
Goutas N, Vlachodimitropoulos D, Bouka M, Lazaris AC, Nasioulas G, Gazouli M (2008) BRAF and K-RAS mutation in a Greek papillary and medullary thyroid carcinoma cohort. Anticancer Res 28(1A):305–308
Givens DJ, Buchmann LO, Agarwal AM, Grimmer JF, Hunt JP (2014) BRAF V600E does not predict aggressive features of pediatric papillary thyroid carcinoma. Laryngoscope 124(9):E389–E393. doi:10.1002/lary.24668
Boric M, Stanicic J, Dabelic N, Jukic T, Kusic Z (2009) Iodine supplementation in pregnancy. Acta clinica Croatica 48(4):469–473
Goretzki PE, Witte J, Dotzenrath C, Schulte KM, Simon D, Roher HD (1998) Geographical differences of thyroid carcinoma and basic molecular principles. Langenbecks Arch Chir Suppl Kongressbd 115:200–202
Fleury Y, van Melle G, Woringer V, Temler E, Gaillard RC, Portmann L (1999) Iodine nutrition and prevalence of goiter in adolescents in the Canton of Vaud. Schweiz Med Wochenschr 129(47):1831–1838
Lind P, Kumnig G, Heinisch M, Igerc I, Mikosch P, Gallowitsch HJ, Kresnik E, Gomez I, Unterweger O, Aigner H (2002) Iodine supplementation in Austria: methods and results. Thyroid 12(10):903–907. doi:10.1089/105072502761016539
Guo HQ, Zhao H, Zhang ZH, Zhu YL, Xiao T, Pan QJ (2014) Impact of molecular testing in the diagnosis of thyroid fine needle aspiration cytology: data from mainland China. Dis Markers 2014:912182. doi:10.1155/2014/912182
Acknowledgments
The study was supported in part by the Hungarian Health Research Council (ETT-10-151/2009) as well as Osseus Foundation. We also thank Violetta Kalocsáné Piurkó for the preparation of paraffin-embedded samples.
Author information
Authors and Affiliations
Corresponding author
Additional information
Bálint Tobiás and Csaba Halászlaki equally contributed to this work.
Rights and permissions
About this article

Cite this article
Tobiás, B., Halászlaki, C., Balla, B. et al. Genetic Alterations in Hungarian Patients with Papillary Thyroid Cancer. Pathol. Oncol. Res. 22, 27–33 (2016). https://doi.org/10.1007/s12253-015-9969-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12253-015-9969-9