
Abstract
Diastolic dysfunction encompasses both those who are asymptomatic and those who have heart failure symptoms. Preclinical diastolic dysfunction (PDD), defined as diastolic dysfunction with preserved ejection fraction (EF) without the presence of heart failure symptoms, is prevalent and may progress to heart failure with preserved EF (HFpEF). While the causative factors of HFpEF are multifactorial, targeting PDD and its associated comorbidities prior to development of symptoms can reduce development of heart failure. Diabetes, coronary artery disease, hypertension, and renal dysfunction are targets of treatment in those with diastolic dysfunction that may decrease the risk of heart failure development. This review will focus on PDD, its epidemiology, pathophysiology, comorbid conditions, and management that may prevent development of heart failure.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Heart failure (HF) affects over five million American adults, and projected estimates show growth of this epidemic by 25 % over the next 15 years as the population of the USA continues to age [1]. While the underlying pathophysiology of heart failure encompasses both systolic and diastolic dysfunction, heart failure itself is a clinical diagnosis [2]. One classification system for heart failure is reliant on the ejection fraction (EF), where in patients with symptoms of heart failure, an EF of <40 % is termed heart failure with reduced ejection fraction (HFrEF) and an EF of ≥50 % is termed heart failure with preserved EF (HFpEF). HFpEF encompasses approximately half of all heart failure cases [3].
In contemporary heart failure literature, the terms systolic heart failure and diastolic heart failure have lost popularity, given the multifactorial contributions to heart failure development, as well as the fact that diastolic dysfunction may be present in both HFrEF and HFpEF [4]. Therefore, the term HFpEF has largely replaced diastolic heart failure, recognizing that many factors, not just diastolic dysfunction, contribute to HFpEF. Additionally, while all patients with HFrEF have systolic dysfunction, a large proportion has concomitant diastolic dysfunction [5].
Classification of Heart Failure Development and Progression
The four stages of heart failure as per the American College of Cardiology Foundation and American Heart Association (ACCF/AHA) classification reflect the risk associated with development and progression of structural heart disease to symptomatic heart failure [6]. Stages A and B reflect asymptomatic disease, and stages C and D reflect symptomatic heart failure. Stage A is defined as high risk for HF development based on comorbid conditions, without structural heart disease. Stage B is defined as structural heart disease, such as systolic or diastolic dysfunction identified on cardiac imaging, without signs or symptoms of HF. Stages C and D are defined as symptomatic HF and disease refractory to treatment, respectively.
Therefore, stage A encompasses those with comorbid cardiac conditions at high risk of HF development, and stage B includes preclinical diastolic dysfunction. Targeting diastolic dysfunction is essential as there is known progression from stage A and B to stage C and D heart failure [7]. Furthermore, there is rapid increase in mortality and reduction in quality of life with progression from HF stages A to D [8, 9].
Diastolic Dysfunction Defined
The gold standard for evaluation of diastolic dysfunction is invasive hemodynamic measurements with cardiac catheterization, characterizing the rate of left ventricular pressure decline, time constant of left ventricular relaxation tau, and the stiffness modulus. In clinical practice, however, invasive measurements for diastolic dysfunction are generally not performed given the availability of noninvasive, accurate, and efficient measurements of diastolic function with imaging modalities. The use of echocardiography, as well as more recent cardiac magnetic resonance imaging (CMR), allows for determination of the stiffness and relaxation of the heart. With Doppler echocardiography, the early (E) and atrial (A) phases of diastolic left ventricular filling can be characterized. Furthermore, the mitral annulus velocity (e′) during diastole can be measured with tissue Doppler. The E/e′ reflects left ventricular filling pressures, and the E/A ratio is an estimate of the ventricular relaxation pattern [10]. More recently, strain rate imaging has also been employed to better characterize cardiac deformity [11]. CMR offers improved spatial resolution compared to traditional echocardiography, and there has been increasing interest in its use in diastolic function assessment [12].
The American Society of Echocardiography (ASE) classification of diastolic dysfunction based on Doppler echocardiography is as follows: grade Ia (mild, impaired relaxation), grade II (moderate, evidence of elevation of filling pressures), and grades III and IV (severe, reversible, or fixed reduction in compliance) [13].
Pathophysiology of Diastolic Dysfunction
Diastole, the phase where the left ventricle fills with blood, is dependent on the interaction of numerous factors including ventricular relaxation and ventricular stiffness. Simplified, diastole can be thought of as the following components: isovolumetric relaxation, rapid and slow filling, and atrial contraction [14]. The contribution of the atrial “kick” component is highly dependent on left atrial pressures as well as ventricular compliance. Diastolic dysfunction can consist of abnormality in one or more of these diastolic components and is characterized by abnormal relaxation with or without elevations in left atrial filling pressures. Diastolic dysfunction stems from disorder of myocytes, extracellular matrix, and ventricular vascular coupling.
Understanding how intracellular myocyte disorder affects diastolic function contributes to potential treatment targets. These include changes in titin or microtubules, calcium handling and sensitivity, cardiomyocyte infiltration, and neurohormonal as well as endothelial dysfunction [15–17]. Both animal and human studies have found that in an inflammatory and oxidative stress state, lack of nitric oxide synthase, titin isoform shifts, and myosin binding protein C phosphorylation contribute to diastolic dysfunction [18–21]. In the later stages of diastolic dysfunction, concentric remodeling occurs, with cardiomyocytes that become thicker and less compliant.
Extracellular matrix disorder also contributes to diastolic dysfunction via changes in ventricular compliance. Excess collagen leads to increased myocardial stiffness [22]. From a cellular and molecular perspective, extracellular matrix changes may precede detection of gross hypertrophy and increased wall thickness [23]. And, while there may initially be normal left ventricular geometry at rest, abnormal left ventricular cavity dimensions may be elicited with exercise [24].
Studies of HFpEF suggest that diastolic dysfunction also stems from dysfunction of ventricular and vascular coupling. Normally, the left ventricular stiffness is intricately coupled with systemic resistance. However, with dysfunction in left ventricular and arterial stiffness, the dynamic Starling mechanisms that govern this relationship are impaired and ventricular stiffness increases disproportionately more than arterial stiffness [25, 26].
In summary, diastolic physiology is dependent on ventricular relaxation and compliance, and dysfunction occurs when there is disorder of myocytes, extracellular matrix, and the relationship between ventricular and vascular interaction.
Epidemiology of Preclinical Diastolic Dysfunction
Recent studies have focused on improving the epidemiologic understanding of preclinical diastolic dysfunction (PDD), to identify risk factors and associated comorbidities. In the general adult population, through echocardiographical assessment of diastolic function, the prevalence of mild PDD is approximately 21 %, and that of moderate to severe PDD is approximately 7 % [5, 9].
Advanced age was found to be associated with an increased prevalence of PDD. In an analysis of 1038 subjects with mean age of 76 years from the Framingham Heart Study, 36 % had PDD [27]. Similarly, in a study of 2001 subjects between the ages of 65 and 84 years from an Italian population, PDD was found to have prevalence of 35 % [28].
The presence of cardiovascular comorbidities, including hypertension, myocardial infarction, coronary artery disease, diabetes, and obesity, led to increased prevalence of PDD. Redfield et al. found that in the elderly with hypertension or coronary artery disease, the prevalence of mild PDD increased to 48 % and of moderate to severe PDD increased to 17 % [5]. Similarly, Abhayaratna et al. identified hypertension, myocardial infarction, coronary artery disease, obesity, and diabetes as predictors of diastolic dysfunction development [9].
Hence, the epidemiological studies demonstrated that PDD is prevalent in the general adult population and becomes even more prevalent in the setting of advanced age and cardiovascular comorbidities.
Natural History of Preclinical Diastolic Dysfunction
Those with PDD may develop symptoms and thus progress to symptomatic heart failure. Studies have demonstrated the 1-year incidence of HF development as being approximately 2 % [7, 29]. By 3 years, the incidence of HF development increases to 12 % [29].
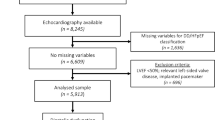
There are two major factors associated with increased incidence of heart failure development. First, worsening diastolic dysfunction is associated with increased risk of HF development. Second, the presence of comorbid conditions is also predictive of HF development (Fig. 1). These findings have important treatment implications.

Heart failure risk, development, and progression based on the American College of Cardiology Foundation and American Heart Association heart failure staging (reprinted from the Journal of the American College of Cardiology, vol 63 no 5, Siu-Hin Wan, Mark W. Vogel, and Horng H. Chen, Pre-Clinical Diastolic Dysfunction, 407–416, Copyright (2014), with permission from Elsevier)
The severity of diastolic dysfunction, based on diastolic grade, was directly associated with the risk of progression to symptomatic heart failure, as evidenced by the increased risk of incident HF hospitalization and death associated with moderate to severe left ventricular diastolic dysfunction [30]. Kane et al. found that over a 6-year period, in those with normal diastolic function, the incidence of progression to HF was 3 %. In those with mild diastolic dysfunction, the incidence of progression from PDD to HF was 8 %. However, in those with diastolic dysfunction that was moderate to severe, the incidence of progression from PDD to HF was 12 % [7].
Cardiac comorbid conditions also drive progression of PDD to symptomatic heart failure. Correa de Sa et al. found that hypertension (hazard ratio 11) and peripheral vascular disease (hazard ratio 7) were associated with increased HF development [31]. Diabetes mellitus is also an important condition associated with increased HF progression. From et al. found that subjects with diabetes and diastolic dysfunction had a 37 % risk of HF development over 5 years, compared to 17 % in those with diabetes alone [32].
Systemic comorbidities such as renal, pulmonary, or hematological impairment are associated with worsening diastolic function and also lead to increased risk of heart failure development [29]. Additionally, systemic comorbidities lead to decreased cardiopulmonary reserve and increase the likelihood of development of symptomatic HF. Those with systemic comorbid conditions, namely, renal, pulmonary, or hematological impairment, have an increased risk of progression from PDD to HF of 10 % over a 4-year period [27].
Renal function has previously been extensively reported as associated with heart failure progression. Impairment in renal endocrine response and subsequent fluid overload play a vital pathophysiological role in HF development [33]. Vogel et al. found that renal dysfunction was independently associated with HF development, and in those with GFR <60 mL/min/1.73 m2 compared to those with normal renal function, there was a hazard ratio of 2 for HF development [29].
Management of Preclinical Diastolic Dysfunction and Preventing Heart Failure Development
The findings from the Natural History section reinforce that the progression of diastolic dysfunction to symptomatic heart failure is dependent on both severity of diastolic dysfunction as well as associated comorbidities, and therefore, treatment should focus both on preventing or reversing diastolic dysfunction and on treatment of important comorbid conditions [27].
Targeting Diastolic Dysfunction
Based on the underlying pathophysiology of diastolic dysfunction, pharmacological options for treating diastolic dysfunction and preventing HF development focus on agents that act on the myocyte, on the extracellular matrix with cardiac remodeling, or on the ventricular vascular interaction.
Intracellular acting agents and extracellular matrix agents that have been studied include drugs that modulate calcium, nitric oxide, aldosterone, and natriuretic peptides. Ranolazine has been studied for its intracellular calcium effects, tetrahydrobiopterin for its nitric oxide effects, and tranilast for its antifibrotic effects. Additional pharmacological agents currently under investigation and that have shown promise include ivabradine (reduces cardiac hypertrophy and fibrosis), endothelial nitric oxide synthase activators, matrix metalloproteinase 9 inhibitors, alagebrium (reducing advanced glycation end products), and anakinra (interleukin 1 receptor antagonist) [34]. In recent studies, ranolazine, tetrahydrobiopterin, tranilast, and ivabradine have been shown to improve diastolic dysfunction and/or reduce fibrosis [35–38]. However, further research is needed at this time to evaluate if these medications not only improve diastolic function but also ultimately prevent heart failure development.
The Treatment of Preserved Cardiac Function Heart Failure with an Aldosterone Antagonist (TOPCAT) trial found that in those with preserved ejection fraction, treatment with spironolactone did not significantly reduce the cardiovascular composite end point including death but did significantly reduce heart failure hospitalization, likely due to fibrosis and hypertrophy reversal [39]. However, further information is needed regarding their use in preventing HF development [40].
Clarkson et al. demonstrated that in patients with HFpEF, the infusion of B-type natriuretic peptide (BNP) resulted in hemodynamic enhancement and beneficial neurohormonal effects in response to exercise [41]. The administration of BNP for stable chronic heart failure has been investigated, given BNP’s inhibitory effects on left ventricular fibrosis and myocyte hypertrophy [42]. Acute BNP administration in subjects with PDD also results in improvement in fluid balance via renal natriuresis enhancement [33]. The use of chronic BNP administration has been demonstrated to have improvement in diastolic parameters and improvement in left ventricular remodeling and may be a potential therapy for prevention of heart failure development [43].
LCZ696, a combined angiotensin receptor and neprilysin inhibitor, has received much attention in treatment of heart failure with reduced ejection fraction, demonstrating reduction in death and HF hospitalization in this population when compared to enalapril [44]. This compound is also being studied in those with HFpEF, and it was found that among those who received LZC696 versus valsartan, they had greater reduction of NT-proBNP levels over 12 weeks [45]. Further studies are needed to evaluate whether LCZ696 can not only treat heart failure but also prevent development of heart failure.
Given the ventricular vascular coupling pathophysiology of diastolic dysfunction, the renin-angiotensin-aldosterone pathway has been a prime focus for potential therapeutic targets. Angiotensin-converting enzyme inhibitors (ACEIs) have been extensively studied in the setting of diastolic function, and it has been demonstrated that left ventricular hypertrophy may regress with ACEI treatment [46]. Additional human studies have also suggested that combination therapy with ACEI and diuretics further improves diastolic dysfunction, which may reduce heart failure development risk, although this remains to be further studied [47].
Beta blockers have also been of great interest in preventing HF, and while outcome data regarding HFpEF development remain poorly defined, there is evidence of improved diastolic function with beta blocker use [48]. Phosphodiesterase-5 (PDE5) inhibition has been of great interest as in vitro and animal studies have shown promise for use of this agent as a treatment strategy for diastolic dysfunction. However, in a large human trial (RELAX), PDE5 inhibition did not improve clinical outcomes in HFpEF [49, 50].
Targeting Comorbid Conditions
The Screening to Prevent Heart Failure (STOP-HF) trial focused on strategies to reduce heart failure development and found that using a BNP-based screening strategy, patients at risk of development of ventricular dysfunction and heart failure were more likely to be identified [51]. The study included over 1000 subjects from multiple outpatient practices in Ireland, which are over 40 years old with cardiovascular comorbidities including hypertension, hyperlipidemia, obesity, vascular disease, diabetes, arrhythmias, or valvular disease. Among those in the intervention group and found to be at higher risk as defined by elevated BNP levels (>50 pg/mL), greater use of renin-angiotensin-aldosterone agents led to reduction in development of diastolic dysfunction and incident heart failure [51]. The STOP-HF suggests that targeting comorbidities among those at risk of heart failure development may reduce the risk of worsening ventricular dysfunction and symptomatic heart failure development.
Important cardiac and systemic comorbidities to target include hypertension, peripheral vascular disease, diabetes mellitus, renal dysfunction, chronic obstructive disease (COPD), coronary artery disease (CAD), anemia, and obesity.
Multiple agents have been studied for the treatment of hypertension and CAD. Especially among those with hypertension, ACEI has been demonstrated in human studies to reduce the risk of heart failure development [52]. Given the importance of targeting hypertension, diuretics and calcium channel blockers have also been studied in addition to ACEI. In hypertensive individuals, diuretics have been shown to prevent heart failure development [53].
Those with diabetes mellitus may develop diabetic cardiomyopathy via both intracellular and extracellular matrix changes that result in structural and functional cardiac impairment. Strict glycemic control and blood pressure control are essential [54, 55]. The beneficial effects of ACEI and beta blockers have also been extensively studied in the setting of diabetes mellitus [56].
Renal dysfunction has been shown to portend a worse prognosis among those with heart failure [57]. Similar to those with diabetes, ACEI has been demonstrated to be a cornerstone of renal dysfunction treatment and is important in reducing heart failure progression [58]. In renal dysfunction, given reports of beneficial cardiovascular effects of vitamin D, this agent has been studied as a potential therapeutic option for reduction of diastolic dysfunction. However, the PRIMO randomized trial failed to find structural and diastolic improvements with chronic vitamin D therapy [59].
COPD and anemia treatment, given its pathophysiological involvement in heart failure development, may also reduce risk of incident HF. World Health Organization group III pulmonary hypertension describes the association of lung disease with pulmonary hypertension and subsequent development of right-sided heart failure. Anemia has been linked with poor outcomes among those with HF, and the study of iron deficiency remains ongoing among those with heart failure [60–62]. While there is a lack of studies directly looking at treatment of these comorbidities in HF, the pathophysiological implications suggest that guideline-directed treatment of these conditions may reduce heart failure development.
Obesity has been associated with heart failure development and highlights the importance of targeting this epidemic in the general adult population [63]. In the heart failure population, there has been a reported “obesity paradox,” in which higher body mass indices (BMIs) were associated with decreased mortality in heart failure. However, this may be from earlier HF identification in those who are obese with more medical care utilization and further highlights the importance of early identification of PDD subjects in the population [64]. Exercise, long term and in moderation, has been demonstrated to improve functional capacity in those with chronic HF [65].
In summary, targeting the cardiovascular and systemic comorbidities of hypertension, coronary artery disease, diabetes mellitus, renal dysfunction, COPD, anemia, and obesity is essential in the prevention of heart failure development and progression.
Conclusions and Further Research
Compared to HFrEF, there has been a relative paucity of evidence-based treatment strategies for HFpEF. What is known is that PDD is prevalent, and there is significant progression to symptomatic HF, especially among the high-risk elderly population. Both diastolic dysfunction and comorbid conditions contribute to heart failure development and progression. The underlying pathophysiology of diastolic dysfunction, based on intracellular matrix, extracellular matrix, and ventricular vascular coupling, guides treatment targets to reverse or halt worsening diastolic function. Further studies are needed to better characterize preclinical diastolic dysfunction and to discover further targets for this entity to prevent development of HFpEF. In addition, given heart failure as a systemic condition, studies targeting relevant diastolic dysfunction comorbid conditions, such as diabetes and renal dysfunction, are important for preventing heart failure development. In addition to clinical studies, further mechanistic studies are also necessary in preclinical diastolic dysfunction to guide strategies for heart failure prevention.
References
Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Borden WB, et al. Heart disease and stroke statistics–2013 update: a report from the American Heart Association. Circulation. 2013;127(1):e6–245. doi:10.1161/CIR.0b013e31828124ad.
McKee PA, Castelli WP, McNamara PM, Kannel WB. The natural history of congestive heart failure: the Framingham study. N Engl J Med. 1971;285(26):1441–6.
Bursi F, Weston SA, Redfield MM, Jacobsen SJ, Pakhomov S, Nkomo VT, et al. Systolic and diastolic heart failure in the community. JAMA. 2006;296(18):2209–16. doi:10.1001/jama.296.18.2209.
Paulus WJ, Tschope C. A novel paradigm for heart failure with preserved ejection fraction: comorbidities drive myocardial dysfunction and remodeling through coronary microvascular endothelial inflammation. J Am Coll Cardiol. 2013. doi:10.1016/j.jacc.2013.02.092.
Redfield MM, Jacobsen SJ, Burnett Jr JC, Mahoney DW, Bailey KR, Rodeheffer RJ. Burden of systolic and diastolic ventricular dysfunction in the community: appreciating the scope of the heart failure epidemic. JAMA. 2003;289(2):194–202.
Jessup M, Abraham WT, Casey DE, Feldman AM, Francis GS, Ganiats TG, et al. 2009 focused update: ACCF/AHA Guidelines for the Diagnosis and Management of Heart Failure in Adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the International Society for Heart and Lung Transplantation. Circulation. 2009;119(14):1977–2016.
Kane GC, Karon BL, Mahoney DW, Redfield MM, Roger VL, Burnett Jr JC, et al. Progression of left ventricular diastolic dysfunction and risk of heart failure. JAMA. 2011;306(8):856–63. doi:10.1001/jama.2011.1201.
Wan SH, Vogel MW, Chen HH. Pre-clinical diastolic dysfunction. J Am Coll Cardiol. 2014;63(5):407–16. doi:10.1016/j.jacc.2013.10.063.
Abhayaratna WP, Marwick TH, Smith WT, Becker NG. Characteristics of left ventricular diastolic dysfunction in the community: an echocardiographic survey. Heart. 2006;92(9):1259–64.
Ommen SR, Nishimura RA, Appleton CP, Miller FA, Oh JK, Redfield MM, et al. Clinical utility of Doppler echocardiography and tissue Doppler imaging in the estimation of left ventricular filling pressures: a comparative simultaneous Doppler-catheterization study. Circulation. 2000;102(15):1788–94.
Sutherland GR, Di Salvo G, Claus P, D’Hooge J, Bijnens B. Strain and strain rate imaging: a new clinical approach to quantifying regional myocardial function. J Am Soc Echocardiogr. 2004;17(7):788–802. doi:10.1016/j.echo.2004.03.027.
Caudron J, Fares J, Bauer F, Dacher JN. Evaluation of left ventricular diastolic function with cardiac MR imaging. Radiographics. 2011;31(1):239–59. doi:10.1148/rg.311105049.
Nagueh SF, Appleton CP, Gillebert TC, Marino PN, Oh JK, Smiseth OA, et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography. J Am Soc Echocardiogr. 2009;22(2):107–33. doi:10.1016/j.echo.2008.11.023.
Nishimura RA, Tajik AJ. Evaluation of diastolic filling of left ventricle in health and disease: Doppler echocardiography is the clinician’s Rosetta Stone. J Am Coll Cardiol. 1997;30(1):8–18.
Cazorla O, Freiburg A, Helmes M, Centner T, McNabb M, Wu Y, et al. Differential expression of cardiac titin isoforms and modulation of cellular stiffness. Circ Res. 2000;86(1):59–67.
Gaasch WH, Zile MR. Left ventricular diastolic dysfunction and diastolic heart failure. Annu Rev Med. 2004;55:373–94.
Kass DA, Bronzwaer JG, Paulus WJ. What mechanisms underlie diastolic dysfunction in heart failure? Circ Res. 2004;94(12):1533–42.
Berg TJ, Snorgaard O, Faber J, Torjesen PA, Hildebrandt P, Mehlsen J, et al. Serum levels of advanced glycation end products are associated with left ventricular diastolic function in patients with type 1 diabetes. Diabetes Care. 1999;22(7):1186–90.
Silberman GA, Fan TH, Liu H, Jiao Z, Xiao HD, Lovelock JD, et al. Uncoupled cardiac nitric oxide synthase mediates diastolic dysfunction. Circulation. 2010;121(4):519–28. doi:10.1161/CIRCULATIONAHA.109.883777.
van Heerebeek L, Borbely A, Niessen HW, Bronzwaer JG, van der Velden J, Stienen GJ, et al. Myocardial structure and function differ in systolic and diastolic heart failure. Circulation. 2006;113(16):1966–73. doi:10.1161/CIRCULATIONAHA.105.587519.
Flashman E, Redwood C, Moolman-Smook J, Watkins H. Cardiac myosin binding protein C: its role in physiology and disease. Circ Res. 2004;94(10):1279–89. doi:10.1161/01.RES.0000127175.21818.C2.
Borlaug BA, Paulus WJ. Heart failure with preserved ejection fraction: pathophysiology, diagnosis, and treatment. Eur Heart J. 2011;32(6):670–9. doi:10.1093/eurheartj/ehq426.
Hamdani N, Bishu KG, von Frieling-Salewsky M, Redfield MM, Linke WA. Deranged myofilament phosphorylation and function in experimental heart failure with preserved ejection fraction. Cardiovasc Res. 2013;97(3):464–71. doi:10.1093/cvr/cvs353.
Borlaug BA. The pathophysiology of heart failure with preserved ejection fraction. Nat Rev Cardiol. 2014;11(9):507–15. doi:10.1038/nrcardio.2014.83.
Borlaug BA, Kass DA. Ventricular-vascular interaction in heart failure. Heart Fail Clin. 2008;4(1):23–36. doi:10.1016/j.hfc.2007.10.001.
Kawaguchi M, Hay I, Fetics B, Kass DA. Combined ventricular systolic and arterial stiffening in patients with heart failure and preserved ejection fraction: implications for systolic and diastolic reserve limitations. Circulation. 2003;107(5):714–20.
Lam CS, Lyass A, Kraigher-Krainer E, Massaro JM, Lee DS, Ho JE, et al. Cardiac dysfunction and noncardiac dysfunction as precursors of heart failure with reduced and preserved ejection fraction in the community. Circulation. 2011;124(1):24–30. doi:10.1161/CIRCULATIONAHA.110.979203.
Mureddu GF, Agabiti N, Rizzello V, Forastiere F, Latini R, Cesaroni G, et al. Prevalence of preclinical and clinical heart failure in the elderly. A population-based study in Central Italy. Eur J Heart Fail. 2012;14(7):718–29. doi:10.1093/eurjhf/hfs052.
Vogel MW, Slusser JP, Hodge DO, Chen HH. The natural history of preclinical diastolic dysfunction: a population-based study. Circ Heart Fail. 2012;5(2):144–51. doi:10.1161/CIRCHEARTFAILURE.110.959668.
Ren X, Ristow B, Na B, Ali S, Schiller NB, Whooley MA. Prevalence and prognosis of asymptomatic left ventricular diastolic dysfunction in ambulatory patients with coronary heart disease. Am J Cardiol. 2007;99(12):1643–7.
Correa de Sa DD, Hodge DO, Slusser JP, Redfield MM, Simari RD, Burnett JC, et al. Progression of preclinical diastolic dysfunction to the development of symptoms. Heart. 2010;96(7):528–32. doi:10.1136/hrt.2009.177980.
From AM, Scott CG, Chen HH. The development of heart failure in patients with diabetes mellitus and pre-clinical diastolic dysfunction a population-based study. J Am Coll Cardiol. 2010;55(4):300–5.
McKie PM, Schirger JA, Costello-Boerrigter LC, Benike SL, Harstad LK, Bailey KR, et al. Impaired natriuretic and renal endocrine response to acute volume expansion in pre-clinical systolic and diastolic dysfunction. J Am Coll Cardiol. 2011;58(20):2095–103. doi:10.1016/j.jacc.2011.07.042.
Zouein FA, de Castro Bras LE, da Costa DV, Lindsey ML, Kurdi M, Booz GW. Heart failure with preserved ejection fraction: emerging drug strategies. J Cardiovasc Pharmacol. 2013;62(1):13–21. doi:10.1097/FJC.0b013e31829a4e61.
Lovelock JD, Monasky MM, Jeong EM, Lardin HA, Liu H, Patel BG, et al. Ranolazine improves cardiac diastolic dysfunction through modulation of myofilament calcium sensitivity. Circ Res. 2012;110(6):841–50. doi:10.1161/CIRCRESAHA.111.258251.
Moens AL, Takimoto E, Tocchetti CG, Chakir K, Bedja D, Cormaci G, et al. Reversal of cardiac hypertrophy and fibrosis from pressure overload by tetrahydrobiopterin: efficacy of recoupling nitric oxide synthase as a therapeutic strategy. Circulation. 2008;117(20):2626–36. doi:10.1161/CIRCULATIONAHA.107.737031.
Kelly DJ, Zhang Y, Connelly K, Cox AJ, Martin J, Krum H, et al. Tranilast attenuates diastolic dysfunction and structural injury in experimental diabetic cardiomyopathy. Am J Physiol Heart Circ Physiol. 2007;293(5):H2860–9. doi:10.1152/ajpheart.01167.2006.
Busseuil D, Shi Y, Mecteau M, Brand G, Gillis MA, Thorin E, et al. Heart rate reduction by ivabradine reduces diastolic dysfunction and cardiac fibrosis. Cardiology. 2010;117(3):234–42. doi:10.1159/000322905.
Pitt B, Pfeffer MA, Assmann SF, Boineau R, Anand IS, Claggett B, et al. Spironolactone for heart failure with preserved ejection fraction. N Engl J Med. 2014;370(15):1383–92. doi:10.1056/NEJMoa1313731.
Edelmann F, Wachter R, Schmidt AG, Kraigher-Krainer E, Colantonio C, Kamke W, et al. Effect of spironolactone on diastolic function and exercise capacity in patients with heart failure with preserved ejection fraction: the Aldo-DHF randomized controlled trial. JAMA. 2013;309(8):781–91. doi:10.1001/jama.2013.905.
Clarkson PB, Wheeldon NM, MacFadyen RJ, Pringle SD, MacDonald TM. Effects of brain natriuretic peptide on exercise hemodynamics and neurohormones in isolated diastolic heart failure. Circulation. 1996;93(11):2037–42.
Tamura N, Ogawa Y, Chusho H, Nakamura K, Nakao K, Suda M, et al. Cardiac fibrosis in mice lacking brain natriuretic peptide. Proc Natl Acad Sci U S A. 2000;97(8):4239–44. doi:10.1073/pnas.070371497.
Chen HH, Glockner JF, Schirger JA, Cataliotti A, Redfield MM, Burnett Jr JC. Novel protein therapeutics for systolic heart failure: chronic subcutaneous B-type natriuretic peptide. J Am Coll Cardiol. 2012;60(22):2305–12. doi:10.1016/j.jacc.2012.07.056.
McMurray JJ, Packer M, Desai AS, Gong J, Lefkowitz MP, Rizkala AR, et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med. 2014;371(11):993–1004. doi:10.1056/NEJMoa1409077.
Solomon SD, Zile M, Pieske B, Voors A, Shah A, Kraigher-Krainer E, et al. The angiotensin receptor neprilysin inhibitor LCZ696 in heart failure with preserved ejection fraction: a phase 2 double-blind randomised controlled trial. Lancet. 2012. doi:10.1016/S0140-6736(12)61227-6.
Devereux RB, Palmieri V, Sharpe N, De Quattro V, Bella JN, de Simone G, et al. Effects of once-daily angiotensin-converting enzyme inhibition and calcium channel blockade-based antihypertensive treatment regimens on left ventricular hypertrophy and diastolic filling in hypertension: the prospective randomized enalapril study evaluating regression of ventricular enlargement (preserve) trial. Circulation. 2001;104(11):1248–54.
Yip GW, Wang M, Wang T, Chan S, Fung JW, Yeung L, et al. The Hong Kong diastolic heart failure study: a randomised controlled trial of diuretics, irbesartan and ramipril on quality of life, exercise capacity, left ventricular global and regional function in heart failure with a normal ejection fraction. Heart. 2008;94(5):573–80. doi:10.1136/hrt.2007.117978.
Bergstrom A, Andersson B, Edner M, Nylander E, Persson H, Dahlstrom U. Effect of carvedilol on diastolic function in patients with diastolic heart failure and preserved systolic function. Results of the Swedish Doppler-echocardiographic study (SWEDIC). Eur J Heart Fail. 2004;6(4):453–61. doi:10.1016/j.ejheart.2004.02.003.
Westermann D, Becher PM, Lindner D, Savvatis K, Xia Y, Frohlich M, et al. Selective PDE5A inhibition with sildenafil rescues left ventricular dysfunction, inflammatory immune response and cardiac remodeling in angiotensin II-induced heart failure in vivo. Basic Res Cardiol. 2012;107(6):308. doi:10.1007/s00395-012-0308-y.
Redfield MM, Chen HH, Borlaug BA, et al. Effect of phosphodiesterase-5 inhibition on exercise capacity and clinical status in heart failure with preserved ejection fraction: a randomized clinical trial. JAMA. 2013:1–10. doi:10.1001/jama.2013.2024
Ledwidge M, Gallagher J, Conlon C, Tallon E, O’Connell E, Dawkins I, et al. Natriuretic peptide-based screening and collaborative care for heart failure: the STOP-HF randomized trial. JAMA. 2013;310(1):66–74. doi:10.1001/jama.2013.7588.
Arnold JM, Yusuf S, Young J, Mathew J, Johnstone D, Avezum A, et al. Prevention of heart failure in patients in the heart outcomes prevention evaluation (HOPE) study. Circulation. 2003;107(9):1284–90.
Davis BR, Piller LB, Cutler JA, Furberg C, Dunn K, Franklin S, et al. Role of diuretics in the prevention of heart failure: the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial. Circulation. 2006;113(18):2201–10. doi:10.1161/CIRCULATIONAHA.105.544031.
The Diabetes Control and Complications Trial (DCCT) Research Group. Effect of intensive diabetes management on macrovascular events and risk factors in the Diabetes Control and Complications Trial. Am J Cardiol. 1995;75(14):894–903.
Zhang X, Chen C. A new insight of mechanisms, diagnosis and treatment of diabetic cardiomyopathy. Endocrine. 2012;41(3):398–409. doi:10.1007/s12020-012-9623-1.
Hayat SA, Patel B, Khattar RS, Malik RA. Diabetic cardiomyopathy: mechanisms, diagnosis and treatment. Clin Sci (Lond). 2004;107(6):539–57. doi:10.1042/CS20040057.
Gottlieb SS, Abraham W, Butler J, Forman DE, Loh E, Massie BM, et al. The prognostic importance of different definitions of worsening renal function in congestive heart failure. J Card Fail. 2002;8(3):136–41.
Ljungman S, Kjekshus J, Swedberg K. Renal function in severe congestive heart failure during treatment with enalapril (the Cooperative North Scandinavian Enalapril Survival Study [CONSENSUS] Trial). Am J Cardiol. 1992;70(4):479–87.
Thadhani R, Appelbaum E, Pritchett Y, Chang Y, Wenger J, Tamez H, et al. Vitamin D therapy and cardiac structure and function in patients with chronic kidney disease: the PRIMO randomized controlled trial. JAMA. 2012;307(7):674–84. doi:10.1001/jama.2012.120.
Ezekowitz JA, McAlister FA, Armstrong PW. Anemia is common in heart failure and is associated with poor outcomes: insights from a cohort of 12 065 patients with new-onset heart failure. Circulation. 2003;107(2):223–5.
Bolger AP, Bartlett FR, Penston HS, O’Leary J, Pollock N, Kaprielian R, et al. Intravenous iron alone for the treatment of anemia in patients with chronic heart failure. J Am Coll Cardiol. 2006;48(6):1225–7. doi:10.1016/j.jacc.2006.07.015.
Anker SD, Comin Colet J, Filippatos G, Willenheimer R, Dickstein K, Drexler H, et al. Ferric carboxymaltose in patients with heart failure and iron deficiency. N Engl J Med. 2009;361(25):2436–48. doi:10.1056/NEJMoa0908355.
Kenchaiah S, Evans JC, Levy D, Wilson PW, Benjamin EJ, Larson MG, et al. Obesity and the risk of heart failure. N Engl J Med. 2002;347(5):305–13. doi:10.1056/NEJMoa020245.
Curtis JP, Selter JG, Wang Y, Rathore SS, Jovin IS, Jadbabaie F, et al. The obesity paradox: body mass index and outcomes in patients with heart failure. Arch Intern Med. 2005;165(1):55–61. doi:10.1001/archinte.165.1.55.
Belardinelli R, Georgiou D, Cianci G, Purcaro A. Randomized, controlled trial of long-term moderate exercise training in chronic heart failure: effects on functional capacity, quality of life, and clinical outcome. Circulation. 1999;99(9):1173–82.
Acknowledgments
Dr. Chen received Research Grants from the National Institutes of Health PO1 HL 76611, R01 HL-84155, and Scios, Inc.; Mayo Clinic has filed patents for chimeric natriuretic peptides; Mayo Clinic has licensed patents to Capricor Therapeutics and Anexon with other patents pending at the US patent office; Dr. Chen received royalties from Capricor Therapeutics, Anexon, Inc., and UpToDate and is the cofounder of Zumbro Discovery, Inc.
Compliance with Ethics Guidelines
ᅟ
Conflict of Interest
Siu-Hin Wan has no relevant conflicts. Horng Chen has grants from the National Institutes of Health, non-financial support from Mayo Clinic, others from Zumbro Discovery, and grants from Scios, Inc., outside the submitted work. In addition, Dr. Chen has a patent Capricor Therapeutics, Anexon, Inc., and UpToDate with royalties paid.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by the author.
Author information
Authors and Affiliations
Corresponding author
Additional information
This article is part of the Topical Collection on Heart Failure Prevention
Rights and permissions
About this article

Cite this article
Wan, SH., Chen, H.H. Targeting Preclinical Diastolic Dysfunction to Prevent Heart Failure: Contemporary Insights. Curr Cardiovasc Risk Rep 9, 40 (2015). https://doi.org/10.1007/s12170-015-0466-1
Published:
DOI: https://doi.org/10.1007/s12170-015-0466-1