
Abstract
Herpes simplex virus (HSV) infections are common and widespread; nevertheless, their outcome can be of unpredictable prognosis in neonates and in immunosuppressed patients. Anti-HSV therapy is effective, but the emergence of drug-resistant strains or the drug toxicity that hamper the treatment is of great concern. Vaccine has not yet shown relevant benefit; therefore, palliative prophylactic measures have been adopted to prevent diseases. This short review proposes to present concisely the history of HSV, its taxonomy, physical structure, and replication and to explore the pathogenesis of the infection, clinical manifestations, laboratory diagnosis, treatment, prophylaxis and epidemiology of the diseases.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Herpes simplex virus (HSV) infections represent an enormous global health problem. Currently more than 3.7 billion people under the age of 50 (67% of the population) are infected with HSV-1 and 417 million people between 17 and 49 years of age suffer of HSV-2 infection (World Health Organization 2015). The establishment of latency with periodic reactivation, normally benign, is an important feature of the infection. Increased morbidity and mortality are reported in neonates and patients with immunodeficiency, including those with HIV and transplant-associated infections (Espada et al. 2015). Approximately 1500–2000 new cases of neonatal infection are diagnosed each year with 60% mortality when not appropriately treated (World Health Organization 2015). Moreover, in the USA alone, over 400,000 people suffer of recurrent ocular HSV episodes requiring specific medication and corneal transplant in severe cases. The medical, social, and economic burden of HSV infection has been estimated over to US$ 400 million every year in the USA (Chentoufi et al. 2012). Several anti-HSV drugs are approved for clinical use, and among them are iododeoxyuridine, trifluridine, vidarabine, phosphonoformate, cidofovir, acyclovir, valacyclovir, penciclovir, and famciclovir. However, resistant HSV strains emerge particularly in immunosuppressed patients and drug toxic side effects were reported. There is no effective vaccine against HSV infections (Cardozo et al. 2013).
History
Some descriptions of genital lesions that resembled those caused by HSV were found in Sumerian tablet (dated 3rd Millennium BC) and on the Ebers Papyrus (circa 1500 BC) (Roizman et al. 2007). In ancient Greece, the physician Hippocrates documented lesions putatively caused by HSV and called them herpes (derived from the Greek word herpein—reptile, to creep) because the lesions appeared near each other and were vesicular. The first author to describe disease with lesions as occurs for herpes zoster was Celsius. Herodotus was the first historian to call the disease as herpes febrilis manifested by fever, small blisters in the mouth, and sores on the lips. The pharmacist and physician Galen attributed the lesions as the way for the body to release the malignant tumors (Wigg and Miranda 2008). John Astruc, the physician of the King Louis XIV, published a book De Morbis Veneris in which he wrote about genital herpes after the study of the venereal disease in French prostitutes, followed by Fournier writing, in 1896, about the diagnosis and treatment of genital herpes (Roizman et al. 2007; Kim 2011).
Herpesviridae family
The Herpesviridae family includes over 200 members, capable of infecting different species, and among them are eight currently known to cause disease in humans (Santos et al. 2012). The human herpesvirus (HHV) are grouped into three subfamilies, Alphaherpesvirinae, Betaherpesvirinae, and Gammaherpesvirinae, based on the genoma structure, tissue tropism, cytopathologic effect, site of latent infection, pathogenesis, and manifestations of the disease (Murray et al. 2015).
Members of the Alphaherpesvirinae subfamily are characterized by a wide range of host. Short reproductive cycle, ability to spread rapidly between cells and to lyse infected cells efficiently, and the establishment of latent infections in sensory ganglia are the main features. The subfamily includes the following genera: Simplexvirus—herpes simplex virus types 1 and 2 (HSV-1, HSV-2) and Varicellovirus—varicella-zoster virus (VZV). Members of the Betaherpesvirinae subfamily have a restricted host range and a long replicative cycle with slow progression of infection in cell cultures. They may be maintained latent in glandular tissues, lymphoreticular cells, the kidneys, and other tissues. There are two genera: Cytomegalovirus—human cytomegalovirus (CMV) and Roseolovirus—human herpesvirus types 6 and 7 (HHV-6 and HHV-7). Gammaherpesvirinae subfamily viruses establish latent infections mainly in lymphoblastoid cells. Some may produce lytic infections in epithelioid and fibroblastic cells and have oncogenic potential. It contains the genera: Lymphocryptovirus—Epstein-Barr virus (EBV) and Rhadinovirus—human herpesvirus type 8 (HHV-8) (Santos et al. 2012; Kukhanova et al. 2014).
Herpes simplex virus structures
HSV is an enveloped virus with a linear double-stranded DNA genome enclosed by an icosahedral capsid composed of 162 capsomeres. The virion is spherical with 186 nm in diameter with glycoprotein spikes anchored to the envelope (Arduino and Porter 2008). The genome consists of two covalently linked components, designated as L (long) and S (short). Each component is formed by unique sequences (UL e US, respectively) flanked by regions of repeated and inverted sequences that facilitate replication of the genome (Murray et al. 2015). The DNA molecular weight is estimated to approximately 150 kbp, with a G+C content of 68% for HSV-1 and 69% for HSV-2 (Roizman et al. 2007). The capsid is composed by viral proteins VP5, VP19C, VP23, VP24, VP26, and the protein encoded by the U L 6 gene (Silva and Bowers 2009). Between the capsid and the envelope lies an amorphous proteinaceous layer called tegument. It is composed of more than 20 proteins important in the regulation of viral replicative cycle, and among them are (a) α-trans-inducing factor (α-TIF), known as VP16, involved in transcription of immediate early genes (IE), (b) the virion host shut-off protein (VHS) or VP22, responsible for degrading the mRNA of the host cell in the cytoplasm, and (c) VP1-2 which may play a role in DNA release at the nuclear pore during viral entry. The envelope consists of a lipid bilayer and anchors approximately 11 viral glycoproteins, four of which (gB, gD, gH, and gL) are essential for virus entry into cells (Arduino and Porter 2008).
The replication
The infection is initiated by the adsorption, mediated by viral glycoproteins that bind to the glycosaminoglycan chains, present on the cell surface. Among them, heparan sulfate (HS) is considered the main HSV-binding receptor, having a key role in adherence of glycoproteins C (gC) and B on the surface of the target cell (Di Giovine et al. 2011). The interaction of gC and gB with HS receptor is labile until the participation of gD in the process. Several cellular receptors for gD are known as herpesvirus entry mediator (HVEM), the nectins 1 and 2, and a specific form of HS called 3-O-sulfated heparan sulfate (3-OS HS) (Li et al. 2014). When gD interacts with one of these receptors, its polypeptide chain undergoes a conformational change enabling the interaction with the heterodimer gH/gL. This interaction exposes the fusion domains of gB and of the heterodimer leading to fusion of the viral envelope with the plasma membrane of the target cell (Di Giovine et al. 2011).
After penetration into the cytoplasm, the nucleocapsid is transported via microtubules of cytoskeleton to a nuclear membrane pore, where the viral DNA is released in the nucleus. In the cell nucleus, the tegument protein VP16 complexes with cellular protein called host cell factor (HCF) and interacts with the octamer-binding protein Oct-1 associated to the viral DNA, forming the activator or pre-initiation complex. The processes of transcription and replication of the viral genome, as well as the assembly of progeny capsids, take place within the nucleus (Roizman and Whitley 2013).
The HSV lytic cycle involves the regulated expression of sequential and coordinated manner of three sets of viral genes: α or immediate early (IE), β or early (E), and γ or late (L). Initially, the viral DNA is transcribed by the host cell RNA polymerase II and the first genes to be transcribed are the IE genes. After the formation of the activating complex, six IE proteins are synthesized in the early stages of a productive infection: ICP0, ICP4, ICP22, ICP27, ICP47, and a protein encoded by the U S 1.5 gene. The peak of synthesis of these proteins occurs at approximately 3 h postinfection. Once accumulated in sufficient quantity, α proteins return to the nucleus to activate transcription and translation of the β genes, in early proteins or β polypeptides, responsible for the replication of viral nucleic acid, including DNA polymerase and thymidine kinase. The peak of early protein synthesis occurs in 6 h postinfection. As β proteins are expressed, several cellular proteins migrate to the nucleus and gather to form the replication complex in the prereplicative sites where the synthesis of viral DNA begins (Knipe and Cliffe 2008).
After the genome replication, the third group of genes is expressed. The γ genes are regulated by α and β proteins and encode late proteins which form the virus structural proteins, such as tegument and capsid proteins and glycoprotein spikes. The capsid formation occurs through scaffolding proteins that are transported to the nucleus (Cardone et al. 2012).
The transition of the nucleocapsid from the space between the inner and outer nuclear membranes to the cytoplasmic membrane is not well defined. Three hypotheses have been proposed: dual envelopment, single nuclear envelopment, and single cytoplasmic envelopment. The replication process takes approximately 18 to 20 h and the egress of the virus in cells is dependent gD and gH (Roizman et al. 2007).
The pathogenesis
Transmission of HSV depends on intimate and personal contact between a susceptible individual and an individual who is excreting the virus. For infection to be initiated, the virus must come into direct contact with mucosal surfaces or skin with continuity solutions (Butel 2012). Generally, infections by HSV-1 are limited to the oropharynx and the virus is transmitted by respiratory droplets or saliva, and most often by kissing. HSV-2 is mainly transmitted through sexual activity (World Health Organization 2015).
Following the virus replication in the entry site, the intact virion or its nucleocapsid is transported through retrograde axonal flow to the sensory or autonomic ganglia, where the latency is established, preferably in the trigeminal ganglia for HSV-1 and in dorsosacral roots for HSV-2. Recurrences occur when the latent virus is reactivated, being carried by anterograde axonal flow to the region of the primary infection (Knipe and Cliffe 2008). The process of reactivation of latency is triggered by local stimuli, such as injury to the innervated tissue by neurons harboring latent HSV, or by systemic factors as physical or emotional stress, fever, exposure to ultraviolet light, menstruation, and hormonal imbalance (Roizman and Whitley 2013). Infected cells suffer severe structural and biochemical changes induced by virus replication. Among the structural changes are modifications in cellular chromatin, double cell membranes with folds, fragmentation and dispersion of the Golgi apparatus membranes, insertion of viral proteins in cell membranes, rearrangement of microtubule network, and formation of intranuclear inclusion bodies. Furthermore, there are cellular biochemical changes such as blocking protein synthesis, mRNA degradation, blocking of transcription and reduction of RNA synthesis, inhibition of mRNA processing, and selective protein degradation (Roizman et al. 2007).
Clinical manifestations
Generally, the oropharyngeal involvement occurs in the primary HSV-1 infection. There is a great variety of symptoms in the course of the infection, ranging from fully asymptomatic until a combination of fever, throat ulcers, ulcerative and vesicular lesions, gingivostomatitis (usually in primary HSV-1 infection in children and adolescents), edema, located lymphadenopathy, anorexia, and pain. The symptomatic cases typically affect the lips, tongue, gingiva, buccal mucosa, and palate (Arduino and Porter 2008).
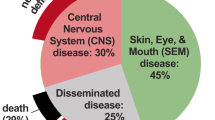
Most cases of genital herpes are caused by HSV-2, although the prevalence of HSV-1 is increasing, mainly in young people, due to the practice of oral sex. Genital herpes is characterized by ulcerative vesicles in the penis and in the cervix, vulva, vagina, or perineum (Penello et al. 2010). The reactivation of orofacial infection, and also genital, is pre-announced by a prodromal stage in which the patient feels pain, burning sensation, itching, or tingling. Other manifestations are keratoconjunctivitis, cutaneous lesions by cuts or abrasions on the skin, paronychia/whitlow (fingers), glossitis, herpes gladiatorum (body), and erythema multiform, a rare skin rash on the back of arms and hand (Arduino and Porter 2008). In neonate, HSV infection may cause a generalized, devastating, and often fatal disease called the generalized infection of the newborn acquired in utero or during the canal passage in natural delivery or postnatally from family members or hospital personnel (Murray et al. 2015). Encephalitis, one of the complications following primary infection, is associated with a high mortality rate and neurologic sequelae among survivors. Compromised patients by malnutrition and immunosuppression are at increased risk for severe HSV infections. HSV lesions can spread and these patients may develop progressive disease involving the respiratory tract, esophagus, and intestinal mucosa (Butel 2012; Prasad et al. 2012).
Laboratory diagnosis
Although physicians easily identify the recurrent infections by the lesions and anamnesis, in the primary infections, atypical manifestations, and asymptomatic shedding, laboratory diagnosis is necessary. Virus isolation from vesicle fluid in cell culture is the most definitive assay for the diagnosis in that the cytopathic effect is detected after 2–3 days of cultivation. The infected cells become enlarged with globular appearance and cell fusion is one of the features with the formation of syncytia (Legoff et al. 2014; Murray et al. 2015).
The polymerase chain reaction (PCR) due to the sensitivity and specificity is used for viral genome detection in specimens poor of virus. The diagnosis of HSV encephalitis by PCR in cerebrospinal fluid is faster and more sensitive than cell culture and, therefore, is the test of choice. Specimens obtained directly from the lesions, whenever feasible, can also be assayed by this method and for further strain differentiation (Geller et al. 2012; Legoff et al. 2014).
When necessary, serological tests should be used in asymptomatic person to demonstrate the infection and can be carried out western blotting, immunoassay, and immunofluorescence (Geller et al. 2012; Legoff et al. 2014).
Treatment
Halogenated nucleoside analogs, such as iododeoxyuridine (IDU) and trifluridine, were the first antivirals developed for HSV infection. The mechanism of action of these antivirals consists in the incorporation of their triphosphorylated forms and the blockage of the nascent viral DNA strand with the sequent inhibition of virus replication. No selective action is attributed to these drugs because cell DNA synthesis is also compromised with the same mechanism, therefore being highly toxic when systemically administered (Lopes 2012).
The major breakthrough in the therapy of HSV infection was the development of nucleoside analogs endowed with selective mechanism of action. Acyclovir (ACV) was the first and still is the antiviral of choice for treatment of the disease. Penciclovir with similar mechanism to that of ACV was developed later. ACV and penciclovir prodrugs, respectively, valaciclovir and famciclovir begun to be widely used due to their lower toxicity and better bioavailability than their counterparts.
For its action, ACV needs to be phosphorylated by thymidine kinase (TK); however, the affinity of viral TK to monophosphorylate the drug is a hundred times greater than that of cellular enzyme. Sequential di- and triphosphorylations are equally done by cellular TK. The ACV-triphosphate inhibits viral DNA synthesis by two mechanisms and inhibits guanosine-triphosphate incorporation competitively by its chemical structural analogy or terminating the nascent viral DNA chain after its incorporation by the absence of 3′-hydroxyl in ACV. Therefore, no additional deoxynucleoside-triphosphate can be linked (Kimberlin and Whitley 2007; Torres et al. 2012).
Some mechanisms involved in HSV resistance to ACV refer to a complete deficiency of viral TK activity, its decreased production, its altered substrate specificity, or a viral DNA polymerase with altered substrate specificity. Approximately 95% of resistant cases are attributed to mutations on the U L 23 gene encoding for TK and 5% to mutations on the U L 30 gene encoding for viral DNA polymerase (Frobert et al. 2014).
Vidarabine (Ara-A) is an adenosine nucleoside analog that also exerts its effect by inhibiting viral DNA synthesis. It was approved in the USA for HSV keratoconjunctivitis, recurrent epithelial keratitis, and encephalitis. Large volume is needed intravenously for its poor solubility and it is rapidly converted to hypoxanthine arabinoside with weak antiviral activity. These are the main limitations of Ara-A in clinical use (Woster 2012).
The phosphonoformate or foscarnet is a structural analog of pyrophosphate and has been used in ACV-resistant infections. It binds to viral DNA polymerase at the pyrophosphate site, inhibiting non-competitively the binding of nucleosides. The foscarnet resistance is due to point mutations in the DNA polymerase gene and typically is associated with prolonged or repeated exposure of the drug. Its low bioavailability and the occurrence of gastrointestinal intolerance hamper its oral use, and therefore, it should be administered by intravenous route (Torres et al. 2012).
Cidofovir is a phosphonate analog of cytidine and was the first nucleotide analog approved for clinical use. For its activation, cellular kinase sequentially attaches two additional phosphate groups, converting cidofovir to its active diphosphate form. As viral enzyme is not required for initial drug phosphorylation, similar level of diphosphate cidofovir is found in both infected and uninfected cells. The nephrotoxicity is a major problem, and therefore, its use in therapy requires caution (Brown et al. 2015).
Vaccines
The vaccines against HSV are still not a reality available for routine clinical use, but research into these has been contributing in a decisive manner to the appearance of new technologies in immunoprophylaxis. As early as 1938, formalin-inactivated HSV vaccine was used, albeit, with discrete outcomes (Chentoufi et al. 2012). Several other vaccine approaches have been tested, including HSV mutants, heterologous or non-human herpesvirus, antigens expressed in live vectors, and virus genetically modified (Roizman et al. 2007).
Subsequent vaccines strategies include discontinuously replicating virus, known as “disabled infectious single cycle” or “DISC”. It is a non-pathogenic virus but capable of inducing humoral and cellular immune response as the wild virus, without the development of any disease. Animals vaccinated with DISC showed a statistically significant protection against primary HSV-1 infection and recurrent outbreaks. The subunit vaccines are also potential candidates, because HSV glycoproteins gB and gD are fundamental in the stimulation of specific cellular immunity, activating the population of cytotoxic lymphocytes. Seronegative guinea pigs vaccinated with a concentrate of viral glycoproteins sensitized the T lymphocytes to recognize gB and gD and presented a prophylactic action against the HSV infection (Chentoufi et al. 2012).
Epidemiology
HSV infections are distributed worldwide and have been reported in both developed and developing countries, including remote Brazilian Indian tribes. The seroprevalence in adults is about 80 to 90% for HSV-1 and varies between 10 and 25% for HSV-2 in most studies (Reil et al. 2008; Whitley 2014).
HSV-1 spreads by direct contact with saliva or through contaminated appliances. The source of infection in children is usually adult with symptomatic HSV lesion or asymptomatic viral shedding by saliva (Butel 2012). HSV-2 infections are usually acquired through sexual contact; therefore, antibodies to virus are rarely found before ages of onset of sexual activity. It is estimated that 400 million people worldwide are currently infected with HSV-2 (Whitley 2014; World Health Organization 2015). Some risk factors described in the acquisition of this virus include a history of a prior sexually transmitted disease, early age for first sexual intercourse, number of abortions, and high number of sexual partners (Penello et al. 2010).
In the USA, approximately 1 in 1000 live births (2500–4000 per year) is infected with HSV. The mortality rate among pregnant women with disseminated HSV infection is reported as greater than 50%. Fetal deaths also have occurred in more than 50% of cases, although mortality did not necessarily correlate with the death of the mother. The Centers for Disease Control and Prevention (CDC) estimates the incidence of HSV encephalitis to be approximately 40–50 cases per year; however, disease occurrence is undoubtedly higher (Roizman et al. 2007).
The high incidence of HSV infection has to be taken as a major concern by public health authority through systematic prevention campaign, being the silent and sexually transmitted disease, and lack of an efficient vaccine.
Change history
28 July 2017
An erratum to this article has been published.
References
Arduino PG, Porter SR (2008) Herpes simplex virus type 1 infection: overview on relevant clinico-pathological features. J Oral Pathol Med 37:107–121
Brown AEC, Cohen MN, Tong S, Braverman RS, Roonev JF, Giller R, Levin MJ (2015) Pharmacokinetics and safety of intravenous cidofovir for life-threatening viral infections in pediatric hematopoietic stem cell transplant recipients. Antimicrob Agents Chemother 59:3718–3725
Butel JS (2012) Herpesvírus. In: Brooks GF, Carroll KC, Butel JS, Morse SA, Mietzner TA (eds) Microbiologia Médica de Jawetz, Melnick e Adelberg, 25th edn. AMGH, Porto Alegre, pp. 433–455
Cardone G, Heymann JB, Cheng N, Trus BL, Steven AC (2012) Procapsid assembly, maturation, nuclear exit: dynamic steps in the production of infectious herpesvirions. Adv Exp Med Biol 726:423–439
Cardozo FT, Larsen IV, Carballo EV, Jose G, Stern RA, Brummel RC, Camelini CM, Rossi MJ, Simões CM, Brandt CR (2013) In vivo anti-herpes simplex virus activity of a sulfated derivate of Agaricus brasiliensis mycelial polysaccharide. Antimicrob Agents Chemother 57:2541–2549
Chentoufi AA, Kritzer E, Yu DM, Nesburn AB, Benmohamed L (2012) Towards a rational design of an asymptomatic clinical herpes vaccine: the old, the new, and the unknown. Clin Dev Immunol 1:1–16
Di Giovine P, Settembre EC, Bhargava AK, Luftig MA, Lou H, Cohen GH, Eisenberg RJ, Krummenacher C, Carfi A (2011) Structure of herpes simplex virus glycoprotein D bound to the human receptor nectin-1. PLoS Patog 7:1–13
Espada SF, Faccin-Galhardi LC, Rincão VP, Bernardi ALS, Lopes N, Longhini R, Mello JCP, Linhares REC, Nozawa C (2015) Antiviral activity of Trichilia catigua bark extracts for herpesvirus and poliovirus. Curr Pharm Biotechnol 16:1–9
Frobert E, Burrel S, Ducastelle-Lepretere S, Billaud G, Ader F, Casalegno JS, Nave V, Boutolleau D, Michallet M, Lina B, Morfin F (2014) Resistance of herpes simplex viruses to acyclovir: an update from a ten-year survey in France. Antivir Res 111:36–41
Geller M, Neto MS, Ribeiro MG, Oliveira L, Naliato ECO, Abreu C, Schechtman RC (2012) Herpes simples: atualização clínica, epidemiológica e terapêutica. J Bras Doenças Sex Transm 24:260–266
Kim J (2011) Herpes simplex virus type 1 glycoprotein gm and the membrane associated protein UL11 are required for virus-induced cell fusion and efficient virus entry. Dissertation, Konkuk University
Kimberlin DW, Whitley RJ (2007) Antiviral therapy of HSV-1 and HSV-2. In: Arvin A, Campadelli-Fiume G, Mocarski E, Moore PS, Roizman B, Whitley R, Yamanishi K (eds) Human herpesviruses: biology, therapy, and immunoprophylaxis, 1st edn. Cambridge University Press, Cambridge, pp. 1153–1174
Knipe DM, Cliffe A (2008) Chromatin control of herpes simplex virus lytic and latent infection. Nat Rev Microbiol 6:211–221
Kukhanova MK, Korovina AN, Kochetkov SN (2014) Human herpes simplex virus: life cycle and development of inhibitors. Biochemistry 79:1635–1652
Legoff J, Péré H, Bélec L (2014) Diagnosis of genital herpes simplex virus infection in the clinical laboratory. Virol J 11:1–17
Li L, Qiu Z, Yan L, Liang F, Ye H, Cai Y, Guo W, Li Y, Yue J (2014) Herpes B virus gD interaction with its human receptor—an in silico analysis approach. Theor Biol Med Model 11:1–16
Lopes N (2012) Avaliação da atividade antiviral de um polissacarídeo sulfatado de Caesalpinia ferrea e do flavonoide quercetina contra o vírus herpes simplex tipo 1 (HSV-1). Dissertação, Universidade Estadual de Londrina
Murray PR, Rosenthal KS, Pfaller MA (2015) Medical microbiology. Elsevier, Rio de Janeiro
Penello AM, Campos BC, Simão MS, Gonçalves MS, Souza PMT, Salles RS, Pellegrini E (2010) Herpes Ggnital. J Bras Doenças Sex Transm 22:64–72
Prasad KM, Watson AM, Dickerson FB, Yolken RH, Nimgaonkar VL (2012) Exposure to herpes simplex virus type 1 and cognitive impairments in individuals with schizophrenia. Schizophr Bull 38:1137–1148
Reil H, Bartlime A, Drerup J, Grewing T, Korn K (2008) Clinical validation of a new triplex real-time polymerase chain reaction assay for the detection and discrimination of herpes simplex virus types 1 and 2. J Mol Diagn 10:361–367
Roizman B, Knipe DM, Whitley RJ (2007) Herpes simplex viruses. In: Knipe DM, Howley PM (eds) Fields Virology, 5th edn. Lippincott Williams & Wilkins, Philadelphia, pp. 2502–2601
Roizman B, Whitley RJ (2013) An inquiry into the molecular basis of HSV latency and reactivation. Annu Rev Microbiol 67:355–374
Santos MPM, Morais MPLA, Fonseca DDD, Faria ABS, Silva IHM, Carvalho AAT, Leão JC (2012) Herpesvírus humano: tipos, manifestações orais e tratamento. Odontol Clín-Cient 11:191–196
Silva S, Bowers WJ (2009) Herpes virus amplicon vectors. Viruses 1:594–629
Torres NI, Castilla V, Bruttomesso AC, Eiras J, Galagovsky LR, Wachsman MB (2012) In vitro antiviral activity of dehydroepiandrosterone, 17 synthetic analogs and ERK modulators against herpes simplex virus type 1. Antivir Res 95:37–48
Whitley RJ (2014) Herpes simplex virus. In: Scheld WM, Whitley RJ, Marra CM (eds) Infections of the central nervous system, 4th edn. Lippincott Williams & Wilkins, Philadelfia, pp. 137–156
Wigg MD, Miranda MMFS (2008) Viroses dermotrópicas. In: Santos NOS, Romanos MTV, Wigg MD (eds) Introdução à Virologia Humana, 2nd edn. Guanabara Koogan, Rio de Janeiro, pp. 177–211
World Health Organization (2015) Herpes simplex virus. http://www.who.int/mediacentre/factsheets/fs400/en/. Accessed 31 Jan 2016
Woster PM (2012) Antiviral agents and protease inhibitors. In: Lemke TL, Williams DA, Roche VF, Zito SW (eds) Foye’s principles of medicinal chemistry, 7th edn. Lippincott Williams & Wilkins, Philadelphia, pp. 1267–1308
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
An erratum to this article is available at https://doi.org/10.1007/s12223-017-0539-2.
Rights and permissions
About this article

Cite this article
Rechenchoski, D.Z., Faccin-Galhardi, L.C., Linhares, R.E.C. et al. Herpesvirus: an underestimated virus. Folia Microbiol 62, 151–156 (2017). https://doi.org/10.1007/s12223-016-0482-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12223-016-0482-7