
Abstract
Studies show that mothers with depression are more likely to engage in unsupportive emotion-related socialization behaviors, and mothers’ negative emotion socialization can interfere with the development of emotion regulation in children. However, insufficient studies examine the relationship between mothers’ depressive symptoms, emotion socialization, and children’s emotion regulation. The present study used short-term longitudinal data to investigate the mediating role of maternal emotion socialization on the effect of maternal depressive symptoms on children’s emotion regulation. Participants included 180 mothers of six-to-12-year-old children. First, we measured maternal depressive symptoms and mothers’ reactions to their children’s negative emotions, operationalizing emotion socialization. Then we collected data about the children’s emotion regulation reported by mothers six months later. A structured equation modeling analysis indicated that maternal emotion socialization completely mediated the impact of mothers’ depressive symptoms on children’s emotion regulation with a significant indirect effect. The present study used short-term longitudinal data and highlighted the significant impact of mothers’ depressive symptoms on children’s emotion regulation mediated by maternal emotion socialization. The results suggest a need for early detection and appropriate intervention of mothers’ depressive symptoms. Even for mothers with depression, efforts to recognize and improve their emotion-related parenting behavior could be helpful for their children.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Between 10 and 20% of the world’s population suffers from temporary or persistent depression during their lifetime, and the prevalence in women is 1.5 times higher than in men (Kessler et al., 2013; World Health Organization, 2021). An individual’s depression can make it difficult to function in daily life and directly or indirectly affect those close to them. In particular, a mother with depression can significantly affect her children’s emotions, development, and future mental health (Goodman, 2007; Goodman et al., 2011; Lovejoy et al., 2000). Previous studies have reported the effects of mothers’ depressive symptoms on children’s various outcomes. For example, children with depressed mothers have an increased risk of depressive disorders and other internalized or externalized disorders, and researchers also report difficulties in academic achievement (Gajios & Beaver, 2017; Gibb et al., 2012; Goodman et al., 2011; Kuckertz et al., 2018; O’Connor et al., 2018). In addition, researchers have examined how maternal depression affects children’s development, explicitly noting disruptions in the development of emotion regulation (Feng et al., 2008; Silk et al., 2006).
Emotion regulation is an external and internal process that involves the individual’s monitoring, evaluation, and modification of emotional responses to achieve specific goals (Thompson, 1994). Children’s emotion regulation ability plays a significant role in improving present adaptation and decreasing future psychopathologies (Cole et al., 2009; Zahn–Waxler et al., 2000). Moreover, maternal depression is one of the crucial factors causing individual differences in children’s emotion regulation capacity (Boedeker et al., 2019; Hoffman et al., 2006; Marcal, 2021). Thus, researchers examined several paths of the adverse effects of maternal depression on children’s emotion regulation (Goodman, 2007; Marcal, 2021). For instance, depression can prevent mothers from having sufficient energy and the ability to respond to children’s demands. Specifically, since the mother experiences an overload of negative emotions, it decreases her emotional availability and reduces her sensitivity and reactivity to her children. In addition, it can also lower her tolerance for her children’s maladaptive behaviors (Boedeker et al., 2019; Hoffman et al., 2006; Kuckertz et al., 2018; Lin et al., 2019). Consequently, mothers with depression tend to respond to their children in less structured ways, feel increased irritability, and behave more invasively because they have trouble regulating their emotions (Marcal, 2021; Nickerson et al., 2011). Ultimately, they may become the models for less effective emotion regulation strategies, inhibiting the expression of positive emotions and adaptively regulating negative emotions (Marcal, 2021; Premo & Kiel, 2016; Thomassin et al., 2017; Wu et al., 2017).
Mothers’ depressive symptoms and emotion socialization
Emotion socialization is an emotion-related parenting behavior vital in developing children’s emotions and emotion regulation capacity (Spinrad et al., 2020). It is a process in which children learn to accept, regulate, and cope with their expressed emotions based on their parents’ reactions (Eisenberg et al., 1998). In particular, parents’ supportive or unsupportive responses to children’s negative emotions play an essential role as a direct coach or indirect model in helping the child learn to experience, express, and handle negative emotions such as anxiety, anger, and sadness (Eisenberg et al., 1998; Jones et al., 2002).
Several studies have found that parents’ psychopathology, especially the mother’s depression, relates to negative emotion socialization (Breaux et al., 2016; Hastings et al., ;2014 Labella et al., 2021). Depressed mothers are less sensitive to the cues of their children’s negative emotions than non-depressed mothers, so they may not be able to identify children’s negative emotions or provide sufficient support (Boedeker et al., 2019). Therefore, they tend not to let their children express negative emotions adequately or accept them (Lin et al., 2019). They are also likely to be unsupportive of their children’s negative emotions and sometimes overwhelmed, so they show unregulated responses (Bao & Kato, 2020; Silk et al., 2006). Such responses result in emotion socialization, inhibiting children from developing appropriate ways of handling their negative emotions.
Emotion socialization and emotion regulation
Children usually acquire emotion regulation ability through the socialization process in the family, in which mothers play crucial roles as the primary caregivers during their children’s early childhood (Morris et al., 2017). In addition, previous studies about emotion socialization highlighted the familial environment during the developmental process of emotion regulation (Eisenberg et al., 1998). Mothers can provide emotion socialization via various routes, including encouraging children to express their emotions, soothing negative emotions, or teaching adaptive strategies. For example, if mothers encourage children to express and accept negative emotions, their children can alleviate and recover their negative emotions (Eisenberg et al., 2001). Moreover, when seeking how to cope with and solve stressors that cause children’s negative emotions, parents can help children learn problem-solving skills (Silk et al., 2011). For instance, when mothers respond supportively to negative emotions, their children develop positive emotion regulation capacity. However, mothers’ non-supportive reactions relate to negative emotionality and emotion regulation difficulties from early childhood to adolescence. Namely, minimizing the severity of what situations children identify, responding punitively to children’s negative emotional expressions, or showing distress reactions eventually result in various adverse outcomes (Breaux et al., 2018; Briscoe et al., 2019; Cole et al., 2009; Fabes et al., 1990; Hooper et al., 2018; O’Neal & Magai, 2005).
Present Study
While previous research looked at the various paths linking mother’s depressive symptoms to children’s adverse outcomes (Kuckertz et al., 2018; Marcal, 2021), few studies investigated emotion socialization as a mediating variable (Briscoe et al., 2019; Wu et al., 2017). Specifically, not many studies examined the effect of emotion socialization with a prospective design focusing on children’s emotion regulation. Therefore, the current study aimed to examine whether maternal emotion socialization mediates the effect of mothers’ depressive symptoms on children’s emotion regulation with a short longitudinal design. We hypothesized that mothers with depression present negative emotion socialization, negatively affecting children’s emotion regulation ability after six months.
Method
Participants and procedure
A total of 180 mothers with school-aged children in Korea participated in the present study. This study originated from a project investigating the cross-sectional relationship between mothers’ parenting and children’s adjustment, after which we planned additional research to examine the longitudinal effects of mothers’ depressive symptoms and emotion socialization on children’s emotion regulation. The institutional review board of the researcher’s university approved this additional study. Six months after the completion of the first project, we re-recruited the parents among 809 participants from the earlier study, and 207 parents agreed to participate in the current study. Researchers handed study questionnaires to children at school to deliver to their mothers who had agreed to participate. The mothers filled out the questionnaires at home, sealed them, and the children returned them to the school; the researchers collected the questionnaires from the school. In addition, the researchers provided the participants with brief feedback on the results of the K-CBCL, which assessed their children’s behavior problems. There was no penalty for withdrawing participation.
Finally, we analyzed data from 180 participants, excluding data from 24 participants who were fathers or other caregivers and three who omitted their demographic information. As the result of checking whether the mothers and children participating in this study differ from those participating only in the first round, there was no significant difference between the two groups in mothers’ depressive symptoms and emotion socialization and children’s emotion regulation. The mothers’ mean age was 41.06 (SD = 3.79), and the range was 29–51 years. The children of participants included 93 girls and 87 boys, and the average age was 9.35 years (SD = 1.76).
Measures
Mothers’ depressive symptoms
We measured mothers’ depressive symptoms with the Korean version of the Center for Epidemiologic Studies Depression Scale-Revised (K-CES-D-R; Lee et al., 2016). K-CES-D-R is a 20-item scale that asks respondents to rate how often they have experienced symptoms associated with depression over the past week, such as restless sleep, poor appetite, and loneliness. We translated and standardized the K-CES-D-R from CES-D-R (Eaton et al., 2004), derived from CES-D developed by Radloff (1977). Scores range from 0 to 60, with higher scores indicating more severe depressive symptoms. The internal consistency was 0.98 in the standardization study of the Korean version (Lee et al., 2016) and 0.88 in this study.
Emotion socialization
Mothers completed the Korean version (Kim, 1995) of the Coping with Children’s Negative Emotions Scale (CCNES; Fabes et al. 1990) to measure parental emotion socialization. The CCNES includes 12 hypothetical scenarios in which a child is upset, sad, or angry (e.g., “If my child becomes angry because he/she is sick or hurt and can’t go to his/her friend’s birthday party, I would. . .”). For each scenario, mothers responded on a seven-point Likert scale indicating the likelihood that they would react in expressive encouragement, emotion-focused, problem-focused, minimizing, punishing, or distress reactions. We categorized the results into “supportive” and “non-supportive” emotion socialization practices (Fabes et al., 2001).
“Supportive reactions” included expressive encouragement (e.g., “Encourage my child to express his/her feelings of anger and frustration”), emotion-focused (e.g., “Comfort my child and try to make his/her feel better”), and problem-focused reactions (e.g., “Help my child think about ways that he/she can still be with friends). The “non-supportive reactions” included punitive (e.g., “Send my child to his/her room to cool off), minimization (e.g., “Tell my child not to make a big deal out of missing the party”), and distress reactions (e.g., “Distressed myself when children express negative emotion”). We found good reliability for the CCNES and the Korean version of the CCNIES. Cronbach’s alphas were 0.94–0.95 for expressive encouragement, emotion-focused, and problem-focused responses in supportive reactions and 0.85–0.92 for punitive, minimizing, and distressing responses in non-supportive reactions in the present study.
In the current study, for the structural equation modeling analysis, we named “supportive reactions” as “lack of supportive reactions” after reverse-coding so that higher scores indicated a more remarkable lack of supportive reactions. Finally, we used “lack of supportive reactions” and “non-supportive reactions” as measurement variables of emotion socialization. In this study, Cronbach’s alphas of “lack of supportive reactions” and “non-supportive reactions” were 0.88 and.89, respectively.
Children’s emotion regulation
Mothers assessed children’s emotion regulation ability using the Emotion Regulation Checklist (ERC), developed by Shields and Cicchetti (1997) and translated into the Korean language by Choi and Oh (2014). An adult familiar with the child, such as a parent or teacher, can complete the ERC. The ERC evaluates emotionality (affective lability, intensity, balance, flexibility, and appropriateness of expression of emotion) and is an important emotion regulation process. Based on the results of factor analysis on the data of 513 children between the ages of six and 12 years, Shields and Cicchetti (1997) divided the ERC into two subscales: lability/negativity (comprising items about mood swings, reactivity, emotion intensity, and dysregulated positive emotion), and emotion regulation (covering equanimity, emotional understanding, and empathy). Cronbach’s alphas were 0.89 for the overall scale, 0.96 for lability/negativity, and 0.83 for emotion regulation in Shields and Cicchetti (1997). In Choi and Oh (2014), Cronbach’s alphas were 0.86 and 0.76 for lability/negativity and emotion regulation subscales, respectively. In this study, we renamed emotion regulation to dysregulation after reverse-coding to prevent a negative correlation between two variables measuring one latent variable. Cronbach’s alphas were 0.72 for lability/negativity and 0.74 for dysregulation.
Data analyses
We used SPSS 24.0 to conduct a descriptive and one-way analysis of variance (ANOVA). Three participants had one or two missing values in the total responses. To investigate the impact of missing data, we performed Little’s (1988) Missing Completely at Random (MCAR) test. Results supported the MCAR assumption, χ2 (897) = 921.666, p = .277. Thus, we concluded that we could estimate missing data in SPSS with an expectation–maximization procedure. However, we analyzed the correlation between variables before examining the mediating model. Since the age of children can affect emotion regulation capacity, we included it in the correlation analysis. However, we excluded it from the mediating model because there was no significant correlation.
We used the maximum likelihood estimation of SEM models to examine the mediating effect of maternal emotion socialization on the relationship between mothers’ depressive symptoms and children’s emotion regulation difficulties. We performed structural equation modeling (SEM) with AMOS 25.0 (Arbukle, 2015). In addition, we examined the model fit using the comparative fit index (CFI), Bentler–Bonett Normed Fit Index (NFI), and root mean square error of approximation (RMSEA). Conventionally, CFI and NFI values that are greater than 0.90 and an RMSEA value that is closer to zero are indicative of an acceptable model fit. To determine the significance of the mediating and indirect effects, we used the bias-corrected percentile confidence intervals yielded by 1,000 bootstrap iterations (Preacher & Hayes, 2008). We considered the mediation effects statistically significant if a zero value did not feature within the 95% confidence intervals of the bootstrap samples.
Results
Correlation analysis
Table 1 presents the correlation analysis and descriptive statistics (i.e., means and standard deviations). The results showed significant correlations between mothers’ depressive symptoms, two types of emotion socialization, and two dimensions of children’s emotion regulation (r = .17–0.36, p = .23–0.00). Lack of supportive and non-supportive reactions showed significant positive correlations with emotion dysregulation (r = .23, p = .01; r = .24, p = .01, respectively) but was not significant with lability/negativity. The age of the children did not significantly correlate with any variables.
Structural equation modeling analyses
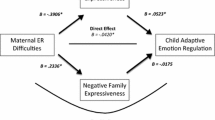
We conducted structural equation modeling (SEM) analysis to examine the mediating effect of maternal emotion socialization on the relationship between mothers’ depressive symptoms and children’s emotion regulation. The results revealed a good model fit (χ2 (df = 3, N = 180) = 4.64, n.s; CFI = 0.98; NFI = 0.96; RMSEA = 0.055, 90% CI = 0.000–0.148). Moreover, we found an association between mothers’ depressive symptoms and maternal emotion socialization (β = 0.45, p = .002), which in turn related to children’s emotion regulation after six months (β = 0.36, p = .043). However, the direct effect of mothers’ depressive symptoms was no longer significant, meaning maternal emotion socialization mediated the relationship between mothers’ depressive symptoms and children’s emotion regulation completely. By bootstrapping, examining the indirect effect of mothers’ depressive symptoms on children’s emotion regulation after six months through emotion socialization yielded the following results: β = 0.16, 95% CI = 0.00–0.45, illustrated in Fig. 1.

Structured Equation Model and Standardized Path Coefficients
Note. N = 180. ES = Emotion Socialization. *p < .05; **p < .01; ***p < .001.
Discussion
The present study evaluated the short-term longitudinal association between mothers’ depressive symptoms, emotion socialization, and children’s emotion regulation in a Korean community sample. SEM analysis indicated a significant complete mediating effect of maternal emotion socialization between mothers’ depressive symptoms and children’s emotion regulation. In addition, mothers’ depressive symptoms predicted their negative emotion socialization. There have been various studies on depressed mothers’ difficulties in parenting. For instance, mothers with depression show less availability, sensitivity, reactivity, and support during interactions with their children (Lin et al., 2019; Lovejoy et al., 2000). By contrast, sometimes, they are more likely to be hostile or dysregulate their reaction toward their children because they have weak stress tolerance (Bao & Kato, 2020; Priel et al., 2020; Silk et al., 2006). We found an association between a mother’s depressive symptoms and maternal emotion socialization, defined operationally as reactions to children’s negative emotions. This finding is consistent with previous studies relating mothers’ affective disorders and negative emotionality to negative emotion socialization (Briscoe et al., 2019; Labella et al., 2021). In addition, this study’s meaningfulness is in examining the study model with school-aged children, while previous studies focused on infants or preschool children (Breaux et al., 2016; Premo & Kiel, 2016).
While we also found a significant association between depressive symptoms and a lack of supportive responses, the correlation with non-supportive responses was stronger. Supportive reactions include encouraging children to express negative emotions such as anger and sadness, accepting those expressions, helping them recover their negative emotions, and coping with stress that causes negative emotions. Mothers’ non-supportive responses involve minimizing the situation’s perceived severity, punishing the negative emotional expression, and getting distressed herself. Previous studies also reported that depression showed a stronger relationship with non-supportive reactions (Breaux et al., 2016; Silk et al., 2011). It might be related to mothers with depression being better able to recall what they did wrong rather than what they lacked. Considering inconsistencies between recalls of depressed mothers’ reactions from the mothers and young adult children (Labella et al., 2021), mothers with depression may tend to over-report non-supportive responses. In addition, we confirmed that mothers’ depressive symptoms and emotion socialization had a prospective association with children’s emotion regulation. This result is similar to previous studies that reported children with emotion regulation problems were likely to have a depressed mother (Lin et al., 2019; Thomassin et al., 2017). Moreover, it is consistent with significant associations of maternal emotion socialization with children’s emotion regulation (Premo & Kiel, 2016; Price & Kiel, 2022).
We used two subscales to measure children’s emotion regulation, i.e., emotion regulation which we renamed dysregulation, and liability/negativity. The former is about how well children understand and react to emotions, while the latter relates to how labile or strong children express their emotions. We found a relationship between mothers’ depressive symptoms, dysregulation, and liability/negativity. However, we also found maternal emotion socialization related only to dysregulation. Therefore, emotion socialization affects emotion regulation skills that help children recognize and handle negative emotions. At the same time, we did not find a significant relationship between maternal emotion socialization and emotion lability/negativity. For example, a study with clinical patients pointed out that emotion negativity may stem from children’s innate characteristics (Breaux et al., 2018; Briscoe et al., 2019) also concluded temperament strongly affected negative emotions. Thus, children may inherit their emotion lability/negativity from the mother’s temperamental traits, or the mother’s emotionality or availability may be an influencing factor.
Finally, this study prospectively showed the mediating effect of maternal emotion socialization on the relationship between mothers’ depressive symptoms and children’s emotion regulation. Some studies have examined the relationship between the three variables: mothers’ depressive symptoms, emotion-related parenting behaviors, and children’s emotion regulation (Kuckertz et al., 2018; Wu et al., 2017). In addition, some studies examined the mediating effect of various emotion-related parenting behaviors (e.g., emotion availability, dysregulated maternal care) (Hoffman et al., 2006; Priel et al., 2020). Still, others confirmed the effects of mothers’ depressive symptoms and emotion socialization on children’s various outcomes (Briscoe et al., 2019; Silk et al., 2011; Wu et al., 2017). However, we found no study that directly and prospectively examined the relationship between mothers’ depressive symptoms, maternal emotion socialization, and children’s emotion regulation. We tested the mediation model between the three variables and found that maternal emotion socialization completely mediated the impact of mothers’ depressive symptoms on children’s emotion regulation.
Although there have been many studies on the pathways and mechanisms by which mothers’ depressive symptoms affects children (Boedeker et al., 2019; Goodman, 2007; Hoffman et al., 2006; Nickerson et al., 2011), our results confirmed that the mediating role of negative emotion socialization is essential, at least in children’s emotion regulation. However, as the results of correlation analysis, maternal emotion socialization did not significantly correlate with children’s emotion lability/negativity. Therefore, it is necessary to examine whether a mother’s depressive symptoms and emotion socialization affect the two sub-dimensions of a child’s emotion regulation differently in the future. Children’s emotion regulation ability is the most critical variable that can predict children’s adaptation in the future and present (Cole et al., 2009; Zahn-Waxler et al., 2000). Genetic and environmental factors can affect the development of children’s emotion regulation, and mothers’ depressive symptoms may relate to both aspects (Propper & Moore, 2006). Our findings emphasize emotion socialization as the critical environmental pathway of mothers’ depressive symptoms on children’s emotion regulation.
However, the present study has several limitations. First, the sample size of this study was small. The mediating effect was statistically significant but marginal. If future studies could enroll more participants, researchers could examine whether mothers’ depressive symptoms or emotion socialization have different results depending on children’s emotion regulation subdimensions or whether there are other mediating effects of the two subtypes of maternal emotion socialization. In addition, since we did not initially plan this study as a longitudinal study, only a small percentage of the data collected from the first round responded to the second evaluation. The data of people who only participated in the first round were not significantly different from those who participated in both rounds. However, the possibility of a biased sample still exists.
The second relates to measurement. We measured the CES-D, which asks about symptoms of depression in the last week, only once. To evaluate persistent depression rather than situational depression, we need other questionnaires or repeated measures. Additionally, because we measured all variables through mothers’ self-reports, mothers with depression may perceive their responses as more unsupportive and report their children’s behavior as more dysregulated. Therefore, a multi-faceted evaluation would be helpful, including a child’s report on the mother’s reactions to their negative emotions or a behavioral measurement of the child’s emotion regulation.
Third, data in the present study was from the community population, so the level of mothers’ depressive symptoms was not high. Consequently, these low levels of depression may have influenced the results. Therefore, it may be inappropriate to generalize the current results to mothers whose depression is more than moderate in severity.
Finally, this study implies that the model for the role of a mother’s depression and emotion socialization in the development of children’s emotional regulation, mainly studied in Western cultures, can also apply to Asian cultures that suppress emotional expression more. However, in the future, it would be helpful to investigate what cultural differences exist in the actual patterns of emotion socialization of mothers and their effects on the relationship between mothers’ depression and children’s emotion regulation.
Despite these limitations, the results of the present study have practical implications. Previous studies emphasized the importance of mothers’ emotionality and emotion socialization, especially for preschool-age children (Price & Kiel, 2022; Wu et al., 2017). Our findings suggest mothers’ depressive symptoms and emotion-related socialization behaviors still affect children’s emotion regulation, even in school-aged children. Therefore, interventions for improving the mental health of mothers with school-aged children can prevent children’s maladjustment and enhance their adaptation in the future. It also indicates that interventions based on schools or local communities can be effective. Finally, even in the cases of somewhat depressed mothers, parenting education that focuses on understanding the effects of parenting behaviors (especially emotion socialization) would be helpful to mitigate the negative impact of mothers’ emotional states on a child’s emotionality and emotion regulation.
Data Availability
The data set is available upon request.
Code Availability
Not applicable.
References
Bao, J., & Kato, M. (2020). Determinants of maternal emotion socialization: Based on Belsky’s process of parenting model. Frontiers in Psychology, 11. https://doi.org/10.3389/fpsyg.2020.02044.
Boedeker, K., Fuchs, A., Fuehrer, D., Kluczniok, D., Dittrich, K., Reichl, C., Reck, C., Kaess, M., Hindi Attar, C., Moehler, E., Neukel, C., Bierbaum, A., Zietlow, A., Jaite, C., Lehmkuhl, U., Winter, S. M., Herpertz, S., Brunner, R., Bermpohl, F., & Resch, F. (2019). Impact of maternal early life maltreatment and maternal history of depression on child psychopathology: Mediating role of maternal sensitivity? Child Psychiatry and Human Development, 50(2), 278–290. https://doi.org/10.1007/s10578-018-0839-z.
Breaux, R. P., Harvey, E. A., & Lugo-Candelas, C. I. (2016). The role of parent psychopathology in emotion socialization. Journal of Abnormal Child Psychology, 44(4), 731–743. https://doi.org/10.1007/s10802-015-0062-3.
Breaux, R. P., McQuade, J. D., Harvey, E. A., & Zakarian, R. J. (2018). Longitudinal associations of parental emotion socialization and children’s emotion regulation: The moderating role of ADHD symptomatology. Journal of Abnormal Child Psychology, 46(4), 671–683. https://doi.org/10.1007/s10802-017-0327-0.
Briscoe, C., Stack, D. M., Dickson, D. J., & Serbin, L. A. (2019). Maternal emotion socialization mediates the relationship between maternal and adolescent negative emotionality. Journal of Youth and Adolescence, 48(3), 495–509. https://doi.org/10.1007/s10964-018-0945-z.
Choi, J. Y., & Oh, K. J. (2014). Cumulative childhood trauma and psychological maladjustment of sexually abused children in Korea: Mediating effects of emotion regulation. Child Abuse & Neglect, 38(2), 296–303. https://doi.org/10.1016/j.chiabu.2013.09.009.
Cole, P. M., Dennis, T. A., Smith-Simon, K. E., & Cohen, L. H. (2009). Preschoolers’ emotion regulation strategy understanding: Relations with emotion socialization and child self-regulation. Social Development, 18(2), 324–352. https://doi.org/10.1111/j.1467-9507.2008.00503.x.
Eaton, W. W., Smith, C., Ybarra, M., Muntaner, C., & Tien, A. (2004). Center for epidemiologic Studies Depression Scale: Review and revision (CESD and CESD-R). In M. E. Maruish (Ed.), The use of psychological testing for treatment planning and outcomes assessment: Instruments for adults (pp. 363–377). Lawrence Erlbaum Associates Publishers.
Eisenberg, N., Cumberland, A., & Spinrad, T. L. (1998). Parental socialization of emotion. Psychological Inquiry, 9(4), 241–273. https://doi.org/10.1207/s15327965pli0904_1.
Eisenberg, N., Cumberland, A., Spinrad, T. L., Fabes, R. A., Shepard, S. A., Reiser, M., & Guthrie, I. K. (2001). The relations of regulation and emotionality to children’s externalizing and internalizing problem behavior. Child Development, 72(4), 1112–1134. https://doi.org/10.1111/1467-8624.00337.
Fabes, R. A., Eisenberg, N., & Bernzwing, J. (1990). The comping with children’s negative emotion scale: Procedures and scoring [Unpublished doctoral dissertation]. Arizona State University, Tempe, USA.
Fabes, R. A., Leonard, S. A., Kupanoff, K., & Martin, C. L. (2001). Parental coping with children’s negative emotions: Relations with children’s emotional and social responding. Child Development, 72(3), 907–920. https://doi.org/10.1111/1467-8624.00323.
Feng, X., Shaw, D. S., Kovacs, M., Lane, T., O’Rourke, F. E., & Alarcon, J. H. (2008). Emotion regulation in preschoolers: The roles of behavioral inhibition, maternal affective behavior, and maternal depression. Journal of Child Psychology and Psychiatry and Allied Disciplines, 49(2), 132–141. https://doi.org/10.1111/j.1469-7610.2007.01828.x.
Gibb, B. E., Grassia, M., Stone, L. B., Uhrlass, D. J., & McGeary, J. E. (2012). Brooding rumination and risk for depressive disorders in children of depressed mothers. Journal of Abnormal Child Psychology, 40(2), 317–326. https://doi.org/10.1007/s10802-011-9554-y.
Goodman, S. H. (2007). Depression in mothers. Annual Review of Clinical Psychology, 3, 107–135. https://doi.org/10.1146/annurev.clinpsy.3.022806.091401.
Goodman, S. H., Rouse, M. H., Connell, A. M., Broth, M. R., Hall, C. M., & Heyward, D. (2011). Maternal depression and child psychopathology: A meta-analytic review. Clinical Child and Family Psychology Review, 14(1), 1–27. https://doi.org/10.1007/s10567-010-0080-1.
Hastings, P., Klimes-Dougan, B., Kendziora, K., Brand, A., & Zahn-Waxler, C. (2014). Regulating sadness and fear from outside and within: Mothers’ emotion socialization and adolescents’ parasympathetic regulation predict the development of internalizing difficulties. Development and Psychopathology, 26(4pt2), 1369–1384. https://doi.org/10.1017/S0954579414001084.
Hoffman, C., Crnic, K. A., & Baker, J. K. (2006). Maternal depression and parenting: Implications for children’s emergent emotion regulation and behavioral functioning. Parenting: Science and Practice, 6(4), 271–295. https://doi.org/10.1207/s15327922par0604_1.
Hooper, E. G., Wu, Q., Ku, S., Gerhardt, M., & Feng, X. (2018). Maternal emotion socialization and child outcomes among african Americans and European Americans. Journal of Child and Family Studies, 27(6), 1870–1880. https://doi.org/10.1007/s10826-018-1020-9.
Jones, S., Eisenberg, N., Fabes, R. A., & MacKinnon, D. P. (2002). Parents’ reactions to elementary school children’s negative emotions: Relations to social and emotional functioning at school. Merrill-Palmer Quarterly, 48(2), 133–159. https://doi.org/10.1353/mpq.2002.0007.
Kessler, R. C., & Bromet, E. J. (2013). The epidemiology of depression across cultures. Annual Review of Public Health, 34, 119–138. https://doi.org/10.1146/annurev-publhealth-031912-114409.
Kim, H. J. (1995). Mother’s perception of children’s coping with negative emotions [Unpublished master’s thesis]. Sookmyung Women’s University, Seoul, Republic of Korea.
Kuckertz, J. M., Mitchell, C., & Wiggins, J. L. (2018). Parenting mediates the impact of maternal depression on child internalizing symptoms. Depression and Anxiety, 35(1), 89–97. https://doi.org/10.1002/da.22688.
Labella, M., Ruiz, S., Harris, S., & Klimes-Dougan, B. (2021). Emotion socialization in mothers with mood disorders: Affective modeling and recollected responses to childhood emotion. Development and Psychopathology, 33(4), 1156–1169. https://doi.org/10.1017/S0954579420000395.
Lee, H., Oh, S., Lee, K., & Park, J. Y. (2016). Validation of the korean version of Center for epidemiologic Studies Depression Scale-Revised. Cambridge University Press.
Lin, B., Kaliush, P., Conradt, E., Terrell, S., Neff, D., Allen, A., & Crowell, S. (2019). Intergenerational transmission of emotion dysregulation: Part I. Psychopathology, self-injury, and parasympathetic responsivity among pregnant women. Development and Psychopathology, 31(3), 817–831. https://doi.org/10.1017/S0954579419000336.
Little, R. J. (1988). A test of missing completely at random for multivariate data with missing values. Journal of the American Statistical Association, 83(404), 1198–1202. https://doi.org/10.1080/01621459.1988.10478722.
Lovejoy, M. C., Graczyk, P. A., O’Hare, E., & Neuman, G. (2000). Maternal depression and parenting behavior: A meta-analytic review. Clinical Psychology Review, 20(5), 561–592. https://doi.org/10.1016/s0272-7358(98)00100-7.
Marcal, K. E. (2021). Pathways to adolescent emotional and behavioral problems: An examination of maternal depression and harsh parenting. Child Abuse and Neglect, 113, 104917. https://doi.org/10.1016/j.chiabu.2020.104917.
Morris, A. S., Criss, M. M., Silk, J. S., & Houltberg, B. J. (2017). The impact of parenting on emotion regulation during childhood and adolescence. Child Development Perspectives, 11(4), 233–238. https://doi.org/10.1111/cdep.12238.
Nickerson, A., Bryant, R. A., Aderka, I. M., Hinton, D. E., & Hofman, S. F. (2011). The impacts of parental loss and adverse parenting on mental health: Findings from the National Comorbidity Survey – Replication. Psychological Trauma: Theory Research Practice and Policy, 5, 119–127. https://doi.org/10.1037/a0025695.
O’Connor, E. E., Langer, D. A., & Tompson, M. C. (2018). Maternal depression and youth internalizing and externalizing symptomatology: Severity and chronicity of past maternal depression and current maternal depressive symptoms. Journal of Abnormal Child Psychology, 45, 557–568. https://doi.org/10.1007/s10802-016-0185-1.
O’Neal, C. R., & Magai, C. (2005). Do parents respond in different ways when children feel different emotions? The emotional context of parenting. Development and Psychopathology, 17, 467–487. https://doi.org/10.1017/S0954579405050224.
Preacher, K. J., & Hayes, A. F. (2008). Contemporary approaches to assessing mediation in communication research. In A. F. Hayes, M. D. Slater, & L. B. Snyder (Eds.), The Sage sourcebook of advanced data analysis methods for communication research, (pp. 13–54). Sage Publications. https://doi.org/10.4135/9781452272054.n2.
Premo, J. E., & Kiel, E. J. (2016). Maternal depressive symptoms, toddler emotion regulation, and subsequent emotion socialization. Journal of Family Psychology, 30(2), 276–285. https://doi.org/10.1037/fam0000165.
Price, N. N., & Kiel, E. J. (2022). Longitudinal links among mother and child emotion regulation, maternal emotion socialization, and child anxiety. Research on Child and Adolescent Psychopathology, 50(2), 241–254. https://doi.org/10.1007/s10802-021-00804-1.
Priel, A., Zeev-Wolf, M., Djalovski, A., & Feldman, R. (2020). Maternal depression impairs child emotion understanding and executive functions: The role of dysregulated maternal care across the first decade of life. Emotion, 20(6), 1042–1058. https://doi.org/10.1037/emo0000614.
Propper, C., & Moore, G. A. (2006). The influence of parenting on infant emotionality: A multi-level psychobiological perspective. Developmental Review, 26(4), 427–460. https://doi.org/10.1016/j.dr.2006.06.003.
Radloff, L. S. (1977). The CES-D scale: A self-report depression scale for research in the general population. Applied Psychological Measurement, 1(3), 385–401. https://doi.org/10.1177/014662167700100306.
Shields, A., & Cicchetti, D. (1997). Emotion regulation among school-age children: The development and validation of a new criterion Q-sort scale. Developmental Psychology, 33(6), 906–916. https://doi.org/10.1037/0012-1649.33.6.906.
Silk, J. S., Shaw, D. S., Forbes, E. E., Lane, T. L., & Kovacs, M. (2006). Maternal depression and child internalizing: The moderating role of child emotion regulation. Journal of Clinical Child and Adolescent Psychology, 35(1), 116–126. https://doi.org/10.1207/s15374424jccp3501_10.
Silk, J. S., Shaw, D. S., Prout, J. T., O’Rourke, F., Lane, T. J., & Kovacs, M. (2011). Socialization of emotion and offspring internalizing symptoms in mothers with childhood-onset depression. Journal of Applied Developmental Psychology, 32(3), 127–136. https://doi.org/10.1016/j.appdev.2011.02.001.
Spinrad, T. L., Morris, A. S., & Luthar, S. S. (2020). Introduction to the special issue: Socialization of emotion and self-regulation: Understanding processes and application. Developmental Psychology, 56(3), 385–389. https://doi.org/10.1037/dev0000904.
Thomassin, K., Suveg, C., Davis, M., Lavner, J. A., & Beach, S. R. (2017). Coparental affect, children’s emotion dysregulation, and parent and child depressive symptoms. Family Process, 56(1), 126–140. https://doi.org/10.1111/famp.12184.
Thompson, R. A. (1994). Emotion regulation: A theme in search of definition. Monographs of the Society for Research in Child Development, 59(2/3), 25–52. https://doi.org/10.2307/1166137.
World Health Organization (2021, September 13). Depression: Key facts. https://www.who.int/news-room/fact-sheets/detail/depression
Wu, Q., Feng, X., Hooper, E., & Ku, S. (2017). Maternal emotion socialization, depressive symptoms and child emotion regulation: Child emotionality as a moderator. Infant and Child Development, 26(1), e1979. https://doi.org/10.1002/icd.1979.
Zahn-Waxler, C., Klimes-Dougan, B., & Slattery, M. J. (2000). Internalizing problems of childhood and adolescence: Prospects, pitfalls, and progress in understanding the development of anxiety and depression. Development and Psychopathology, 12(3), 443–466. https://doi.org/10.1017/S0954579400003102.
Funding
This research was supported by Inha University (grant no. 68044).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethis approval
The authors’ institutional review board approved this study. The authors performed the research following the ethical standards in the 1964 Declaration of Helsinki and its later amendments.
Consent to participate
All participants provided informed consent to participate in the present study.
Consent for publication
All participants provided informed consent for the data to be published.
Conflicts of Interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Choi, J.Y., Eoh, Y. & Kang, J.H. Emotion socialization mediates the short-term longitudinal relationship between mothers’ depressive symptoms and children’s emotion regulation. Curr Psychol 43, 3599–3606 (2024). https://doi.org/10.1007/s12144-023-04528-x
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12144-023-04528-x