
Abstract
Despite the apparent association between depressive experience and life satisfaction, little is known whether the two constructs are linked under a causal process. Previous investigations have suggested correlations based on the between-person differences, but such mere presence of cross-sectional association is insufficient to claim whether depressive experiences share concurring bases with cognitive evaluation of life satisfaction. This study thus focused on identifying the contemporaneous correlation between experiences of depression and life satisfaction and tested whether complex subcomponents of well-being intercorrelate in a time-synchronized way. This study utilized a dataset including adults from midlife to older age in the Korean Longitudinal Study of Aging (KLoSA). The survey assessed depressive symptoms and domains of satisfaction throughout eight waves of repeated follow-ups every 2 years. The analysis examined the associations with between-person (cross-sectional) and within-person (longitudinal) effects. We found that the extent of longitudinal correlation between the two constructs was generally lower in the within-person than between-person associations, indicated as temporal asynchrony. The satisfactions in domains of health and economic status showed a relatively higher within-person correlation while satisfaction in spousal and children relationships showed minimalized within-person correlations. The result suggests that the link between depressive experience and life satisfaction is less concurrent, ruling out the explanatory model that views subjective well-being as a direct causal construction of affective experience within a specific time point. Our finding implies that the observed association between depressive symptoms and life satisfaction is largely based on accumulated through lifetime indirect pathways rather than direct reference of appraised information.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
In explaining intercorrelations between various indicators of psychological well-being, the frameworks in revealing the association between measurements strongly depend on whether the researcher takes into account temporal variabilities or not. Two forms of framework can be contrasted, in that whereas cross-sectional correlation captures shared variability about the coexistence of variables at one moment in time at the group level, dynamic longitudinal correlation captures how these variables relate to each other over time within individuals (i.e., inter-individual versus intra-individual). Unarguably, it has been pointed out that between-person variations are more compounded with multiple sources of causal underpinnings other than the very psychological process, which leaves the majority of cross-sectional observations unelucidated (Rohrer & Murayama, 2023). The overlooked nature of temporal variability of mental health indicators can lead to a significant drawback since a lack of personalized models of psychopathology lures erroneous intervention targets or less timed strategies that imply low relevance to individual processes (Wright & Woods, 2020).
With regard to this critical awareness, studies in the field of depression research have also aimed to compare how depressive symptoms exhibit a formal structure of correlations with one another and how such associations differ by the methodological approaches: cross-sectional or time-series longitudinal data (Wichers et al., 2021). The temporal dynamics of depressive disorder have been historically recognized, and the disorder was previously categorized as a mood disorder that characterizes fluctuating symptoms. Depression may be indicative of varying individuals including those showing stably low or high symptoms over time or some other individuals that show temporary exacerbation or a period of a depressive episode within a confined timeframe (Nelson et al., 2017). The empirical investigations also showed that a strong between-person correlation of depressive symptoms does not correspond to the structures of within-person symptom changes, and such inconsistencies have led to highlighting the importance of assessing intensive longitudinal data (Hamaker & Wichers, 2017; Kievit et al., 2013). Specifically, some depressive experiences (e.g., sadness) exhibit a high correlation in cross-sectional designs but such pattern is not supported in designs of temporal correlation (Wichers et al., 2021). It is typically construed that The cross-sectional design may roughly reflect correspondence as a trait-level explanation, whereas the longitudinal design is more reflective of state-specific properties (Brose et al., 2019), thus requiring differential interpretation in their causal assumption.
Exploring the individual-level variability of depressive symptoms may also be relevant in understanding how they are theoretically linked to a more extended construct of well-being (Pavot & Diener, 2008). According to the tripartite formulation of Subjective Well-Being (SWB), the construct of SWB is viewed as a composition of two affective experiences (positive and negative affect) and the overall cognitive appraisal (life satisfaction) (Diener, 1984). While there is a broad consensus that affective and evaluative elements constitute SWB, there remains debate about the nature of relationships between the compositions and the underlying causal basis that the tripartite constructs work. Multiple models have been proposed to explain the relationships between the affective and appraisal components of SWB and these models can be broadly differentiated based on their extent of assumptions on a causal basis (Busseri & Sadava, 2011). First, the ‘composite model’ suggests that there is no inherent need for a causal link between affective experiences and the cognitive appraisal of life satisfaction; they are simply seen as independently separated components (Heintzelman et al., 2020; Joshanloo, 2016; Kapteyn et al., 2015). This perspective negates the presence of a meaningful relationship between affective experience and the concept of SWB can be viewed as a compound of external connotations. In contrast, according to the ‘causal system model’ the subcomponents of emotional experience and cognitive evaluation are viewed as causally interconnected. In other words, individuals rely on various pieces of information to evaluate the satisfaction of their lives, including the effects they experience, both positive and negative (Joshanloo & Jovanović, 2021; Schimmack et al., 2002; Schimmack & Oishi, 2005; Schwarz & Strack, 1991). Along with affective experience, episodes of depressed mood can also be easily accessible in evaluating life satisfaction and can be utilized to construct life satisfaction online. Put together, the underlying causal assumption on the psychological phenomenon fundamentally differs between the two models, and this leads to significant differences in interpreting the outcomes of SWB and depression measures (Edwards & Bagozzi, 2000; Fried, 2017).
There have been studies aiming to empirically verify and explore the relationships between the subcomponents of SWB, but there is room for improvement in specific methodological approaches. Specifically, the previous studies examined predictive relationships between the SWB components over a longer time range, spanning almost a decade, assuming that life satisfaction should be influenced by affective states from a decade ago (Busseri, 2015; Metler & Busseri, 2017). Such an approach, however, attempted to link the components beyond an overly extended time that may not be indicative of causal paths. Instead, the investigation should have examined whether relatively recent affective experiences are being taken into account when evaluating life satisfaction, and whether such accessibility of information is observed as temporal coherency or synchrony across an extended period. If the temporal coherency between affective experiences and cognitive evaluation is observed to be weak, it may otherwise suggest a weak theoretical basis for claiming that causal dynamics constitute SWB. In other words, such a result would suggest opposing evidence for the ‘causal system model.’
Moreover, in the search for longitudinal observational studies, researchers have been exploring the experiential effects on well-being, but most study designs focus on micro-timescales (hours of time gap) that investigate the influence of transient states (de Vries et al., 2021). Even in the recent micro-longitudinal investigation, the time gaps between the waves were around days to weeks (Busseri & Quoidbach, 2022). Such an approach, however, may be awry from the evaluative nature of life satisfaction in that momentary assessment does not consider experiences aggregated over time (Steptoe, 2019). Studies examining dynamics at the levels of multiple years are exceedingly rare, and extended time-ranged design is required to reflect different entities of dynamics.
Lastly, another complication of depression is that clinical features may be affected by late-life psychosocial and biological changes with aging (Grayson & Thomas, 2013). In the period of midlife and later ages, transitions in health and socioeconomic status profoundly affect well-being and psychological distress (Sivertsen et al., 2015). Despite ample evidence of relevant psychosocial factors, the conclusions remain unclear in differentiating whether the intercorrelated factors of depressive symptoms in later life are a mere reflection of pre-existing individual differences rather than ongoing within-individual changes of symptoms limited in the timeframe of middle and later life.
The main research goal is to test the ‘causal system model’ of SWB with regard to depressive symptoms. The current study aimed to examine two main goals: (1) Identify the presence and extent of contemporaneous association between depressive experience and life satisfaction, and (2) determine whether the presenting contemporaneous structure maps onto specific domains of satisfaction. Based on a representative longitudinal panel dataset, we utilized 14 years of repeated measures of depressive symptoms and life satisfaction. By comparing cross-sectional (between-person) and longitudinal (within-person) association strengths, we aimed to explore how late-life depressive symptoms dynamically fluctuate with major domains of life satisfaction, and how it mismatches with cross-sectional inference. This examination thus attempts to delineate the structural models of SWB components that include affective experiences and cognitive appraisal. The within-person temporal coherence should be observed if any of the latent factors or direct influence is causally concurring between the SWB components. On the contrary, if the relationship only holds in a cross-sectional approach, the evidence that life satisfaction refers to the concurring depressive mood in evaluation would be unsupported.
Method
Participants
The analysis was based on nationally representative data collected in the Korean Longitudinal Study of Aging (KLoSA), which has followed up with individuals aged 45 or older since August 2006. The panel was randomly sampled under stratified residential districts and housing types. The KLoSA protocol was approved by the Institutional Review Board of the Korea Centers for Disease Control and Prevention. All participants provided written informed consent. The survey was conducted by trained interviewers in face-to-face home visits. The survey was conducted once in two years, and the total dataset utilized eight waves from 2006 to 2020. To maximize the intra-individual variabilities, the participants with full adherence (8-time points, 14 years) were analyzed in the final dataset.
The participants suspected to have cognitive impairment were screened by age-, gender-, and education-specified norms (≥ 2 standard deviations) of the Korean version of the Mini-Mental State Examination (K-MMSE) (Han et al., 2008). The participants under the age of 60 were applied with the closest age norm of 60 to 64. The cases with any missing variables were excluded. The participants without current spouses or children were also excluded.
To minimize the possible dropout rates at the later period of old-old ages, the analysis was confined to the age ranges from 45 to 70 at the initial wave, which covers longitudinal effects across midlife to older ages. The final dataset included 636 participants with full adherence in eight waves (Table 1).
Depressive symptoms
Depressive symptoms were measured by the Center for Epidemiological Studies Depression (CES-D) scale (Kohout et al., 1993). CES-D scales each item by the frequency (days) of a specified symptom during the last week by response categories of “hardly ever,” “some of the time,” or “most of the time.” The shorter version has been validated in the population of either older adults or East-Asian culture (Boey, 1999; Irwin et al., 1999; Lee & Chokkanathan, 2008). Due to item updates made in the fifth wave survey (from Andersen to Boston Form), the three items of CES-D were excluded from the analysis. The current study utilized seven items that were consistently applied in the eight following waves.
The items included five negative-loaded items (depressed mood, effortful daily activity, sleep difficulty, feeling lonely, cannot get going) and two positive-loaded items (doing well, without much complaint). The positive-loaded items were reverse-coded. The main analysis utilized the total sum score of CES-D and additionally explored two sum scores of negatively and positively loaded items respectively. In the current dataset, the correlations between the CES-D items were moderately strong when cross-sectionally averaged across eight waves (within negative items: r = 0.40 ~ 0.62; within positive items: r = 0.73). On the other hand, the correlations between positive- and negative-sum scores showed a weak association across eight waves (r = 0.00 ~ 0.25). The internal consistency in the first wave showed that items were within an acceptable/questionable range of reliability (Cronbach alpha = 0.60). A previous study showed a moderate to strong association between CES-D and affective experience, and proved indicative of state measures of PANAS (Positive and Negative Affective Schedule) (Terracciano et al., 2003).
Satisfaction
Overall status of well-being was measured with ratings on four domains (health, economic status, relationship with children, relationship with spouse), followed by a single item of overall life satisfaction (Frisch et al., 2005; Huebner, 1994). A previous study showed sound psychometric properties and validity of single-item satisfaction item measures (Cheung & Lucas, 2014). The satisfaction level was measured with a 100-point rating scale and the response scales ranged from 0 (completely dissatisfied) to 100 (completely satisfied). The wave-averaged partial correlation coefficient between overall life satisfaction and the other four life domain satisfactions ranged from 0.52 to 0.59 when controlling for age, gender, and education. The internal consistency across five satisfaction measures in the first wave showed a moderate level of reliability (Cronbach alpha = 0.78).
Statistical analysis
The main scope of the study focused on the association between depressive symptoms and satisfaction ratings (five measures). The two forms of correlation were compared: inter-individual and intra-individual correlation. The inter-individual associations were assessed with average coefficients of cross-sectional partial correlation across eight waves. The partial correlation indicated Pearson’s correlation coefficient while controlling for the shared effects of age, sex, and education.
The intra-individual associations were assessed with the repeated measures correlation (RMC) method (Bakdash & Marusich, 2017). RMC is a statistical technique for determining the overall within-individual association for paired measures assessed on two or more occasions for multiple individuals (Bland & Altman, 1995). By utilizing analysis of covariance (ANCOVA), which typically adjusts for inter-individual variability, RMC removes measured variance of between-subject effects. In this way, the RMC method finds the best linear fit for each participant using parallel regression lines (same slopes) with varying intercepts. The RMC coefficient calculates the correlation coefficient by a root-squared ratio of (the predicted sum of squares/total sum of squares) ranging from − 1 to 1. The 95% confidence interval was referred to determine the statistical significance of coefficients and differences between coefficients.
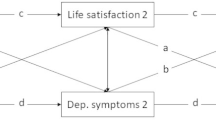
The overall gaps between the cross-section partial correlation and longitudinal repeated correlation were interpreted as the relative importance of within- or between-person effects between the variables of interest. Schematic illustration shows the simplified cases when the effect of within- or between-person association mismatches. The exemplar case shows inconsistent directionality signs (i.e., Simpson’s paradox) (Fig. 1A), or attenuated association (Fig. 1B) in the repeated correlation. The two forms of correlation were subtracted to indicate the discrepant association effects.

Schematic illustration of differences in the within-person and between-person association. (A) Disagreeing signs of association of positive within-person effect and negative between-person effect. (B) Attenuated within-person association compared to the between-person association
Results
For the descriptive purpose, the longitudinal patterns of depressive symptoms (CES-D) and satisfaction ratings were shown across eight waves (Fig. 2). While some individuals showed temporally coinciding patterns of fluctuation (i.e., simultaneous increase or decrease), other individuals showed no such correspondence.

Seven individual example cases illustrate heterogeneous trajectories of inversed satisfaction (mean of five domains) and depressive symptoms (CES-D total score). Line colors indicate an individual’s longitudinal trajectories. Individual lines were fitted across repeated measures of eight waves. Lines were smoothed using the locally weighted smoothing (LOESS) method
The within-person variability (time-series standard deviation across eight waves) yielded a single measure of variability and its populational distribution. The within-person variations (Mean intra-subject variability: 10.9 ~ 13.2) were relatively lower than between-subject variations (SD: 14.4 ~ 18.7) (Table 2).
The two forms of correlation between depressive symptoms and life satisfaction domains were compared by between-person effect (cross-sectional partial correlation) and within-person effect (longitudinal repeated correlation). When examining associations, within-person correlation showed generally lower association strength than averaged between-person correlations (Fig. 3). The extent of the decrease in correlation coefficient ranged from 0.08 to 0.20. According to confidence interval ranges, the within-person association of health satisfaction remained highest compared to other satisfaction domains. The cross-sectional partial correlations showed a statistically significant positive association between depressive symptoms and the five satisfaction domains when all of the waves were lumped into the analysis set (r = -0.28 ~ -0.19, df = 5085).

Comparison between between-person partial correlation and within-person contemporaneous correlation. Correlations are between depressive symptoms (CES-D total score) and five domains of Satisfaction levels. Satisfaction levels include domains of health, economic status, spousal relationship, children relationship, and overall life domain. Error bars indicate 95% confidence interval. Coefficients and confidence intervals were averaged across eight waves in the cross-sectional results
When the association was separately examined by two depressive sub-scores (positive and negative), it showed that negative-loaded item scores (e.g. depressive mood) showed a relatively stronger association with satisfaction level than positive-loaded (e.g. doing well) in both methods of correlation approaches (Table 3). More specifically, the attenuated within-person correlation was more prominent between negative-loaded depressive symptoms and health satisfaction (coefficient decrease of 0.13). On the other hand, the attenuated association was prominent between positive depressive symptoms and social relationship satisfaction (coefficient decrease of 0.15 ~ 0.17).
Discussion
The current study examined the cross-sectional and longitudinal association between depressive symptoms and life satisfaction domains from midlife to older ages. The main aim was to determine whether the well-known association between life satisfaction and affective experience can also be observed in a temporally coherent way. The results revealed that within-person contemporaneous correlations were profoundly lower than between-person cross-sectional correlations. Moreover, such discrepant results were prominent in domains of interpersonal satisfaction rather than in health and economic satisfaction.
It was first shown that the overall directionality of the correlation remained consistent, but the strength of association became weaker in the within-person correlation. This main finding indicates that a major proportion of temporal fluctuations from depressive symptoms are reflective of between-person differences rather than dynamics of within-person processes. Such distinguished pattern was consistent with the previous study which compared the structural model of between- and within-person affective experiences (Möwisch et al., 2019). It showed that the within-person variability required more narrowly defined affective boundaries to build a better model. In other words, within-person variabilities were not effectively covered by broad higher-order latent factors (e.g., negative affectivity), and the model required further differentiation of lower-level sub-facets. For example, individuals may exhibit a stronger tendency to show negative affectivity of both anger and worrying, but such tendency may not be observed at a within-person level, in that one may not report both affective states simultaneously. Likewise, the current study finding suggests that the seemingly related constructs share less of a within-person process, and also suggest that the constructs of both depressive symptoms and domains of life satisfaction can be dissociated when assessed at specific time points.
Another implication from the lowered within-person correlation is how the components of SWB (affective experience and evaluative satisfaction) interact with each other. In the same vein, previous work showed that the prospective predictability of affective experience on life satisfaction was minimal, and concluded from these confined results that the relationship between the two components was less likely to be causal (Busseri, 2015). Recent work from the same research group extended the previous finding and suggested weak evidence of a causal link between the SWB components (Busseri & Quoidbach, 2022). Though the analytic rationale of these investigations fundamentally differed from the current study, it points to similar conclusions. As shown in the within-person correlations, the causal basis underlying affective experience and life satisfaction lacked supporting evidence and the observed relationship would be largely indirect.
Indeed, while causal effects cannot be definitively concluded from the observational study (Rohrer & Murayama, 2023), there are some lists of possible explanation that generates such indirect effects. The between-person association that is not manifested as within-person correlation may indicate other sources of variation, namely pre-existing individual differences that have been accumulated before the entrance of the selected age range (i.e., late midlife). Some previous evidence also suggests that individual differences that compose between-person correlations may emerge from accumulated influence between the multitude of variables, rather than from concurring psychological processes of lower-level sub-facets (Gustavson et al., 2012).
The secondary finding was the significantly lower within-person correlation between depressive symptoms and social relationship satisfaction, and that such lacking contemporaneous association was more prominent than other domains of satisfaction. This suggests that individuals with dissatisfactory relationships tended to show higher depressive symptoms, but higher depressive symptoms at a specific time point were not accompanied by relationship dissatisfaction. On the contrary to the low within-person association, previous studies have noted late-life interpersonal stressors as a major factor that accounts for depressive symptoms (Burger et al., 2020; Fried et al., 2015). However, the discordant associations necessitate time-dependent explanations of how interpersonal stressors play a role in late-life depression. One possible reason is that interpersonal conflict and stressors especially in intimate and familial relationships tend to be chronic in nature and difficult to be terminated during later life. One previous study suggested that the presenting effect of relationship stressors in later life can be substantial, but the effect tends to persist for several years (Krause & Rook, 2003). Moreover, in the same research, they showed that interpersonal problems in one’s social relationship (e.g., with children) tended to recur in others as well (e.g., with friends), suggesting the construct generalizes to overall dissatisfaction rather than operating in a time-constrained way. This implies that late-life social relationship quality correlates with depressive symptoms in a more endogenous way (i.e., effect of inner psychological process), rather than an exogenous way (i.e., effect of external events).
Contrary to the disagreeing observations in interpersonal satisfaction, economic status, and health showed a relatively lower discrepancy between the two approaches, which suggests that some proportion of between-person effects were temporally coherent variabilities across 14 years of late-life trajectory. Despite previous evidence that the impact of fixed socioeconomic status grows weaker at later ages, the dynamic relationship between wealth and subjective well-being has been supported by longitudinal studies or quasiexperimental design (George, 2010; Ong et al., 2019; Sobel et al., 2019). Likewise, newly occurring economic strain can play a larger role in constituting well-being during later ages (Chiao et al., 2012). Such additional burdens during later life may also hold true in the domain of health, as shown in the previous research that showed the shifting importance of health factors in the composition of SWB (Windle et al., 2010). These lines of research suggest that individuals undergo significant changes in physical health and economic status during the midlife and late-life period and this correspondence of fluctuation highlights how the influx of health and economic burden can signify the occurrence of clinical depression.
The current study findings comprehensively suggest that the formerly known relationship between depression and life satisfaction should represent trait-level correlations, and require multiple alternative explanations other than state-level inference. Taken together, the trait-level association may appear in either time-mismatched or time-invariant effects.
Lastly, the current study findings provide implications for how the construct of SWB is heterogeneously configured within a specific population. Previous literature suggests that older population and non-individualistic cultural contexts tend to put less weight on hedonic experience on SWB and invest less in the extent to which they value pleasant emotional experiences (Joshanloo, 2019; Lee et al., 2020; Suh et al., 1998). Lacking evidence of common temporal coherence between depressive experience and life satisfaction suggests that older adults’ affective experiences are less likely to be referred to in the evaluation of overall life quality.
The current study shares the aim with recent approaches that similarly compare the difference between longitudinal and cross-sectional symptomatology. Notably, however, it should be noted that the current study design took advantage of a relatively long measurement interval between the waves (i.e., 2 years). Overall, the strength of the current study regards the extent of the time range that covered 14 years of longitudinal assessment which may have enabled the study to encompass the time-constrained nature of depressive symptoms. As depicted in the illustrative example (Fig. 2), heightened depressive symptoms do not tend to persist through the years, and such a pattern strongly questions previous investigations that have set a narrow time scope. The analytic scope of the current study can be of specific strength since the fluctuating nature of depressive symptoms and other affective processes can profoundly differ by the scope of time frames, and the current study interpretation needs to be confined to the process of slow waxes and wanes that last months or years (Dormann & Griffin, 2015). Unlike momentary experiences of affectivity, depressive syndrome can prevail as “episodes” that last months or years (Ferrari et al., 2013). Thus, measurement intervals in the current study on a longer time scale can provide an extensive picture of symptomatology that expands to a longer lifespan.
There are several critical limitations that need further discussion. First, the current study lacks formal diagnostic information on major depressive disorder. The positive predictive value of the short-version of CES-D has been reported low (35%) in the previous validation study (Irwin et al., 1999), and the overreliance on such self-report scales may have led to increased prevalence. In other words, the cases of increased CES-D scores can be easily observed not due to depressive symptoms but due to other general distress or demoralization. Thus, the current study should be cautious in extending the conclusions to the conceptualization of clinical diagnosis of depressive disorders. Second, the large dropouts throughout longitudinal follow-up indicate that the current dataset is highly biased to include exceptionally healthy older adults who maintained the eight waves of the survey. Thus, individuals who were under chronically active symptoms may not have been included in the dataset. Lastly, the current investigation focusing on contemporaneous correlation may have missed time-lagged effects between the two constructs of interest. Although previous literature suggests that the effect of life stressor on depressive symptoms in older adults tend to be exhibited in a concurrent way rather than in a time-lagged way (Dautovich et al., 2014), the indirectness of the causal link may be suggestive of numerosity of causal pathways generates cross-sectional association rather than a lack of true linkage.
In sum, we provided findings that depressive symptom correlation with life satisfaction can differ by the temporal source of variation. Our findings provide insight that requires future endeavors to examine how the well-known risk factors of depression should be cautiously interpreted when drawn from cross-sectional research.
Data availability
The KLoSA data are publicly available and downloadable from the employment survey site and nationally representative sample cohort studies including anthropometric and psychosocial data. The final dataset is available in the repository (https://data.mendeley.com/datasets/4jxchjhvbp/1).
References
Bakdash, J. Z., & Marusich, L. R. (2017). Repeated measures correlation. Frontiers in Psychology, 8(MAR), 456. https://doi.org/10.3389/FPSYG.2017.00456/BIBTEX.
Bland, M., & Altman, D. G. (1995). Calculating correlation coefficients with repeated observations: Part 1–Correlation within subjects. BMJ: British Medical Journal, 310(6977), 446. https://doi.org/10.1136/BMJ.310.6977.446.
Boey, K. W. (1999). Cross-validation of a short form of the CES-D in Chinese elderly. International Journal of Geriatric Psychiatry, 14(8), 608–617. https://doi.org/10.1002/(SICI)1099-1166(199908)14:8608::AID-GPS9913.0.CO;2-Z.
Brose, A., Schmiedek, F., Gerstorf, D., & Voelkle, M. C. (2019). The measurement of within-person affect variation. Emotion. https://doi.org/10.1037/EMO0000583.
Burger, J., Stroebe, M. S., Perrig-Chiello, P., Schut, H. A., Spahni, S., Eisma, M. C., & Fried, E. I. (2020). Bereavement or breakup: Differences in networks of depression. Journal of Affective Disorders, 267(November 2019), 1–8. https://doi.org/10.1016/j.jad.2020.01.157.
Busseri, M. A. (2015). Toward a resolution of the tripartite structure of Subjective Well-Being. Journal of Personality, 83(4), 413–428. https://doi.org/10.1111/jopy.12116.
Busseri, M. A., & Quoidbach, J. (2022). The structure of everyday happiness is best captured by a latent subjective well-being factor. Journal of Research in Personality, 96(July 2021), 104177. https://doi.org/10.1016/j.jrp.2021.104177.
Busseri, M. A., & Sadava, S. W. (2011). A review of the tripartite structure of Subjective Well-Being: Implications for conceptualization, operationalization, analysis, and synthesis. Personality and Social Psychology Review, 15(3), 290–314. https://doi.org/10.1177/1088868310391271.
Cheung, F., & Lucas, R. E. (2014). Assessing the validity of single-item life satisfaction measures: Results from three large samples. Quality of Life Research, 23(10), 2809–2818. https://doi.org/10.1007/S11136-014-0726-4/TABLES/6.
Chiao, C., Weng, L. J., & Botticello, A. L. (2012). Economic strain and well-being in late life: Findings from an 18-year population-based longitudinal study of older Taiwanese adults. Journal of Public Health, 34(2), 217–227. https://doi.org/10.1093/pubmed/fdr069.
Dautovich, N. D., Dzierzewski, J. M., & Gum, A. M. (2014). Older adults display concurrent but not delayed associations between Life stressors and depressive symptoms: A Microlongitudinal Study. The American Journal of Geriatric Psychiatry, 22(11), 1131–1139. https://doi.org/10.1016/J.JAGP.2013.02.008.
de Vries, L. P., Baselmans, B. M. L., & Bartels, M. (2021). Smartphone-based Ecological Momentary Assessment of Well-Being: A systematic review and recommendations for Future studies. Journal of Happiness Studies, 22(5), 2361–2408. https://doi.org/10.1007/s10902-020-00324-7.
Diener, E. (1984). Subjective well-being. Psychological Bulletin, 95(3), 542–575. https://doi.org/10.1037/0033-2909.95.3.542.
Dormann, C., & Griffin, M. A. (2015). Optimal time lags in panel studies. Psychological Methods, 20(4), 489–505. https://doi.org/10.1037/MET0000041.
Edwards, J. R., & Bagozzi, R. P. (2000). On the nature and direction of relationships between constructs and measures. Psychological Methods, 5(2), 155–174. https://doi.org/10.1037/1082-989X.5.2.155.
Ferrari, A. J., Somerville, A. J., Baxter, A. J., Norman, R., Patten, S. B., Vos, T., & Whiteford, H. A. (2013). Global variation in the prevalence and incidence of major depressive disorder: A systematic review of the epidemiological literature. Psychological Medicine, 43(3), 471–481. https://doi.org/10.1017/S0033291712001511.
Fried, E. I. (2017). What are psychological constructs? On the nature and statistical modelling of emotions, intelligence, personality traits and mental disorders. 11(2), 130–134. https://doi.org/10.1080/17437199.2017.1306718
Fried, E. I., Nesse, R. M., Guille, C., & Sen, S. (2015). The differential influence of life stress on individual symptoms of depression. Acta Psychiatrica Scandinavica, 131(6), 465–471. https://doi.org/10.1111/acps.12395.
Frisch, M. B., Clark, M. P., Rouse, S. V., Rudd, M. D., Paweleck, J. K., Greenstone, A., & Kopplin, D. A. (2005). Predictive and Treatment Validity of Life Satisfaction and the Quality of Life Inventory. 12(1), 66–78. https://doi.org/10.1177/1073191104268006.
George, L. K. (2010). Still happy after all these years: Research Frontiers on Subjective Well-being in later life. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 65B(3), 331–339. https://doi.org/10.1093/geronb/gbq006.
Grayson, L., & Thomas, A. (2013). A systematic review comparing clinical features in early age at onset and late age at onset late-life depression. Journal of Affective Disorders, 150(2), 161–170. https://doi.org/10.1016/j.jad.2013.03.021.
Gustavson, K., Røysamb, E., von Soest, T., Helland, M. J., Karevold, E., & Mathiesen, K. S. (2012). Reciprocal longitudinal associations between depressive symptoms and romantic partners’ synchronized view of relationship quality. Journal of Social and Personal Relationships, 29(6), 776–794. https://doi.org/10.1177/0265407512448264.
Hamaker, E. L., & Wichers, M. (2017). No Time like the Present. Current Directions in Psychological Science, 26(1), 10–15. https://doi.org/10.1177/0963721416666518.
Han, C., Jo, S. A., Jo, I., Kim, E., Park, M. H., & Kang, Y. (2008). An adaptation of the Korean mini-mental state examination (K-MMSE) in elderly koreans: Demographic influence and population-based norms (the AGE study). Archives of Gerontology and Geriatrics, 47(3), 302–310. https://doi.org/10.1016/J.ARCHGER.2007.08.012.
Heintzelman, S. J., Kushlev, K., Lutes, L. D., Wirtz, D., Kanippayoor, J. M., Leitner, D., Oishi, S., & Diener, E. (2020). ENHANCE: Evidence for the efficacy of a comprehensive intervention program to promote subjective well-being. Journal of Experimental Psychology: Applied, 26(2), 360–383. https://doi.org/10.1037/xap0000254.
Huebner, E. S. (1994). Preliminary Development and Validation of a multidimensional life satisfaction scale for children. Psychological Assessment, 6(2), 149–158. https://doi.org/10.1037/1040-3590.6.2.149.
Irwin, M., Artin, K. H., & Oxman, M. N. (1999). Screening for Depression in the older Adult: Criterion Validity of the 10-Item Center for Epidemiological Studies Depression Scale (CES-D). Archives of Internal Medicine, 159(15), 1701–1704. https://doi.org/10.1001/ARCHINTE.159.15.1701.
Joshanloo, M. (2016). Factor structure of Subjective Well-being in Iran. Journal of Personality Assessment, 98(4), 435–443. https://doi.org/10.1080/00223891.2015.1117473.
Joshanloo, M. (2019). Lay conceptions of Happiness: Associations with reported Well-Being, personality traits, and Materialism. Frontiers in Psychology, 10, https://doi.org/10.3389/fpsyg.2019.02377.
Joshanloo, M., & Jovanović, V. (2021). Similarities and differences in predictors of life satisfaction across age groups: A 150-country study. Journal of Health Psychology, 26(3), 401–411. https://doi.org/10.1177/1359105318819054.
Kapteyn, A., Lee, J., Tassot, C., Vonkova, H., & Zamarro, G. (2015). Dimensions of Subjective Well-Being. Social Indicators Research, 123(3), 625–660. https://doi.org/10.1007/s11205-014-0753-0.
Kievit, R. A., Frankenhuis, W. E., Waldorp, L. J., & Borsboom, D. (2013). Simpson’s paradox in psychological science: a practical guide. Frontiers in Psychology, 4. https://doi.org/10.3389/fpsyg.2013.00513.
Kohout, F. J., Berkman, L. F., Evans, D. A., & Cornoni-Huntley, J. (1993). Two shorter forms of the CES-D (Center for Epidemiological Studies Depression) depression symptoms index. Journal of Aging and Health, 5(2), 179–193. https://doi.org/10.1177/089826439300500202.
Krause, N., & Rook, K. S. (2003). Negative Interaction in Late Life: Issues in the Stability and Generalizability of Conflict Across relationships. The Journals of Gerontology: Series B, 58(2), P88–P99. https://doi.org/10.1093/geronb/58.2.P88.
Lee, A. E. Y., & Chokkanathan, S. (2008). Factor structure of the 10-item CES-D scale among community dwelling older adults in Singapore. International Journal of Geriatric Psychiatry, 23(6), 592–597. https://doi.org/10.1002/GPS.1944.
Lee, S. H., Choi, I., Choi, E., Lee, M., Kwon, Y., Oh, B., & Cole, S. W. (2020). Psychological well-being and gene expression in Korean adults: The role of age. Psychoneuroendocrinology, 120, 104785. https://doi.org/10.1016/j.psyneuen.2020.104785.
Metler, S. J., & Busseri, M. A. (2017). Further evaluation of the tripartite structure of Subjective Well-Being: Evidence from longitudinal and experimental studies. Journal of Personality, 85(2), 192–206. https://doi.org/10.1111/jopy.12233.
Möwisch, D., Schmiedek, F., Richter, D., & Brose, A. (2019). Capturing Affective Well-being in Daily Life with the Day Reconstruction Method: A Refined View on positive and negative affect. Journal of Happiness Studies, 20(2), 641–663. https://doi.org/10.1007/s10902-018-9965-3.
Nelson, B., McGorry, P. D., Wichers, M., Wigman, J. T. W., & Hartmann, J. A. (2017). Moving from static to dynamic models of the onset of mental disorder a review. JAMA Psychiatry, 74(5), 528–534. https://doi.org/10.1001/jamapsychiatry.2017.0001.
Ong, Q., Theseira, W., & Ng, I. Y. H. (2019). Reducing debt improves psychological functioning and changes decision-making in the poor. Proceedings of the National Academy of Sciences, 116(15), 7244–7249. https://doi.org/10.1073/pnas.1810901116.
Pavot, W., & Diener, E. (2008). The satisfaction with Life Scale and the emerging construct of life satisfaction. The Journal of Positive Psychology, 3(2), 137–152. https://doi.org/10.1080/17439760701756946.
Rohrer, J. M., & Murayama, K. (2023). These are not the effects you are looking for: Causality and the Within-/Between-Persons distinction in Longitudinal Data Analysis. Advances in Methods and Practices in Psychological Science, 6(1), 251524592211408. https://doi.org/10.1177/25152459221140842.
Schimmack, U., & Oishi, S. (2005). The influence of chronically and temporarily accessible information on life satisfaction judgments. Journal of Personality and Social Psychology, 89(3), 395–406. https://doi.org/10.1037/0022-3514.89.3.395.
Schimmack, U., Oishi, S., & Diener, E. (2002). Cultural influences on the relation between pleasant emotions and unpleasant emotions: Asian dialectic philosophies or individualism-collectivism? Cognition and Emotion, 16(6), 705–719. https://doi.org/10.1080/02699930143000590.
Schwarz, N., & Strack, F. (1991). Context effects in attitude surveys: Applying cognitive theory to Social Research. European Review of Social Psychology, 2(1), 31–50. https://doi.org/10.1080/14792779143000015.
Sivertsen, H., Bjørkløf, G. H., Engedal, K., Selbæk, G., & Helvik, A. S. (2015). Depression and quality of life in older persons: A review. In Dementia and Geriatric Cognitive Disorders (Vol. 40, Issues 5–6, pp. 311–339). Karger Publishers. https://doi.org/10.1159/000437299.
Sobel, I., Semyonov, M., & Lewin-Epstein, N. (2019). The Dynamic Relationship Between Wealth and Subjective Well-Being Among Mid-Life and Older Adults in Israel. In C. S. Gaël Brulé (Ed.), Wealth (s) and subjective well-being (pp. 415–442).
Steptoe, A. (2019). Happiness and health. Annual Review of Public Health, 40(1), 339–359. https://doi.org/10.1146/annurev-publhealth-040218-044150.
Suh, E., Diener, E., Oishi, S., & Triandis, H. C. (1998). The shifting basis of life satisfaction judgments across cultures: Emotions versus norms. Journal of Personality and Social Psychology, 74(2), 482–493. https://doi.org/10.1037/0022-3514.74.2.482.
Terracciano, A., McCrae, R. R., & Costa, P. T. (2003). Factorial and construct validity of the Italian positive and negative affect schedule (PANAS). European Journal of Psychological Assessment, 19(2), 131–141. https://doi.org/10.1027//1015-5759.19.2.131.
Wichers, M., Riese, H., Hodges, T. M., Snippe, E., & Bos, F. M. (2021). A narrative review of Network studies in Depression: What different methodological approaches tell us about Depression. Frontiers in Psychiatry, 12, 1865. https://doi.org/10.3389/FPSYT.2021.719490/BIBTEX.
Windle, G., Woods, R. T., & Markland, D. A. (2010). Living with Ill-Health in older age: The role of a resilient personality. Journal of Happiness Studies, 11(6), 763–777. https://doi.org/10.1007/s10902-009-9172-3.
Wright, A. G. C., & Woods, W. C. (2020). Personalized Models of Psychopathology. In Annual Review of Clinical Psychology (Vol. 16, Issue 1, pp. 49–74). Annual Reviews. https://doi.org/10.1146/annurev-clinpsy-102419-125032.
Acknowledgements
This work was supported by the Ministry of Education of the Republic of Korea and the National Research Foundation of Korea (NRF-2022S1A5A8055166).
Funding
This work was supported by the Ministry of Education of the Republic of Korea and the National Research Foundation of Korea (NRF- 2022S1A5A8055166).
Author information
Authors and Affiliations
Contributions
SK conducted designing, analyzing, manuscript writing.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest.
Ethics approval
The study procedure was reviewed by the Institutional Review Board (IRB) of the Pusan National University, and it received an IRB waiver of consent because the study is a secondary analysis study using de-identified and public-use data (PNU IRB/2023_128_HR).
Informed consent
The patients/participants provided their written informed consent to participate in this study.
All participants informed consent form.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Kwak, S. Longitudinal asynchrony between depressive symptoms and life satisfaction: a 14-year contemporaneous correlation. Curr Psychol 43, 15611–15620 (2024). https://doi.org/10.1007/s12144-023-05543-8
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12144-023-05543-8