
Abstract
A 70-year-old man affected by bone metastases from castration resistant prostate cancer underwent Alpharadin (223Ra-dichloride) therapy (6 administrations of 50 kBq per kg i.v., once every 4 weeks). The inter-fraction variability of the absorbed dose to lesions was evaluated for four injections. Dosimetric assessments were performed following the MIRD approach and a recently published methodology. The mean absorbed dose and standard deviation for 4 lesions [mean (σ %)] were: 434 mGy (15 %) and 516 mGy (21 %) for the right and left humeral head, 1205 mGy (14 %) and 781 mGy (8 %) for the right and left glenoid. The estimated total absorbed dose after the whole treatment, considering also the relative-biological effectiveness of alpha particles (RBE = 5), yielded a D RBE range of 13–36 Gy. A good correlation between 99mTc and 223Ra uptake was obtained (R 2 = 0.7613). The tumour–non-tumour (TNT) ratio of 8 lesions (those above, plus 4 additional), monitored by six 99mTc-MDP bone scans over a period of about 10 months, evidenced a TNT reduction in two lesions (−42 and −48 %), but in most lesions the TNT remained fairly constant, evidencing that 223Ra-dichloride therapy tends to prevent further progression of osseous disease, leading to chronicity of the metastatic status.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Clinical trials have shown the safety and efficacy of palliation of painful bone metastases in patients with castration resistant prostate cancer (CRPC) using 223Ra-dichloride. The ALSYMCA trial demonstrated significantly improved overall survival and a delay in the time to symptomatic skeletal metastases with very low toxicity, thus, 223Ra-dichloride has become a new standard of care for these patients [1–9]. Marketing authorisation from the European Commission was recently received for Alpharadin (223Ra-dichloride) Xofigo©, solution for injection for the treatment of men with CRPC, symptomatic bone metastases and no visceral metastases. The standard administration protocol of 223Ra-dichloride consists of six monthly administrations of 50 kBq/kg.
223Ra emits useful photons for imaging, mainly at 81, 84 and around 95 keV (X-rays), and at 154, 269, 324, and 338 keV (gamma rays); however, due to the low number of photons, quantitative imaging was always considered challenging. Two previous studies addressed the possibility of in vivo assessment of pharmacokinetic and biodistribution [10], and quantitative planar imaging with gamma-camera [11]. Recently, two further studies reported the possibility of in vivo image-based macrodosimetric assessments. Chittenden et al. [12] evaluated absorbed dose to organs during a Phase 1, open-label study, administrating 100 kBq per kg of body weight (twice the activity of the standard protocol). Pacilio et al. [13] presented a suitable methodology for dosimetry of bone metastases with a standard treatment protocol; 24 lesions from 9 patients affected by osseous metastases from CRPC were studied, assessing the absorbed dose to lesion by MIRD approach [14, 15]. The feasibility of macrodosimetric studies during routine treatments was also proven, but the variability of dosimetric assessments between fractions deserved to be studied, to establish if dosimetry after each administration is required to evaluate the total absorbed dose to lesion. Moreover, the usefulness of macrodosimetry should be still demonstrated, investigating the possibility of establishing dose–response correlations.
In the present case report, the inter-administration variability of absorbed dose to lesion was studied, and the lesion response was monitored in terms of radiopharmaceutical uptake.
Case report
A 70–year-old man affected by bone metastases from CRPC underwent treatment with 223Ra-dichloride. The patient was enrolled in a multicentre study (protocol 88-8223/16216) of the Bayer HealthCare Pharmaceuticals, entitled “Radium-223 chloride in treatment of CRPC patients with bone metastasis”. According to the eligibility criteria, the patient provided written informed consent, had histologically confirmed, progressive bone predominant metastatic CRPC, with several bone metastases detected on 99mTc-MDP bone scan, and no known visceral and/or brain metastases. The patient had an Eastern Cooperative Oncology Group (ECOG) performance-status score of 0 [16], a life expectancy longer than 6 months, and adequate hematologic, renal, and liver function. Before the treatment with 223Ra-dichloride, the patient had not received external radiotherapy or systemic radionuclide therapy with other radioisotopes. He had no evidence of malignant lymphadenopathy that was more than 3 cm in the short-axis diameter, presence of visceral metastases, and imminent or established spinal cord compression. Treatment with 223Ra-dichloride followed the standard protocol: 6 injections of 50 kBq per kg of body weight (one every 4 weeks). Biokinetics and dosimetric evaluations were assessed for a total of 4 lesions (right and left humeral heads and right and left glenoids), whereas follow-up by 99mTc-MDP whole-body (WB) scan was performed also for 4 additional lesions (right coxo femoral, right trochanter, right and left iliac wing).
A GE dual-head gamma-camera (Infinia Hawkeye 4 SPECT/CT), equipped with 3/8-in. crystal was employed. Proper gamma-camera calibrations, for both 223Ra and 99mTc, were performed in terms of sensitivity (to convert image counts into activity) and transmission curve measurements (to correct image counts for attenuation and scatter by the methodology of the pseudo-extrapolation number) [14]. Further details about the calibration procedures can be found in Ref. [13]. 99mTc-MDP WB scans were performed with antero-posterior views, LEHR collimator, energy window centred at 140 keV (20 % wide), scan speed of 14 cm/min, and administration of 740 MBq. Patients’ images with 223Ra were collected acquiring antero-posterior planar static images with double-peak acquisition (two energy windows centred at 82 and 154 keV, 20 % wide), MEGP collimator, and an acquisition time of about 30 min. The patient underwent CT scan and first WB scan about 69 days before the first injection of 223Ra-dichloride. Immediately before the first injection, a static transmission image was also acquired (to perform attenuation correction) with a flood source filled with 185 MBq of 99mTc, and an acquisition time of about 4 min, with and without the patient on the couch.
After the first, third, fifth, and sixth injection of 223Ra-dichloride, biokinetic studies were performed, acquiring antero-posterior planar static images at different times. The time scheduling was similar for the four studies: about 1 h, 1 day, between 2 and 4 days and between 7 and 9 days, after the 223Ra-dichloride administration. In two cases (first and sixth injection), an additional late acquisition was performed between 11 and 13 days after the administration.
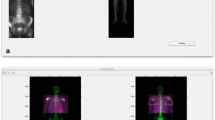
Due to the low quality of 223Ra images, the lesions were contoured on the WB scan, and then the regions-of-interest (ROIs) were overlapped on the 223Ra static images and transmission image. To improve the accuracy of the ROIs positioning, transmission and static images were coregistered with the WB scan by means of an in-house developed MATLAB (7.13.0.564, R2011b) toolkit. To further improve image co-registration (above all for the late acquisitions, having a low counting statistics), 223Ra images were processed with a Wiener filter to enhance contrast-ratio (CR) and signal-to-noise-ratio (SNR) [13]. Figure 1 reports an example of co-registration between WB and static image (anterior view, the static image was acquired at 1.5 h after the first administration), performed after filtering the static image. The activity of 223Ra in a source region at a given time was calculated following the methodology reported by MIRD Pamphlet No. 16 [14], performing background, attenuation, and scatter corrections. The background subtraction was performed with the Bujis method [14, 17], further details on the application of this methodology in the present study can be found in Ref. [13].

Example of coregistration between a99mTc-MDP WB image and a static 223Ra image (acquired at 1.5 h after administration, anterior view), performed with the MATLAB toolkit, delineating shoulders and body contour
Biokinetics data were fitted with MATLAB, with a bi-exponential (when a wash-in phase was observed) or mono-exponential curve. The cumulated activity was calculated by analytic integration of the fitting curve from 0 to infinity. According to the MIRD approach [15], the absorbed dose to lesion was calculated as the product between the cumulated activity and the self-irradiation S factor for 223Ra, corresponding to the lesion mass. The lesion mass was estimated by delineation of CT images, considering a mean lesion density of 1.4 g/cm3 [18]. The self-irradiation S factor for the given lesion mass was calculated from the OLINDA/EXM tabulations referred to spherical masses [19], by fitting the tabulated data with an inverse power law.
The correlation between the activity of 99mTc (“99mTc percent uptake”) and that of 223Ra (223Ra percent uptake) contained in each lesion was studied by linear regression analysis. The methodology for estimating 99mTc and 223Ra percent uptakes has been previously reported [13].
To monitor the response of the lesions during and after treatment, the patient underwent additional WB scans: 4 days before the third injection, 11 days before the fifth injection, and three more at 16, 45, and 93 days after the last injection. Uptake of the lesions was assessed in terms of uptake ratio between lesion and normal bone (hereinafter called TNT), calculated dividing the mean counts in the lesion by mean counts in the normal bone (both corrected for attenuation and scatter). The normal bone considered here was a part of the left crest of ilium.
Figure 2 reports all data deriving from quantification on scintigraphic images. Figure 2a shows the activity normalized at t = 24 h, as a function of acquisition time, for right and left humeral head, and right and left glenoid, after the first injection of 223Ra-dichloride. For each lesion, the 24-h normalization value was calculated from the corresponding biokinetics fit. Figure 2b reports the dose assessments after the first, third, fifth, and sixth administration. For each lesion, mean value of absorbed dose to lesion and corresponding percent standard deviation was [mean (σ %)]: right humeral head, [434 mGy (15 %)]; left humeral head, [516 mGy (21 %)]; right glenoid, [1205 mGy (14 %)]; left glenoid, [781 mGy (8 %)]. The correlation between 99mTc and 223Ra percent uptakes is reported in Fig. 2c for the four lesions for which absorbed dose was assessed, reporting data from all the biokinetics studies. Unfortunately, the acquisitions of WB scans acquired during the treatment did not correspond exactly to the 223Ra injections times, so the 99mTc percent uptakes were associated to 223Ra ones using the WB scan temporally closest to the instant of the 223Ra administration. Nevertheless, the R 2 is 0.7613, showing a significant correlation between the uptakes of the two radiopharmaceuticals. Figure 2d reports the TNT values, calculated on serial WB scans, as a function of the time elapsed after the first WB scan. The instants of 223Ra administrations are also indicated in the figure with vertical lines. The percent difference between the first TNT value (before the first 223Ra injection) and that temporally closest to the last administration, for the 8 lesions observed, ranged from −48 to 4 %. Two lesions evidenced a TNT decrease: right trochanter and right coxofemoral, with reductions of 42 and 48 %, respectively. For other lesions, TNT remained about constant, varying between −14 and 4 %. Two successive scans after that temporally closest to the last administration of 223Ra confirmed a fairly constant trend of TNT values.

Data deriving from quantification on images: a activities normalized at t = 24 h, as a function of time after the first injection of 223Ra-dichloride, for right and left humeral head, right and left glenoid (for each lesion, the 24-h normalization value was calculated from the corresponding biokinetics fit); b dose assessments for right and left humeral head, right and left glenoid, performed after the first, third, fifth, and sixth injection of 223Ra-dichloride; c correlation between 99mTc uptake and 223Ra activity extrapolated at time t = 0, for the four lesions for which absorbed dose was assessed, reporting data from all the biokinetics studies; d 99mTc uptake ratio between lesion and normal tissue (TNT) at different time before, during, and after the cycle of administrations of 223Ra, as a function of the time elapsed after the first scan (the instants of 223Ra administrations are indicated in the figure with vertical lines)
Figure 3 shows all WB scans (only anterior views), acquired before, during, and after the 223Ra treatment, reporting also, on the top of each image, the time elapsed from the first WB scan.

The WB scans (anterior views), acquired before, during, and after the 223Ra treatment, reporting the time elapsed from the first WB scan on the top of each image
Discussion
Figure 2a shows that the wash-in phase of radiopharmaceutical uptake is rapid, resulting in a negligible impact on the calculation of the cumulated activity. So it would be possible to avoid the early acquisition, to limit the discomfort in patients with pain. The level of variability for repeated inter-fraction absorbed dose assessments indicates that measurements after each administration of 223Ra would be advisable for accurate dosimetry, even though an analysis of experimental uncertainty would also be required to come to this conclusion. However, a good enough estimation could also be obtained multiplying by 6 the mean value of absorbed dose derived from some (not necessarily all) administrations, distributed during the whole treatment. In the present study, the estimated total absorbed dose to lesion, after a full cycle of administrations, accounting also for the suggested value of relative biological effectiveness for alpha particles (RBE = 5) [20], yields a D RBE ranging from about 13 to 36 Gy.
Despite the non-perfect temporal matching between the WB scan acquisitions and the 223Ra injections, the very good correlation between 99mTc and 223Ra percent uptakes reported in Fig. 2c indicates that the 223Ra-dichloride lesion uptake is well enough represented by 99mTc-MDP WB scans, so the lesions can be confidently delineated on 99mTc-MDP WB images. The correlation between 99mTc and 223Ra percent uptakes may suggest that, for a given lesion, the variation of the absorbed doses with respect to the first dosimetric assessment could be estimated by the variation of uptake of 99mTc-MDP, but this would occur as long as the biokinetics of the lesions remains the same from one injection to another. Unfortunately, it was not always the case. For instance, the increase of absorbed dose to the right glenoid at the sixth injection, 19 % with respect to the mean value (see Fig. 2b), is mostly explained by the increase of 12 % of the effective half time. Similarly for the left humeral head, the absorbed dose increase at the sixth injection of about 31 % is mainly due to an increment of about 27 % of the effective half time. The follow-up of uptake in lesions represented by Fig. 2d shows a sensible uptake reduction for the right trochanter and the right coxofemoral. Moreover, Fig. 3 also shows a visible reduction for the right femur (not quantified in Fig. 2d). However, for most lesions, a stabilization of the level of uptake was noticed: this is a direct indication that 223Ra-dichloride therapy tends to stop the progression of the osseous disease, leading to chronicity of the metastases. Thus, radiopharmaceutical uptake of metastatic bone could be inadequate as endpoint for studying dose–response correlation. However, time to radiological progression, or, even more importantly, time to symptomatic skeletal events (defined as: the need of radiation therapy to relieve symptoms, new symptomatic pathological bone fractures, tumor-related orthopaedic surgical intervention, or spinal cord compression), and overall survival could be more appropriate as endpoints.
Conclusions
The feasibility of in vivo quantitative imaging and macrodosimetry of bone lesions is confirmed. The follow-up of the level of uptake of the 223Ra can be efficiently and quantitatively performed by 99mTc-MDP imaging. For about 1 year, the level of uptake of the radiopharmaceuticals remained stable for most lesions. This does not testify in favour of the uptake in lesion for studying the dose–response correlation, but symptomatic skeletal event-free survival, or overall survival, could also be considered as endpoints.
References
Nilsson S, Larsen RH, Fossa SD, Balteskard L, Borch KW, Westlin JE, et al. First clinical experience with α-emitting radium-223 in the treatment of skeletal metastases. Clin Cancer Res. 2005;11:4451–9.
Nilsson S, Franzen L, Parker C, Tyrrell C, Blom R, Tennvall J, et al. Bone-targeted radium-223 in symptomatic, hormone-refractory prostate cancer: a randomised, multicentre, placebo-controlled phase II study. Lancet Oncol. 2007;8:587–94.
Parker CC, Pascoe S, Chodacki A, O’Sullivan JM, Germá JR, O’Bryan-Tear CG, et al. A randomized, double-blind, dose-finding, multicenter, phase 2 study of radium chloride (Ra 223) in patients with bone metastases and castration-resistant prostate cancer. Eur Urol. 2013;63:189–97.
Pandit-Taskar N, Larson SM, Carrasquillo JA. Bone-seeking radiopharmaceuticals for treatment of osseous metastases, part 1: α therapy with 223Ra-dichloride. J Nucl Med. 2014;55:268–74.
Nilsson S, Strang P, Aksnes AK, Franzèn L, Olivier P, Pecking A, et al. A randomized, dose–response, multicenter phase II study of radium-223 chloride for the palliation of painful bone metastases in patients with castration-resistant prostate cancer. Eur J Cancer. 2012;48:678–86.
Larsen RH, Saxtorph H, Skydsgaard M, Borrebaek J, Jonasdottir TJ, Bruland OS, et al. Radiotoxicity of the α-emitting bone-seeker Ra-223 injected intravenously into mice: histology, clinical chemistry and hematology. In Vivo. 2006;20:325–31.
Jadvar H, Quinn DI. Targeted α-particle therapy of bone metastases in prostate cancer. Clin Nucl Med. 2013;38:966–71.
Henriksen G, Breistol K, Bruland OS, Fodstad O, Larsen RH. Significant antitumor effect from bone-seeking, α-particle-emitting Ra-223 demonstrated in an experimental skeletal metastases model. Cancer Res. 2002;62:3120–5.
Parker C, Nilsson S, Heinrich D, Helle SI, O’Sullivan JM, Fossa SD, et al. Alpha emitter radium-223 and survival in metastatic prostate cancer. N Engl J Med. 2013;369:213–23.
Carrasquillo JA, O’Donoghue JA, Pandit-Taskar N, Humm JL, Rathkopf DE, Slovin SF, et al. Phase I pharmacokinetic and biodistribution study with escalating doses of Ra-dichloride in men with castration-resistant metastatic prostate cancer. Eur J Nucl Med Mol Imaging. 2013;40:1384–93.
Hindorf C, Chittenden S, Aksnes AK, Parker C, Flux GD. Quantitative imaging of 223Ra-chloride (Alpharadin) for targeted alpha-emitting radionuclide therapy of bone metastases. Nucl Med Commun. 2012;33:726–32.
Chittenden S, Hindorf C, Parker CC, Lewington VJ, Pratt BE, Johnson B, et al. Phase 1, open-label study of the biodistribution, pharmacokinetics and dosimetry of Radium-223 dichloride (223Ra dichloride) in patients with hormone refractory prostate cancer and skeletal metastases. J Nucl Med. 2015;56:1304–9.
Pacilio M, Ventroni G, De Vincentis G, Cassano B, Pellegrini R, Di Castro E, et al. Dosimetry of bone metastases in targeted radionuclide therapy with alpha-emitting 223Ra-dichloride. Eur J Nucl Med Mol Imaging. 2015. doi:10.1007/s00259-015-3150-2.
Siegel JA, Thomas SR, Stubbs JB, Stabin MG, Hays MT, Koral KF, et al. Mird Pamphlet No. 16 techniques for quantitative radiopharmaceutical biodistribution data acquisition and analysis for use in human radiation dose estimates. J Nucl Med. 1999;40:37s–61s.
Loevinger R, Budinger TF, Watson EE. MIRD primer for absorbed dose calculations. Revised. New York, NY: The Society of Nuclear Medicine; 1991.
Oken MM, Creech RH, Tormey DC, Horton J, Davis TE, McFadden ET, et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol. 1982;5:649–55.
Buijs WC, Siegel JA, Boerman OC, Corstens FH. Absolute organ activity estimated by five different methods of background correction. J Nucl Med. 1998;39:2167–72.
Cristy M, Eckerman KF. Specific absorbed fractions of energy at various ages from internal photon sources Technical Report ORNL/TM-8381/V1, Oak Ridge National Laboratory, TN, USA; 1987.
Stabin MG, Sparks RB, Crowe E. OLINDA/EXM: the second-generation personal computer software for internal dose assessment in nuclear medicine. J Nucl Med. 2005;46:1023–7.
Sgouros G, Roeske JC, McDevitt MR, Palm S, Allen BJ, Fisher DR, et al. MIRD pamphlet no. 22 (abridged): radiobiology and dosimetry of α-particle emitters for targeted radionuclide therapy. J Nucl Med. 2010;51:311–28.
Acknowledgments
The patient enrolled in this research was participating in a multicenter study (protocol 88-8223/16216) sponsored by Bayer HealthCare Pharmaceuticals, entitled “Radium-223 chloride in treatment of CRPC patients with bone metastasis”. The authors declare that this study complies with the current law of the country (Italy) where it was performed.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None.
Rights and permissions
About this article

Cite this article
Pacilio, M., Ventroni, G., Cassano, B. et al. A case report of image-based dosimetry of bone metastases with Alpharadin (223Ra-dichloride) therapy: inter-fraction variability of absorbed dose and follow-up. Ann Nucl Med 30, 163–168 (2016). https://doi.org/10.1007/s12149-015-1044-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12149-015-1044-9