
Abstract
While there is evidence that histories of adverse childhood experiences (ACEs) are common in university students and are associated with an increased risk of mental health difficulties, current research has limited geographic and cross-cultural representation. Comparing ACEs across diverse contexts using a standardized measure can illuminate geographic and sociocultural similarities or differences in exposure. The present study aimed to assess ACE exposure and its relationship with mental health symptoms in university students from seven countries. We sampled 5945 university students from the United States, Canada, England, South Africa, Spain, Argentina, and Uruguay. Participants completed the Adverse Childhood Experiences International Questionnaire (ACE-IQ) and the Inventory of Depression and Anxiety Symptoms (IDAS). Most participants (94.8%) reported exposure to at least one type of ACE and 61% reported exposure to four or more types. Repeated exposure to at least one ACE was reported by 70.2% and repeated exposure to at least four ACEs was reported by 21.2%. Spanish students had significantly lower ACE exposure than other students. Cumulative ACE exposure was significantly higher among students in lower income countries, but when repeated exposure was considered these differences fell away. For the total sample, cumulative ACE exposure was significantly associated with severity of depression symptoms, anxiety symptoms, and suicidality. Findings indicate that universities globally should be guided by a trauma-informed approach that recognizes students as a psychologically vulnerable group carrying a long-standing burden of childhood adversity.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Adverse childhood experiences (ACEs) are defined as “childhood events that vary in severity, are often chronic, and occur in a child’s family or social environment to cause harm or distress” (Kalmakis & Chandler, 2014, p.1497). These events include various forms of childhood abuse and neglect, as well as family stressors such as parental mental illness, incarceration, and divorce. The long-term mental health impacts of ACEs have become increasingly clear. In the general population, adults who have experienced ACEs are more likely than non-exposed adults to develop mood, anxiety, behavioral, and substance use disorders, among others (Kessler et al., 2010). Exposure to multiple ACEs greatly increases this risk: adults who report a history of four or more different ACEs have significantly higher odds of having mental health difficulties than those without this level of exposure (Hamby et al., 2021; Hughes et al., 2017). There is growing evidence that exposure to multiple ACEs results in increased allostatic load and cognitive and emotional deficits that extend into adulthood, creating life-long mental health vulnerabilities (Danese & McEwen, 2012; Grassi-Oliveira et al., 2008; Kim et al., 2013; Pechtel & Pizzagalli, 2011).
While university students are often viewed as a relatively privileged group compared to the general population, accumulating evidence suggests that a history of ACEs is common in higher education samples and predicts an increased risk for mental health disorders (Karatekin, 2018; Watt et al., 2020; Windle et al., 2018). Indeed, a higher number of ACEs predicts worsening of depression, anxiety, and suicidality over just a single semester (Karatekin, 2018). Identifying the extent of ACE exposure in different university populations can inform targeted mental health promotion initiatives and enhanced service provision for at-risk students. However, ACE exposure in university students varies widely across studies, creating a rather confusing picture. Most research has been conducted in the United States, where the proportion of college students reporting at least one ACE has ranged from 48 to 75% (Forster et al., 2018; Karatekin, 2018; Khrapatina & Berman, 2017; Merians et al., 2019; Windle et al., 2018). In the few studies conducted with university populations outside the United States, the percentage of students reporting at least one ACE varies even more considerably: for example, 20% in the Ukraine (Burlaka et al., 2020), 45% in China (Ji & Wang, 2018), 50% in Korea (Kim, 2017), 56% in Northern Ireland (McGavock & Spratt, 2014), 58% in Zambia (Zhang et al., 2020), 74% in both Hong Kong (Ho et al., 2019) and Germany (Wiehn et al., 2018), 79% in South Africa (Mall et al., 2018), 84% in England (Martin-Denham & Donaghue, 2020) and 86% in Eritrea (Kelifa et al. 2021). The proportion that meets the threshold of four ACEs identified by Hughes et al. (2017) as significantly increasing the risk for mental illness is similarly diverse across countries: for example, 32% in Watt et al.’s (2020) United States study, 25% in Germany (Wiehn et al., 2018), 19% in Hong Kong (Ho et al., 2019), 12% in Northern Ireland (McGavock & Spratt, 2014), and 8% in Korea (Kim, 2017).
Direct comparisons of ACE exposure between university students in different countries is limited by measurement variation. For example, some studies have used all ten items from Felliti et al.’s (1998) original ACE measure (Khrapatina & Berman, 2017; Watt et al., 2020; Windle et al., 2018), while some have used only selected items from that scale, leaving out ACEs such as emotional and physical neglect (Burlaka et al., 2020; Karatekin, 2018; Zhang et al., 2020). Others have used a combination of different measures (Ji & Wang, 2018). A few studies (Ho et al., 2019; Kelifa et al., 2021; Kim, 2017; Wiehn et al., 2018) have used the World Health Organization’s (2020) 13-item Adverse Childhood Experiences-International Questionnaire (ACE-IQ), which includes ACEs not measured by Felliti et al.’s (1998) scale, such as peer violence and community violence. Differences in the type and number of ACEs measured, and variation in the wording of items, can considerably hamper an overall picture of ACE exposure in university students worldwide and restrict direct comparisons of ACE exposure across different university samples (Hughes et al., 2017; Lacey & Minnis, 2020). By contrast, using a standardized ACE measure across contexts can provide a clearer overall picture of ACE exposure among students globally and identify real geographic and sociocultural similarities or differences across university populations.
Alhowaymel et al. (2021) argue that “ACEs are influenced by globally diverse cultural, social, environmental, and economic factors” (pg. 22). For example, cultural and contextual norms regarding parental authority, gender roles, and physical punishment can affect the prevalence of different forms of abuse (Finkelhor et al., 2013; Ho et al., 2019). Perceptions of whether behavior is abusive, and the willingness to disclose abusive experiences, may also vary across sociocultural contexts (Fontes & Plummer, 2010). Further, children growing up in lower-income countries may experience more non-abuse family adversity than those residing in higher-income settings (Solberg & Peters, 2020). The limited geographic representation of ACE research with university students restricts the identification of ACE patterns that may be universal or distinct to certain higher education settings. A better understanding of ACE exposure among university students in diverse geographic and socio-cultural contexts will enhance the degree to which campus mental health support programmers can understand and meet the specific needs of their student population.
The present study aimed to assess exposure to a broad range of ACEs in an international sample of university students across seven different countries, using a single standardized measure. Specifically, the aims of the present study were to: 1) examine cumulative exposure to ACEs (that is, the mean total number of ACEs) in the international sample and in each specific country, 2) examine rates of exposure to each category of ACE in the international sample and in each specific country, and 3) examine the association of cumulative ACE exposure with mental health symptoms.
Method
Participants and Procedures
Participants were university students (n = 9171) who were recruited from 12 universities spanning 7 countries (U.S. [five universities across four states: Colorado, New Mexico, New York, Virginia], Argentina, Spain, Uruguay, England, Canada [two universities in Ontario province], and South Africa) between February 2019 and March 2020 to complete an online survey exploring risk and protective factors of substance use outcomes (see Bravo et al., 2021 for more information). Across all sites, students completed the same core battery of measures translated into the native language. To minimize burden on participants, we utilized a planned missing data design (i.e., matrix sampling, Graham et al., 2006; Schafer, 1997) which has been used in other large multi-site college student studies (e.g., Bravo et al., 2018). For the purpose of this study, the analytic sample was limited to the 5945 students who completed the measure of ACEs (of whom 70.1% were female; U.S., [n = 2917; 66.9% female], Canada [n = 1156; 65.5% female], South Africa [n = 472; 82.8% female], Spain [n = 471; 70.7% female], Argentina [n = 520; 76.0% female], Uruguay [n = 90; 91.1% female], England [n = 319; 80.3% female].
For the U.S. sites, Canadian sites, England site, and South African site students were recruited from Psychology Department pools and received research participation credit. In Argentina and Uruguay, students were recruited by disseminating an invitation through online social networks, e-mail listings and flyers, and participants who completed the survey took part in a raffle of prizes (Uruguay: 10 cash prizes [each of ≈US$ 20 at the time]; Argentina: 25 prizes each one of ≈US$ 10 at the time [10 vouchers for a bookstore and 15 cash prizes]). In Spain, an email was sent to all students at a public university located in the Eastern region of Spain inviting them to participate in the research. The participants received 5 euros for completing the survey, which was available until the funds were consumed. Study procedures were approved by the institutional review boards (or their international equivalent) at the participating universities.
Measures
Adverse Childhood Experiences – International Questionnaire (ACE-IQ; WHO, 2020)
The ACE-IQ was developed specifically for use as a cross-national measure of ACEs to allow direct standardized comparisons of ACE exposure, and associated risk factors and outcomes, across different countries (WHO, 2020). The ACE-IQ assesses exposure to 13 categories of adverse experience during childhood. The number of ACE categories to which a respondent was exposed is then summed to create a total or cumulative ACE score, ranging from 0 to 13. There are single items measuring parental mental illness, substance abuse, incarceration, or divorce/separation/death, each with a no/yes response option (scored 0 or 1, respectively). ‘Yes’ responses indicate exposure to that ACE and are counted towards the total ACE score. Family violence, physical abuse, sexual abuse, emotional abuse, physical neglect, emotional neglect, peer bullying, witnessing community violence and exposure to collective violence are each assessed with multiple items (for example, there are two items assessing exposure to physical abuse and three items assessing family violence), all rated on a frequency scale of never, once, a few times, many times. For these nine ACEs, exposure to an ACE requires an affirmative response to at least one item measuring that ACE (for example, exposure to physical abuse requires an affirmative response to at least one of the two items assessing physical abuse). Each ACE category that the participant has been exposed to is scored 1 and counted towards the total ACE score (absence of exposure to an ACE category is scored zero). To distinguish between less and more severe forms of childhood adversity, the ACE-IQ has two different scoring algorithms to determine exposure to these nine ACEs. In the ‘binary’ scoring method, any level of exposure to an ACE (once, a few times or many times) qualifies as an affirmative response and is counted towards the total ACE score. In this method, the total score out of 13 is referred to as the ACE ‘binary’ score. In the ‘frequency’ scoring method, only a response of ‘many times’ (that is, frequent exposure) qualifies as an affirmative response and is counted towards the total ACE score. In this method, the total ACE score out of 13 is referred to as the ACE ‘frequency score’. Sexual abuse is an exception: any level of exposure (single or multiple) qualifies as an affirmative response in both scoring methods.
These scoring methods can be illustrated with the two items measuring physical abuse (did a parent, guardian or other household member spank, slap, kick, punch or beat you up?; and did a parent, guardian or other household member hit or cut you with an object, such as a stick [or cane], bottle, club, knife, whip, etc.?). Physical abuse is counted towards the ACE binary score if the participant responds ‘once’, ‘a few times’ or ‘many times’ to at least one of these items. Physical abuse is counted towards the frequency score only if the participant responds ‘many times’ to at least one of these items. The frequency method therefore uses a higher threshold for identifying ACEs related to violence, abuse, and neglect.
In the current study, we excluded the ACE items assessing exposure to collective violence (e.g., war, terrorism, or militia violence), because over the past 25 years this form of violence has been rare in the countries sampled. Our study therefore included 12 of the 13 ACEs on the ACE-IQ, with a total possible score of 12 for both the binary and frequency scoring methods.
In this study, we report the mean total or cumulative ACE score for each country and the total sample, using both the binary and the frequency scoring algorithms. We also report the rate of exposure to each ACE category (that is, the proportion of participants in each country and the total sample that endorsed each ACE), using both the binary and the frequency scoring methods. Finally, we assess whether the binary and the frequency cumulative scores are associated with mental health symptoms. The predictive validity of both the binary and the frequency ACE-IQ total scores has previously been established (Kidman et al., 2019; Kim, 2017).
The ACE-IQ was beta-tested across the different English-speaking sites and no adaptations in wording were deemed necessary. To adapt the ACE-IQ for the Spanish-speaking sites in Spain, Argentina, and Uruguay, four Spanish and Argentinian researchers proficient in English and with expertise in test adaptation and childhood adversity translated the measure independently. After reaching agreement for the Spanish-Argentinian and Spanish-Castilian versions, minor changes were made to keep the final Spanish version as similar as possible across sites. However, some minor differences across Spanish measures were retained to correctly adapt the measure to the cultural context (for example, we kept “cachetada” in the Argentinian version while we kept the term “bofetada” in the Castilian Spanish version to refer to “being slapped”). The versions for Uruguay and Argentina were identical.
Inventory of Depression and Anxiety Symptoms (IDAS; Watson et al., 2007)
The IDAS is a 64-item measure of mental health. Participants reported how much they have felt or experienced each item during the past two weeks using a 5-point Likert Scale (1 = not at all, 5 = extremely). The IDAS contains 10 specific symptom scales (suicidality, lassitude, insomnia, appetite loss, appetite gain, ill temper, wellbeing, panic, social anxiety, and traumatic intrusions) and two broader scales (general depression and dysphoria). For purposes of the present study, we examined the following seven symptom scales: general depression (α = .92), insomnia (α = .82), suicidality (α = .87), ill temper (α = .74), social anxiety (α = .87), panic (α = .89) and traumatic intrusions (α = .83).
The wording of the IDAS was also beta-tested in all the English-speaking sites and no changes in wording were deemed necessary. Translation of the IDAS for the Spanish sites followed the same procedures as for the ACE-IQ.
Statistical Analyses
To test study aims, we first conducted descriptive analyses to examine mean cumulative ACE scores and the percent of students who endorsed each ACE-IQ category, in each country and in the total sample, using both the binary and frequency scoring methods. To examine country differences in mean number of ACEs, we conducted two one-way ANOVAs comparing the means on the binary and frequency total scores across countries (a Bonferroni correction was used to detect specific differences across countries). To examine associations between the ACE-IQ binary and frequency total scores with the seven symptom scales of the IDAS, we conducted both: a) a bivariate correlation model and b) a comprehensive multivariate regression model for each symptom scale. Both models were conducted using Mplus 8.3 (Muthén & Muthén 1998–2018). Within the multivariate regression model, both ACE-IQ binary and frequency total scores were simultaneously estimated as statistical predictors of mental health outcomes (gender, age, and childhood subjective socioeconomic status were included as covariates). We examined the unique direct effects of each predictor variable on mental health outcomes using bias-corrected bootstrapped estimates (Efron & Tibshirani, 1993) based on 10,000 bootstrapped samples, which is robust to small departures from normality (Erceg-Hurn & Mirosevich, 2008). Missing data were handled using full information maximum likelihood (Muthén & Muthén, 1998–2018). Given our large sample size (i.e., large statistical power), statistical significance was determined by 99% confidence intervals that do not contain zero for all analyses.
Results
The mean number of endorsed ACEs and the proportion of participants endorsing each specific ACE in the total sample and in each country are reported in Table 1, for both the binary and the frequency scoring methods.
Overall Exposure to ACEs
Within the total sample, and using the binary scoring method, 94.8% of students reported experiencing at least one ACE (U.S., 93.1%; Canada, 95.6%; South Africa, 98.3%; Spain, 91.1%; Argentina, 99.4%; Uruguay, 98.9%; England, 97.2%) and 61.0% reported experiencing 4 or more ACEs (U.S., 58.7%; Canada, 62.3%; South Africa, 71.8%; Spain, 41.6%; Argentina, 75.8%; Uruguay, 80%; England, 57.4%). Within the total sample, and using the more conservative frequency scoring method, 70.2% of students reported experiencing at least one ACE (U.S., 70.9%; Canada, 67.6%; South Africa, 78.8%; Spain, 52.9%; Argentina, 78.7%; Uruguay, 82.2%; England, 68.0%) and 21.2% reported experiencing four or more ACEs (U.S., 22.9%; Canada, 19.5%; South Africa, 22.7%; Spain, 9.8%; Argentina, 25.6%; Uruguay, 25.6%; England, 18.2%). As reflected in Table 1, the mean number of ACEs on the binary total score (whereby affirmative responses to any level of exposure to an ACE were summed to create a composite score) was above 4 for the full sample and for each individual country, except Spain. Using the higher threshold for ACE exposure (whereby affirmative responses to frequent exposure to an ACE were included in the composite score), the mean number of ACEs for the full sample dropped to 2.0 and was below 2.5 for all seven countries.
In examining country differences in mean ACE score using the binary scoring method, we found statistically significant differences [F(6, 5938) = 33.73, p < .001] such that South African, Argentinian, and Uruguayan students (these students did not differ from each other) reported significantly higher total scores compared to United States, English, and Canadian students (these students did not differ from each other). All student samples reported a significantly higher score than Spanish students. In examining country differences on the frequency total score (whereby frequent exposure to certain ACEs was counted towards the composite score), we found statistically significant differences [F(6, 5938) = 19.94, p < .001] such that Spanish students again reported a significantly lower score than students from all other countries. Further, we found that Argentinian students reported a higher total score than Canadian students (see Table 1 for means).
Rates of Exposure to Specific ACEs
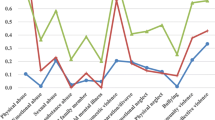
With the binary scoring method for the total sample, the most frequently endorsed ACE category was violence against household members (70.3%), followed by emotional abuse (67.1%). Physical abuse was reported by almost half the sample (47.8%) and sexual abuse by 18.5%. Exposure to violence outside the home was also common, with over half the total sample reporting exposure to community violence (62%) and bullying (56%). The most common family adversity other than familial violence was parental death or separation (32.4%) and the least common was familial incarceration (7.8%). The lowest endorsed category for the full sample was emotional neglect (6.6%).
By contrast, on the frequency scoring method only a minority of the total sample were exposed to violence, abuse, or neglect. For example, rates of physical abuse dropped to 7.4%, physical neglect to 7.5%, emotional abuse to 16.4%, family violence to 28.2%, community violence to 7.5% and bullying to 11.7%. On this scoring algorithm, the most frequently endorsed ACEs in the total sample were parental separation (32.4%), violence against family members (28.2%), and emotional neglect (26.9%; see limitations section), while the lowest endorsed category was physical abuse (7.4%). Comparing rates for specific ACEs across countries on the more conservative frequency scoring algorithm, Uruguay reported the highest rates for seven of the 12 ACEs: physical (9.0%), emotional (20.2%), and sexual abuse (32.6%), violence against family members (36%), familial mental illness (37.1%), parental loss (43%), and bullying (23.6%). Physical neglect (8.8%), familial substance use (17.9%), and familial incarceration (11.3%) were highest in the United States sample. South African students reported the highest rate of emotional neglect (30.8%), while community violence was highest amongst Argentinian students (10.7%). The Spanish sample reported the lowest rate of exposure for every ACE except physical neglect, which was lowest in the Uruguay sample, and sexual abuse, which was lowest in England. Rates of sexual abuse in Uruguay (32.6%) and Argentina (32.8%) were substantially higher than for the other sites.
ACE-IQ Scores and Mental Health
Correlations between ACE-IQ binary and frequency total scores and the seven symptom scales of the IDAS are reported in Table 2. Further, effects from the comprehensive regression model are also reported in Table 2. Higher scores on both the ACE-IQ binary and frequency total score were correlated with more severe symptoms on all seven symptom sub-scales of the IDAS. Within the comprehensive regression model and controlling for the predictive effects of each other and covariates, both binary and frequency total scores were statistically significantly associated with mental health symptoms on all seven sub-scales, except that the binary score was not significantly associated with suicidality.
It is important to note that we tested for structural invariance of the correlational and the regression models across countries (i.e., examining moderation), by conducting χ2 difference tests comparing a freely estimated multi-group model to a constrained multi-group model (i.e., constraining the correlation/regression paths of the model) to determine whether constraining the paths to be equivalent across countries resulted in a worse fitting model. Given that the χ2 test statistic is sensitive to sample size (Brown, 2015), we also relied on model comparison criteria of ΔCFI ≤.01 (Cheung & Rensvold, 2002). Overall, constrained multi-group models indicated model invariance across countries (correlation model: CFI = .996; ΔCFI = .004; regression model: CFI = .999; ΔCFI = .001), indicating associations were similar in strength across countries.
Discussion
ACE exposure rates and the associated risk for mental health difficulties in university populations have only been recently examined and current findings are limited by both measurement variation and a lack of geographic representation. Within the present study, we report on exposure to a comprehensive range of ACEs, and associated mental health difficulties, in a cross-country sample of university students using a single measure. The sample included students from North America, Europe, Africa, and South America. We assessed mean cumulative ACEs, exposure rates for each type of ACE, and associations between cumulative ACEs and mental health, using both scoring methods offered by the ACE-IQ, which effectively reflect two different definitions of ACE exposure.
Cumulative ACE Exposure
According to previous research, an accumulation of four or more different ACEs predicts significantly higher risk of mental health difficulties in adult populations (Hamby et al., 2021; Hughes et al., 2017). On the binary scoring method, which assesses exposure to different adversities independent of frequency, the average total number of ACEs for the full sample was above four (4.32) and 60% of the sample had experienced four or more ACEs. Students in every country except Spain had a mean number of ACE exposures above this threshold and are therefore, on average, in the high-risk range for mental health difficulties.
Further, students from countries with the lowest per capita gross national incomes (GNIs) in the sample (South Africa, Argentina, and Uruguay) had a significantly higher total number of ACEs than those from countries with the highest per capita GNIs (the United States, United Kingdom, and Canada). This is in line with findings that lower socioeconomic position is associated with a greater risk of ACEs (Alhowaymel et al., 2021; Walsh et al., 2019) and punitive parenting (Roubinov & Boyce, 2017), possibly because financial hardship and disadvantaged neighborhood conditions increase parental stress levels (Bywaters et al., 2015; Crouch et al., 2019). Cross-cultural differences in parenting norms and practices, for example more authoritarian versus more authoritative parenting styles, may also contribute to geographical variations in ACEs (Finkelhor et al., 2013; Ho et al., 2019). However, parenting styles within a specific country are not always homogenous (Roman et al., 2016). A nuanced approach is needed to explore cross-cultural differences in ACEs such as child maltreatment or neglect, as parenting practices need to be understood and evaluated within their specific cultural and community context (Raman & Hodes, 2012).
The more conservative ACE-IQ scoring algorithm for ACE exposure requires repeated, rather than single or occasional, exposure to experiences of abuse, neglect, and violence. On this scoring approach the average number of ACEs in the total sample was 2.0. While this is lower than the binary rate, it nevertheless confirms that exposure to multiple forms of ACEs is the norm in this international sample of students. Further, a fifth of the sample reported four or more exposures even on this more conservative measure.
Notably, most of the significant cross-country differences in overall ACE exposure disappeared when the more conservative scoring measure was used. This suggests that cumulative exposure to any adverse childhood events may differ significantly across students in different countries, possibly due to cross-country income differentials, but rates of exposure to repeated, sustained childhood adversity may be more universal. It is possible that in lower-income countries, which have lower levels of education and fewer child-rearing support services, occasional punitive parenting practices (such as shouting or slapping) may be more normative than in higher-income contexts, while more systematic, repeated abuse may be less acceptable across a range of countries, regardless of income level.
On both scoring algorithms, Spanish students reported significantly lower ACE exposure than students in other countries. Previous studies with the Spanish general population (Perales et al., 2013) and Spanish young adults (Gomis-Pomares & Villanueva, 2020) also report lower ACE rates than those reported in samples from other countries (Massetti et al., 2020). These results may suggest the existence of specific protective factors. Spain is a developed country representing the “family welfare regime” (Parra et al., 2019, pp. 3), a model characterized by strong familial bonds that are sustained even during emerging adulthood due to high economic dependence, living with the family, and the pervasiveness of the Catholic tradition. All these features likely shape patterns of parenting and social support which, alongside a relatively strong economy, may reduce the prevalence of ACEs. This family model is also highly prevalent in South America, yet it might be less effective under conditions of chronic financial hardship. It is also possible that more subjective factors, such as culturally based perceptions of childhood experiences or norms for disclosing childhood adversities, account for the lower ACE rates reported by the Spanish sample. Future research should examine the possible protective factors that may be operating in Spain to reduce the occurrence of ACEs; this could yield valuable insights that could be applied to countries with higher ACE rates.
Rates of Exposure to Specific ACEs
Exposure to any instance of childhood violence, abuse and neglect was highly prevalent in our total sample. A series of meta-analyses, based largely on retrospective self-report measures assessing any exposure during childhood, reported global prevalence rates of 22.6% for physical abuse, 12.7%, for sexual abuse, 33.6% for emotional abuse, 16.3% for physical neglect, and 18.4% for emotional neglect (Stoltenborgh et al., 2015). Except for emotional neglect (see limitations section), rates of any exposure to these ACE categories were all substantially higher in our total sample. On the frequency scoring algorithm, only a minority of our total sample was exposed to these adversities repeatedly, but the rates were nevertheless concerning, ranging from 7.4% to 28.2% across the different abuse, violence, and neglect types. In the World Mental Health Surveys (WMHS) with general adult populations in nine countries (Kessler et al., 2010), the proportion of participants reporting repeated physical abuse was comparable with ours, but rates of repeated sexual abuse, neglect, and family violence were substantially lower (emotional abuse, bullying and community violence were not assessed). On both scoring algorithms, then, our international sample of university students had higher exposure rates for many ACEs than would be expected based on previous global prevalence studies. In post-hoc analyses for their meta-analyses, Stoltenborgh and colleagues found that college students reported significantly higher rates of both physical (Stoltenborgh et al., 2013) and emotional abuse (Stoltenborgh et al., 2012) than other populations. While this may suggest a particularly high burden of ACEs in tertiary education settings, it is also possible that university students have fresher recall of childhood experiences than general populations of adults (Kim, 2017) and are also more willing than both older adults and adolescents to disclose ACEs to researchers, particularly if the research topic is linked to courses they are studying, such as Psychology.
Participants in Argentina and Uruguay reported rates of childhood sexual abuse (CSA) that were approximately double those reported in the high-income sites. There is a paucity of previous research on the prevalence of CSA in South American countries against which to compare our findings. In an Argentinian college sample, sexual abuse was reported by 19% of the sample (Bringiotti & Raffo, 2010). This is much lower than the rate in our study, however measurement and sampling differences limit direct comparisons. Our findings may reflect the general association between ACEs and income level, however the rate of CSA in South Africa, also an LMIC, was not as high as in Argentina and Uruguay. Despite the absence of official reports on sexual abuse, the available information indicates that CSA is a highly prevalent, and growing, problem in Argentina (Ministerio de Justicia y Derechos Humanos-UNICEF, 2021; Unidad Fiscal Especializada en Violencia contra las Mujeres, 2019). Therefore, the high rate of CSA found in our study likely reflects a reality for Latin-American children and adolescents. Different reporting norms across cultures may also contribute to the pattern we found; for example, a recent public policy focus on addressing childhood abuse in Argentina may have helped to make ACEs more visible and acknowledged by victims (Prokopez et al., 2020). We recommend that future research should investigate rates of CSA in Argentina and Uruguay more systematically, to examine if the high rates we found are replicated and, if so, to explore the possible reasons for the high prevalence of CSA in these contexts.
It is important to note that, on both the binary and frequency scoring methods, childhood emotional abuse was commonly endorsed. Emotional abuse has often been neglected in child maltreatment studies (Stoltenborgh et al., 2012) and has been excluded from several previous ACE studies with university students. Our findings emphasize the importance of routinely including this form of childhood adversity in ACE research with university students and other populations.
Relationship between ACE Exposure and Mental Health Difficulties
In previous studies with university samples in specific countries, cumulative ACE exposure has consistently predicted mental health difficulties (Burlaka et al., 2020; Karatekin, 2018; Kim, 2017; Watt et al., 2020; Windle et al., 2018), regardless of how ACES are defined or measured. Our study replicates these findings with a more diverse, internationally representative sample: regardless of how frequently specific adversities occurred, cumulative exposure to different types of ACEs in childhood was associated with greater severity of mental health symptoms at the university level. The high rates of mental health difficulties in international samples of university students (Auerbach et al., 2018) may then partly be explained by cumulative ACE exposure, which is the norm rather than the exception for our international sample.
In previous studies with smaller samples of university students in specific countries, both binary (Wang et al., 2019; Zhang et al., 2020) and frequency (Karatekin, 2018) approaches to cumulative ACE exposure have predicted suicidality. Suicidality in our larger, international student sample was predicted only by cumulative ACEs, suggesting that repeated childhood experiences of abuse, neglect and violence are more likely than occasional experiences to create risk for suicidality in young adulthood. Suicide is a leading cause of student death (Turner et al., 2013) and targeting suicide prevention initiatives towards students with histories of repeated childhood adversity may help to reduce suicide risk and overall mortality in this population.
Our cross-sectional study prevents any definitive conclusions about the exact nature of the relationship between cumulative ACE exposure and later mental health difficulties. The pathways and mechanisms of this relationship need further exploration. We recommend that the next stage of research on ACEs among university populations should focus on examining potential moderating factors (to identify which university students who have experienced multiple ACEs are most at risk of different mental health difficulties), mediating factors (to direct prevention and intervention efforts towards addressing key processes whereby past ACE exposures create current mental health difficulties) and the specific patterning of adversities that increases risk for specific mental health disorders (Lacey et al., 2020). This more fine-grained approach will better equip universities to identify and support those ACE-exposed students who may be most at risk of mental health difficulties.
Limitations
Strengths of our study include the use of a large international sample, a standardized measure including a broad range of ACEs, and the inclusion of both a binary and a frequency approach to assessing ACEs. These address many of the common conceptual and methodological limitations of ACE research (Lacey & Minnis, 2020). Our findings using the two ACE-IQ scoring methods confirm that different definitions and thresholds for ACEs can yield quite different pictures of overall exposure. While there is ongoing debate about which ACE assessment methods are optimal (Lacey & Minnis, 2020), it at least seems clear that binary and frequency/severity measures should not be directly compared with one another when considering ACE exposure rates and that definitions of ACE exposure (any experience versus repeated experiences) should always be stated explicitly by researchers. Our study has also been able to show that ACE exposure carries risk for mental health outcomes amongst university students regardless of the frequency of exposure. Previous studies with university populations have not compared the mental health risks associated with any versus frequent ACE exposure.
Our study also has some limitations. First, the ACE-IQ relies on retrospective self-report data, which is subject to inaccurate recall and reporting bias (Hughes et al., 2017; Naicker et al., 2017). However, retrospective assessments of major and more easily defined childhood adversities have been shown to have acceptable psychometric properties (Hardt & Rutter, 2004). Second, the somewhat ambiguous wording of the scoring instructions for emotional neglect on the ACE-IQ resulted in a higher exposure rate for this ACE on the more conservative frequency algorithm compared with the less conservative binary algorithm. It is likely that inverse rates in fact apply. In the absence of further scoring clarification from the WHO, the rates of emotional neglect reported here should be treated with caution. Third, utilization of various sampling methods (e.g., e-mail listings, online invitations via social networks, pools of students) across countries may have impacted differences across countries in our results. Moreover, the use of volunteer student samples is subject to selection bias. For example, either more psychologically vulnerable students or psychologically healthy students may elect to participate in online surveys. Further, most countries sampled from one university and results may not replicate among students from differing regions within each country. This may particularly be the case for the Uruguay sample, which was smaller than the other samples, and results regarding this sub-sample (for example, comparisons of exposure rates to other countries in the study) should be treated with more caution. In addition, our total sample, and the sample from each country, skewed towards females. Several of our study sites recruited from Psychology courses, which traditionally have an over-representation of female students (Sander & de la Fuente, 2020), and this may have skewed the study results. Finally, we assessed self-reported mental health difficulties rather than the presence of clinically significant, diagnosed mental disorders. However, the IDAS scales are good predictors of the presence of clinical diagnoses (Stasik-O’Brien et al., 2019).
Conclusion
The majority of students in our international sample have experienced multiple forms of childhood adversity and, even on the most conservative measure, a fifth have experienced four or more. Further, cumulative exposure to any and to repeated forms of childhood adversity both predicted worse mental health at university level. These findings indicate that university students across countries carry a long-standing psychological burden of childhood adversity. Greater investment in policies and programmes to reduce child maltreatment and other severe family adversities could yield a long-term developmental benefit by reducing risk for mental health difficulties in emerging adulthood. Our findings further highlight the urgent need for the development of trauma-informed university campuses, in parallel with the growing movement for trauma-informed schools (Overstreet & Chafouleas, 2016). All university stakeholders (including students, faculty, residence staff, management, and campus health service providers) should be educated about, and sensitive to, the high rates of exposure to childhood adversity in student populations and the long-term impact of this on student mental health and functioning (SAMHSA, 2014). Finally, future research should aim to identify which ACE-exposed students have the highest risk for negative mental health outcomes, and which factors may ameliorate this risk, to better support students through their university years.
Data Availability
Data and analytic outputs are available at DOI https://doi.org/10.17605/OSF.IO/UX8RK
Code Availability
Not applicable.
References
Alhowaymel, F. K., Kalamakis, K., & Jacelon, C. (2021). Developing the concept of adverse childhood experiences: A global perspective. Journal of Pediatric Nursing, 56, 18–23. https://doi.org/10.1016/j.pedn.2020.10.004
Auerbach, R. P., Mortier, P., Bruffaerts, R., Alonso, J., Benjet, C., Cuijpers, P., Demyttenaere, K., Ebert, D. D., Green, J. G., Hasking, P., Murray, E., Nock, M. K., Pinder-Amaker, S., Sampson, N. A., Stein, D. J., Vilagut, G., Zaslavsky, A. M., Kessler, R. C.; WHO WMH-ICS Collaborators. (2018). WHO world mental health surveys international college student project: Prevalence and distribution of mental disorders. Journal of Abnormal Psychology, 127(7), 623–638. https://doi.org/10.1037/abn0000362.
Bravo, A. J., Prince, M. A., Pilatti, A., Mezquita, L., Keough, M. T., Hogarth, L., & Cross-Cultural Addictions Study Team. (2021). Young adult concurrent use and simultaneous use of alcohol and marijuana: A cross-national examination among college students in seven countries. Addictive Behaviors Reports, 14, 100373. https://doi.org/10.1016/j.abrep.2021.100373
Bravo, A. J., Villarosa-Hurlocker, M. C., Pearson, M. R., & Protective Strategies Study Team. (2018). College student mental health: An evaluation of the DSM–5 self-rated level 1 cross-cutting symptom measure. Psychological Assessment, 30(10), 1382–1389. https://doi.org/10.1037/pas0000628
Bringiotti, M. I., & Raffo, P. E. (2010). Abuso sexual infanto-juvenil. Prevalencia y caracteristicas de estudiantes Universitarios de la Ciudad de Buenos Aires. Revista de Derecho de Familia, 46, 293–305.
Brown, T. A. (2015). Confirmatory factor analysis for applied research (2nd ed.). Guilford Press.
Burlaka, V., Hong, J. S., Churakova, I., Surdiak, O., Proskura, V., & Shvets, D. (2020). The role of adverse childhood experiences and corporal punishment in early adulthood depression and substance use among Ukrainian college students. Journal of Family Violence, 35, 285–295. https://doi.org/10.1007/s10896-019-00110-x
Bywaters P., Bunting, L., Davidson, G., Hanratty, J., Mason, W., McCartan, C., & Steils, N. et al. (2015). The relationship between poverty, child abuse and neglect: An evidence review. : Joseph Rowntree Foundation. https://www.jrf.org.uk/report/relationship-between-poverty-child-abuse-and-neglect-evidence-review23EffectivePublic.
Cheung, G. W., & Rensvold, R. B. (2002). Evaluating goodness-of-fit indexes for testing measurement invariance. Structural Equation Modeling, 9(2), 233–255. https://doi.org/10.1207/S15328007SEM0902_5
Crouch, E., Radcliff, E., Brown, M., & Hung, P. (2019). Exploring the association between parenting stress and a child’s exposure to adverse childhood experiences (ACEs). Child and Youth Services Review, 102, 186–192. https://doi.org/10.1016/j.childyouth.2019.05.019
Danese, A., & McEwen, B. S. (2012). Adverse childhood experiences, allostasis, allostatic load and age-related disease. Physiology & Behavior, 106, 29–39. https://doi.org/10.1016/j.physbeh.2011.08.019
Efron, B., & Tibshirani, R. J. (1993). An introduction to the bootstrap (Vol. 57). Chapman & Hall/CRC.
Erceg-Hurn, D. M., & Mirosevich, V. M. (2008). Modern robust statistical methods: An easy way to maximize the accuracy and power of your research. American Psychologist, 63(7), 591–601. https://doi.org/10.1037/0003-066X.63.7.591
Felitti, V. J., Anda, R. F., Nordenberg, D., Williamson, D. F., Spitz, A. M., Edwards, V., & Marks, J. S. (1998). Relationship of child abuse and household dysfunction to many of the leading causes of death in adults: The adverse childhood experiences (ACE) study. American Journal of Preventive Medicine, 14(4), 245–258. https://doi.org/10.1016/s0749-3797(98)00017-8
Finkelhor, D., Ji, K., Mikton, C., & Dunne, M. (2013). Explaining lower rates of sexual abuse in China. Child Abuse and Neglect, 37(10), 852–860. https://doi.org/10.1016/j.chiabu.2013.07.006
Fontes, L. A., & Plummer, C. (2010). Cultural issues in disclosures of child sexual abuse. Journal of Child Sexual Abuse, 19(5), 491–518. https://doi.org/10.1080/10538712.2010.512520
Forster, M., Grigsby, T. J., Rogers, C. J., & Benjamin, S. M. (2018). The relationship between family-based adverse childhood experiences and substance use behaviors among a diverse sample of college students. Addictive Behaviors, 76, 298–304. https://doi.org/10.1016/j.addbeh.2017.08.037
Gomis-Pomares, A., & Villanueva, L. (2020). The effect of adverse childhood experiences on deviant and altruistic behavior during emerging adulthood. Psicothema, 32(1), 33–39. https://doi.org/10.7334/psicothema2019.142
Graham, J. W., Taylor, B. J., Olchowski, A. E., & Cumsille, P. E. (2006). Planned missing data designs in psychological research. Psychological Methods, 11(4), 323–343. https://doi.org/10.1037/1082-989X.11.4.323
Grassi-Oliveira, R., Ashy, M., & Stein, L. M. (2008). Psychobiology of childhood maltreatment: Effects of allostatic load. Brazilian Journal of Psychiatry, 30(1), 60–68. https://doi.org/10.1590/S1516-44462008000100012
Hamby, S., Elm, J. H. L., Howell, K. H., & Merrick, M. T. (2021). Recognizing the cumulative burden of childhood adversities transforms science and practice for trauma and resilience. American Psychologist, 76(2), 230–242. https://doi.org/10.1037/amp0000763
Hardt, J., & Rutter, M. (2004). Validity of adult retrospective reports of adverse childhood experiences: Review of the evidence. Journal of Child Psychology and Psychiatry, 45(2), 260–273. https://doi.org/10.1111/j.1469-7610.2004.00218.x
Ho, G. W. K., Chan, A. C. Y., Chien, W.-T., Bressington, D. T., & Karatzias, T. (2019). Examining patterns of adversity in Chinese young adults using the adverse childhood experiences—International questionnaire (ACE-IQ). Child Abuse & Neglect, 88, 179–188. https://doi.org/10.1016/j.chiabu.2018.11.009
Hughes, K., Bellis, M. A., Hardcastle, K. A., Sethi, D., Butchart, A., Mikton, C., Jones, L., & Dunne, M. P. (2017). The effect of multiple adverse childhood experiences on health: A systematic review and meta-analysis. The Lancet Public Health, 2(8), e356–e366. https://doi.org/10.1016/S2468-2667(17)30118-4
Ji, S., & Wang, H. (2018). A study of the relationship between adverse childhood experiences, life events, and executive function among college students in China. Psychology: Research & Review, 31, 28. https://doi.org/10.1186/s41155-018-0107-y
Kalmakis, K. A., & Chandler, G. E. (2014). Adverse childhood experiences: Towards a clear conceptual meaning. Journal of Advanced Nursing, 70(7), 1489–1501. https://doi.org/10.1111/jan.12329
Karatekin, C. (2018). Adverse childhood experiences (ACEs), stress and mental health in college students. Stress and Health, 34(1), 36–45. https://doi.org/10.1007/s00213-010-2009-2
Kelifa, M. O., Yang, Y., Carly, H., Bo, W., & Wang, P. (2021). How adverse childhood experiences relate to subjective wellbeing in college students: The role of resilience and depression. Journal of Happiness Studies, 22, 2103–2123. https://doi.org/10.1007/s10902-020-00308-7
Kessler, R., et al. (2010). Childhood adversities and adult psychopathology in the WHO world mental health surveys. The British Journal of Psychiatry, 197(5), 378–385. https://doi.org/10.1192/bjp.bp.110.080499
Khrapatina, I., & Berman, P. S. (2017). The impact of adverse childhood experiences on health in college students. Journal of Child and Adolescent Trauma, 10(3), 275–287. https://doi.org/10.1007/s40653-016-0093-0
Kidman, R., Smith, D., Piccolo, L. R., & Kohler, H. P. (2019). Psychometric evaluation of the adverse childhood experience international questionnaire (ACE-IQ) in Malawian adolescents. Child Abuse & Neglect, 92, 139–145. https://doi.org/10.1016/j.chiabu.2019.03.015
Kim, P., Evans, G. W., Angstadt, M., Shaun Ho, S., Sripada, C. S., Swain, J. E., Liberzon, I., & Luan Phan, K. (2013). Childhood poverty, chronic stress, and adult brain. Proceedings of the National Academy of Sciences Nov 2013, 110(46), 18442–18447. https://doi.org/10.1073/pnas.1308240110
Kim, Y. H. (2017). Associations of adverse childhood experiences with depression and alcohol abuse among Korean college students. Child Abuse & Neglect, 67, 338–348. https://doi.org/10.1016/j.chiabu.2017.03.009
Lacey, R., Howe, L., Kelly-Irving, M., Bartley, M., & Kelly, Y. (2020). The clustering of adverse childhood experiences in the Avon longitudinal study of parents and children: Are gender and poverty important? Journal of Interpersonal Violence, 37, 2218–2241. https://doi.org/10.1177/0886260520935096
Lacey, R. E., & Minnis, H. (2020). Practitioner review: Twenty years of research with adverse childhood experience scores - advantages, disadvantages and applications to practice. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 61(2), 116–130. https://doi.org/10.1111/jcpp.13135
Mall, S., Mortier, P., Taljaard, L., Roos, J., Stein, D. J., & Lochner, C. (2018). The relationship between childhood adversity, recent stressors, and depression in college students attending a south African university. BMC Psychiatry, 18, 63. https://doi.org/10.1186/s12888-017-1583-9
Martin-Denham, S. L., & Donaghue, J. J. (2020). The impact and measure of adverse childhood experiences: Reflections of undergraduates and graduates in England. Journal of Public Health, 30, 1023–1032. https://doi.org/10.1007/s10389-020-01359-z
Massetti, G. M., Hughes, K., Bellis, M. A., & Mercy, J. (2020). Global perspective on ACEs. In G. J. G. Asmundson & T. O. Afifi (Eds.), Adverse childhood experiences: Using evidence to advance research, practice, policy, and prevention (pp. 209–231). Elsevier Academic Press. https://doi.org/10.1016/B978-0-12-816065-7.00011-2
McGavock, L., & Spratt, T. (2014). Prevalence of adverse childhood experiences in a university population: Associations with use of social services. The British Journal of Social Work, 44(3), 657–674. https://doi.org/10.1093/bjsw/bcs127
Merians, A. N., Baker, M. R., Frazier, P., & Lust, K. (2019). Outcomes related to adverse childhood experiences in college students: Comparing latent class analysis and cumulative risk. Child Abuse & Neglect, 87, 51–64. https://doi.org/10.1016/j.chiabu.2018.07.020
Ministerio de Justicia y Derechos Humanos-UNICEF (2021). Un análisis de los datos del programa Las Víctimas contra las Violencias 2020-2021 (No. 9. Serie Violencia contra niñas, niños y adolescentes). https://www.unicef.org/argentina/informes/serie-violencia-contra-ninas-ninos-y-adolescentes
Muthén, L.K., Muthén, B.O., (1998–2020). Mplus User’s Guide. Seventh Edition. Los Angeles, CA: Muthén & Muthén.
Naicker, S. N., Norris, S. A., Mabaso, M., & Richter, L. M. (2017). An analysis of retrospective and repeat prospective reports of adverse childhood experiences from the south African birth to twenty plus cohort. PLoS One, 12(7), e0181522. https://doi.org/10.1371/journal.pone.0181522
Overstreet, S., & Chafouleas, S. M. (2016). Trauma-informed schools: Introduction to the special issue. School Mental Health, 8(1), 1–6. https://doi.org/10.1007/s12310-016-9184-1
Parra, Á., Sánchez-Queija, I., García-Mendoza, M., Coimbra, S., Egídio Oliveira, J., & Díez, M. (2019). Perceived parenting styles and adjustment during emerging adulthood: A cross-national perspective. International Journal of Environmental Research and Public Health, 16(15), 2757. https://doi.org/10.3390/ijerph16152757
Pechtel, P., & Pizzagalli, D. A. (2011). Effects of early life stress on cognitive and affective function: An integrated review of human literature. Psychopharmacology, 214(1), 55–70. https://doi.org/10.1007/s00213-010-2009-2
Perales, J., Olaya, B., Fernandez, A., Alonso, J., Vilagut, G., Forero, C. G., et al. (2013). Association of childhood adversities with the first onset of mental disorders in Spain: Results from the ESEMeD project. Social Psychiatry and Psychiatric Epidemiology, 48(3), 371–384. https://doi.org/10.1007/s00127-012-0550-5
Prokopez, C. R., Vallejos, M., Farinola, R., Alberio, G., Caporusso, G. B., Cozzarin, L. G., Chiapella, L. C., Fuentes, P., & Daray, F. M. (2020). The history of multiple adverse childhood experiences in patients with schizophrenia is associated with more severe symptomatology and suicidal behavior with gender-specific characteristics. Psychiatry Research, 293, 113411. https://doi.org/10.1016/j.psychres.2020.113411
Raman, S., & Hodes, D. (2012). Cultural issues in child maltreatment. Journal of Paediatric Child Health, 48(1), 30–37. https://doi.org/10.1111/j.1440-1754.2011.02184.x
Roman, N. V., Makwakwa, T., & Marlies Lacante, M. (2016). Perceptions of parenting styles in South Africa: The effects of gender and ethnicity. Cogent Psychology, 3(1), 1153231. https://doi.org/10.1080/23311908.2016.1153231
Roubinov, D. S., & Boyce, W. T. (2017). Parenting and SES: Relative values or enduring principles? Current Opinion in Psychology, 15, 162–167. https://doi.org/10.1016/j.copsyc.2017.03.001
Sander, P., & de la Fuente, J. (2020). Undergraduate student gender, personality and academic confidence. International Journal of Environmental Research and Public Health, 17(15), 5567. https://doi.org/10.3390/ijerph17155567
Schafer, J. L. (1997). Analysis of incomplete multivariate data. Chapman Hall.
Solberg, M. A., & Peters, R. M. (2020). Adverse childhood experiences in non-westernized nations: Implications for immigrant and refugee health. Journal of Immigrant and Minority Health, 22(1), 145–155. https://doi.org/10.1007/s10903-019-00953-y
Stasik-O’Brien, S. M., Brock, R. L., Chmielewski, M., Naragon-Gainey, K., Koffel, E., McDade-Montez, E., O'Hara, M. W., & Watson, D. (2019). Clinical utility of the inventory of depression and anxiety symptoms (IDAS). Assessment, 26(5), 944–960. https://doi.org/10.1177/1073191118790036
Stoltenborgh, M., Bakermans-Kranenburg, M. J., Alink, L. R. A., & van IJzendoorn, M. H. (2012). The universality of childhood emotional abuse: A meta-analysis of worldwide prevalence. Journal of Aggression, Maltreatment & Trauma, 21(8), 870–890. https://doi.org/10.1080/10926771.2012.708014
Stoltenborgh, M., Bakermans-Kranenburg, M. J., Alink, L. R. A., & van IJzendoorn, M. H. (2015). The prevalence of child maltreatment across the globe: Review of a series of meta-analyses. Child Abuse Review, 24, 37–50. https://doi.org/10.1002/car.2353
Stoltenborgh, M., Bakermans-Kranenburg, M. J., van Ijzendoorn, M. H., & Alink, L. R. (2013). Cultural-geographical differences in the occurrence of child physical abuse? A meta-analysis of global prevalence. International Journal of Psychology, 48(2), 81–94. https://doi.org/10.1080/00207594.2012.697165
Substance Abuse and Mental Health Services Administration (2014). SAMHSA's concept of trauma and guidance for a trauma-informed approach. https://store.samhsa.gov/sites/default/files/d7/priv/sma14-4884.pdf
Turner, J. C., Leno, E. V., & Keller, A. (2013). Causes of mortality among American college students: A pilot study. Journal of College Student Psychotherapy, 27(1), 31–42. https://doi.org/10.1080/87568225.2013.739022
Unidad Fiscal Especializada en Violencia contra las Mujeres (2019). Relevamiento de fuentes secundarias de datos sobre violencia sexual a nivel país y en la Ciudad Autónoma de Buenos Aires. Ministerio Público Fiscal. https://www.mpf.gob.ar/ufem/files/2019/10/Informe_UFEM.pdf
Walsh, D., McCartney, G., Smith, M., & Armour, G. (2019). Relationship between childhood socioeconomic position and adverse childhood experiences (ACEs): A systematic review. Journal of Epidemiology & Community Health, 73, 1087–1093. https://doi.org/10.1136/jech-2019-212738
Wang, Y.-R., Sun, J., Lin, P.-Z., Zhang, H.-H., Mu, G.-X., & Cao, F.-L. (2019). Suicidality among young adults: Unique and cumulative roles of 14 different adverse childhood experiences. Child Abuse & Neglect, 98, 104183. https://doi.org/10.1016/j.chiabu.2019.104183
Watson, D., O'Hara, M. W., Simms, L. J., Kotov, R., Chmielewski, M., McDade-Montez, E. A., Gamez, W., & Stuart, S. (2007). Development and validation of the inventory of depression and anxiety symptoms (IDAS). Psychological Assessment, 19(3), 253–268. https://doi.org/10.1037/1040-3590.19.3.253
Watt, T., Ceballos, N., Kim, S., Pan, X., & Sharma, S. (2020). The unique nature of depression and anxiety among college students with adverse childhood experiences. Journal of Child and Adolescent Trauma, 13(2), 163–172. https://doi.org/10.1007/s40653-019-00270-4
Wiehn, J., Hornberg, C., & Fischer, F. (2018). How adverse childhood experiences relate to single and multiple health risk behaviours in German public university students: A cross-sectional analysis. BMC Public Health, 18, 1005. https://doi.org/10.1186/s12889-018-5926-3
Windle, M., Haardörfer, R., Getachew, B., Shah, J., Payne, J., Pillai, D., & Berg, C. J. (2018). A multivariate analysis of adverse childhood experiences and health behaviors and outcomes among college students. Journal of American College Health, 66(4), 246–251. https://doi.org/10.1080/07448481.2018.1431892
World Health Organization (2020). Adverse Childhood Experiences International Questionnaire (ACE-IQ). https://www.who.int/publications/m/item/adverse-childhood-experiences-international-questionnaire-(ace-iq)
Zhang, J., Tang, B. W., Liu, M. W., Yuan, S., Yu, H. J., Zhang, R., Huang, X. C., Nzala, S. H., Chikoya, M., Wang, P. G., & He, Q. Q. (2020). Association of adverse childhood experiences with health risk behaviors among college students in Zambia. International Journal of Behavioral Medicine, 27(4), 400–405. https://doi.org/10.1007/s12529-020-09863-y
Acknowledgements
This project was completed by the Cross-cultural Addictions Study Team (CAST), which includes the following investigators (in alphabetical order): Adrian J. Bravo, William & Mary (Coordinating PI); Christopher C. Conway, Fordham University; James M. Henson, Old Dominion University; Lee Hogarth, University of Exeter; Manuel I. Ibáñez, Universitat Jaume I de Castelló; Debra Kaminer, University of Cape Town; Matthew Keough, York University; Laura Mezquita, Universitat Jaume I de Castelló; Generós Ortet, Universitat Jaume I de Castelló; Matthew R. Pearson, University of New Mexico; Angelina Pilatti, National University of Cordoba; Mark A. Prince, Colorado State University; Jennifer P. Read, University of Buffalo; Hendrik G. Roozen, University of New Mexico; Paul Ruiz, Universidad de la República.
Funding
Dr. Bravo was supported by a training grant (j) from the National Institute on Alcohol Abuse and Alcoholism (NIAAA) in the United States during the duration of data collection for this project. Data collection was supported, in part, by grant T32-AA018108. NIAAA had no role in the study design, collection, analysis or interpretation of the data, writing the manuscript, or the decision to submit the paper for publication. Data collection in Spain was also supported by grant UJI-A2019–08 from the Universitat Jaume and RTI2018–099800-B-I00 from the Spanish Ministry of Science, Innovation and Universities (MCIU). Data collection in Argentina was also supported by grants from the National Secretary of Science and Technology (FONCYT, grant number PICT 2018-3170) and by grants from the Secretary of Science and Technology- National University of Córdoba (SECyT-UNC).
Author information
Authors and Affiliations
Consortia
Contributions
All authors contributed to the study conception and design. Data analysis was performed by Adrian Bravo. The first draft of the manuscript was written by Debra Kaminer and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics Approval
Institutional ethical approval for data collection was sought and formally granted at each site.
Consent to Participate
All participants provided informed consent to participate.
Conflict of Interest
The authors declare no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Kaminer, D., Bravo, A.J., Mezquita, L. et al. Adverse childhood experiences and adulthood mental health: a cross-cultural examination among university students in seven countries. Curr Psychol 42, 18370–18381 (2023). https://doi.org/10.1007/s12144-022-02978-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12144-022-02978-3