
Abstract
This phase 1/2 study aimed to identify the maximum tolerated dose, the recommended phase 2 dose (RP2D), and efficacy of the clofarabine, etoposide, and cyclophosphamide combination regimen in adult patients with relapsed/refractory acute lymphoblastic leukemia (ALL). Patients aged ≥ 15 years with relapsed/refractory ALL were enrolled. Escalating doses of clofarabine (20–30 mg/m2/day × 5 days), etoposide (50–100 mg/m2/day × 5 days), and cyclophosphamide (200–440 mg/m2/day × 5 days) were administered. Dose-limiting toxicity was defined as Grade 3 or more non-hematological toxicities and others. A total of 18 patients (B-ALL; n = 13, T-ALL; n = 5) were recruited in phase 1; however, the protocol was amended to close study without proceeding to phase 2. Three patients were enrolled in cohort 1, three in cohort 2, six in cohort 3, and six in cohort 4. The RP2D of clofarabine, etoposide, and cyclophosphamide was 30, 100, and 440 mg/m2 daily, respectively. Complete remission (CR) was achieved in four patients (22%) and CR without platelet recovery in four patients (22%), with an overall response rate of 44%. The RP2D of the combination therapy was successfully determined in this study.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In the past few decades, the therapeutic outcome of adult acute lymphoblastic leukemia (ALL) was significantly improved, mainly due to intensive pediatric-based protocols of chemotherapy [1,2,3]. However, the survival of adult patients with relapsed/refractory ALL is still unsatisfactory [4,5,6]. The complete remission (CR) rates for relapsed/refractory ALL in recent studies were 20–83%, and the long-term disease-free survival was only 7–24% [7]. Because CR is a requisite for subsequent allogeneic hematopoietic stem cell transplantation (allo-HSCT), low CR rates associated with current chemotherapy regimens indicate that few patients with relapsed/refractory ALL undergo allo-HSCT. Recently, other treatment options such as immunotherapy targeting ALL surface markers expressed on B lymphoblasts are highlighted. One option is the use of bispecific T cell engager antibodies that bind to the surface antigens on two different target cells [8]. Another immunotherapeutic strategy is represented by inotuzumab ozogamicin, a novel monoclonal antibody against CD22 conjugated to the calicheamicin [9]. Another promising novel therapy is adoptive immunotherapy using chimeric antigen receptor-modified T (CAR-T) cells [10]. Although these strategies have been shown to increase response rate and overall survival (OS) in patients with relapsed/refractory ALL, these immunotherapies potentially correlate with the following: (1) not considered curative; (2) increase the risk of veno-occlusive disease/sinusoidal obstruction syndrome (VOD/SOS); (3) most importantly, not effective for T-ALL. Thus, novel chemotherapeutic options are still needed for relapsed/refractory ALL, and further studies are required to validate these options.
Clofarabine is a second-generation purine nucleoside analog that has been investigated in several phase 1 and 2 trials either as a single agent or in combination for relapsed/refractory acute leukemia in pediatric and adult patients [11,12,13,14,15,16]. For pediatric patients, previous studies demonstrated the recommended phase 2 dose (RP2D) of clofarabine (40 mg/m2/day for 5 days), etoposide (100 mg/m2/day for 5 days), and cyclophosphamide (440 mg/m2/day for 5 days) in phase 1 [13] and an overall response rate of 44% in phase 2 [16]. However, the available information of safety and efficacy in adult patients with relapsed/refractory ALL are still limited. The Japan Adult Leukemia Study Group (JALSG) conducted this multi-institutional phase 1/2 study (JALSG RR-ALL214) with an aim to identify the maximum tolerated dose (MTD), RP2D, and efficacy of the clofarabine, etoposide, and cyclophosphamide combination regimen (CLEC) in adult patients with relapsed/refractory ALL. This study was registered at UMIN-CTR (ID, 000015373).
Materials and methods
Patients and eligibility criteri
Patients aged 15–60 years with relapsed/refractory ALL (B-ALL, T-ALL, and Philadelphia chromosome-positive ALL) were enrolled in this study. Relapse was defined using the standard criteria as reappearance of disease after previous achievement of CR, and primary refractory disease was defined as persistent disease after standard induction therapy. Other inclusion criteria were Eastern Cooperative Oncology Group performance status 0–2, SpO2 > 94%, creatinine clearance level > 60 mL/min, serum direct bilirubin level < 2.0 mg/dL, and normal electrocardiogram results. Patients with prior allo-HSCT were also included. The key exclusion criteria were presence of other active cancers, central nervous system involvement, uncontrolled systemic infection, positivity for hepatitis B or C infection, and presence of serious organ dysfunction after prior allo-HSCT. The protocol was approved by the Institutional Review Board of each hospital. Written informed consent was obtained from all patients before registration in accordance with the Declaration of Helsinki. This study was initiated on November 2014 and closed for patient inclusion in October 2018.
Treatment and trial design
This study was planned to be conducted as a multi-institutional phase 1/2 study. The primary objective of this study was to identify the MTD, RP2D, and efficacy of the CLEC regimen in adult patients with relapsed/refractory ALL. A standard 3 + 3 design [17] was used for dose escalation in phase 1, followed by an expanded cohort at the established RP2D in phase 2. However, the protocol was amended due to difficulty recruiting participants in August 2018 and this study was closed for patient inclusion without proceeding to phase 2. Doses were escalated in six cohorts (cohort − 1 to cohort 4). Escalating doses of clofarabine (20–30 mg/m2/day for 5 days), etoposide (50–100 mg/m2/day for 5 days), and cyclophosphamide (200–440 mg/m2/day for 5 days) were used (details are shown in Table 1). Clofarabine, etoposide, and cyclophosphamide were administered for 2 h, 1.5 h, and 1 h, respectively. All three drugs were administered for 5 consecutive days. Granulocyte-colony stimulating factor was administered on day 6 of induction chemotherapy and continued until recovery of neutrophil counts > 2 × 109/L. Infection prophylaxis was recommended as per institutional guidelines. In cases of non-CR, the CLEC regimen was repeated for a maximum of two cycles. Grade 4 neutropenia and thrombocytopenia that persisted for more than 29 days after the first cycle required a second induction cycle with 20% dose reduction. Grade 3 non-hematological toxicities occurring in the first cycle required suspension of the second induction cycle until recovery to Grade 1 before resuming subsequent treatment with 25% dose reduction. Dose reduction of the second induction cycle was not required for patients who developed infection during the first cycle. Whether or not to proceed to the next cohort was determined based on safety data and the recommendation of the Safety Data Monitoring Committee.
Toxicity and response criteria
Treatment-related adverse events were evaluated using the National Cancer Institute’s Common Terminology Criteria for Adverse Events (version 4.0). Dose-limiting toxicity (DLT) was defined in the first cycle as Grade 4 or more infection, febrile neutropenia, bleeding, vomiting, infusion reaction, and liver toxicities and Grade 3 or more other non-hematological toxicities, excluding complications due to the progression of leukemia. Prolonged severe myelosuppression (peripheral neutrophil counts < 0.5 × 109/L and platelet counts < 20 × 109/L) that persisted until 42 days from the start of chemotherapy was also defined as DLT, when it was not due to the progression of leukemia. Response to treatment was determined by the investigators. Briefly, CR was defined as < 5% bone marrow blasts with maturation of all other cell lineages, peripheral neutrophil counts > 1 × 109/L, platelet counts > 100 × 109/L, and no evidence of extramedullary leukemia. CR without platelet recovery (CRp) was defined as meeting all criteria for a CR except platelet recovery. Non-CR was defined as > 5% blasts after the second induction therapy.
Statistical analysis
The cohort of patients was three (or six) based on a standard 3 + 3 design. Continuous variables were summarized using median and range and categorical variable were summarized using frequency and proportion. All statistical analyses were performed using the SAS software, version 9.4 (SAS Institute Inc., Cary, NC).
Results
A total of 18 patients (B-ALL; n = 13, T-ALL; n = 5) were enrolled in the four cohorts (cohort 1 to cohort 4). These patients had a median (range) age of 42 (19–58) years, and the median level of leukemic blasts in the bone marrow was 52% (2–95%). Eleven (61%) received three or more prior regimens, and six (33%) had undergone prior allo-HSCT. The patients’ characteristics are summarized in Table 2. Three patients were enrolled in cohort 1 (clofarabine 20 mg/m2/day, etoposide 75 mg/m2/day, and cyclophosphamide 340 mg/m2/day), three in cohort 2 (clofarabine 20 mg/m2/day, etoposide 75 mg/m2/day, and cyclophosphamide 440 mg/m2/day), and three in cohort 3 (clofarabine 30 mg/m2/day, etoposide 75 mg/m2/day, and cyclophosphamide 440 mg/m2/day). One patient in cohort 3 died of tumor lysis syndrome (Grade 5, defined as a DLT); therefore, we evaluated MTD in additional three patients in cohort 3. No further DLT was noted in cohort 3, and we proceeded to the next cohort based on recommendation of the Safety Data Monitoring Committee. Six patients have to be treated at the dose level to be declared as MTD. Therefore, six patients were enrolled in cohort 4 (clofarabine 30 mg/m2/day, etoposide 100 mg/m2/day, and cyclophosphamide 440 mg/m2/day). Although, one patient in cohort 4 developed sepsis (Grade 4, defined as DLT), MTD was not reached in this cohort. Therefore, the RP2Ds of clofarabine, etoposide, and cyclophosphamide were 30, 100, and 440 mg/m2/day, respectively, each given for 5 consecutive days. Patients’ characteristics and treatment efficacies of each cohort are listed in Table 3.
The most common toxicity observed was myelosuppression. All patients had Grade 4 neutropenia, lymphocytopenia, and thrombocytopenia. Fifteen patients (83%) had Grade 3 anemia. However, myelosuppression was not considered a DLT, as it resolved within 42 days. A total of 15 (83%) patients had Grade 3 or 4 infectious complications (10 with febrile neutropenia, three with catheter-related infection, and two with sepsis). Two (11%) patients had a Grade 3 increased alanine aminotransferase level; however, neither Grade 3 or 4 direct bilirubin level increased nor clinical diagnosis of VOD/SOS was documented. Overall, the common non-hematological treatment-related adverse events in > 10% of patients were febrile neutropenia (56%), gastrointestinal disorders (33%), increased alanine aminotransferase level (22%), catheter-related infection (17%), sepsis (11%), fatigue (11%), increased aspartate aminotransferase level (11%), and increased creatinine level (11%). The major treatment-related adverse events are summarized in Table 4.
Importantly, we noted that two patients who developed DLT in this study. One patient in cohort 3 (case 7 as shown in Table 3) died of tumor lysis syndrome (Grade 5). This patient was a 31-year-old woman who showed extremely high white blood cell counts (208 × 109/L) at the time of chemotherapy. Although approaches to prevent tumor lysis syndrome, including laboratory monitoring, use of uric acid-reducing drugs including rasburicase, and adequate hydration were used, this patient developed clinical tumor lysis syndrome (acute renal failure, cardiac dysfunction, and seizure) and died 5 days after chemotherapy. This toxicity was defined as a DLT. Another patient in cohort 4 (case 17) developed sepsis (Grade 4) day 16 on chemotherapy. This toxicity was also defined as a DLT. On the other hand, one patient in cohort 1 (case 2) developed sepsis (Grade 4); however, this toxicity was not defined as a DLT. Because this was considered to be complication due to progression of leukemia. In addition, one patient in cohort 2 (case 5) developed prolonged severe myelosuppression and skin eruption (Grade 3) after the second induction cycle. Eventually this patient died of adult respiratory distress syndrome (Grade 5) 55 days after second induction chemotherapy. DLTs were assessed only in the first cycle; therefore, these toxicities also were not defined as DLT.
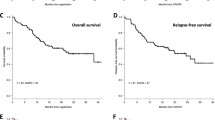
Overall, CR was achieved in four patients (22%), CRp in four patients (22%), and the overall response rate was 44%. The median (range) time to achieve CR/CRp was 27.5 (21–43) days. Seven (88%) of these eight patients with CR achieved their best response after the first cycle. Regarding immunophenotype, the overall response rate was 46% (two for CR and four for CRp) in B-ALL (n = 13) and 40% (two for CR) in T-ALL (n = 5). Responses were observed in all cohorts: in cohort 1 (n = 3), two patients achieved CRp; in cohort 2 (n = 3), one achieved CRp; in cohort 3 (n = 6), two achieved CR and one achieved CRp; in cohort 4 (n = 6), two achieved CR. Although, the median (range) follow-up duration was very short (8.5; 0.1–19.9 months; n = 18), the median response duration was 7.2 (0.6–13.2) months (n = 8). In addition, the median duration from prior allo-HSCT to study entry was 17.6 (6.8–39.5) months (n = 6). Eventually, 15 (83%) patients (eight patients with CR and seven patients with non-CR) underwent allo-HSCT. The median duration from study entry to post-study allo-HSCT was 2.1 (1.3–14.5) months (n = 13, data were not available in two cases) and the median duration from response to post study allo-HSCT was 1.3 (0.3–13.9) months (n = 13, were not available in two cases).
Discussion
In the present phase 1/2 study, we successfully determined the MTD and RP2D of clofarabine when used in combination with etoposide and cyclophosphamide in adult patients with relapsed/refractory ALL. During this study period, the novel agents such as blinatumomab [8], inotuzumab ozogamicin [9], and tisagenlecleucel [10] became available not only in the commercial form but also in the form used in the phase 1 studies in Japan. In addition, while the complete evaluation was still ongoing, the HOVON phase 3 study reported in the 59th annual meeting of the American Society of Hematology [18] that clofarabine added to standard chemotherapy did not improve OS. These might affect the difficulty of recruiting participants, and eventually this study was closed without proceeding to phase 2.
Although MTD was not reached with the doses evaluated in the target dose cohort, the RP2Ds of clofarabine, etoposide, and cyclophosphamide were determined to be 30, 100, and 440 mg/m2/day, respectively, each administered for 5 consecutive days. As a single agent of clofarabine, MTD was 52 mg/m2/day for 5 days in the pediatric phase 1 study [11, 12]. Combined with etoposide and cyclophosphamide, in the pediatric phase 1 study, Hijiya et al. reported that the RP2Ds of clofarabine, etoposide, and cyclophosphamide were 40, 100, and 440 mg/m2/day, respectively, each administered for 5 consecutive days [13]. In contrast, a single-agent adult phase 1 study showed that the MTD was 40 mg/m2/day for 5 days [14]. Comparisons between pediatric and adult studies have indicated that the optimal dose of clofarabine when used in combination with etoposide and cyclophosphamide is < 40 mg/m2/day. Our study included both adolescent and young adult (AYA) patients (n = 8), who were defined as individuals aged 39 years or younger, and adult patients (n = 10). Therefore, it is important to mention that there are limitations in analyzing the safety of the therapy in the AYA and adult generations with same eligibility (especially in adult patients). However, in our study, four of 6 patients in cohort 4 (recommended dose cohort) were aged 40 or older. Hence based on previous reports and the results of our study, we recommend clofarabine 30 mg/m2/day for 5 days when used in combination with etoposide (100 mg/m2/day for 5 days) and cyclophosphamide (440 mg/m2/day for 5 days) in adult patients with relapsed/refractory ALL.
Regarding safety, the most common toxicity observed was myelosuppression, such as neutropenia, lymphocytopenia, and thrombocytopenia. Although Grade 3 infectious complications were frequently observed, no patient developed Grade 5 infection in this study. Furthermore, four (22%) patients proceeded to the second induction cycle; however, no patient required dose reduction. Comparing our results to those of previous studies including several salvage regimens, we observed a comparable incidence of infectious toxicities and reduced severity of febrile episodes with lower mortality [16, 19,20,21]. The difference in mortality observed between our study and previous studies might be influenced by the small number of patients analyzed in our study. Several other factors including patient age and performance status might have contributed to lower mortality. Generally, salvage chemotherapies for relapsed/refractory acute leukemia frequently induce viral and fungal infections [22]. Although severe neutropenia and lymphocytopenia were observed, the frequency of documented viral and fungal infection did not increase in the present study. We assessed DLTs only during the first cycle; therefore, careful monitoring and prophylactic or preemptive anti-infectious strategies should be considered in CLEC treatment, especially in the second cycle. Importantly, we did not observe clinically diagnosed VOD/SOS, although, in other series, this was frequently reported [9, 16, 23]. In the pediatric phase 2 study of the CLEC regimen, VOD/SOS was observed in 12% of patients. In that report, patients with VOD/SOS had undergone allo-HSCT within 12 months before study entry, and no additional case of VOD/SOS was observed in enrolled patients after the study protocol was amended to exclude patients with prior allo-HSCT [16]. Therefore, prior allo-HSCT and heavy pretreatment were considered risk factors for developing VOD/SOS during CLEC treatment. Six patients (33%) had undergone prior allo-HSCT, and 11 patients (61%) received three or more prior regimens; however, we did not observe clinically diagnosed VOD/SOS. Although we could not compare our results to those of previous studies, the duration from the last chemotherapy or prior allo-HSCT to study entry could affect the low incidence of VOD/SOS. Moreover, it is possible that the lower dose of clofarabine (30 mg/m2/day for 5 days in our study) may play an important role in preventing VOD/SOS. However, it is important to note that we observed two patients who developed a Grade 3 increased alanine aminotransferase level in cohort 4. Therefore, close monitoring of liver function is recommended during and after CLEC treatment, especially in those who underwent prior allo-HSCT. The question of whether VOD/SOS is less frequent in the present procedure should be evaluated in a further study including the outcome of proceeding to allo-HSCT after CLEC treatment.
As for the effectiveness, the CLEC regimen showed efficacy (CR = 22%, CRp = 22%, and overall response = 44%) in patients with relapsed/refractory and heavily pretreated adult ALL. Clofarabine had a response rate of 17% when used as a single agent in patients with relapsed/refractory ALL [15]. In the current study, in agreement with other salvage regimens [19,20,21], we observed an overall response rate of 44%. Recently, the mini-HCVD with inotuzumab ozogamicin regimen showed a high overall response rate (78%) in adults with relapsed/refractory ALL [23]. In addition, adoptive immunotherapy with CD19-targeted CAR-T cells showed a surprisingly high CR rate (90%) in relapsed/refractory ALL [10]. However, the concerns of these procedures are the development of VOD/SOS, observed at a rate of 15% in the mini-HCVD with inotuzumab ozogamicin regimen, and it can be complicated by cytokine release syndrome that requires corticosteroid treatment, which may increase infection risk in adoptive immunotherapy. Furthermore, these strategies are ineffective for T-ALL. As we mentioned before, now several novel agents are available. However, novel chemotherapeutic options are still needed for relapsed/refractory ALL. Therefore, selection of the optimal salvage regimen should be carefully considered based on comorbidities, immunophenotype, type of prior therapy, and toxicity profile of the chemotherapy regimen. In previous studies, 30–40% of patients were bridged successfully to allo-HSCT [19,20,21]. Notably, 15 (83%) of 18 patients (including seven patients with non-CR) proceeded to post-study allo-HSCT in our study. This difference can reflect different practices among patient choice, donor availabilities, and options provided by healthcare systems. In addition, five of seven patients with non-CR showed hypoplastic bone marrow without leukemic blasts in peripheral blood. These patients might have a sufficient reduction in disease burden, and these preliminary results encouraged the use of the CLEC regimen as a further attempt to bridge these patients to allo-HSCT. Other investigators have also reported success after using a combination of clofarabine, cyclophosphamide, and etoposide as a bridge therapy to allo-HSCT [24]. However, we did not evaluate the outcome of the CLEC treatment after allo-HSCT with a longer follow-up; therefore, the availability of this procedure should be evaluated in further studies. A phase 2 study should evaluate the efficacy and safety of these RP2Ds in adult patients with ALL; however, we need to focus more on the potential role of the bridging therapy to allo-HSCT, especially in T-ALL.
The CLEC regimen was well tolerated in adult patients with relapsed/refractory ALL. The severity of toxicities with the CLEC regimen was comparable to that of other salvage regimens. The RP2Ds of clofarabine, etoposide, and cyclophosphamide were 30, 100, and 440 mg/m2/day, respectively, each administered for 5 days.
References
Dianne P, Adam G, Hermann B. Improvement in survival in younger patients with acute lymphoblastic leukemia from the 1980s to the early 21st century. Blood. 2009;113:1408–11.
Huguet F, Leguay T, Raffoux E, Thomas X, Beldjord K, Delabesse E, et al. Pediatric-inspired therapy in adults with Philadelphia chromosome-negative acute lymphoblastic leukemia: the GRAALL-2003 study. J Clin Oncol. 2009;27:911–8.
Sakura T, Hayakawa F, Sugiura I, Murayama T, Imai K, Usui N, et al. High-dose methotrexate therapy significantly improved survival of adult acute lymphoblastic leukemia: a phase III study by JALSG. Leukemia. 2018;32:626–32.
Fielding AK, Richards SM, Chopra R, Lazarus HM, Litzow MR, Buck G, et al. Medical Research Council of the United Kingdom Adult ALL Working Party; Eastern Cooperative Oncology Group. Outcome of 609 adults after relapse of acute lymphoblastic leukemia (ALL); an MRC UKALL12/ECOG 2993 study. Blood. 2007;109:944–50.
Gökbuget N, Dombret H, Ribera JM, Fielding AK, Advani A, Bassan R, et al. International reference analysis of outcomes in adults with B-precursor Ph-negative relapsed/refractory acute lymphoblastic leukemia. Haematologica. 2016;101:1524–33.
Kako S, Kanamori H, Kobayashi N, Shigematsu A, Nannya Y, Nakamae M, et al. Outcome after first relapse in adult patients with Philadelphia chromosome-negative acute lymphoblastic leukaemia. Br J Haematol. 2013;161:95–103.
Frey NV, Luger SM. How I treat adults with relapsed or refractory Philadelphia chromosome-negative acute lymphoblastic leukemia. Blood. 2015;126:589–96.
Kantarjian H, Stein A, Gökbuget N, Fielding AK, Schuh AC, Ribera JM, et al. Blinatumomab versus chemotherapy for advanced acute lymphoblastic leukemia. N Engl J Med. 2017;376:836–47.
DeAngelo DJ, Stock W, Stein AS, Shustov A, Liedtke M, Schiffer CA, et al. Inotuzumab ozogamicin in adults with relapsed or refractory CD22-positive acute lymphoblastic leukemia: a phase 1/2 study. Blood Adv. 2017;15:1167–80.
Maude SL, Frey N, Shaw PA, Aplenc R, Barrett DM, Bunin NJ, et al. Chimeric antigen receptor T cells for sustained remissions in leukemia. N Engl J Med. 2014;371:1507–17.
Jeha S, Gandhi V, Chan KW, McDonald L, Ramirez I, Madden R, et al. Clofarabine, a novel nucleoside analog, is active in pediatric patients with advanced leukemia. Blood. 2004;103:784–9.
Koh K, Ogawa C, Okamoto Y, Kudo K, Inagaki J, Morimoto T, et al. Phase 1 study of clofarabine in pediatric patients with relapsed/refractory acute lymphoblastic leukemia in Japan. Int J Hematol. 2016;104:245–55.
Hijiya N, Gaynon P, Barry E, Silverman L, Thomson B, Chu R, et al. A multi-center phase I study of clofarabine, etoposide and cyclophosphamide in combination in pediatric patients with refractory or relapsed acute leukemia. Leukemia. 2009;23:2259–64.
Kantarjian HM, Gandhi V, Kozuch P, Faderl S, Giles F, Cortes J, et al. Phase I clinical and pharmacology study of clofarabine in patients with solid and hematologic cancers. J Clin Oncol. 2003;21:1167–73.
Kantarjian H, Gandhi V, Cortes J, Verstovsek S, Du M, Garcia-Manero G, et al. Phase 2 clinical and pharmacologic study of clofarabine in patients with refractory or relapsed acute leukemia. Blood. 2003;102:2379–86.
Hijiya N, Thomson B, Isakoff MS, Silverman LB, Steinherz PG, Borowitz MJ, et al. Phase 2 trial of clofarabine in combination with etoposide and cyclophosphamide in pediatric patients with refractory or relapsed acute lymphoblastic leukemia. Blood. 2011;118:6043–9.
Storer BE. Design and analysis of phase I clinical trials. Biometrics. 1989;45:925–37.
Rijneveld AW, Holt B, Weerdt O, Biemond BJ, Loosdrecht A, Petersen E, et al. Clofarabine added to standard treatment in adult patients with newly diagnosed ALL: first results of the randomized phase III HOVON-100 Study. Blood. 2017;130(Supplement 1):2606.
Koller CA, Kantarjian HM, Thomas D, O’Brien S, Rios MB, Kornblau S, et al. The hyper-CVAD regimen improves outcome in relapsed acute lymphoblastic leukemia. Leukemia. 1997;11:2039–44.
Camera A, Annino L, Chiurazzi F, Fazi P, Cascavilla N, Fabbiano F, et al. GIMEMA ALL—rescue 97: a salvage strategy for primary refractory or relapsed adult acute lymphoblastic leukemia. Haematologica. 2004;89:145–53.
Specchia G, Pastore D, Carluccio P, Liso A, Mestice A, Rizzi R, et al. FLAG-IDA in the treatment of refractory/relapsed adult acute lymphoblastic leukemia. Ann Hematol. 2005;84:792–5.
Möttönen M, Uhari M, Lanning M, Tuokko H. Prospective controlled survey of viral infections in children with acute lymphoblastic leukemia during chemotherapy. Cancer. 1995;75:1712–7.
Jabbour E, Ravandi F, Kebriaei P, Huang X, Short NJ, Thomas D, et al. Salvage chemoimmunotherapy with inotuzumab ozogamicin combined with mini-hyper-CVD for patients with relapsed or refractory Philadelphia chromosome-negative acute lymphoblastic leukemia: a phase 2 clinical trial. JAMA Oncol. 2018;4:230–4.
Gossai N, Verneris MR, Karras NA, Gorman MF, Patel NJ, Burke MJ. A clofarabine-based bridging regimen in patients with relapsed ALL and persistent minimal residual disease (MRD). Bone Marrow Transplant. 2014;49:440–2.
Acknowledgements
The authors thank all investigators and members of participating hospitals in ALL studies conducted by the JALSG.
Funding
This work was supported in part by a grant for Practical Research for Innovative Cancer Control Grant No. JP19ck0106331 from the Japan Agency for Medical Research and Development (AMED).
Author information
Authors and Affiliations
Consortia
Contributions
Administrative support: all authors. Conception and design: all authors. Provision of study materials or patients: all authors. Collection and assembly of data: AMS. Data analysis and interpretation: AH. Manuscript writing: all authors. Final approval of manuscript: all authors.
Corresponding author
Ethics declarations
Conflict of interest
Hitoshi Kiyoi reports research funding from Chugai Pharmaceutical, Kyowa Kirin, Zenyaku Kogyo, FUJIFILM, Daiichi Sankyo, Astellas Pharma, Otsuka Pharmaceutical, Nippon Shinyaku, Eisai, Pfizer Japan, Takeda Pharmaceutical, Novartis Pharma, Sumitomo Dainippon Pharma, Sanofi, Perseus Proteomics and Celgene, and consulting fees from Astellas Pharma, Amgen Astellas BioPharma, and Daiichi Sankyo, and honoraria from Bristol-Myers Squibb, Astellas Pharma, and Novartis Pharma. Yasushi Miyazaki reports research funding from Sumitomo Dainippon Pharma, Pfizer Japan, Chugai Pharmaceutical, and Takeda Pharmaceutical, and honoraria from Chugai Pharmaceutical, Kyowa Kirin, Astellas Pharma, Otsuka Pharmaceutical, Nippon Shinyaku, Novartis Pharma, Sumitomo Dainippon Pharma, and Celgene. Other authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
About this article

Cite this article
Saito, T., Hatta, Y., Hayakawa, F. et al. Combination of clofarabine, etoposide, and cyclophosphamide in adult relapsed/refractory acute lymphoblastic leukemia: a phase 1/2 dose-escalation study by the Japan Adult Leukemia Study Group. Int J Hematol 113, 395–403 (2021). https://doi.org/10.1007/s12185-020-03032-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12185-020-03032-3