
Abstract
Hepatitis B surface antigen (HBsAg) loss is an ideal treatment endpoint for patients with chronic hepatitis B (CHB). We investigated the predictive value of on-treatment HBsAg levels for HBsAg loss in hepatitis B e antigen (HBeAg)-negative CHB patients who received 120-week PEG-IFNα-2a treatment. Serum HBV DNA, HBsAg, and anti-HBs levels were assayed at baseline and every 3 months during the treatment. Of 81 patients, 12 achieved HBsAg loss, 20 achieved HBsAg < 100 IU/mL, and 49 maintained HBsAg ≥ 100 IU/mL. HBsAg loss rate was only 3.7% at 48 weeks, while it reached to 11.1% and 14.8% after treatment of 96 weeks and 120 weeks. The cutoff HBsAg levels at 12 weeks predicting HBsAg loss at 96 weeks and 120 weeks of treatment were 400 IU/mL and 750 IU/mL, with AUC 0.725 and 0.722, positive predictive value (PPV) 29.41% and 30.56%, and negative predictive value (NPV) 93.75% and 97.78%, respectively. The cutoff HBsAg levels at 24 weeks predicting HBsAg loss at 96 weeks and 120 weeks of treatment were 174 IU/mL and 236 IU/mL respectively, with AUC 0.925 and 0.922, PPV 40.0% and 46.15%, and both NPV 100%. The predictive ability of the cutoff HBsAg levels at 24 weeks was better than that at 12 weeks for HBsAg loss at either 96 or 120 weeks (χ2 = 3.880, P = 0.049 and χ2 = 4.412, P = 0.036). These results indicate that extended therapy is critical to HBsAg loss in HBeAg-negative CHB patients during PEG-IFN treatment, and the HBsAg level at 24 weeks can be used to predict HBsAg loss during tailoring PEG-IFN therapy.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Hepatitis B virus (HBV) replication and detectable serum HBV DNA are closely associated with the progression of liver disease, liver decompensation, and occurrence of liver cirrhosis and hepatocellular carcinoma in patients with chronic hepatitis B (CHB) (Chen et al. 2006; Seto et al. 2018). Antiviral therapy is the most important and effective treatment to slow disease progression and reduce mortality associated with liver disease (Hui and Lau 2006; WHO 2017). Antiviral therapy enables CHB patients to improve long-term outcomes by maintaining HBV replication and hepatitis B surface antigen (HBsAg) at low levels and achieving HBsAg loss/seroconversion. Interferon (IFN) exerts direct antiviral and immunoregulatory activities (Li et al. 2017; Mak et al. 2019), which serve to inhibit HBV replication, eliminate virus-infected cells by specific and non-specific immunities to HBV (Koffas et al. 2018), clear covalently closed circular DNA (cccDNA) in liver, and reduce HBsAg levels (Gill et al. 2011).
Some studies have examined the efficacy of indicators for predicting effects of antiviral therapy or sustained viral response after treatment (Marcellin et al. 2009; Chan et al. 2011b). HBsAg is a unique parameter which determines drug withdrawal in HBeAg-negative patients after antiviral treatment, and an ideal endpoint of antiviral therapy for HBeAg-positive and HBeAg-negative CHB (Terrault et al. 2018). Many studies have demonstrated a correlation between serum HBsAg levels and cccDNA content in liver (Chan et al. 2007; Giersch et al. 2017). HBsAg levels can thus be used to differentiate HBeAg negative CHB and inactive carriers (Brunetto et al. 2010), and to predict response in patients receiving PEG-IFN therapy (Sonneveld et al. 2013). Serum HBsAg levels have been found to be significantly lower in inactive HBsAg carriers compared with patients with active liver inflammation (Chan et al. 2010; Cornberg et al. 2017), so serum HBsAg level is regarded as an important indicator of active liver inflammation (Manesis et al. 2010; Liu et al. 2016; Xie et al. 2019). HBsAg loss is also indicative of good long-term outcome in CHB patients (Terrault et al. 2018). HBsAg loss reflects the extent of infected-cell clearance and the immune control of HBV. However, in HBeAg-negative patients received treatment of 180 μg/week pegylated interferon α-2a (PEG-IFNα-2a) injection plus lamivudine or 180 μg/week PEG-IFNα-2a alone for 48 weeks, HBsAg loss only occurred in 3% and 5% patients at 6 months, though it increased to 8% after 3 years of follow-up (Marcellin et al. 2009). The incidence of HBsAg loss under standard PEG-IFNα-2a therapy is unsatisfactory. It was reported that the HBsAg response on early treatment could predict HBsAg loss after add-on or switch to PEG-IFNα-2a therapy in patients on nucleoside (acid) analogues (NA) therapy (Ning et al. 2014; Li et al. 2015). Therefore, it’s of great importance to develop new approaches for predicting the HBsAg loss in patients treated with antiviral agents. To our knowledge, there are few reports on how to predict HBsAg loss in naive HBeAg-negative CHB during PEG-IFNα-2a treatment. In this study, we investigated dynamic changes in HBsAg levels during PEG-IFNα-2a treatment and assessed the capability of early serum HBsAg kinetics for predicting HBsAg loss in patients with HBeAg-negative CHB.
Materials and Methods
Patients and Treatment
This prospective study enrolled 91 antiviral naïve HBeAg-negative patients with CHB who were treated in Department of Hepatology Division 2, Beijing Ditan Hospital from May 2013 to May 2016. The patients with HBeAg-negative CHB were enrolled according the inclusion and exclusion criteria (Table 1). Enrolled patients received weekly subcutaneous injections of 180 μg PEG-IFNα-2a for tailoring course. The total course of treatment should not exceed 120 weeks. Treatment would be stopped if HBsAg loss with undetectable serum HBV DNA occurred and confirmed by twice test with an interval of 12 weeks. The patients with sustained HBsAg level decrease during treatment would be continually treated up to 120 weeks, and treatment would be discontinued if HBsAg level was not decreased as compared to the previous 6 months. The use of other immunosuppressive, regulatory, and/or antiviral drugs was prohibited during PEG-IFNα-2a treatment. Patients who discontinued PEG-IFNα-2a treatment would be on survey during study period. However, patients should receive treatment of entecavir (ETV) if they had hepatitis relapse after stopping PEG-IFNα-2a treatment, defined as HBV DNA load ≥ 2000 IU/mL and alanine aminotransferase (ALT) level > 40 U/L.
Laboratory Measurements
HBV DNA load and serological markers (HBsAg, HBeAg, and anti-HBe), liver function, renal function, blood glucose, alpha fetoprotein (AFP) and blood count were tested at baseline and every 3 months during PEG-IFNα-2a treatment. Liver fibrosis scan (FibroScan 502, EchosensTM, Paris, France), ultrasound (Acuson Sequoia, Siemens, Erlangen, Germany) or CT (Computed Tomography System, LightSpeed VCT, LightSpeed Pro32, Tokyo, Japan) imaging examination were performed at baseline and every 6 months. Anti-HBs was tested in patients who achieved HBsAg loss.
Liver function, renal function, blood sugar, and blood lipids were detected by Hitachi 7600 fully automatic biochemical analyzer (Wako Pure Chemical Industries, Ltd., Tokyo, Japan). Blood routine was examined using automatic blood cell analyzer (COURTER LH755, California, USA). HBV DNA load was detected by CobasTaqMan96 real-time quantitative PCR detection reagent (detection of off-line < 20 IU/mL) (Roche, Pleasanton, CA, USA). HBsAg, anti-HBs, and HBeAg were detected using Abbott Architect i2000 kits (Abbott Laboratories, Abbott Park, IL, USA). Serum HBsAg levels were determined by Abbott Architect HBsAg QT assay (range: 0.05–250 IU/mL). Samples were finally diluted 1:1000 with the Architect HBsAg diluent to expand the upper limit of the dynamic range from 250 to 250,000 IU/mL. HBsAg loss was defined as an HBsAg level < 0.05 IU/mL. Anti-HBs levels were measured using an Architect i2000 kit (Abbott Laboratories), with a range of 0.00–1000 mIU/L. Anti-HBs levels ≥ 10 mIU/L is considered positive.
Efficacy Endpoints
The primary endpoint was HBsAg loss/seroconversion during treatment. The secondary endpoints included HBsAg decline, compared with baseline, and undetectable HBV DNA after treatment.
Drug Safety
Kidney function, and peripheral blood neutrophil and platelet counts were determined before treatment and every 1–3 months. Parameter of thyroid function, and anti-thyroglobulin and thyroid peroxidase antibodies were monitored every 3 months during treatment.
Statistical Analysis
Continuous variables were expressed as mean ± standard deviation or median (range), as appropriate. HBV DNA (IU/mL) and HBsAg (IU/mL) were logarithmically transformed for analysis. For patients with negative HBsAg levels, the results were taken as the lower limit of detection (0.05 IU/mL for HBsAg) for the purposes of calculation. To investigate factors associated with HBsAg seroclearance, continuous variables including HBV DNA and HBsAg were compared by Mann–Whitney U tests, and categorical variables were analyzed using Fisher’s exact tests. The area under the receiver operating characteristic (ROC) curve was used to analyze the predictive value of HBsAg kinetics for HBsAg seroclearance, and the best cut-off value was determined from the coordinates of the ROC curve. All statistical tests were two-sided. Statistical significance was taken as P < 0.05. Statistical analysis was performed using SPSS statistical software version 13.0 (Chicago, IL, USA).
Results
Population and Response
Among the 91 patients enrolled at the beginning, 3 patients withdrew before 12 weeks of treatment because of side effects of PEG-IFNα-2a, 5 patients lost continuous follow-up observation, and 2 patients withdrew because of unexpected pregnancy. So 81 patients were included in the study for analysis in the end (Fig. 1).

Flow diagram of patient enrollment, allocation, treatment, and follow-up. CDT, cumulative discontinuation of treatment.
Serum HBsAg levels decreased continually during treatment. Patients were grouped as complete response, partial response, and poor response according to their HBsAg level reached loss < 100 IU/mL or not during PEG-IFNα-2a treatment (Chan et al. 2011a, b). There were 12 (14.81%) patients who achieved HBsAg loss and undetectable HBV DNA [considered as the complete-response group (group 1)], 20 (24.69%) patients had HBsAg positive but < 100 IU/mL [defined as the partial-response group (group 2)], and 49 patients had HBsAg level ≥ 100 IU/mL [defined as the poor-response group (group 3)]. The demographics and baseline clinical characteristics in three groups are shown in Table 2. No patient developed decomposition of liver function and hepatic cell carcinoma during study period. No hepatitis relapse occurred in patients of group 1 and group 2, but eight patients in poor response group had hepatitis relapse after PEG-IFN treatment was discontinued and received ETV therapy.
HBV DNA Level
All patients in completed response group, 90.0% (2/20) of patients in partial response group, and 75.5% (37/49) of patients in poor response group, archived undetectable HBV DNA levels at 36 weeks (Fig. 2). Among total patients, there were 95.06% (77/81) achieved HBV DNA negative conversion at 48 weeks. In complete response group, all patients maintained undetectable HBV DNA level during the study period.

Rates of patients obtained undetectable HBV DNA level in HBsAg poor-, partial-, and complete-response groups, which was 100% in complete-response group at 36 weeks after treatment.
HBsAg Kinetics
After 12-week treatment, the decline of HBsAg levels from baseline were 0.534 ± 0.559, 0.386 ± 0.644, and 0.053 ± 0.316 log10IU/mL in group 1, group 2, and group 3, respectively. After adjustment for differences at baseline, the degree of HBsAg decline was significantly higher in groups 1 and 2 than in group 3 (F = 11.39, P < 0.0001). After treatment of 24 weeks, the degree of HBsAg decline became significant different among three groups (F = 30.30, P < 0.0001), and the magnitude of deviation enlarged during subsequent treatment. HBsAg level in group 1 continued to decrease through the treatment course; however, the decline reached a plateau after 72 weeks in groups 2 and 3 (Fig. 3).

Dynamic changes of serum HBsAg levels in different patient groups during 120-weeks. HBsAg level declined slightly in poor response patients, in the partial-response group those declined continually early treatment time but reached a plateau after 72 weeks, and in complete response group those decreased sustainably.
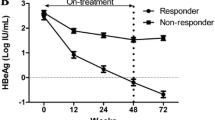
Among 12 patients who achieved HBsAg loss, 11 patients obtained HBsAg < 100 IU/mL at 48 weeks. 41.66% (5/12) of HBsAg loss occurred within 72 weeks after treatment, and 58.33% occurred between 72 and 120 weeks (Fig. 4). During the 48-week standard PEG-IFN treatment, HBsAg loss rate was only 3.7%, while it reached to 6.2%, 11.1% and 14.8% when the treatment was extended to 72, 96, and 120 weeks, respectively.

HBsAg loss following different time of PEG-IFNα-2a treatment. Rate of HBsAg loss increased by extended PEG-IFN treatment (A). Most HBsAg loss occurred between 72 weeks and 120 weeks after treatment (B).
Prediction of HBsAg Loss During Treatment
The cut-off value for HBsAg levels at 12 weeks predicting HBsAg loss at 96 weeks and at 120 weeks was 400 IU/mL and 750 IU/mL respectively, while the cutoff value at 24 weeks predicting HBsAg loss at 96 weeks and at 120 weeks were 174 IU/mL and 236 IU/mL. To predict HBsAg loss at 96 weeks, the area under the ROC curve (AUC) of 24 weeks was 0.925 (95% CI, 0.853–0.990), and that of 12 weeks was 0.725 (95% CI, 0.505–0.940). For predicting HBsAg loss at 120 weeks, the AUC of 24 weeks was 0.922 (95% CI, 0.853–0.984), and that of 12 weeks was 0.722 (95% CI, 0.547–0.888). The predictive abilities at 24 weeks were thus stronger than those at 12 weeks to predict for HBsAg loss at both 96 and 120 weeks (χ2 = 3.880, P = 0.049 and χ2 = 4.412, P = 0.036, respectively) (Fig. 5).

Predictive abilities of HBsAg level at 12 weeks and 24 weeks for HBsAg loss during PEG-IFN treatment. Regardless of predicting HBsAg loss occurred during the treatment of 96 weeks (A) or HBsAg loss occurred within 120 weeks (B) after treatment, the cutoff value of HBsAg levels at 12 weeks had lower AUC and NPV than the cutoff value of HBsAg levels at 24 weeks.
Safety
It’s reported that 58 patients (71.6%) had influenza-like syndrome, and 56 patients (69.1%) had neutrophils decrease which reached abnormal levels (< 2 × 109/L) in 21 patients. Platelet counts decrease occurred in 55 cases (67.9%), and it reached lower than the low detection limit (< 100 × 109/L) in 32 patients. Abnormal thyroid function was observed in three patients, of whom two developed hyperthyroidism and one developed thyroid hypofunction; but all recovered at the end of PEG-IFN therapy after specific treatments. However, drug doses were not necessarily adjusted in patients with decreased neutrophil and/or platelet counts, or in those with thyroid dysfunctions. Serum creatinine and urea nitrogen levels remained normal throughout treatment in all patients.
Discussion
Most of HBeAg-negative CHB patients develop obvious liver inflammation (Hadziyannis and Papatheodoridis 2006), and rarely achieve spontaneous remission (Chu et al. 2002; Li et al. 2019). Around 29%–38% of patients with HBeAg-negative CHB are at stage of cirrhosis at the time of their first diagnosis (Yim and Lok 2006). Due to high rate of hepatitis relapse after drug withdrawal and no defined criteria for stopping treatment, most patients need long-term antiviral treatment with NA to maintain the inhibition of HBV replication (Papatheodoridis 2011).
Compared with NA therapy, PEG-IFN treatment has higher sustained viral response in CHB patients, and some patients can achieve HBsAg loss (Lau et al. 2005; Lampertico et al. 2013). PEG-IFNα-2a is recommended as the first line drug for antiviral therapy in CHB patients regardless of its side effects (Chinese Society of Infectious Diseases 2019; EASL 2017; Terrault et al. 2018), while only 20%–30% of HBeAg-negative patients obtained a sustained viral response after standard antiviral therapy with PEG-IFNα-2a at 180 μg/week for 48 weeks (Rijckborst et al. 2010). Sustained viral response rate was 11.8% of genotype-D HBV-infected naïve patients treated 48 weeks of PEG-IFNα-2a at 180 μg/week injection, and it increased to 28.8% by extending treatment to 96 weeks, and the HBsAg loss rate increased from 0 to 5.8% at 96 weeks (Lampertico et al. 2013). PEG-IFNα-2a combined with lamivudine treatment failed to increase the efficacy (Marcellin et al. 2009). In NA-experienced patients who switch to PEG-IFNα-2a, 16.8% patients achieved HBsAg loss at the end of 48 weeks treatment, and the rate of HBsAg loss increased to 24.1% when treatment time was extended to 96 weeks (Hu et al. 2018). Therefore, in our study, all patients received PEG-IFNα-2a injection alone and the treatment was extended to increase the rate of HBsAg loss. We found that 14.81% of HBeAg-negative CHB obtained HBsAg loss after tailoring course of PEG-IFN treatment. The rate of HBsAg loss (14.81%) is higher than the ones previously reported in HBeAg-positive CHB patients (3.0%) and HBeAg-negative CHB patients (3.3%) who received standard of 48 week PEG-IFNα-2a treatment (Lau et al. 2005; Marcellin et al. 2004). In this study, only 3 of 81 patient achieved HBsAg loss within 48 weeks of treatment, but most HBsAg loss occurred during the prolonged treatment. 75.0% of patients who obtained HBsAg loss needed extended treatment, and more than half of HBsAg loss occurred from 72 to 120 weeks. In the patients who had HBsAg loss, HBV DNA load maintained undetectable level during study period including the patients who discontinue treatment. These results indicate that extended treatment help to increase HBsAg loss rate in patients treated with PEG-IFNα-2a.
Serum HBsAg level was positively associated with cccDNA in hepatic cells and should therefore be monitored (Chan et al. 2007; Giersch et al. 2017), especially during IFN treatment, to determine when to stop treatment and to predict the efficacy of the treatment (Chan et al. 2011a; Li et al. 2019). Chan et al. reported that, in the inactive carriers, serum HBsAg levels could predict spontaneous HBsAg clearance. HBsAg < 100 IU/mL predicted HBsAg loss with 75% sensitivity and 91% specificity, and subjects had a long-term positive outcome after 88 ± 26 months (range, 21–139) of follow-up (Chan et al. 2011b). Regardless of HBsAg loss, patients may have good long-term outcome if they achieved HBsAg < 100 IU/mL after antiviral therapy. However, an annual relapse rate for hepatitis B of 1.5%–3.3% has been reported (Chu and Liaw 2007; Hsu et al. 2002). In patients with spontaneous HBeAg seroconversion, there were 14%, 18%, and 22% patients who developed HBeAg-negative hepatitis after of 3, 5, and 10 years of follow-up (Hsu et al. 2002), and hepatocellular carcinoma occurred in HBeAg-negative patients (Hadziyannis and Papatheodoridis 2006). Nevertheless, no patients who achieved HBsAg loss died of liver cancer or cirrhosis after 61.7 months (range, 12–179) of follow-up (Chen et al. 2002). Therefore, achieving HBsAg loss after IFN treatment is critical important except for predicting a sustained viral response or relapse after therapy.
In our study, except 12 patients achieved HBsAg loss, there were 24.6% patients who achieved HBsAg level < 100 IU/mL. These patients might have sustained viral response. HBsAg level dropped rapidly and continuously in completed response patients, which was similar in partial response patients within 72 weeks of treatment. However, HBsAg levels reached a plateau during 72–96 weeks of treatment in partial response patients. In patients of poor response group, HBsAg levels only fell slightly during total treatment course. At 24 weeks, the HBsAg level of patients in completed response group decreased faster and the absolute HBsAg level was significantly lower than those in partial response group. These results suggest that early HBsAg decline might help predict occurrence of HBsAg loss during extended PEG-IFN treatment.
In this study, the HBsAg level at treatment of 12 and 24 weeks can also be used to predict occurrence of HBsAg loss at 96 and 120 weeks, especially with high NPV. The specificity and NPV of HBsAg level at 24 weeks to HBsAg loss occurred whether at treated 96 weeks or 120 weeks were 100%, and with AUC 0.925 and 0.922 respectively. Our results suggest that the patients will hardly achieve HBsAg loss after the following PEG-IFN treatment to 120 weeks if their HBsAg level cannot reach the cutoff levels at 24 weeks.
Of all patients, there were 95.06% (77/81) achieved undetectable level HBV DNA at 48 weeks treatment. The rate of HBV DNA negative conversion was higher than those (25.09% and 63.27% respective) in large clinical trials of patients with HBeAg positive and HBeAg negative CHB at end of 48 weeks treatment (Lau et al. 2005; Marcellin et al. 2004). The difference might be from the discrepancy in patient’s composition among the studies. In this study, although the rates of undetectable HBV DNA were similar among the three groups, serum HBV DNA in patients in the complete response group became undetectable within 36 weeks. These results further support that early undetectable HBV DNA levels is associated with HBsAg loss.
Some limitations existed in our study. The efficacy of PEG-IFN treatment for CHB is affected by HBV genotype. Without data of viral genotype, the effect of viral genotype on HBsAg loss during PEG-IFN treatment wasn’t analyzed in our study. Although HBsAg loss is associated with long-term good outcome in patients infected with HBV, the incidence of HCC and hepatitis relapse cannot be completely eliminated (Simonetti et al. 2010). The long-term benefits of PEG-IFN treatment, including the occurrence of HBsAg loss and the development of cirrhosis or HCC, await further observation.
In conclusion, results in this study show that extended treatment help to increase HBsAg loss rate in HBeAg-negative CHB patients treated with PEG-IFN. The HBsAg level at 24 weeks can be used to predict HBsAg loss during tailoring PEG-IFN therapy.
References
Brunetto MR, Oliveri F, Colombatto P, Moriconi F, Ciccorossi P, Coco B, Romagnoli V, Cherubini B, Moscato G, Maina AM, Cavallone D, Bonino F (2010) Hepatitis B surface antigen serum levels help to distinguish active from inactive hepatitis B virus genotype D carriers. Gastroenterology 139:483–490
Chan HL, Wong VW, Tse AM, Tse CH, Chim AM, Chan H, Wong GL, Sung JJ (2007) Serum hepatitis B surface antigen quantitation can reflect hepatitis B virus in the liver and predict treatment response. Clin Gastroenterol Hepatol 5:1462–1468
Chan HL, Wong VW, Wong GL, Tse CH, Chan HY, Sung JJ (2010) A longitudinal study on the natural history of serum hepatitis B surface antigen changes in chronic hepatitis B. Hepatology 52:1232–1241
Chan HL, Wong GL, Chim AM, Chan HY, Chu SH, Wong VW (2011a) Prediction of off-treatment response to lamivudine by serum hepatitis B surface antigen quantification in hepatitis B e antigen-negative patients. Antivir Ther 16:1249–1257
Chan HL, Wong GL, Tse CH, Chan HY, Wong VW (2011b) Viral determinants of hepatitis B surface antigen seroclearance in hepatitis B e antigen-negative chronic hepatitis B patients. J Infect Dis 204:408–414
Chen YC, Sheen IS, Chu CM, Liaw YF (2002) Prognosis following spontaneous HBsAg seroclearance in chronic hepatitis B patients with or without concurrent infection. Gastroenterology 123:1084–1089
Chen CJ, Yang HI, Su J, Jun S, Jen CL, You SL, Lu SN, Huang GT, Iloeje UH, REVEAL-HBV Study Group (2006) Risk of hepatocellular carcinoma across a biological gradient of serum hepatitis B virus DNA level. JAMA 295:65–73
Chinese Society of Infectious Diseases, Chinese Medical Association; Chinese Society of Hepatology, Chinese Medical Association (2019) The Guidelines of Prevention and Treatment for Chronic Hepatitis B (2019 Version). Zhonghua Gan Zang Bing Za Zhi. 27:938–961
Chu CM, Liaw YF (2007) Spontaneous relapse of hepatitis in inactive HBsAg carriers. Hep Intl 1:311–315
Chu CJ, Hussain M, Lok AS (2002) Quantitative serum HBV DNA levels during different stages of chronic hepatitis B infection. Hepatology 36:1408–1415
Cornberg M, Wong WS, Locarnini S, Brunetto M, Janssen HLA, Chan HL (2017) The role of quantitative hepatitis B surface antigen revisited. J Hepatol 66:398–411
European Association for the Study of the Liver. European Association for the Study of the Liver. EASL 2017 (2017) Clinical Practice Guidelines on the management of hepatitis B virus infection. J Hepatol 67:370–398
Giersch K, Lena A, Tassilo V, Maura D, Marc L (2017) Serum HBV pgRNA as a clinical marker for cccDNA activity. J Hepatol 66:460–462
Gill U, Micco L, Li L, Peppa D, Ushiro-Lumb I, Foster G, Maini M, Kennedy P (2011) Pegylated interferon alpha modulates innate immunity in eag positive chronic hepatitis B and determines changes in HBSag quantification. J Hepatol 54:S32
Hadziyannis SJ, Papatheodoridis GV (2006) Hepatitis B e antigen-negative chronic hepatitis B: natural history and treatment. Semin Liver Dis 26:130–141
Hsu YS, Chien RN, Yeh CT, Sheen IS, Chiou HY, Chu CM, Liaw YF (2002) Long-term outcome after spontaneous HBeAg seroconversion in patients with chronic hepatitis B. Hepatology 35:1522–1527
Hu P, Shang J, Zhang W, Gong G, Li Y, Chen X, Jiang J, Xie Q, Dou X, Sun Y, Li Y, Liu Y, Liu G, Mao D, Chi X, Tang H, Li X, Xie Y, Chen X, Jiang J, Zhao P, Hou J, Gao Z, Fan H, Ding J, Zhang D, Ren H (2018) HBsAg Loss with peg-interferon alfa-2a in hepatitis B patients with partial response to nucleos(t)ide analog: new Switch Study. J Clin Transl Hepatol Mar 28:25–34
Hui CK, Lau GK (2006) Current issues and future directions in treatment. Semin Liver Dis 26:192–197
Koffas A, Dolman GE, Kennedy PT (2018) Hepatitis B virus reactivation in patients treated with immunosuppressive drugs: a practical guide for clinicians. Clin Med (Lond) 18:212–218
Lampertico P, Viganò M, Di Costanzo GG, Sagnelli E, Fasano M, Di Marco V, Boninsegna S, Farci P, Fargion S, Giuberti T, Iannacone C, Regep L, Massetto B, Facchetti F, Colombo M, PegBe Liver Study Group (2013) Randomised study comparing 48 and 96 weeks peginterferon α-2a therapy in genotype D HBeAg-negative chronic hepatitis B. Gut 62:290–298
Lau GK, Piratvisuth T, Luo KX, Marcellin P, Thongsawat S, Cooksley G, Gane E, Fried MW, Chow WC, Paik SW, Chang WY, Berg T, Flisiak R, McCloud P, Pluck N, Peginterferon Alfa-2a HBeAg-Positive Chronic Hepatitis B Study Group (2005) Peginterferon Alfa-2a, lamivudine, and the combination for HBeAg-positive chronic hepatitis B. N Engl J Med 352:2682–2695
Li GJ, Yu YQ, Chen SL, Fan P, Shao LY, Chen JZ, Li CS, Yi B, Chen WC, Xie SY, Mao XN, Zou HH, Zhang WH (2015) Sequential combination therapy with pegylated interferon leads to loss of hepatitis B surface antigen and hepatitis B e antigen (HBeAg) seroconversion in HBeAg-positive chronic hepatitis B patients receiving long-term entecavir treatment. Antimicrob Agents Chemother 7:4121–4128
Li MH, Zhang L, Qu XJ, Lu Y, Shen G, Wu SL, Chang M, Liu RY, Hu LP, Li ZZ, Hua WH, Song SJ, Xie Y (2017) Kinetics of hepatitis B surface antigen level in chronic hepatitis b patients who achieved hepatitis B surface antigen loss during pegylated interferon alpha-2a treatment. Chin Med J (Engl) 130:559–565
Li MH, Yi W, Zhang L, Lu Y, Lu HH, Shen G, Wu SL, Hao HX, Gao YJ, Chang M, Liu YR, Hu LP, Cao WH, Chen QQ, Li JN, Wan G, Xie Y (2019) Predictors of sustained functional cure in HBeAg-negative patients achieving HBsAg seroclearance with interferon-alfa-based therapy. J Viral Hepat 26(Suppl. 1):32–41
Liu J, Yang HI, Lee MH, Jen CL, Batrla-Utermann R, Lu SN, Wang LY, You SL, Chen CJ (2016) Serum Levels of Hepatitis B Surface Antigen and DNA Can Predict Inactive Carriers With Low Risk of Disease Progression. Hepatology 64:381–389
Mak LY, Seto WK, Fung J, Yuen MF (2019) Novel developments of hepatitis B: treatment goals, agents and monitoring tools. Expert Rev Clin Pharmacol 12:109–120
Manesis EK, Papatheodoridis GV, Hadziyannis E (2010) significance of serum HBsAg levels for the definition of the inactive hepatitis B carrier state. Hepatology 52(SUPPL):560A
Ning Q, Han M, Sun Y, Jiang J, Tan D, Hou J, Tang H, Sheng J, Zhao M (2014) Switching from entecavir to PegIFN alfa-2a in patients with HBeAg-positive chronic hepatitis B: a randomised open-label trial (OSST trial). J Hepatol 61:777–784
Papatheodoridis GV (2011) Treatment of HBeAg-negative chronic hepatitis B patients with nucleos(t)ide analogues. Liver Int 31:95–103
Marcellin P, Lau GK, Bonino F, Farci P, Hadziyannis S, Jin R, Lu ZM, Piratvisuth T, Germanidis G, Yurdaydin C, Diago M, Gurel S, Lai MY, Button P, Pluck N, Peginterferon Alfa-2a HBeAg-Negative Chronic Hepatitis B Study Group (2004) Peginterferon alfa-2a alone, lamivudine alone, and the two in combination in patients with HBeAg-negative chronic hepatitis B. N Engl J Med 351:1206–1217
Marcellin P, Bonino F, Lau GK, Farci P, Yurdaydin C, Piratvisuth T, Jin R, Gurel S, Lu ZM, Wu J, Popescu M, Hadziyannis S, Peginterferon alfa-2a in HBeAgnegative Chronic Hepatitis B Study Group (2009) Sustained response of hepatitis B e antigen-negative patients 3 years after treatment with peginterferon alpha-2a. Gastroenterology 136:2169–2179
Patrick M, Lau George KK, Ferruccio B, Patrizia F, Stephanos H, Jin Rui L, Zhi-Meng PT, Georgios G, Cihan Y, Moises D, Selim G, Ming-Yang L, Peter B, Nigel P (2004) Peginterferon Alfa-2a HBeAg-Negative Chronic Hepatitis B Study Group. Peginterferon alfa-2a alone, lamivudine alone, and the two in combination in patients with HBeAg-negative chronic hepatitis B. N Engl J Med 351:1206–1217
Patrick M, Ferruccio B, Lau George KK, Patrizia F, Cihan Y, Teerha P, Rui J, Gurel Selim L, Jian Z-MW, Matei P, Stephanos H, Peginterferon alfa-2a in HBeAg-negative Chronic Hepatitis B Study Group (2009) Sustained response of hepatitis B e antigen-negative patients 3 years after treatment with peginterferon alpha-2a. Gastroenterology 136:2169–2179
Rijckborst V, ter Borg MJ, Cakaloglu Y, Ferenci P, Tabak F, Akdogan M, Simon K, Raptopoulou-Gigi M, Ormeci N, Zondervan PE, Verhey E, van Vuuren AJ, Hansen BE, Janssen HL, PARC Study Group (2010) A randomized trial of peginterferon alpha-2a with or without ribavirin for HBeAg-negative chronic hepatitis B. Am J Gastroenterol 105:1762–1769
Seto WK, Lo YR, Pawlotsky JM, Yuen MF (2018) Chronic hepatitis B virus infection. Lancet 392:2313–2324
Simonetti J, Bulkow L, McMahon BJ, Homan C, Snowball M, Negus S, Williams J et al (2010) Clearance of hepatitis B surface antigen and risk of hepatocellular carcinoma in a cohort chronically infected with hepatitis B virus. Hepatology 51:1531–1537
Sonneveld MJ, Hansen BE, Piratvisuth T, Jia JD, Zeuzem S, Gane E, Liaw YF, Xie Q, Heathcote EJ, Chan HL, Janssen HL (2013) Response-guided peginterferon therapy in hepatitis B e antigen-positive chronic hepatitis B using serum hepatitis B surface antigen levels. Hepatology 58:872e80
Terrault NA, Lok ASF, McMahon BJ, Chang KM, Hwang JP, Jonas MM, Brown RS Jr, Bzowej NH, Wong JB (2018) Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology 67:1560–1599
WHO. Global hepatitis report 2017. Geneva. https://www.who.int/hepatitis/publications/global-hepatitisreport2017/en/. Accessed 4 April 2019
Xie Y, Yi W, Zhang L, Lu Y, Hao HX, Gao YJ, Ran CP, Lu HH, Chen QQ, Shen G, Wu SL, Chang M, Hu LP, Liu RY, Sun L, Wan G, Li MH (2019) Evaluation of a logistic regression model for predicting liver necroinflammation in hepatitis B e antigen-negative chronic hepatitis B patients with normal and minimally increased alanine aminotransferase levels. J Viral Hepat 26(Suppl. 1):42–49
Yim HJ, Lok AS (2006) Natural history of chronic hepatitis B virus infection: what we knew in 1981 and what we know in 2005. Hepatology 43:S173–S181
Acknowledgements
This study was funded in part by the Beijing Hospitals Authority of Hospitals Clinical Medicine Development of Special Funding Support (XMLX 201706), the National Science and Technology Major Project of China (2017ZX10203202-003, 2017ZX10201201-001-006, and 2017ZX10201201-002-006), Beijing Science and Technology Commission (D161100002716002), and the Digestive Medical Coordinated Development Center of Beijing Hospitals Authority (XXZ0302 and XXT28).
Author information
Authors and Affiliations
Contributions
YX designed the study. ML, LZ, YL, QC, HL, FS and ZZ performed the data collection and patient followup. YX and GW conducted data analysis. ML and LZ drafted the manuscript. LZ and YX revised and finalized the manuscript. All authors read and approved the final version of the manuscript.
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Animal and Human Rights Statement
The study was approved by the Institutional Review Board of Beijing Ditan Hospital (Approval number: JDL2013-031-07). Written informed consent was obtained from all patients, and the study was registered at clinicaltrials.gov (Clinical Trials. gov ID: NCT02387684).
Rights and permissions
About this article

Cite this article
Li, M., Zhang, L., Lu, Y. et al. Early Serum HBsAg Kinetics as Predictor of HBsAg Loss in Patients with HBeAg-Negative Chronic Hepatitis B after Treatment with Pegylated Interferonα-2a. Virol. Sin. 36, 311–320 (2021). https://doi.org/10.1007/s12250-020-00290-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12250-020-00290-7