
Abstract
We aimed to investigate whether the frontal lobe bottom and cerebellum tuber vermis (FLB–CTV) line on brain perfusion scintigraphy, using iodine-123 isopropyl iodoamphetamine single photon emission computed tomography (I-123 IMP SPECT) images, is useful to determine an axial angle parallel to the anterior commissure-posterior commissure (AC–PC) line. We measured the angular differences between the AC–PC line and the FLB–CTV line on midsagittal brain magnetic resonance imaging (MRI) scans of 100 patients. We also evaluated the angular differences of the FLB–CTV line between the IMP SPECT images and the computed tomography for attenuation correction (CTAC) images in the same 100 patients, using a reference line on the CTAC images. Furthermore, the inter-reader reproducibility of the FLB–CTV line measurements on IMP SPECT images of 50 patients between two readers was evaluated using the intra-class correlation coefficient (ICC) and 95% confidence interval (CI). The mean and standard deviation of the angular differences between the AC–PC and FLB–CTV lines on midsagittal brain MRI scans were − 1.24° and 1.14°, respectively. The mean and the standard deviation of the angular differences of the FLB–CTV line in the IMP SPECT and CTAC images were 0.87° and 0.48°, respectively. The ICC of the FLB–CTV line measurements on IMP SPECT images was 0.99 (95% CI 0.98–0.99). We demonstrated that the FLB–CTV line was almost parallel to the AC–PC line and could be reconstructed using IMP SPECT images. The FLB–CTV line can be used as additional evidence to set the axial angle parallel to the AC–PC line.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
In 1988, Talairach et al. reported that the anterior commissure–posterior commissure (AC–PC) line could be used as a standard imaging reference line for stereotaxis in the human brain using magnetic resonance imaging (MRI) [1]. The AC–PC line connects the superior edge of the anterior commissure and the inferior edge of the posterior commissure and is used to reconstruct axial images to facilitate better visualization of the human brain. Furthermore, using this line ensures improved reproducibility between operators for decisions regarding the slice section and is used as a reference plane for data conversion of brain images for most imaging modalities used in neuroscientific clinical practice and research [2, 3].
The AC–PC line can be produced by visualizing the AC and PC using high-resolution MRI. Concurrently, low-resolution brain single-photon emission computed tomography (SPECT) imaging itself cannot visualize the AC and PC; therefore, axial images parallel to AC–PC line cannot be reconstructed using brain SPECT imaging. Although the orbitomeatal line is used to perform an axial SPECT imaging of the brain, it is identified from the body surface and needs to be aligned perpendicular to the collimator while positioning the patient. However, each patient cannot maintain this position. Additionally, this line was reportedly not parallel to the AC–PC line [4]. To the best of our knowledge, there have been no reports of an alternative line to position the axial angle parallel to the AC–PC line to perform brain SPECT imaging. The anatomical landmarks to create the AC–PC line cannot be definitively confirmed via computed tomography (CT); however, Kim et al. reported that the tuberculum sellae-external occipital protuberance (TS-EOP) and tuberculum sellae-internal occipital protuberance (TS-IOP) lines, using extracranial skull structures, could be used as an alternative reference line to set the axial angle parallel to the AC–PC line [4]. Furthermore, Friston et al. reported a method to directly estimate the AC–PC line using four internal landmarks [frontal pole point of the brain (FP), inferior aspect of the anterior corpus callosum (CC), the subthalamic point (TH), and the occipital pole point (OP)] from brain positron emission tomography (PET) images [5]. Consequently, we focused on the idea of drawing a line parallel to the AC–PC line using recognizable landmarks on the contour of the brain through SPECT imaging. Therefore, we propose that the frontal lobe bottom and cerebellum tuber vermis (FLB–CTV) line, using brain perfusion scintigraphy with iodine-123 isopropyl iodoamphetamine SPECT (I-123 IMP SPECT) imaging, is useful in determining an axial angle parallel to the AC–PC line.
2 Materials and methods
3 Ethical approval
Our institutional review board approved this retrospective study and waived the requirement of obtaining informed consent due to the retrospective nature of the study.
3.1 Angular differences between the AC–PC and FLB–CTV lines on brain MRI scans
3.1.1 Patients
We performed a retrospective analysis of 100 consecutive outpatients (46 men and 54 women; age range: 24–91 years; mean age: 75 years), each of whom underwent brain MRI from June 2014 to August 2015 to diagnose intracranial pathologies.
3.1.2 MRI protocol
MRI was performed in all patients using a 1.5 T MRI system (Signa HDx; GE Healthcare, Chicago, IL, USA), with an 8-channel head coil and the images were subsequently acquired in the sagittal plane through a T2-weighted fast spin echo sequence with a 5 mm section thickness and a 6 mm slice spacing. Additionally, the repetition time (ms) to echo time (ms) was 4000/106, flip angle was 90°, the number of excitations (NEX) was 2, the field of view was 36.6 × 22 cm, the matrix was 256 × 256, and the acquisition time was 88 s.
3.1.3 Quantitative analysis
To investigate whether the FLB–CTV line could be used as an alternative reference for the AC–PC line, the angular differences between the AC–PC and FLB–CTV lines were measured on the midsagittal MRI scans created, using an angle measurement tool in the picture archiving and communication systems (PACS) monitor. This FLB–CTV line was defined as the one connecting the FLB and the point projecting to the more occipital side of the CTV (Fig. 1). While measuring the angular differences between the AC–PC and FLB–CTV lines, we noted that their values were relatively negative when the FLB–CTV line was set to the caudal side of the AC–PC line via the FLB coordinates. Additionally, we used Student’s t test to investigate whether there was a significant difference between the FLB–CTV line, which had shifted to the cranial and caudal sides against the AC–PC line. The AC–PC and the FLB–CTV lines of each patient were measured by a radiology technician with 13 years of experience in MRI.

Definitions of the AC–PC and FLB–CTV lines. The AC–PC line (double-headed blue arrowhead): the line connecting the AC and PC. The FLB–CTV line (double-headed red arrowhead): the line connecting the FLB and CTV. AC–PC anterior commissure–posterior commissure, FLB–CTV frontal lobe bottom and cerebellum tuber vermis
3.2 Angular differences in the FLB–CTV line between the I-123 IMP SPECT and CT for attenuation correction (CTAC) images
3.2.1 Patients
We performed a retrospective analysis of 100 consecutive outpatients (32 men and 68 women; age range: 23–90 years; mean age: 74 years), each of whom underwent I-123 IMP SPECT imaging from November 2015 to December 2016 to diagnose various neurodegenerative diseases.
3.2.2 I-123 IMP SPECT imaging protocol
We collected SPECT data for approximately 20 min using a SPECT system with a dual detector-type Gamma-camera (Infinia Hawkeye 4 SPECT/CT; GE Healthcare) and an extended low-energy general-purpose collimator = (total angular range: 360, view angle: 6°, repeat: five times), 5 min after an intravenous injection of 222 MBq of I-123 IMP (the patient remained in a quiet room with eyes closed). The matrix size was 128 × 128, and the center of the collection window was 159 keV (energy window range: ± 10%). The images were then reconstructed with a 5.52 mm section thickness using the ordered subset expectation maximization method (iteration 6 subsets 10) with the Butterworth filter (power factor 10, cutoff 0.40 cycles/cm), and the image pixel size of 2.76 mm/pixel. Scatter correction was not performed. Attenuation correction was performed using CTAC, with the CTAC images acquired in helical mode with a fixed tube voltage of 140 kVp and a tube current of 2.5 mA. The CT parameters were as follows: collimation was 5 mm, detector configuration was 4 × 5 mm, pitch was 1.9 mm/rotation, and gantry rotation time was 2.6 rotations per minute. All transverse CTAC images were also reconstructed with a 5 mm section thickness, using filtered back-projection reconstruction. The CT scan was performed in the cephalocaudal direction and all subsequent CT images were obtained in a range from the top to the bottom of the head.
3.2.3 Quantitative analysis
We calculated the angular differences in the FLB–CTV line between the I-123 IMP SPECT and the CTAC images in the same patient, using an angle measurement tool in the Xeleris Functional Imaging Workstation (GE Healthcare) on midsagittal images obtained with I-123 IMP. Following which, we investigated whether these I-123 IMP SPECT images could be used to set the FLB–CTV line. The FLB–CTV line of each patient was measured by a radiology technician with 13 years of experience in nuclear medicine examination (Fig. 2). Furthermore, the inter-reader reproducibility of the FLB–CTV line measurements on the I-123 IMP SPECT images in the cohort of 50 patients was evaluated for two readers (reader 1: radiology technician with 13 years of experience, 5 years of nuclear medicine examination experience; reader 2: radiology technician with 4 years of experience, but no nuclear medicine examination experience).

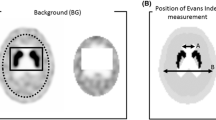
The FLB–CTV line on each image. a The FLB–CTV line on the I-123 IMP SPECT image. b The FLB–CTV line on the CTAC image. CTAC computed tomography attenuation correction, FLB–CTV frontal lobe bottom and cerebellum tuber vermis, I-123 IMP SPECT iodine-123 isopropyl iodoamphetamine single-photon emission computed tomography
3.2.4 Statistical analysis
The inter-reader reproducibility of the FLB–CTV line measurements on the I-123 IMP SPECT images in the 50 patients who were randomly selected from the cohort of 100 patients was evaluated using the intra-class correlation coefficient (ICC) and a 95% confidence interval (CI) for the two readers. Statistical analysis was performed using EZR (easy R) software (Saitama Medical Center, Jichi Medical University, Saitama, Japan).
4 Results
4.1 Angular differences between the AC–PC and FLB–CTV lines on brain MRI scans
The mean ± standard deviation of the angular differences between the AC–PC and FLB–CTV lines on the midsagittal brain MRI scans was 1.24 ± 1.14 (range: − 4° to 2°). There was a significant difference between the FLB–CTV line which shifted to the cranial and caudal sides against the AC–PC line (P < 0.00001).
4.2 Angular differences in the FLB–CTV line between the I-123 IMP SPECT and CTAC images
The mean ± standard deviation of the angular differences in the FLB–CTV line between the I-123 IMP SPECT and the CTAC images was 0.87° ± 0.48° (range: 0°–2°). Additionally, the ICC of the FLB–CTV line measurements on the I-123 IMP SPECT images was 0.99 (95% CI: 0.98–0.99) (Fig. 3).

Inter-reader ICC in the measurement of the FLB–CTV line. The FLB–CTV line measurements between readers 1 and 2 are plotted here. Inter-reader ICC = 0.99 (95% CI: 0.98–0.99). FLB–CTV frontal lobe bottom and cerebellum tuber vermis, ICC intra-class correlation coefficient
5 Discussion
Here, we attempted to determine an alternative line to set the axial angle parallel to the AC–PC line using SPECT imaging.
Evidences regarding the positioning of the AC–PC line using landmarks have previously been reported for both CT and PET images. Kim et al. reported that the TS-EOP and TS-IOP lines in brain CT images are nearly parallel to the AC–PC line used in brain MR images and both can easily be used as reference lines in brain CT scanning [4]. However, I-123 IMP SPECT images cannot be used to visualize the skull; therefore, the TS-EOP and TS-IOP lines cannot be used as an alternative to the AC–PC line in SPECT images. Furthermore, Friston et al. reported a method to directly estimate the AC–PC line position using four internal landmarks from brain PET images (FP, CC, TH, and OP) [5]. However, Minoshima et al. reported that these four internal landmarks could only be identified via visual inspection by experts in brain anatomy and PET imaging [6]. It is evident that the resolution of SPECT images are considerably inferior to that of PET images; therefore, it can be reasonably assumed that identification of these four internal landmarks would be relatively difficult via SPECT imaging. Due to the aforementioned reasons, specific lines are dedicated to each modality, which are often difficult to use with SPECT images. However, we noted that the FLB–CTV line was nearly parallel to the AC–PC line and verified that it could be reconstructed on midsagittal I-123 IMP SPECT images.
The FLB–CTV line was − 1.24° against the AC–PC line and was confirmed to be inclined toward the caudal side of the AC–PC line. This deviation that was considered to be slightly large compared to the results obtained using the aforementioned TS-EOP and TS-IOP lines or the four internal landmarks. However, to the best of our knowledge, there have been no reports of an alternative line that sets the axial angle parallel to the AC–PC line with regard to SPECT imaging. Therefore, using the FLB–CTV line here was considered to be the only method to successfully reconstruct transverse images parallel to the AC–PC line using brain SPECT images. When reconstructing a transverse image with a 150 mm anteroposterior diameter of the brain, an error of − 1.24° results in a maximum error of 3.24 mm against the vertical direction (Fig. 4). However, considering the system’s resolution of the SPECT image (6–10 mm), this error at the level of the SPECT images can be considered negligible. Additionally, the angular differences between the SPECT and CTAC images with regard to the FLB–CTV line was 0.87°, which was also considered negligible. Furthermore, the accuracy with reference to the creation of the FLB–CTV line was nearly unaffected by differences in the operators. High-energy gamma ray of 529 keV emitted by I-123 is known to be treated as scattered radiation in I-123 IMP SPECT imaging and has an inferior resolution than that of other preparations which are used to assess cerebral blood flow, such as Technetium-99 m (Tc-99 m) hexamethylpropyleneamine oxime and Tc-99 m ethyl cysteinate dimer. However, the FLB–CTV line is plotted using the brain’s contour reconstructed via SPECT images. Furthermore, using simple landmarks such as the FLB and the CTV, we were able to draw accurate lines using low-resolution IMP SPECT images and radiology technicians without any experience in nuclear medicine examination were able to visualize the FLB–CTV line.

Effect of the vertical direction error of the FLB–CTV line against the AC–PC line on the I-123 IMP SPECT image. The line connecting the AC–PC line (white line), the FLB–CTV line (red line), and the maximum vertical direction error (green line) is an isosceles triangle with the AC–PC and FLB–CTV lines as its hypotenuses, and the maximum vertical direction error as its base. Therefore, the maximum vertical direction error at − 1.24° is obtained by anteroposterior diameter of a brain (150 mm) × sin(− 1.24). The FLB–CTV line was moved to the AC–PC line for comparison. AC–PC anterior commissure–posterior commissure, FLB–CTV frontal lobe bottom and cerebellum tuber vermis
This study had several limitations. First, changes in shape due to atrophy, tumors, and a decline in the accumulation of IMP against the frontal lobe and the cerebellar tuber could affect the position and accuracy of the line; therefore, it is necessary to confirm the absence of these factors before drawing the FLB–CTV line. Moreover, the effects of these factors on the position and accuracy of the line should be addressed in future studies. Second, the angular differences in the FLB–CTV line between the SPECT and CTAC images were measured in the same cohort of patients. However, the CTAC image was intended to be used for attenuation correction of the SPECT image and is of lower resolution than is the conventional CT image. Therefore, it is our understanding that using the FLB–CTV line reconstructed via CTAC images as a reference line, may have slightly influenced the accuracy evaluation of the FLB–CTV line in the SPECT images. However, the FLB–CTV line is a simple landmark drawn using the brain’s contour and considering the performance of the SPECT/CT apparatus at our institution, using the CTAC images was the best solution. Therefore, it was our understanding that it was best to use the FLB–CTV line of the CTAC images as a reference in this study.
In conclusion, we demonstrated that the FLB–CTV line was nearly parallel to the AC–PC line and could be reconstructed using I-123 IMP SPECT imaging. The FLB–CTV line itself is useful as an additional evidence to set the axial angle parallel to the AC–PC line.
References
Talairach J, Tournoux P. Co-planar stereotaxic atlas of the human brain. New York: Thieme; 1988. p. 122.
Weiss KL, Pan H, Storrs J, Strub W, Weiss JL, Jia L, Eldevik OP. Clinical brain MR imaging prescriptions in Talairach space: technologist- and computer- driven methods. AJNR Am J Neuroradiol. 2003;24:922–9.
Nowinski WL. Modified Talairach landmarks. Acta Neurochir (Wien). 2001;143:1045–57.
Kim YI, Ahn KJ, Chung YA, Kim BS. A new reference line for the brain CT: the tuberculum sellae-occipital protuberance line is parallel to the anterior/posterior commissure line. AJNR Am J Neuroradiol. 2009;30:1704–8.
Friston KJ, Passingham RE, Nutt JG, Heather JD, Sawle GV, Frackowiak RS. Localisation in PET images: direct fitting of the intercommissural (AC–PC) line. J Cereb Blood Flow Metab. 1989;9:690–5.
Minoshima S, Koeppe RA, Mintun MA, Berger KL, Taylor SF, Frey KA, Kuhl DE. Automated detection of the intercommissural line for stereotactic localization of functional brain images. J Nucl Med. 1993;34:322–9.
Funding
The research in this study did not receive any specific aid from funding agencies in the form of grants, equipment, drugs, or any combination of these.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Research involving human participants
All procedures performed in these studies involving human participants were in accordance with the ethical standards as defined by the Institutional Review Board and the 1964 Helsinki Declaration and its later amendments, or comparable ethical standards.
Informed consent
Formal informed consent was not required at our institution to conduct this kind of study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
About this article

Cite this article
Inokuchi, Y., Koya, S., Uematsu, M. et al. Usefulness of the frontal lobe bottom and cerebellum tuber vermis line as an alternative clue to set the axial angle parallel to the AC–PC line in I-123 IMP SPECT imaging: a retrospective study. Radiol Phys Technol 12, 388–392 (2019). https://doi.org/10.1007/s12194-019-00535-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12194-019-00535-5