
Abstract
Previous research has explored the relationship between anxiety, depression, and internet addiction (IA) using variable-centered approaches among secondary school students. However, the long-lasting COVID-19 pandemic worsens the interrelationship among the three mental disorders above. Therefore, the present study evaluated the underlying dynamic changes in the symptoms of these disorders using a network analysis approach. A total of 2,356 Chinese secondary school students were tracked from the very beginning of online learning for four months by completing surveys of the Generalized Anxiety Disorder Scale, Patient Health Questionnaire, and Internet Addiction Test. The cross-sectional symptom network (CSSN) and cross-lagged panel network (CLPN) analyses were utilized for the statistical analysis. Two comorbidities CSSNs were compared, and the symptoms of “uncontrollable worry”, “depressed/moody/nervous being offline”, and “job performance or productivity suffer” were identified as the symptoms with the highest Expected Influence (EI) value in both waves. Additionally, the CLPN revealed that the symptom of “snap or act annoyed if bothered” served as the symptom with the highest in-expected influence (IEI) value, and “anhedonia” (i.e., a depression symptom) and “irritability” (i.e., an anxiety symptom) were identified as the symptom that exhibited the highest out-expected influence (OEI) value. Appropriate interventions targeting the central symptoms may potentially prevent or reduce the risk of anxiety, depression, and IA.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Internet addiction (IA) is characterized by excessive or obsessive behavior related to internet use, manifesting as individuals’ failure to manage their internet use, which is usually accompanied by a series of symptoms, including loss of control, withdrawal, and escape (Young, 1998). A meta-analysis reviewed the published studies from 31 countries and reported that before the outbreak of COVID-19, the weighted average prevalence for IA was 8.90% (95% CI, 7.46-10.59%) in East Asia (Pan et al., 2020). Strikingly, after the outbreak of COVID-19, the prevalence of IA reached 36.7% among the Chinese general population (Y.-Y. Li et al., 2021). The rising prevalence rate of IA might be related to the influence of COVID-19. Due to the rapid spread of the COVID-19 pandemic, students were urged to stay home and study online during the lockdown period of the pandemic. Accordingly, the usage rate of online education in China has dramatically risen from 27.2% (China Internet Network Information Center, 2019) (before the pandemic) to 46.8% (China Internet Network Information Center, 2020) (after the pandemic). Meanwhile, during the pandemic, people may become more likely to over-engage in playing video games and have fewer resources for effective social support, which may all contribute to the rising prevalence and severity of IA (Y.-Y. Li et al., 2021). Noticeably, IA can give rise to a series of negative outcomes, including impaired interpersonal relationships, rising avoidant tendencies, and academic and work efficiency (Hou et al., 2019; Pan et al., 2020). More seriously, IA also shares a close relation with emotional and psychological disorders, such as depression, anxiety disorder, and sleep disturbance (Alimoradi et al., 2019). Besides, adolescents in Asian countries are especially vulnerable to suffering from IA, and Chinese adolescents with IA face a higher probability of exhibiting depression and anxiety (Kwok-Kei Mak, 2014), which highlights the necessity of focusing on IA, especially on Chinese adolescents after the pandemic.
Moreover, the pandemic and the lockdown also greatly impacted individuals’ psychic and psychopathological symptoms (Stanković et al., 2021; Tao et al., 2023b, 2024a, b). Especially, during the pandemic and lockdown, the prevalence rates of depression and anxiety among secondary school students (junior and senior high school students included) (Gao et al., 2021), who were under much academic pressure due to the competitive circumstances of college entrance examinations, rose significantly. Depression and anxiety, identified as two of the most prevalent mental disorders among adolescents, are highly comorbid and can greatly interrupt the healthy development of adolescents, leading to unfavorable outcomes, including disrupted academic performance, impaired social function, and even a rising possibility of self-harm and suicide (Balázs et al., 2013; Gijzen et al., 2021; Tang et al., 2024; Thapar et al., 2022; Wang et al., 2022).
In addition, IA is closely related to depression and anxiety. According to the social displacement hypothesis, spending too much time engaging in online social interactions decreases face-to-face communication and increases difficulties in addressing problems adaptively in the real-world environment (Bessière et al., 2008), which contributes to a greater likelihood of depression and anxiety (Faraci et al., 2022). In line with the theory, a study employed hierarchical regression to explore the relation between anxiety, depression, and social media use and found that overall social media use is related to higher levels of depression and anxiety disorder (Woods & Scott, 2016). Similarly, an eight-year longitudinal study also stated that adolescents who use social media more frequently may face an increasing risk of suffering from depression and anxiety disorder (Coyne et al., 2020). Also, Li et al. (2019) conducted a short-term longitudinal study that demonstrated anxiety and depression were both positively associated with IA over time. More seriously, during the pandemic, the relation between depression, anxiety, and IA may be strengthened. Besalti and Satici (2022) conducted a longitudinal study revealing that students with internet addiction had lower learning satisfaction in online learning environments, which is closely related to the occurrence of depression and anxiety among students (Gabrovec et al., 2022). This finding is in line with the cognitive-behavioral model of pathological internet use, indicating that underlying psychopathology (such as depression or anxiety) is a predisposed vulnerability to internet overuse (Davis, 2001).
Moreover, according to the theory of compensatory internet use, individuals may utilize the internet as a maladaptive coping strategy for real-world issues (Gao et al., 2018). Consequently, students may try to use the internet to satisfy a psychological demand that cannot be satisfied in their real surroundings (Stevens et al., 2019) to escape the anxiety and depression caused by staying at home and studying online (Li et al., 2019). Yet, excessive internet use cannot fulfill unmet psychological demands and may further contribute to the aggregation of depression and anxiety (Jeong et al., 2020). Aligned with the theory, a cross-lagged analytic study indicated that the severity of both depression and IA increased during the pandemic, and the development of depression and IA showed an interactive pattern (Tian et al., 2022), which indicated that the relation between depression and IA can be bidirectional. Yet, the aforementioned studies, perceiving the traditional perspective, treated depression, anxiety, and IA as entities, which overlook the fact that these mental disorders actually consist of different symptoms. Indeed, these studies failed to look into the interaction between the symptoms of depression, anxiety, and IA, hindering further understanding of the possible bidirectional and interactive development pattern, which raises an urgent need for more in-depth research on this issue.
Different from the traditional perspective, network theory may be appropriate for addressing the comorbidity among anxiety, depression, and IA. According to network theory (Borsboom, 2021), a mental disorder manifests from interactions between symptoms. In addition, a symptom of one disorder may trigger symptoms of another, resulting in the onset and maintenance of comorbidity (Cramer et al., 2010). Consequently, assessing the changes between symptoms within several disorders might give a deeper understanding of the mechanisms behind the persistence or resistance of comorbidity (Bringmann et al., 2015). To our knowledge, a cross-sectional network study revealed three IA symptoms (i.e., “anticipation for future online activities”, “fear that life is boring and empty without the internet”, and “spend more time online over going out with others”) bridged the co-occurrence network structure between depression and IA among adolescents in Macau (Cai et al., 2022). In addition, a longitudinal study found that “guilty” (i.e., a symptom of depression) and “escape” (i.e., a symptom of IA) bridged depression and IA, and the central symptoms across two waves were consistent (Zhao et al., 2023). However, Zhao et al. (2023) simply compared the characteristics of the two cross-sectional networks, omitting the directionality changes between symptoms over time. Although the above studies tried to reveal the interrelationship between depression and IA, they ignored the co-occurring psychiatric disorder, anxiety, which may result in a limited effect of prevention or treatments (Nickerson et al., 2017). Hence, the longitudinal feature of symptom networks between anxiety, depression, and IA among secondary school students is worth exploring.
To sum up, the co-occurrence of anxiety, depression, and IA has been well documented in previous studies, but few have provided insight into the underlying mechanisms of symptomology or the changes in the network structures between the three mental disorders over time. Inspired by the network approach, this exploratory study utilized the cross-sectional symptom network (CSSN) and cross-lagged panel network (CLPN) models to elucidate time-varying associations and test the following hypothesis.
-
Aim 1: Identify the central and bridge symptoms between anxiety, depression, and IA among Chinese secondary school students before and after long-term online learning.
-
Aim 2: Integrate cross-lagged panel models in the network analysis framework and estimate autoregressive and cross-lagged pathways of symptoms across time to assess the dynamic changes in interactions between anxiety, depression, and IA symptoms among Chinese secondary school students throughout long-term online learning during the pandemic of COVID-19.
-
Hypothesis 1: As previous studies stated, long-term online learning is usually accompanied by the rising possibility of IA, which shares a close relation with depression and anxiety. Indeed, we hypothesize that the connection between IA, depression, and anxiety becomes tenser throughout long-term online learning, manifesting as the global strength of the network in the second wave being higher than that in the first wave.
Methods
Participants and procedure
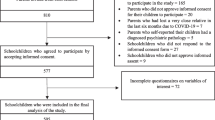
The first wave study randomly recruited 10,104 high school students in February 2022, after two weeks of winter vacation, in 35 high schools in Harbin, China. Given the impact of COVID-19, students had to take the course online for up to four months (June 2022). The second wave of data collection was implemented in the fourth week after the resumption of offline classes and randomly recruited 8,390 high school students. Following the previous study (Zhang et al., 2022), an online survey using the WeChat-based Wenjuanxing application was utilized instead of the conventional face-to-face interview to avoid the transmission of COVID-19. After combining the two waves of data, the total number of valid data was 2,356 (Male, N = 1,219; Female, N = 1,137; Age mean ± SD = 13.84 ± 1.37, age range from 12 to 17). Before participating, each participant as well as their parents read about the specific purpose of the study and electronically completed an informed consent form which introduced the rights they obtained during the whole testing process, such as “you can quit at any moment during the whole procedure without any concern”. The Beijing Normal University ethics committee examined and approved the research (Reference number: 202112220085).
Measures
Generalized anxiety disorder scale (GAD-7)
The GAD-7 is a brief 7 items scale, consisting of items like “Worrying too much about different things”, that measures anxiety symptoms over the previous two weeks on a scale from 0 (not at all) to 3 (nearly every day) (Spitzer et al., 2006). Higher scores indicate more severe anxiety symptoms. The Chinese version of GAD-7 has been proven to be reliable and valid among Chinese adolescents (Tao et al., 2024c). The GAD-7 has high internal consistency in the present study at both wave 1 (α = 0.94) and wave 2 (α = 0.95).
Patient health questionnaire (PHQ-9)
The PHQ-9 is a questionnaire-based depression scale used to assist primary care practitioners in diagnosing depression and monitoring treatment (Kroenke et al., 2001). The Chinese version of PHQ-9 has nine items, (such as “Little interest or pleasure in doing things) scored from 0 (not at all) to 3 (nearly every day), for a total score that ranges from 0 to 27, which was validated as a proper tool to measure the level of depression among Chinese adolescents (Tao et al., 2024c). Higher scores indicate more severe depressive symptoms. The PHQ-9 has high internal consistency in the present study at both wave 1 (α = 0.92) and wave 2 (α = 0.94).
Internet addiction test (IAT)
The IAT is a self-report scale consisting of 20 items designed to measure various characteristics and behaviors associated with internet addiction (IA) over the past month (Young, 1998). Items, such as “How often do you find that you stay online longer than you intended”, are rated on a 5-point Likert scale and can generate a maximum score of 100, with higher scores indicating a higher overall level of IA severity. The Chinese version of the IAT has been well-validated as an efficient tool for assessing the participants’ IA levels among the general Chinese population (Chang & Law, 2008; Liang et al., 2022). The IAT has high internal consistency in the present study at both wave 1 (α = 0.95) and wave 2 (α = 0.96).
Statistical analysis
The present study conducted all analyses utilizing R (version 4.1.3). We used the cross-sectional symptom network (CSSN) and the cross-lagged panel network (CLPN) to estimate network structure. Specific procedures are detailed in the supplement.
First, given that sex and age were significantly associated with anxiety, depression, and IA (Choi et al., 2015), we conducted CSSNs and CLPN characteristics with sex and age included. Second, we compared CSSNs with and without the experience of offline classes during the pandemic of COVID-19.
Results
Prevalence and descriptive statistics
In the present study, we used the cut-off points of 7 (Wang et al., 2022), 8 (Manea et al., 2012), and 40 (Tateno et al., 2018) for screening students inclined to anxiety, depression, and IA. 11.67%, 14,22%, and 31.54% of all participants reported anxiety, depression, and IA at wave 1, respectively. At wave 2, 16%, 17.61%, and 31.54% of all participants reported anxiety, depression, and IA.
The Mean, SD, Skew, and Kurtosis score of each item in the GAD-7, PHQ-9, and IAT questionnaires are shown in Table 1.
Cross-sectional symptom networks (CSSNs)
The entire edge list for the baseline and follow-up networks is given in the supplementary materials (i.e., Table S1 and Table S2). In the baseline network (Part A of Fig. 1), the strongest edges (top three) were between the symptoms IAT6 (i.e., school grades suffer) and IAT8 (i.e., job performance or productivity suffer), IAT3 (i.e., prefer the excitement online) and IAT19 (i.e., spend more time online over going out with others), and GAD1 (i.e., nervousness) and GAD2 (i.e., uncontrollable worry). Different from the follow-up result (Part B of Fig. 1), it was shown that the strongest edges (top three) were between the symptoms PHQ7 (i.e., concentration) and PHQ8 (i.e., motor), IAT19 (i.e., spend more time online over going out with others) and IAT3 (i.e., prefer the excitement online), and GAD1 (i.e., nervousness) and GAD4 (i.e., trouble relaxing). These edges were significantly stronger than many other edges in the network, as indicated by the edge weight difference plots for both networks (see Supplementary Figure S1).

A the symptom network structure of wave (1) B the symptom network structure of wave (2) C EI (expected influence, the higher value stands for higher importance of this node in the network) values of two waves. D the bridge EI values (the higher value stand for a more important connecting effect between two different disorder) of two waves. The lines refer to the relation between two nodes, green ones stand for positive relations and red ones stand for negative relations while the thicker the line is, the closer the relation between these two nodes share
In part C of Fig. 1(see Supplementary Figure S2), the EI of 36 symptoms in the CSSNs is plotted by order of respective values. The symptom (top three), GAD2 (i.e., uncontrollable worry), IAT20 (i.e., depressed/moody/nervous being offline), and IAT8 (i.e., job performance or productivity suffer), had the highest EI value and was the most central symptom both in the baseline and follow-up network. Overall, these symptoms had significantly higher EI centrality than other symptoms within two CSSNs, evinced by the EI centrality difference plots (see Supplementary Figure S3). In part D of Fig. 1 (see Supplementary Figure S4), there were 8 bridge symptoms in the baseline comorbidity network (i.e., IAT14, PHQ2, PHQ6, PHQ8, PHQ9, GAD1, GAD6, GAD5). However, at the follow-up, the number of bridge symptoms decreased to 5 (i.e., PHQ2, PHQ9, GAD2, GAD5, GAD6).
Accuracy plots showed small-to-moderate CIs, suggesting good accuracy for the baseline and follow-up networks (see Supplementary Figure S5).
Network comparison test between wave 1 and wave 2
We compared the network structure and network centrality indices between the two waves. As shown in Figure S6 (left panel), the bootstrap value of the difference in global network strength is significant (network strength among wave 1 was 17.6 and wave 2 was 18.9; S = 1.3, p = 0.025). The right panel in Figure S6 indicated that the maximum difference in any edge weight (1000 permutations) bootstrap value was significantly different (M = 0.20, p = 0.012).
Cross-lagged panel network (CLPN)
All edge weights are given in the Supplementary Materials (see Supplementary Table S3). As shown in Part A of Fig. 2, the connection from the symptom PHQ1 (i.e., anhedonia) to IAT3 (i.e., prefer the excitement online) displayed the strongest cross-lagged connection, followed by the connections from PHQ1 (i.e., anhedonia) to IAT1 (i.e., stay online longer), IAT11 (i.e., anticipation) to IAT16 (i.e., Request an extension for longer time), and PHQ1 (i.e., anhedonia) to IAT12 (i.e., life boring and empty). The above edge weights difference tests indicated that these edges were significantly stronger than most of the other edges.

A the cross-lagged panel network structure. B centrality indices (OEI and IEI) of all items. C autoregressive values of the cross-lagged panel network
Part B of Fig. 2 shows the CLPN for baseline symptoms predicting follow-up symptoms along with the centrality plots for the in-expected influence (IEI, higher value stating that this node is under more influence of other nodes) and out-expected influence (OEI, higher value stating that this node may exhibit more influence on other nodes). Descriptively, the symptoms PHQ1 (i.e., anhedonia) and GAD6 (i.e., irritability) had the highest OEI, whereas the symptoms IAT13 (i.e., snap or act annoyed if bothered) had the highest IEI. These symptoms displayed significantly higher OEI and IEI, respectively, compared to other symptoms in the CLPN (see Supplementary Figure S7). In addition, IAT4 (i.e., form new relationships) and GAD5 (i.e., restlessness) had higher and lower autoregression coefficients (see Part C of Fig. 2). The accuracy plots indicated high accuracy of the CLPN (see Supplementary Figure S8).
The case-drop bootstrapping results indicated strong stability of the EI centrality (CS-C = 0.67) both in the baseline and follow-up networks (see parts A and B of Fig. 3). Likewise, the case-drop bootstrapping results suggested strong stability for the IEI (CS-C = 0.51) and OEI (CS-C = 0.31) in CLPN (see part C of Fig. 3).

Case-dropping bootstrap test of centrality indices. The x-axis indicates the percentage of cases of the original sample included at each step. The y-axis indicates the correlations between the EI, bridge EI, OEI, and IEI from the original network and the EI, bridge EI, OEI, and IEI from the networks re-estimated after excluding increasing percentages of cases. A the cross-sectional network of wave (1) B the cross-sectional network of wave (2) C the cross-lagged panel network
Discussion
Several findings are worth discussing as the first study to explore the comorbidity network structure of anxiety, depression, and IA among secondary school students before and after long-term online learning during the pandemic of COVID-19.
Differences between the baseline and follow-up cross-sectional symptom networks (CSSNs)
First, we compared two comorbidity CSSNs and identified that “uncontrollable worry”, “depressed/moody/nervous being offline”, and “job performance or productivity suffer” served as symptoms with the highest EI value in both wave 1 and wave 2, which stated that these symptoms shared the closest relation with other symptoms in the network of depression, anxiety, and IA. Although the top three central symptoms were consistent over time, the global network strength revealed that the follow-up network structure affected by long-term online learning was significantly stronger than the baseline, which suggested a tighter interaction and rising severity of comorbidity among depression, anxiety, and IA. This result is similar to a previous longitudinal study, which found that containment management measures are likely to lead students to experience hopelessness (Tao et al., 2023a). During online learning, due to containment management, students are forced to stay at home taking online courses and have fewer chances to be involved in physical exercise and face-to-face interpersonal communications (Kadir et al., 2023). Indeed, the effects of containment on students as a repeatedly performed isolation measure are ongoing, such as persistent uncontrollable worry, which is an uncomfortable emotion associated with a protracted event and potential negative events (American Psychological Association, 2015). What’s more, according to the compensatory theory of internet use (Gao et al., 2018), when students face negative emotions like uncontrollable worry as well as an unsatisfied need for interpersonal interactions, students may have difficulty concentrating on their academic work and then engage in internet activities to regulate their emotions and satisfy unmet psychological needs instead (Stevens et al., 2019). Yet online activities are unable to achieve students’ social satisfaction and emotional bonding, and therefore, as the theory of compensatory internet use suggests (Gao et al., 2018), students could show nervousness, depressed mood, low motivation, and efficiency in learning when they are offline (Obeid et al., 2019).
Similarly, a cross-sectional network study found that “job performance or productivity suffer” had the highest strength in the network structure of IA among patients with major depressive disorder (Cai et al., 2022). Consistent with the theory of the social displacement hypothesis (Bessière et al., 2008), we infer that the prolonged online learning status tends to bring about overuse of the internet, making students overly focus on the information shared online (Besalti & Satici, 2022) and impairing the motivation to learn (Mabrur & Suwartono, 2021), consequently negatively impacting academic performance (Reed & Reay, 2015).
The nodes “sleep loss”, “sad mood”, “guilt”, “motor”, “suicide”, “nervousness”, “irritability”, and “restlessness”, were the critical bridge nodes linking the baseline comorbidity network, which partly confirms previous findings (Cai et al., 2022; Zhao et al., 2023). It is important to note that children frequently use the internet at night to avoid conflict with their parents and conceal their online activity (Barthorpe et al., 2020). This results in less sleep and a higher risk of depression, which is consistent with previous findings (Lemola et al., 2015). However, as the theory of the cognitive-behavior model of pathological internet use mentioned (Davis, 2001), long-term internet use may increase the risk of anxiety and depression symptoms after offline learning. Hence, we found that the bridge symptoms decreased to 5 in the follow-up comorbidity network (i.e., sad mood, suicide, uncontrollable worry, restlessness, and irritability).
Characteristics of cross-lagged panel network (CLPN)
Additionally, the CLPN revealed that “snap or act annoyed if bothered” was the highest IEI IA symptom predicted by other symptoms, which indicated that many symptoms in wave 1, such as “anhedonia” and “irritability” may influence “snap or act annoyed if bothered” in wave 2. Meanwhile, “anhedonia” (i.e., a depression symptom) and “irritability” (i.e., an anxiety symptom) had the highest OEI, which stated that those two symptoms may act as the triggering symptoms that give rise to other symptoms, such as “snap or act annoyed if bothered”. This result is consistent with a previous study, which reported that early emotion regulation impacts emotional-behavioral functioning in middle childhood (8 years of age), which influences the onset of IA in adolescence (Cimino & Cerniglia, 2018). The study revealed that the greatest harm of long exposure to online learning is that students tend to show annoyance and irritability if they feel disturbed. Furthermore, long-term addiction to the internet is followed by a tendency towards little interest or pleasure in engagement and becoming easily annoyed or irritable (Besalti & Satici, 2022; Cai et al., 2022). Again, the result of CLPN confirmed the theory of the cognitive-behavioral model of pathological Internet use (Davis, 2001), that the underlying psychopathology (such as depression or anxiety) is a predisposed vulnerability to internet overuse.
Excessive internet use may negatively impact adolescents’ cognition and time utilization, preventing them from focusing on their academic work and feeling less energetic (Salmela-Aro et al., 2017). Prolonged exposure to online learning increases the risk of IA-induced anxiety and depression (Niu et al., 2023; Seki et al., 2019; Stevens et al., 2019). The consistently highest centrality in CSSN and highest OEI in CLPN suggest that “irritability” plays a central downstream effect on IA.
Implication
This study makes an important contribution to the related field in terms of theoretical and practical aspects. Theoretically, the current study addresses the gaps in previous research by examining the associations between long-term online learning, anxiety, depression, and IA among secondary school students. It offers symptom-level and longitudinal evidence to enhance our understanding of these relationships. Practically, the findings of the present study can provide a basis for practical work to improve the mental health of adolescents. Specifically, this study highlights the significance of concern for the mental health of adolescents who learn online or are quarantined. Effective supervision of adolescents’ internet usage should also be prioritized according to our results. Meanwhile, we identified “irritability” and “anhedonia” as the symptoms that may trigger other symptoms of depression, anxiety, and IA. Indeed, interventions aimed at helping adolescents develop more efficient emotional regulation strategies (such as cognitive behavioral therapy) and guiding adolescents to rebuild pleasure in life (such as mindfulness) may be helpful for the early prevention and alleviation of depression, anxiety, and IA.
Limitations and future recommendations
The strengths of this study included the large sample size, highly reliable results, and the use of network analysis to explore the dynamic change in the network structure of anxiety, depression, and IA among secondary school students, which could help pinpoint potential treatment and prevention strategies for students facing these issues (Nickerson et al., 2017). After controlling for age and gender in the analysis, several limitations of this study should be noted. Based on this, we also suggest some research directions that researchers can consider in the future. First, different from the experimental design, the causal associations between anxiety, depression, and IA symptoms across time could not be inferred in this research. Thus, future studies can use experimental design to investigate the causal relation between anxiety, depression, and IA. Second, the study involved high school students from Harbin, China, and was conducted during the pandemic. Thus, even though we calculated the prevalences of anxiety, depression, and IA among participants, these findings may not be applicable to high school students in different provinces or time periods. More large-sample, cross-province, cross-country studies in this area are needed in the future.
Conclusion
In conclusion, this study identified three central symptoms (e.g., “uncontrollable worry”, “depressed/moody/nervous being offline”, and “job performance or productivity suffer”), that were consistent over time. To prevent negative outcomes associated with anxiety, depression, and IA, appropriate interventions targeting these central symptoms warrant attention in future work. Furthermore, key bridge symptoms (e.g., 8 bridge symptoms at baseline and 5 bridge symptoms at follow-up) could be potential targets in the treatment of secondary high school students with comorbidity networks of anxiety, depression, and IA. Finally, to reduce the most affected symptom of IA (i.e., snap or act annoyed if bothered), it is necessary to treat the anxiety (i.e., irritability) and depression (i.e., anhedonia) symptoms immediately when secondary school students return to offline learning.
Code and data availability
Analytic code and data for this work are available upon request.
References
Alimoradi, Z., Lin, C. Y., Broström, A., Bülow, P. H., Bajalan, Z., Griffiths, M. D., Ohayon, M. M., & Pakpour, A. H. (2019). Internet addiction and sleep problems: A systematic review and meta-analysis. Sleep Medicine Reviews,47, 51–61. https://doi.org/10.1016/j.smrv.2019.06.004
American Psychological Association. (2015). Anxiety disorders: DSM-5 selections. American Psychiatric Pubishing.
Balázs, J., Miklósi, M., Keresztény, A., Hoven, C. W., Carli, V., Wasserman, C., Apter, A., Bobes, J., Brunner, R., Cosman, D., Cotter, P., Haring, C., Iosue, M., Kaess, M., Kahn, J. P., Keeley, H., Marusic, D., Postuvan, V., Resch, F., Saiz, P. A., Sisask, M., Snir, A., Tubiana, A., Varnik, A., Sarchiapone, M., & Wasserman, D. (2013). Adolescent subthreshold-depression and anxiety: Psychopathology, functional impairment and increased suicide risk. Journal of Child Psychology and Psychiatry,54(6), 670–677. https://doi.org/10.1111/jcpp.12016
Barthorpe, A., Winstone, L., Mars, B., & Moran, P. (2020). Is social media screen time really associated with poor adolescent mental health? A time use diary study. Journal of Affective Disorders,274, 864–870. https://doi.org/10.1016/j.jad.2020.05.106
Besalti, M., & Satici, S. A. (2022). Online learning satisfaction and internet addiction during Covid-19 pandemic: A two-Wave Longitudinal Study. TechTrends,66(5), 876–882. https://doi.org/10.1007/s11528-022-00697-x
Bessière, K., Kiesler, S., Kraut, R., & Boneva, B. S. (2008). Effects of Internet use and social resources on changes in depression. Information Communication & Society,11(1), 47–70. https://doi.org/10.1080/13691180701858851
Borsboom, D. (2021). A network theory of mental disorders. Annales Medico-Psychologiques,179(1), 86–94. https://doi.org/10.1016/j.amp.2020.11.014
Bringmann, L. F., Lemmens, L. H. J. M., Huibers, M. J. H., Borsboom, D., & Tuerlinckx, F. (2015). Revealing the dynamic network structure of the Beck Depression Inventory-II. Psychological Medicine,45(4), 747–757. https://doi.org/10.1017/S0033291714001809
Cai, H., Bai, W., Sha, S., Zhang, L., Chow, I. H. I., Lei, S. M., Lok, G. K. I., Cheung, T., Su, Z., Hall, B. J., Smith, R. D., & Xiang, Y. T. (2022). Identification of central symptoms in internet addictions and depression among adolescents in Macau: A network analysis. Journal of Affective Disorders,302, 415–423. https://doi.org/10.1016/j.jad.2022.01.068
Chang, M. K., & Law, S. P. M. (2008). Factor structure for Young’s internet addiction test: A confirmatory study. Computers in Human Behavior,24(6), 2597–2619. https://doi.org/10.1016/j.chb.2008.03.001
China Internet Network Information Cente (2019). The 44th Statistical Report on the Development of China’s Internet Network. https://www.cnnic.net.cn/n4/2022/0401/c88-1116.html
China Internet Network Information Cente (2020). The 45th Statistical Report on the Development of China’s Internet Network. https://www.cnnic.net.cn/n4/2022/0401/c88-1088.html
Choi, S. W., Kim, D. J., Choi, J. S., Ahn, H., Choi, E. J., Song, W. Y., Kim, S., & Youn, H. (2015). Comparison of risk and protective factors associated with smartphone addiction and internet addiction. Journal of Behavioral Addictions,4(4), 308–314. https://doi.org/10.1556/2006.4.2015.043
Cimino, S., & Cerniglia, L. (2018). A Longitudinal Study for the Empirical Validation of an Etiopathogenetic Model of Internet Addiction in Adolescence Based on Early Emotion Regulation. BioMed research international,2018, 4038541–4038548. https://doi.org/10.1155/2018/4038541
Coyne, S. M., Rogers, A. A., Zurcher, J. D., Stockdale, L., & Booth, M. (2020). Does time spent using social media impact mental health? An eight year longitudinal study. Computers in Human Behavior,104, 106160. https://doi.org/10.1016/j.chb.2019.106160
Cramer, A. O. J., Waldorp, L. J., van der Maas, H. L. J., & Borsboom, D. (2010). Comorbidity: A network perspective. The Behavioral and Brain Sciences,33(2–3), 137–150. https://doi.org/10.1017/S0140525X09991567
Davis, R. A. (2001). A cognitive-behavioral model of pathological internet use. Computers in Human Behavior,17(2), 187–195. https://doi.org/10.1016/S0747-5632(00)00041-8
Faraci, P., Bottaro, R., Valenti, G. D., & Craparo, G. (2022). Psychological well-being during the Second Wave of COVID-19 pandemic: The mediation role of generalized anxiety. Psychology Research and Behavior Management,15, 695–709. https://doi.org/10.2147/PRBM.S354083
Gabrovec, B., Selak, S., Crnkovic, N., Cesar, K., & Sorgo, A. (2022). Perceived satisfaction with online study during COVID-19 lockdown correlates positively with resilience and negatively with anxiety, Depression, and stress among Slovenian Postsecondary students. International Journal of Environmental Research and Public Health,19(12), Article 7024. https://doi.org/10.3390/ijerph19127024
Gao, T., Li, J., Zhang, H., Gao, J., Kong, Y., Hu, Y., & Mei, S. (2018). The influence of alexithymia on mobile phone addiction: The role of depression, anxiety and stress. Journal of Affective Disorders,225, 761–766. https://doi.org/10.1016/j.jad.2017.08.020
Gao, T., Qin, Z., Hu, Y., Fei, J., Cao, R., Liang, L., Li, C., Mei, S., & Meng, X. (2021). Trajectories of depression and anxiety in Chinese high school freshmen: Associations with Internet addiction. Journal of Affective Disorders,286, 180–186. https://doi.org/10.1016/j.jad.2021.02.074
Gijzen, M. W. M., Rasing, S. P. A., Creemers, D. H. M., Smit, F., Engels, R., & De Beurs, D. (2021). Suicide ideation as a symptom of adolescent depression. A network analysis. Journal of Affective Disorders,278, 68–77. https://doi.org/10.1016/j.jad.2020.09.029
Hou, Y. B., Xiong, D., Jiang, T. L., Song, L. L., & Wang, Q. (2019). Social media addiction: Its impact, mediation, and intervention. Cyberpsychology-Journal of Psychosocial Research on Cyberspace,13(1), Article 4. https://doi.org/10.5817/cp2019-1-4
Jeong, B., Lee, J. Y., Kim, B. M., Park, E., Kwon, J. G., Kim, D. J., Lee, Y., Choi, J. S., & Lee, D. (2020). Associations of personality and clinical characteristics with excessive internet and smartphone use in adolescents: A structural equation modeling approach. Addictive Behaviors,110, 106485. https://doi.org/10.1016/j.addbeh.2020.106485
Kadir, A., Sunarno, S., Oktaviana, A., Zulfah, A. F., Maharani, C. F., Santoso, N. T., Lestari, F., Erwandi, D., & Dhesi, S. K. (2023). Factors Associated with psychosocial symptoms experienced by students in response to COVID-19 pandemic: A multivariate analysis. Inquiry-the Journal of Health Care Organization Provision and Financing,60, 00469580231155720. https://doi.org/10.1177/00469580231155720
Kroenke, K., Spitzer, R. L., & Williams, J. B. (2001). The PHQ-9: Validity of a brief depression severity measure. Journal of General Internal Medicine,16(9), 606–613. https://doi.org/10.1046/j.1525-1497.2001.016009606.x
Kwok-Kei Mak, C. M. L., Watanabe, H., Kim, D. I., Bahar, N., Ramos, M., Young, K. S., Roger, C. M., Ho, N. R., Aum, & Cheng, C. (2014). Epidemiology of internet behaviors and addiction among adolescents in six Asian countries. Cyberpsychology Behavior and Social Networking,17(11), 720–728. https://doi.org/10.1089/cyber.2014.0139
Lemola, S., Perkinson-Gloor, N., Brand, S., Dewald-Kaufmann, J. F., & Grob, A. (2015). Adolescents’ electronic media use at Night, Sleep Disturbance, and depressive symptoms in the Smartphone Age. Journal of Youth and Adolescence,44(2), 405–418. https://doi.org/10.1007/s10964-014-0176-x
Li, G., Hou, G., Yang, D., Jian, H., & Wang, W. (2019). Relationship between anxiety, depression, sex, obesity, and internet addiction in Chinese adolescents: A short-term longitudinal study. Addictive Behaviors,90, 421–427. https://doi.org/10.1016/j.addbeh.2018.12.009
Li, Y. Y., Sun, Y., Meng, S. Q., Bao, Y. P., Cheng, J. L., Chang, X. W., Ran, M. S., Sun, Y. K., Kosten, T., Strang, J., Lu, L., & Shi, J. (2021). Internet addiction increases in the General Population during COVID-19: Evidence from China. The American Journal on Addictions,30(4), 389–397. https://doi.org/10.1111/ajad.13156
Liang, S., Ren, Z., & Yang, G. (2022). Cross-sectional and prospective association between internet addiction and risk of fatigue among Chinese college students. Medicine (Baltimore),101(33), e30034. https://doi.org/10.1097/md.0000000000030034
Mabrur, I. A. M., & Suwartono, T. (2021). Junior high school students’ readiness to participate in e-learning and online EFL classes during the COVID‐19 pandemic. International Social Science Journal,71(241–242), 153–161. https://doi.org/10.1111/issj.12271
Manea, L., Gilbody, S., & McMillan, D. (2012). Optimal cut-off score for diagnosing depression with the Patient Health Questionnaire (PHQ-9): A meta-analysis. Cmaj,184(3), E191–E196. https://doi.org/10.1503/cmaj.110829
Nickerson, A., Schick, M., Schnyder, U., Bryant, R. A., & Morina, N. (2017). Comorbidity of posttraumatic stress disorder and depression in Tortured, Treatment-seeking refugees. Journal of Traumatic Stress,30(4), 409–415. https://doi.org/10.1002/jts.22205
Niu, H., Wang, S., Tao, Y., Tang, Q., Zhang, L., & Liu, X. (2023). The association between online learning, parents’ marital status, and internet addiction among adolescents during the COVID-19 pandemic period: A cross-lagged panel network approach. Journal of Affective Disorders,333, 553–561. https://doi.org/10.1016/j.jad.2023.04.096
Obeid, S., Saade, S., Haddad, C., Sacre, H., Khansa, W., Al Hajj, R., Kheir, N., & Hallit, S. (2019). Internet addiction among Lebanese adolescents: The role of Self-Esteem, anger, Depression, anxiety, social anxiety and fear, Impulsivity, and Aggression—A cross-sectional study. The Journal of Nervous and Mental Disease,207(10), 838–846. https://doi.org/10.1097/NMD.0000000000001034
Pan, Y. C., Chiu, Y. C., & Lin, Y. H. (2020). Systematic review and meta-analysis of epidemiology of internet addiction. Neuroscience and Biobehavioral Reviews,118, 612–622. https://doi.org/10.1016/j.neubiorev.2020.08.013
Reed, P., & Reay, E. (2015). Relationship between levels of problematic internet usage and motivation to study in university students. Higher Education,70(4), 711–723. https://doi.org/10.1007/s10734-015-9862-1
Salmela-Aro, K., Upadyaya, K., Hakkarainen, K., Lonka, K., & Alho, K. (2017). The Dark Side of Internet Use: Two Longitudinal Studies of Excessive Internet Use, Depressive Symptoms, School Burnout and Engagement Among Finnish Early and Late Adolescents. Journal of Youth and Adolescence,46(2), 343–357. https://doi.org/10.1007/s10964-016-0494-2
Seki, T., Hamazaki, K., Natori, T., & Inadera, H. (2019). Relationship between internet addiction and depression among Japanese university students. Journal of Affective Disorders,256, 668–672. https://doi.org/10.1016/j.jad.2019.06.055
Spitzer, R. L., Kroenke, K., Williams, J. B., & Löwe, B. (2006). A brief measure for assessing generalized anxiety disorder: The GAD-7. Archives of Internal Medicine,166(10), 1092–1097. https://doi.org/10.1001/archinte.166.10.1092
Stanković, M., Nešić, M., Čičević, S., & Shi, Z. (2021). Association of smartphone use with depression, anxiety, stress, sleep quality, and internet addiction. Empirical evidence from a smartphone application. Personality and Individual Differences,168, 110342. https://doi.org/10.1016/j.paid.2020.110342
Stevens, M. W. R., King, D. L., Dorstyn, D., & Delfabbro, P. H. (2019). Cognitive–behavioral therapy for internet gaming disorder: A systematic review and meta-analysis. Clinical Psychology and Psychotherapy,26(2), 191–203. https://doi.org/10.1002/cpp.2341
Tang, Q., Zou, X., Gui, J., Wang, S., Liu, X., Liu, G., & Tao, Y. (2024). Effects of childhood trauma on the symptom-level relation between depression, anxiety, stress, and problematic smartphone use: A network analysis. Journal of Affective Disorders,358, 1–11. https://doi.org/10.1016/j.jad.2024.05.018
Tao, Y., Niu, H., Hou, W., Zhang, L., & Ying, R. (2023a). Hopelessness during and after the COVID-19 pandemic lockdown among Chinese college students: A longitudinal network analysis. Journal of Clinical Psychology,79(3), 748–761. https://doi.org/10.1002/jclp.23439
Tao, Y., Niu, H., Li, Y., Liu, X., Wang, S., Ma, Z., Hou, W., & Liu, X. (2023b). Effects of personal relative deprivation on the relationship between anger rumination and aggression during and after the COVID-19 pandemic lockdown: A longitudinal moderated network approach. Journal of Adolescence,95(3), 596–608. https://doi.org/10.1002/jad.12140
Tao, Y., Niu, H., Tang, Q., Wang, S., Zhang, L., Liu, G., & Liu, X. (2024a). The association between online learning, perceived parental relationship, anxiety, and depression symptoms among secondary school students: insight from symptom network and cross-lagged panel network approach. BMC Public Health,24(1), 2133. https://doi.org/10.1186/s12889-024-19675-4
Tao, Y., Tang, Q., Wang, S., Zou, X., Ma, Z., Zhang, L., Liu, G., & Liu, X. (2024b). The impact of long-term online learning on social anxiety and problematic smartphone use symptoms among secondary school students with different levels of fear of missing out: Evidence from a symptom network and longitudinal panel network analysis. Journal of Behavioral Addictions,13(1), 102–119. https://doi.org/10.1556/2006.2023.00081
Tao, Y., Zou, X., Tang, Q., Hou, W., Wang, S., Ma, Z., Liu, G., & Liu, X. (2024c). Mapping network connection and direction between anxiety and depression symptoms across the early, middle, and late adolescents: Insights from a large Chinese sample. Journal of Psychiatric Research,169, 174–183. https://doi.org/10.1016/j.jpsychires.2023.11.035
Tateno, M., Teo, A. R., Shiraishi, M., Tayama, M., Kawanishi, C., & Kato, T. A. (2018). Prevalence rate of internet addiction among Japanese college students: Two cross-sectional studies and reconsideration of cut‐off points of Young’s internet addiction test in Japan. Psychiatry and Clinical Neurosciences,72(9), 723–730. https://doi.org/10.1111/pcn.12686
Thapar, A., Eyre, O., Patel, V., & Brent, D. (2022). Depression in young people. Lancet,400(10352), 617–631. https://doi.org/10.1016/S0140-6736(22)01012-1
Tian, Y., Zhou, M., Wang, L., & Qin, N. (2022). The associations between Depression and Internet Addiction in University students during COVID-19 pandemic period: A cross-lagged analysis. Chinese Journal of Clinical Psychology,30(2), 295–300. https://doi.org/10.16128/j.cnki.1005-3611.2022.02.010
Wang, D., Zhao, J., Ross, B., Ma, Z., Zhang, J., Fan, F., & Liu, X. (2022). Longitudinal trajectories of depression and anxiety among adolescents during COVID-19 lockdown in China. Journal of Affective Disorder,299, 628–635. https://doi.org/10.1016/j.jad.2021.12.086
Woods, H. C., & Scott, H. (2016). Sleepyteens: Social media use in adolescence is associated with poor sleep quality, anxiety, depression and low self-esteem. Journal of Adolescence,51, 41–49. https://doi.org/10.1016/j.adolescence.2016.05.008
Young, K. S. (1998). Internet addiction: The emergence of a New Clinical Disorder. Cyberpsychology & Behavior,1(3), 237–244. https://doi.org/10.1089/cpb.1998.1.237
Zhang, L., Tao, Y., Hou, W., Niu, H., Ma, Z., Zheng, Z., Wang, S., Zhang, S., Lv, Y., Li, Q., & Liu, X. (2022). Seeking bridge symptoms of anxiety, depression, and sleep disturbance among the elderly during the lockdown of the COVID-19 pandemic-A network approach. Frontiers in Psychiatry,13, 919251. https://doi.org/10.3389/fpsyt.2022.919251
Zhao, Y., Qu, D., Chen, S., & Chi, X. (2023). Network analysis of internet addiction and depression among Chinese college students during the COVID-19 pandemic: A longitudinal study. Computers in Human Behavior,138, 107424–107424. https://doi.org/10.1016/j.chb.2022.107424
Acknowledgements
This study was supported by the college students’ mental health education center, Northeast Agricultural University. This study thanks Jie Gui for valuable discussion from Jiangsu Vocational College of Information and Technology. Finally, we would like to extend our sincere gratitude to Zou Xinyuan from the Faculty of Psychology, Beijing Normal University, for her invaluable assistance in the revision process.
Funding
The key subject of the Ministry of Education in the 2023 National Education Science Program: “Empowering College Students’ Mental Health Monitoring and Applications with Artificial Intelligence Technology” (DIA230433).
Author information
Authors and Affiliations
Contributions
Study design: Xiangping Liu. Data collection: Liang Zhang. Analysis and interpretation: Yanqiang Tao. Drafting of the manuscript: Yanqiang Tao. Critical revision of the manuscript: Shujian Wang, and Zijuan Ma.
Corresponding author
Ethics declarations
Ethical approval
The research was examined and approved by the ethics committee of Beijing Normal University (Reference number: 202112220085).
Informed consent
Informed consent was obtained from all individual participants included in the study.
Competing interests
The authors have no conflicts of interest regarding this research study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Tao, Y., Wang, S., Ma, Z. et al. The effect of long-term online learning on anxiety, depression, and internet addiction among secondary school students: insight from a cross-lagged panel network approach. Curr Psychol (2024). https://doi.org/10.1007/s12144-024-06477-5
Accepted:
Published:
DOI: https://doi.org/10.1007/s12144-024-06477-5