
Abstract
Background
Fetal and neonatal alloimmune thrombocytopenia (FNAIT) is caused by anti-HPA alloantibody, and anti-HPA-4b is the most common cause in Japanese. Anti-HPA-5b is frequently detected in pregnant women, but it is still controversial whether anti-HPA-5b causes severe FNAIT.
Case presentation
A Japanese woman with anti-HPA-4b and anti-HPA-5b alloantibodies delivered a baby with severe FNAIT who was both HPA-4b and HPA-5b incompatible. We carefully monitored the patient’s following three pregnancies (the second and the fourth siblings were HPA-4b incompatible and HPA-5b compatible; the third sibling was both HPA-4b and HPA-5b compatible). FNAIT was not observed in all three siblings, although a modest decrease in cord blood platelet count was observed in the HPA-4b incompatible siblings compared to the HPA-4b compatible sibling. Serial monitoring of anti-HPA titer showed that anti-HPA-4b markedly decreased in late pregnancy and recovered after delivery of the HPA-4b incompatible siblings, but these decreases were not observed during the mother’s pregnancy with the HPA-4b compatible sibling. In contrast, anti-HPA-5b remained at a high titer during pregnancy with all three siblings.
Conclusion
Our data indicate that dynamic changes of anti-HPA-4b occur during pregnancy and strongly suggest that anti-HPA-5b was mainly responsible for severe FNAIT in this case.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Fetal and neonatal alloimmune thrombocytopenia (FNAIT) is caused by transplacental transfer of maternal IgG alloantibodies raised against fetal human platelet antigens (HPAs) inherited from the paternal parent. The clinical spectrum ranges widely from no bleeding to life threatening intracranial hemorrhage (ICH). In Caucasians, anti-HPA-1a alloantibody associated FNAIT occurs around 1 in 1000–2000 pregnancies, and it can occur even in the first pregnancy [1]. In contrast, HPA-1a incompatibility is extremely rare in Asians, and anti-HPA-4b alloantibodies are more frequent in Japanese [2]. HPA-4a and -4b are determined by a single nucleotide variant (SNV) in ITGB3 c.G>506A that encodes p.Arg143Gln in platelet glycoprotein (GP) IIIa. HPA-5a and -5b is determined by a SNV in ITGA2 c.G1600A that encodes p.Glu505Lys in GPIa. Antibodies against HPA-5b are frequently detected in pregnant women both in Caucasians and Japanese [3, 4], but it is still controversial whether anti-HPA-5b leads to severe FNAIT [5]. Moreover, there are few reports that investigate serial transitions of anti-HPA-4b and anti-HPA-5b titer in multiple pregnancies of FNAIT cases. We previously reported clinical and serological analysis of the second sibling pregnancy of a FNAIT case with anti-HPA-4b and anti-HPA-5b in the first sibling [6]. Here, in addition to the second pregnancy, we demonstrate the titers of alloantibodies during pregnancies of the third and the fourth siblings of the case. Our data indicate the dynamic changes of anti-HPA-4b during pregnancy and strongly suggest that anti-HPA-5b is mainly responsible for the severe FNAIT in the first sibling.
Case presentation
Clinical presentation
Details of pregnancy and delivery of the first and the second siblings were described previously [6]. In brief, a 20-year-old Japanese woman with gravida 3 para 0 delivered a baby with large cephalohematoma and severe thrombocytopenia (12 × 109/L). Eight months later, the mother was referred to our hospital to manage subsequent pregnancy (gravida 4, para 1). Anti-HPA-4b and anti-HPA-5b antibodies in addition to anti-HLA antibodies (A24 and B54) were detected in maternal serum and the cross-match test between maternal serum and paternal platelets was positive. It is unlikely that anti-HLA antibodies cause FNAIT, because HLA B54 was present and A24 was absent in both the first and the second siblings [6], and these data suggested that anti-HPA-4b and/or anti-HPA-5b were the cause of FNAIT of the first sibling. HPA genotyping using amniotic cells at week 16 of gestation revealed HPA-4b incompatibility and HPA-5b compatibility in the second sibling. We administered intravenous immunoglobulin (IVIG, 1 g/kg/w) from gestational week 32 to 35 to reduce the severity of FNAIT [7]. At 36 weeks, the second sibling was born with no bleeding symptom and normal platelet count (214 × 109/L). Two years later, the mother got subsequent pregnancy (gravida 5, para 2). Since HPA genotyping of the fetus using amniotic cells showed compatibility of both HPA-4b and HPA-5b, FNAIT prophylaxis was not performed and the healthy third sibling was born with normal platelet count (361 × 109/L in cord blood). In the next year, the mother got another pregnancy (gravida 6, para 3), and HPA genotype of the fetus using amniotic cells was HPA-4b incompatible and HPA-5b compatible, just the same as the second sibling. Considering the clinical course of the second sibling, FNAIT prophylaxis with IVIG was not performed and the mother delivered the fourth sibling with no bleeding symptom and normal platelet count (242 × 109/L in cord blood) (Tables 1, 2).
Laboratory investigation
Methods
Detection and titration of anti-HPA-4b and anti-HPA-5b were performed by modified monoclonal antibody-specific immobilization of platelet antigen (MAIPA) assay as previously described [6]. HPA-transfectants were used as the source of HPA, and alloantibodies were considered as positive if the ratio of the reactivity of alloantibodies with HPA-transfectants/the reactivity of alloantibodies with mock-transfectants was greater than 2.0 [8]. HPA was genotyped using WAKFlow HPA Typing kit (Wakunaga, Hiroshima, Japan), based on the polymerase chain reaction-reverse sequence-specific oligonucleotide (PCR-rSSO) method.
Results
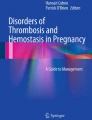
The titers of anti-HPA-4b and anti-HPA-5b were low (× 1) and high (× 64), respectively, at 5 days after the first sibling delivery. In the second sibling pregnancy (HPA-4b incompatible, HPA-5b compatible), the titer of anti-HPA-4b increased to × 4 and × 16 titers at 10 and 19 weeks, respectively. However, its titer unexpectedly decreased to × 1 and undetectable at 30 and 34 weeks of gestation, respectively. Anti-HPA-4b increased again to × 32 titer at one month after delivery. Anti-HPA-5b remained at high titers (× 32 ~ × 128) during the pregnancy. In the third sibling pregnancy (HPA-4b and HPA-5b compatible), both anti-HPA-4b and HPA-5b remained at high titers (anti-HPA-4b: × 32 ~ × 64, anti-HPA-5b: × 128 ~ × 256). In the fourth sibling pregnancy, we checked antibodies titer every 2 weeks since the fetus was HPA-4b incompatible and anti-HPA-4b titer was high (× 64) at gestational week 21. The titer of HPA-4b again markedly decreased to × 8, × 2, and undetectable at 26, 28, and 34 weeks of gestation, respectively, which is the same pattern as shown in the second sibling. Anti-HPA-4b increased again to × 64 titer at 1 month after delivery. Anti-HPA-5b remained at high titers during the course (Fig. 1).

Transition of anti-HPA antibodies during pregnancy of the second to the fourth siblings. Titers of anti-HPA-4b (solid line with square symbol) and anti-HPA-5b (dashed line with triangle symbol) were examined by serial dilution in MAIPA assay employing anti-CD61 and anti-CD49b monoclonal antibodies, respectively
Discussion
We carefully monitored clinical courses and anti-HPA-4b and anti-HPA-5b titers of the following three pregnancies of a woman who developed severe FNAIT in the first sibling. We found that (1) the following three siblings were all HPA-5b compatible, (2) no FNAIT occurred in these siblings even in the presence of HPA-4b incompatibility (the second and the fourth siblings), (3) the titers of anti-HPA-4b unexpectedly decreased to be undetectable in the late pregnancy of the second and the fourth siblings irrespective of prophylactic IVIG, whereas they remained unchanged in the third sibling with HPA-4b compatibility, (4) the anti-HPA-4b may induce modest decrease in the fetal platelet count within normal range, since platelet counts of the second and the fourth sibling slightly decreased as compared with that of the third sibling. Taken together, our data revealed dynamic change of anti-HPA-4b titers during HPA-4b incompatible pregnancy, and strongly suggest that severe FNAIT of the first sibling is mainly caused by anti-HPA-5b, although we could not rule out the possibility of the modest and synergic effect of anti-HPA-4b on the FNAIT.
In Caucasians, anti-HPA-1a is the most common cause of FNAIT, but anti-HPA-4b is the most common cause of FNAIT in Japanese [1, 2]. Anti-HPA-5b is the second most common cause of suspected FNAIT cases both in Caucasians and Japanese [2, 9]. Ohto et al. reported increase in the occurrence of neonatal thrombocytopenia (platelet count < 150 × 109/L) in HPA-5b incompatible pregnancy compared to HPA-5b compatible pregnancy with maternal anti-HPA-5b [2]. However, it is still controversial whether anti-HPA-5b may cause severe FNAIT. Kaplan et al. reported that ICH was developed in 3 out of 39 FNAIT cases with anti-HPA-5b [10]. de Vos et al. also reported that the proportion of severe bleeding cases did not differ between the cases with anti-HPA-1a (11%) and anti-HPA-5b (10%) [11]. On the other hand, employing systematic review and retrospective analysis, Aim et al. recently suggested that anti-HPA-5b may cause mild thrombocytopenia in a small population of neonates, but unlikely causes severe thrombocytopenia [5]. In the present study, severe thrombocytopenia was observed in the first sibling in the presence of both anti-HPA-4b and anti-HPA-5b. In FNAIT with multiple antibodies, it is very difficult to determine which antibody is the dominant antibody in FNAIT. From the epidemiological evidence, one could easily assume that our FNAIT may be caused by anti-HPA-4b. However, our subsequent analysis revealed that anti-HPA-4b is not the main cause of the FNAIT, because HPA-4b incompatibility alone did not induced thrombocytopenia. It is noteworthy that we clearly showed dynamic changes of anti-HPA-4b titer in the late pregnancy and after delivery of the second and the fourth siblings. The titer of anti-HPA-4b became almost undetectable at delivery in the fourth sibling without prophylactic IVIG. The marked decrease in anti-HPA-4b titers was not observed in the third sibling, indicating that immune tolerance during pregnancy is not responsible. Similarly, regarding anti-HPA-1a Killie et demonstrated in a prospective study 92 out of 147 incompatible pregnancies in multigravida showed decline of anti-HPA-1a level during pregnancy and 33 pregnancies showed undetectable anti-HPA-1a alloantibody before delivery [12]. HPA-4b as well as HPA-1a is located on GPIIIa (integrin β3) and endothelial cells express αVβ3. We have demonstrated that anti-HPA-1a antibodies reacted with both platelet GPIIb-IIIa (αIIbβ3) and human umbilical vein endothelial cells (HUVEC) αVβ3. Moreover, the reactivity of anti-HPA-1a against platelets was abolished by pre-incubation of the antibody with HUVEC [12]. Therefore, it is very likely that anti-HPA-4b is absorbed by αVβ3 expressed on highly developed placental endothelial cells in late pregnancy, which leads to the marked decrease of anti-HPA-4b titers. We also noticed that anti-HPA-5b maintained high-titer (× 32– × 256) more than 3 years without boosting by HPA-5b-positive fetuses. These high titers of anti-HPA-5b in our FNAIT are consistent with the suggestion by Ohto et al. that high titer of anti-HPA-5b (≧ 64) is associated with FNAIT [13]. The expression level of GPIa containing HPA-5b antigen on platelet surface has been reported to vary up to 10 folds, which is regulated by polymorphisms of alpha2 gene [14]. Clinical relevance between the GPIa expression level and severity of FNAIT associated with anti-HPA-5b will be an issue to be addressed in the future.
Conclusion
We carefully analyzed the following three pregnancies of a woman with severe FNAIT in the presence of anti-HPA-4b and anti-HPA-5b alloantibodies. Our data revealed that titers of anti-HPA-4b dynamically change during pregnancy with HPA-4b incompatibility and anti-HPA-5b is mainly responsible for our FNAIT case. Careful monitoring of HPA alloantibodies in subsequent pregnancies leads to better understanding of the pathogenesis of FNAIT as well as the management of the pregnancies.
Data availability
The authors declare that the data supporting the findings of this study are available within the article.
References
Peterson JA, McFarland JG, Curtis BR, Aster RH. Neonatal alloimmune thrombocytopenia: pathogenesis, diagnosis and management. Br J Haematol. 2013;161:3–14.
Ohto H, Miura S, Ariga H, Ishii T, Fujimori K, Morita S. The natural history of maternal immunization against foetal platelet alloantigens. Transfus Med. 2004;14:399–408.
Mueller-Eckhardt C, Kiefel V, Grubert A, Kroll H, Weisheit M, Schmidt S, Mueller-Eckhardt G, Santoso S. 348 cases of suspected neonatal alloimmune thrombocytopenia. Lancet. 1989;1:363–6.
Davoren A, Curtis BR, Aster RH, McFarland JG. Human platelet antigen-specific alloantibodies implicated in 1162 cases of neonatal alloimmune thrombocytopenia. Transfusion. 2004;44:1220–5.
Alm J, Duong Y, Wienzek-Lischka S, Cooper N, Santoso S, Sachs UJ, Kiefel V, Bein G. Anti-human platelet antigen-5b antibodies and fetal and neonatal alloimmune thrombocytopenia; incidental association or cause and effect? Br J Haematol. 2022;198:14–23.
Kiyokawa T, Koh Y, Mimura K, Nakayama K, Hosokawa M, Sakuragi M, Morikawa T, Nakao M, Aochi H, Fukumori Y, Kanagawa T, Nagamine K, Kimura T, Tomiyama Y. A case of neonatal alloimmune thrombocytopenia in the presence of both anti-HPA-4b and anti-HPA-5b antibody: clinical and serological analysis of the subsequent pregnancy. Int J Hematol. 2014;100:398–401.
Bussel JB, Berkowitz RL, Lynch L, Lesser ML, Paidas MJ, Huang CL, McFarland JG. Antenatal management of alloimmune thrombocytopenia with intravenous gamma-globulin: a randomized trial of the addition of low-dose steroid to intravenous gamma-globulin. Am J Obstet Gynecol. 1996;174:1414–23.
Hayashi T, Amakishi E, Matsuyama N, Yasui K, Furuta RA, Hori Y, Tanaka S, Fukumori Y, Hirayama F, Inoue M. Establishment of a cell line panel as an alternative source of platelet antigens for a screening assay of anti-human platelet antibodies. Transfus Med. 2011;21:199–204.
Panzer S, Auerbach L, Cechova E, Fischer G, Holensteiner A, Kitl EM, Mayr WR, Putz M, Wagenbichler P, Walchshofer S. Maternal alloimmunization against fetal platelet antigens: a prospective study. Br J Haematol. 1995;90:655–60.
Kaplan C, Morel-Kopp MC, Kroll H, Kiefel V, Schlegel N, Chesnel N, Mueller-Eckhardt C. HPA-5b (Br(a)) neonatal alloimmune thrombocytopenia: clinical and immunological analysis of 39 cases. Br J Haematol. 1991;78:425–9.
de Vos TW, Porcelijn L, Hofstede-van Egmond S, Pajkrt E, Oepkes D, Lopriore E, van der Schoot CE, Winkelhorst D, de Haas M. Clinical characteristics of human platelet antigen (HPA)-1a and HPA-5b alloimmunised pregnancies and the association between platelet HPA-5b antibodies and symptomatic fetal neonatal alloimmune thrombocytopenia. Br J Haematol. 2021;195:595–603.
Killie MK, Husebekk A, Kjeldsen-Kragh J, Skogen B. A prospective study of maternal anti-HPA 1a antibody level as a potential predictor of alloimmune thrombocytopenia in the newborn. Haematologica. 2008;93:870–7.
Ohto H, Yamaguchi T, Takeuchi C, Tohyama Y, Sato A, Morita S. Anti-HPA-5b-induced neonatal alloimmune thrombocytopenia: antibody titre as a predictor. Collaborative Study Group. Br J Haematol. 2000;110:223–7.
Kunicki TJ, Kritzik M, Annis DS, Nugent DJ. Hereditary variation in platelet integrin alpha 2 beta 1 density is associated with two silent polymorphisms in the alpha 2 gene coding sequence. Blood. 1997;89:1939–43.
Acknowledgements
This study was supported in part of a Grant-in-Aid for Scientific Research from the Ministry of Education, Culture, Sports, Science and Technology (Grant no: 22K08476) and from the Ministry of Health, Labor and Welfare (Grant no. 20FC1024) in Japan.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have disclosed no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
About this article

Cite this article
Kiyokawa, T., Mimura, K., Nagamine, K. et al. FNAIT pathogenesis determined by serial analysis of three subsequent pregnancies of a woman with severe fetal and neonatal alloimmune thrombocytopenia (FNAIT) with anti-HPA-4b and anti-HPA-5b alloantibodies in the first sibling. Int J Hematol 118, 146–150 (2023). https://doi.org/10.1007/s12185-023-03559-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12185-023-03559-1