
Abstract
Altought compassionate care is an important factor in health care, remains an unmet need in patients. The studies have been carried out in Anglo-Saxon countries with cultural environments and health systems that are very different from Spanish-speaking contexts. The aim of this study to understand the conceptual, evaluation and clinical application nuances of compassion and compassionate care in Spanish-speaking health care settings, through a systematic review. A search of the scientific literature was carried out following the PRISMA guidelines in ProQuest Central, PubMed and Web Of Science, resulting in 295 studies, of which 27 were selected, based on the following inclusion criteria: the article studied or analyzed the construct of compassion in healthcare setting and the participants were Spanish speakers or the authors spoke of the construct in Spanish. Two blinded evaluators performed the study selection process using the Covidence tool. The agreement between evaluators was in all cases satisfactory. Different definitions of the construct have been identified, that they generally share: the recognition of suffering and the attempt to alleviate it. There are few studies that focus solely on the analysis of compassion, since other concepts appear that are associated with it, such as empathy and self-compassion. Further research is needed to obtain a better and greater understanding of compassionate care adapted to the perceptions of patients and health professionals in different socio-cultural contexts. In this way, instruments that measure compassionate care can be better developed and adjusted, and interventions aimed at promoting compassion can be properly assessed.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Compassion is defined as a deep awareness of the suffering of others along with the desire to alleviate it (Nunberg & Newman, 2011) and is considered a fundamental component of quality health care (Ques, 2019). The conceptualization of this construct is complex since many definitions have been provided, most of which are theoretical, without specificity or clinical applicability and with little conceptual validity (Sinclair et al., 2016a). In current studies, it has been defined as: “a virtuous response that seeks to address the suffering and needs of a person through relational understanding and action.” (Sinclair et al., 2016a).
Furthermore, compassion is often confused with other terms such as empathy and sympathy, with which it is closely related. In fact, in many cases, they are used interchangeably as synonyms (Klimecki, Leiberg, Ricard & Singer, 2014; Preckel et al., 2018). However, compassion enhances the key facets of empathy while adding distinct features of being motivated by love, the altruistic role of the responder, action, and small, supererogatory acts of kindness (Sinclair, Beamer et al., 2016a).
Although compassion has a prominent place in the codes of ethics of professional organizations, and most health care facilities are willing to provide compassionate care, some studies have identified compassion as one of the most important unmet needs of patients (Riggs et al., 2014). This is especially relevant because lack of compassionate care increases adverse medical problems, symptom-control related discomfort, patient complaints, and negligence complaints to the health care system (Sinclair et al., 2017a). In the same vein, health care that includes compassion provides important benefits such as improved physician-patient relationships, increased patient satisfaction, and improved patient symptomatology and quality of life, in addition to aiding recovery (Seppala et al., 2014; Sinclair et al., 2016a).
This significant impact of compassionate care has led good practice policy makers, researchers, and educators in this field worldwide to view compassionate care as a patient’s right (Paterson, 2011), a fundamental professional competence (Callwood, Cooke, & Allan, 2014). Therefore there are theoretical works that attempt to conceptualize this construct (Chachula, 2020; Sinclair et al., 2016a, b, c, 2017a, b; Taylor et al., 2017); as well as qualitative studies that analyze the importance, experience and presence of compassion in the health field from different perspectives (Sinclair et al., 2016a, 2016b, 2016c, 2018), psychotherapeutic interventions based in compassion (Dodds et al., 2015) and reviews of instruments for evaluating compassionate care in clinical settings (Sinclair et al., 2017b).
The scientific evidence discussed above on this line of research, however, comes mostly from Anglo-Saxon countries with cultural backgrounds and health systems different from the Spanish-speaking context. There are differences between the different healthcare systems, for example, in the USA it is a private system while in the Spanish context it is a public system. One of the most characteristic features of the Spanish healthcare system is that it is a decentralized system, with a territorial organization for each Autonomous Community. The Spanish National Health System is somewhat in line with the original British Atlantic model, as opposed to the U.S. model (García-Altés et al., 2019). Firstly, in the Spanish system there is universalization of health services, always on an equal basis, regardless of social and personal circumstances. This means that public health coverage is extended to the entire population (an aspect that does not coincide with the American system). Solidarity is also a characteristic aspect of our healthcare system, i.e., citizens’ contributions are calculated according to their income. In addition, access to health care depends on the degree of need of each patient, something that in America depends on the socioeconomic level and health insurance (Sultana et al., 2020). Another aspect related to the latter is the equity of the system in terms of access to health benefits. Another of the most significant features of the system is its financing. In addition to providing healthcare, the Spanish system tries to provide what could be called “preventive healthcare”, through instruments such as disease prevention policies and health promotion policies, medical benefits, and pharmaceutical benefits (Sultana et al., 2020).
There are few studies that have addressed the term compassion in the Spanish-speaking healthcare context. Taking into account the differences in the health care systems, our research attempts to respond to this gap in the literature, to help health professionals to understand the application and evaluation of compassion among health professionals. Therefore, the objective of the present study is to understand the conceptual nuances, evaluation and clinical application of compassion and compassionate care in the Spanish-speaking healthcare setting, through a systematic review.
Methods
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) standard (Moher et al., 2015). The protocol for the systematic review was registered in PROSPERO (Booth et al., 2012) (CRD42020177268).
The ProQuest Central, PubMed and Web Of Science databases were consulted for relevant records published up to 12 March 2020. PICO approach was used to formulate the following research question (Sackett et al., 1996): What concept the Spanish-speaking population has of the construct of compassion in healthcare?
In the final search, two key words were combined using the following Boolean expression: (compass* AND Spanish) along with the most appropriate field labels in each database. Thus, in ProQuest we searched as follows: noft(compass*) AND noft(English)”, in Web Of Science: TS = (compass* AND English) and in Pubmed: (compass*[Text Word]) AND (English [Text Word]). No time limit was applied but the following additional parameters were marked in all databases: full text, language in Spanish or English, article, literature review or review in scientific journals in full text.
All retrieved articles were uploaded to Covidence Systematic Review Software (2018) an online data mining and screening tool. After elimination of duplicates, two people independently reviewed the titles and abstracts of all papers, excluding those articles that did not meet the inclusion criteria. The full text of the selected articles was then reviewed individually and blinded to judge their eligibility according to the inclusion and exclusion criteria. The reference lists of the selected studies were also inspected to assess the inclusion of quality references that had not appeared in the initial searches. Hand searching followed a snowball sampling to identify relevant articles in the reference lists of potentially useful documentation. Disagreements between the two were resolved by discussion.
Subsequently, Cohen’s Kappa (κ) was calculated (Orwin, 1994) with the objective of evaluating the index of interjudge agreement, considering that values between −1 and 0.40 are understood as unsatisfactory, values between 0.41 and 0.75 as satisfactory and ≥ of 0.76, very satisfactory (Hernández-Nieto, 2002).
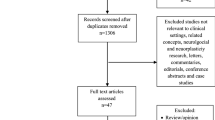
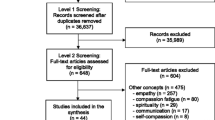
Figure 1 shows the flow chart of the information used to answer the review question.

Flowchart of selection proc
Studies meeting the following criteria were included in this systematic review: (a) the article studied or analyzed the construct of compassion (definition, conceptualization or application of the construct), (b) the participants were Spanish speakers or the authors spoke of the construct in Spanish, (c) the studies focused on the health field, (d) it was published in English or Spanish (e) and its full text was accessible through the University of Valencia databases. As criteria for exclusion were used: (a) the study could not refer only to concepts or terms related to compassion such as self-pity, compassion fatigue or compassion satisfaction, (b) studies that focused on the compassionate use of medicines or medical programs, and (c) papers published in congresses.
A data extraction form was developed and used to obtain relevant information from the included studies. This information is collected in Table 1 and includes: first author, and year of publication, country, sample, variables and instruments, study design, definition of compassion, results, and main conclusions.
Results
Study Selection and Screening
The selection process of the study is shown in Fig. 1. The literature search produced a total of 292 articles. Once the duplicate records were eliminated, the total number of studies was 235. The initial selection excluded 119 papers based on the title and the abstract, and the remaining 116 were read in full text in a second selection process. The reliability of the previous agreement between the two independent raters of the full text screening was satisfactory (κ = 0.53). In the second screening, 91 papers were excluded, making 28 studies eligible for inclusion. In this second screening, the degree of inter-judge agreement was excellent (κ = 0.88).
Characteristics of the Study
The characteristics of the study are summarized in Table 1. Of the articles included in this review, 57% are empirical studies, 14% are validations of psychometric instruments and 29% are theoretical works. Fifty-four percent of the studies originated in Spain, followed by 14% in the United States, 7% in Colombia, 7% in Argentina, and the rest in Chile, Mexico, the Dominican Republic, Peru, and France. Most of the papers were published between 2015 and 2019 (n = 24).
Conceptualization of Compassion
As for the conceptualization of compassion, 61% of the selected studies provided a definition. It has been defined in various ways, for example as a construct, a feeling, a performance, an emotion or a capacity, but the majority (71%) mention the recognition of suffering and the attempt or desire to alleviate it.
There are studies that use various approaches to conceptualize compassion. Two studies explain compassion from different cultural traditions. In them, it is emphasized that from the western tradition it has been proposed that compassion is a complex construction that involves cognitive, affective and behavioral characteristics to alleviate the suffering of others and oneself. From this perspective, compassion is associated to resonate with and accompany shared suffering. While in Eastern theories, unlike this, compassion is understood as a basic quality of human beings rooted in the recognition of suffering and adds the active component of alleviating it, which results in pro-social behaviors in order to generate well-being to the person who suffers.
In this line, one of the studies mentions an operational definition considering the different Buddhist and Western perspectives. Strauss et al. (2016) defined compassion as a cognitive, affective and behavioral process that involves identifying suffering, understanding its universality, feeling emotionally connected or empathic with the experience of the other, tolerating uncomfortable feelings in response to suffering and being motivated to alleviate it/act. This definition is consistent with the description given by studies of the elements that make up compassion (Flores et al., 2018; Klos & Lemos, 2018; Sacristán-Martin et al., 2019; Valentín et al., 2019).
Likewise, other approaches appear to explain compassion such as the evolutionary perspective (which understands that compassion is rooted in our biology), the theory of moral emotions (which defines compassion as an emotion experienced when observing the destruction of a moral value or social standard and encourages us to restore that neglect) or the theoretical model of empathy-altruism (which contemplates the cognitive-affective component (empathy) and the altruistic act to lessen the discomfort of the other).
The rest of the articles included in our study did not contain an exact definition of compassion but conceptualized it from the description of the characteristics or concepts that were related to it.
Applying Compassion in Health Care
Since the present review includes heterogeneous works, it has been thought convenient to present the results distributing them according to the type of study:
Theoretical Studies
The selected theoretical studies that focus on the conceptualization of compassion in the health field in a Spanish-speaking context present very different objectives. Three papers have been identified that focus on compassion during much of the article. Two studies have also been found that focus on the application of compassionate care. The other study explains a project to develop compassionate communities to provide comprehensive care for the needs of individuals in palliative care.
In the remaining three papers, one briefly mentions compassion, as it focuses on describing the characteristics and scope in the therapeutic area of self-compassion. While the other studies are dedicated to analyzing the importance of empathy in the field of psychotherapy and the phenomena that can influence it in a negative way. But they also explain the relationship between mindfulness, empathy and compassion, offering an explanatory model of the association of these constructs and showing the advantages of applying mindfulness and compassion-based interventions (MCI) in the university training of clinical psychologists.
Empirical Studies
The 16 empirical studies included analyzed, as a whole, a total of 2144 medical students, 452 health professionals, 174 patients with pathologies (fibromyalgia, eating disorders, borderline personality disorder, depression, anxiety and adjustment disorders) and 2856 people representative of the general population.
As for the research design, 25% were qualitative studies, 31% were randomized clinical trials, 31% were cross-sectional studies and the rest of the works (12%) were pilot studies.
In relation to the evaluated variables, a great heterogeneity has been obtained as for the independent and dependent variables. The studies considered different outcome variables at the psychological level among which the following stand out: full attention (38%), self-pity (44%), compassionate care/compassion (38%) and empathy (6%). With regard to the compassion variable, in 80% of the works, it was evaluated with generally adapted to the population, with the exception of two of the studies. Finally, only one study (20%) evaluated compassion using cualitative methods through an interview designed to analyze the elements and criteria of a school health center, which include compassion.
In reference to the format of the interventions, six works have been found in which the following compassion-related intervention programs are applied: CBCT, ABCT (García-Campayo et al., 2016b), MBCP program with compassion training, CFT (García-Campayo et al., 2016a) and LKM/CM.
Instrument Validation Studies
As for the works included on instrument validations, three studies (75%) were based on the analysis of the psychometric properties of the Jefferson Scale of Physician Empathy, but in different versions. The results of them confirmed the internal consistency (Cronbach’s alpha around 0.74 and 0.82) and its construct validity based on a three-factor model: perspective taking, compassionate care and the ability to put oneself in the other’s shoes.
Finally, only one study (25%) aimed at translating and validating the instrument “The Compassion Of Others’ Lives scale” (Chang et al., 2014). This scale is based on the theoretical model of empathy-altruism, but only operationalizes the dimensions of empathy and relief behavior by excluding the assessment of altruistic motivations. It allows for an overall score of the degree of compassion towards others, as well as a score for each subscale (empathy and relief of suffering). The results presented satisfactory psychometric properties such as a high internal consistency (Cronbach’s alpha α = 0.93) and the validity of internal factor structure obtained differs from that proposed by the original authors in that this new study divides the scale into two sub-dimensions (empathy and relief of suffering), obtaining a better partial adjustment to the data than that provided by the one-dimensional model with a single factor (compassion).
Discussion
The aim of this study was to understand the conceptual nuances of compassion and compassionate care in the Spanish-speaking health care setting, through a systematic review. Most conceptual studies on compassion in Spanish-speaking healthcare contexts define compassion as the recognition of suffering and the attempt or desire to alleviate it. Some of the studies focus on its role in reinforcing empathy, love, altruism, kindness and action to alleviate suffering (Sinclair et al., 2016a, 2016b, 2016c). Other studies define it as a construct, a feeling, a performance, an emotion or a skill.
Through our review we have noted that there is no agreement on the term compassion since it is conceptualized from different perspectives such as the evolutionary approach, the theory of moral emotions, Buddhism and the differentiation between Eastern and Western culture. However, it has been identified that all definitions have two elements in common: the recognition of suffering and the active component that motivates it to alleviate it. It should be noted that four studies (Asensio-Martínez et al., 2019; Elices et al., 2017; Klos & Lemos, 2018; Montero-Marin et al., 2016) have a common definition, in which they categorize compassion as a complex construct or process involving cognitive, affective and behavioral characteristics in a situation of suffering. This is a multidimensional understanding of compassion that differs from other works that provide one-dimensional conceptualizations, limiting compassion to a feeling, a trait or a virtue.
Compassion is a complex concept that does not always seem to be well understood, as it is often associated with other terms such as empathy, sympathy, pity and other emotions that may arise in response to the suffering of others. In relation to these terms, a study has been identified (Araya & Moncada, 2016) that defines compassion as a feeling of commiseration and pity for those who suffer hardship. In this line, in the study by Benito et al. (2016), it is recognized that in our cultural environment it is a term that is misunderstood and discredited because it is associated with pity and it is necessary and important to differentiate these concepts. This reflection is consistent with another article, in which compassion is not understood as a passive emotion, which would be characteristic of pity, but as a more complex process that involves the desire for others to stop suffering and includes the active search for relief of suffering (Ques, 2019).
As regards the association with empathy, one study (Bellosta-Batalla et al., 2019a, 2019b) explains that empathy is a necessary condition in the healthy approach to suffering, becoming the basis on which, the compassionate attitude is sustained. This paper proposes an explanatory model in which the association between these constructs is established and influences the evolution from empathy to compassion. This evolution supposes a variation in the internal experience of the observer that generates healthy emotions in which the intention to alleviate suffering is included and favors the appearance of compassion. Specifically, the model explains that in the establishment of a healthy empathy and in the desire to alleviate the suffering of others, the different components of compassion are integrated: the increase in sensitivity to the suffering of others (cognitive and emotional empathy), the actions that are carried out with the intention of alleviating it and the effective management of the emotions associated with this approach, avoiding a response of sympathy and/or empathic distress, since a secure base is formed in which there is a separation from the emotions of others. In short, this model mentions that compassion is an extension of empathy since it integrates several essential aspects of it. This view is congruent with other studies that understand compassion as a construct beyond empathy (Sinclair et al., 2016a; Strauss et al., 2016).
The rest of the studies that do not provide a definition, mention some behaviors that characterize the compassionate care of health professionals, such as: getting involved in the feeling and history of patients, expressing concern and understanding for their feelings, actively listening, helping, being present and maintaining communication by showing interest. These aspects of compassionate care are consistent with previous research that explains how the presence of these elements positively influences the overall care experience and the patient’s perception of their physician (Sinclair et al., 2016a).
Despite the findings of this systematic review that contribute to knowledge about the conceptualization and application of compassion in the Spanish-speaking health care setting, our work has certain limitations. After an exhaustive search, few papers have been obtained that have studied only compassion in the Spanish-speaking health care setting, being a total of twenty-seven studies, with very different objectives. It has been noted that there is a greater focus on concepts related to compassion that seems to have led to a paradoxical neglect of the construct itself, as considerably more studies of self-pity, compassion fatigue, or compassion satisfaction have been identified during the article selection process. This fact has led to the inclusion in our analysis of studies that, although primarily focused on the analysis of self-pity or empathy, included a brief description of compassion. In addition, by means of the proposed search strategy, we have tried to collect all the evidence in Spanish language about compassion, but there is scientific information in other studies on this thematic line that has not been identified in this review since it is not framed within our inclusion criteria. In particular, the non-inclusion of grey literature may be an important limitation. Finally, another possible limitation is the use of general search terms, which may result in a less targeted search. However, this was done with the aim of reaching the maximum number of publications on the concept of compassion in the Spanish-speaking healthcare context. All these aspects will be taken into account in future studies.
Based on the results obtained that point out the gaps that still exist in the scientific evidence in this line of research mainly in the Spanish-speaking context, it is considered necessary to carry out in future research the conceptual analysis of compassion based on empirical studies that identify the perceptions and meaning that patients and health professionals attribute to compassionate care. In this way, a more explicit definition of the construct within health care would be obtained, distinguishing it from other contexts and codifying the central elements from the perspective of those who are at the epicenter of the exchange of compassionate care. This would provide an empirical basis for the operationalization of aspects of compassion in clinical practice and thereby contribute to the development of interventions that aim to improve compassionate care in the clinical setting and instruments to measure patients’ experiences of compassion. In this way, future lines of research could focus on the development of compassion assessment instruments adapted to the Spanish-speaking health care context, as well as the development of specific interventions to improve this skill and improve health care.
We believe that this review provides a good basis for even more systematic studies to be carried out in the future. In addition, our work can help to better understand the term compassion in the Spanish-speaking health care setting, which can help to design specific interventions adapted to this context. In this way, interventions can be tailored to the characteristics of health systems in the Spanish-speaking context, taking into account their specific potential and limitations. Therefore, we conclude that it is highly relevant and a priority to carry out more research on compassion in the Spanish-speaking healthcare context that will provide evidence regarding this construct and its application, taking into account the different socio-cultural and healthcare contexts, since it is an area of interest that has been little studied and is showing satisfactory results.
References
Aguado, J., Luciano, J. V., Cebolla, A., Serrano-Blanco, A., Soler, J., & García-Campayo, J. (2015). Bifactor analysis and construct validity of the five-facet mindfulness questionnaire (FFMQ) in non-clinical Spanish samples. Frontiers in Psychology, 6, 1–14. https://doi.org/10.3389/fpsyg.2015.00404.
*Albright, K., Barnard, J., O'Leary, S., Federico, S., Saville, A., Lockhart, S., & Kempe, A. (2016). School-based health centers as medical homes: Parents’ and adolescents’ perspectives. Academic Pediatrics, 16(4), 381–386. https://doi.org/10.1016/j.acap.2015.06.004.
*Alcorta-Garza, A., González-Guerrero, J. F., Tavitas-Herrera, S. E., Rodríguez-Lara, F. J., & Hojat, M. (2005). Validación de la escala de empatía médica de Jefferson en estudiantes de medicina mexicanos. Salud mental, 28(5), 57–63.
Alonso, J., Prieto, L., & Anto, J. M. (1995). The Spanish version of the SF-36 Health Survey (the SF-36 health questionnaire): An instrument for measuring clinical results. Medicina Clínica, 104(20), 771–776.
Alonso, L. M., Caro, S. E., Erazo Coronado, A. M., & Díaz Narváez, V. P. (2013). Measurement of empathetic orientation in medicine students of Universidad del Norte. Barranquilla (Colombia). Revista Salud Uninorte, 29(1), 22–33.
Andreu, Y., Galdón, M. J., Dura, E., Ferrando, M., Murgui, S., García, A., & Ibáñez, E. (2008). Psychometric properties of the Brief Symptoms Inventory-18 (BSI-18) in a Spanish sample of outpatients with psychiatric disorders. Psicothema, 20(4), 844–850.
*Araya, C., & Moncada, L. (2016). Auto-compasión: origen, concepto y evidencias preliminares. Revista Argentina de Clínica Psicológica, 25(1), 67–78.
*Asensio-Martínez, Á., Oliván-Blázquez, B., Montero-Marín, J., Masluk, B., Fueyo-Díaz, R., Gascón-Santos, S., et al. (2019). Relation of the psychological constructs of resilience, mindfulness, and self-compassion on the perception of physical and mental health. Psychology Research and Behavior Management, 12, 1155–1166. https://doi.org/10.2147/PRBM.S225169.
Atienza, F. L., Balaguer, I., & Moreno, Y. (2000). Análisis de la dimensionalidad de la Escala de autoestima de Rosenberg en una muestra de adolescentes valencianos. Revista de Psicología Universitas Tarraconensis, 22, 29–42.
Badia, X., Roset, M., Montserrat, S., Herdman, M., & Segura, A. (1999). The Spanish version of EuroQol: A description and its applications. European Quality of Life scale. Medicina clinica, 112, 79–85.
Bados, A., Solanas, A., & Andrés, R. (2005). Psychometric properties of the Spanish version of Depression, Anxiety and Stress Scale (DASS). Psicothema, 17, 679–683.
Barrachina, J., Soler, J., Campins, M. J., Tejero, A., Pascual, J. C., Alvarez, E., Zanarini, M. C., & Pérez Sola, V. (2004). Validation of a Spanish version of the diagnostic interview for Bordelines-revised (DIB-R). Actas Españolas de Psiquiatría, 32(5), 293–298.
*Bellosta-Batalla, M., Cebolla, A., Pérez-Blasco, J., & Moya-Albiol, L. (2019a). La empatía en el ejercicio y formación de los psicólogos clínicos y sanitaristas, y su relación con mindfulness y compasión. Revista Argentina de Clínica Psicológica, 28(2), 210–220.
*Bellosta-Batalla, M., Garrote-Caparrós, E., Pérez-Blasco, J., Moya-Albiol, L., & Cebolla, A. (2019b). Mindfulness, empatía y compasión: Evolución de la empatía a la compasión en el ámbito sanitario. Revista de Investigación y Educación en Ciencias de la Salud, 4(1), 47–57.
Belmonte, R. M., Garin, O. B., Segura, M. B., Sanz, J. L., Marco, E. N., & Ferrer, M. F. (2011). Functional assessment of cancer therapy questionnaire for breast cancer (FACT-B+ 4). Spanish version validation. Medicina Clínica, 137(15), 685–688. https://doi.org/10.1016/j.medcli.2010.11.028.
*Benito, E., Dones, M., & Babero, J. (2016). El acompañamiento espiritual en cuidados paliativos. Psicooncologia, 13(2–3), 367–384. https://doi.org/10.5209/PSIC.54442.
Bilbao, J.., Olaciregui, A. A., Salazar, G., Rivera, I., Zamorano, A., & Narváez, V. D. (2013). Evaluación de la orientación empática en estudiantes de odontología de la Fundación Universitaria San Martín. Puerto Colombia (Atlántico, Colombia). Salud Uninorte, 29(1), 34–41.
*Blanco, J. M., Caballero, F., García, F. J., Lorenzo, F., & Monge, D. (2018). Validation of the Jefferson scale of physician empathy in Spanish medical students who participated in an early clerkship immersion programme. BMC Medical Education, 18(1), 209–220. https://doi.org/10.1186/s12909-018-1309-9.
Booth, A., Clarke, M., Dooley, G., Ghersi, D., Moher, D., Petticrew, M. y Stewart, L. (2012). The nuts and bolts of PROSPERO: an international prospective register of systematic reviews. Systematic Reviews, 1(1), 1–9. https://doi.org/10.1186/2046-4053-1-2.
Bresó, E., Salanova, M., Schaufeli, W. B., & Nogareda, C. (2007). Nota técnica de prevención 732: Síndrome de estar quemado por el trabajo “Burnout”(III): Instrumento de medición. Accessible at: https://www.researchgate.net/publication/46687214_Sindrome_de_estar_quemado_por_el_trabajo_Burnout_III_Instrumento_de_medicion. Accessed 15 Jun 2021.
Callwood, A., Cooke, D. y Allan, H. (2014). Developing and piloting the multiple mini-interview in pre-registration student midwife selection in a UK setting. Nurse Education Today, 34(12), 1450–1454. https://doi.org/10.1016/j.nedt.2014.04.023.
Cebolla, A., Garcia-Palacios, A., Soler, J., Guillén, V., Baños, R., & Botella, C. (2012). Psychometric properties of the Spanish validation of the Five Facets of Mindfulness Questionnaire (FFMQ). The European Journal of Psychiatry, 26(2), 118–126. https://doi.org/10.4321/S0213-61632012000200005.
Chachula, K. M. A. (2020). Comprehensive review of compassion fatigue in pre-licensure health students: Antecedents, attributes, and consequences. Current Psychology. https://doi.org/10.1007/s12144-020-01122-3.
Chang, J., Fresco, J., & Green, B. (2014). The development and validation of the Compassion of Others’ Lives Scale (the COOL Scale). International Journal of Humanities and Social Science, 4(5), 33–42.
Covidence systematic review software. (2018). Disponible en: www. covidence.org
Davis, M. H. (1983). Measuring individual differences in empathy: Evidence for a multidimensional approach. Journal of Personality and Social Psychology, 44(1), 113–126. https://doi.org/10.1037/0022-3514.44.1.113.
Davies, K. A., Lane, A. M., Devonport, T. J., & Scott, J. A. (2010). Validity and reliability of a brief emotional intelligence scale (BEIS-10). Journal of Individual Differences, 31, 198–208. https://doi.org/10.1027/1614-0001/a000028.
Daza, P., Novy, D. M., Stanley, M. A., & Averill, P. (2002). The depression anxiety stress scale-21: Spanish translation and validation with a Hispanic sample. Journal of Psychopathology and Behavioral Assessment, 24(3), 195–205. https://doi.org/10.1023/A:1016014818163.
Delgado-Fernández, M., Tercedor-Sánchez, P., & Soto-Hermoso, V. M. (2005). Traducción de las Guías para el procesamiento de datos y análisis del Cuestionario Internacional de Actividad Física (IPAQ). Versiones corta y larga. Sevilla: Junta de Andalucía, 16.
Díaz-Marsá, M., Palomares, N., Morón, M. D., Tajima, K., Fuentes, M. E., López-Ibor, J. J., & Carrasco, J. L. (2011). Psychological factors affecting response to antidepressant drugs in fibromyalgia. Psychosomatics, 52(3), 237–244. https://doi.org/10.1016/j.psym.2010.12.014.
*Díaz-Narváez, V. P., Alonso-Palacio, L. M., Caro, S. E., Silva, M., Arboleda-Castillo, J., Bilbao, J., ... & Cervantes, E. F. (2017). Compassionate care component of the construct empathy in medical students in Colombia and Dominican Republic. Acta Medica, 33, 115–121.
Dodds, S. E., Pace, T. W., Bell, M. L., Fiero, M., Negi, L. T., Raison, C. L., & Weihs, K. L. (2015). Feasibility of Cognitively-Based Compassion Training (CBCT) for breast cancer survivors: A randomized, wait list controlled pilot study. Supportive Care in Cancer, 23(12), 3599–3608. https://doi.org/10.1007/s00520-015-2888-1.
Dolores, M. S. P., Garrido-Abejar, M., Notario-Pacheco, B., Bartolomé-Gutiérrez, R., Solera-Martínez, M. & Martínez-Vizcaíno, V. (2013). Validity of the Connor-Davidson resilience scale (10 items) in a population of elderly. Enfermería Clínica, 23(1), 14–21. https://doi.org/10.1016/j.enfcli.2012.11.006.
*Elices, M., Carmona, C., Pascual, J. C., Feliu-Soler, A., Martin-Blanco, A., & Soler, J. (2017). Compassion and self-compassion: Construct and measurement. Mindfulness & Compassion, 2(1), 34–40. https://doi.org/10.1016/j.mincom.2016.11.003.
*Feliu-Soler, A., Pascual, J. C., Elices, M., Martín-Blanco, A., Carmona, C., Cebolla, A., Simón, V., & Soler, J. (2017). Fostering self-compassion and loving-kindness in patients with borderline personality disorder: A randomized pilot study. Clinical Psychology & Psychotherapy, 24(1), 278–286. https://doi.org/10.1002/cpp.2000.
*Flores, S. L., Molina, E. H., Osuna, J. B., Vargas, R. M., & Vicuña, M. N. (2018). All with you: A new method for developing compassionate communities-experiences in Spain and Latin-America. Annals of Palliative Medicine, 7, 15–31. https://doi.org/10.21037/apm.2018.03.02.
García, J. C., Rodero, B., Alda, M., Sobradiel, N., Montero, J., & Moreno, S. (2008). Validation of the Spanish version of the Pain Catastrophizing Scale in fibromyalgia. Medicina Clínica, 131(13), 487–492. https://doi.org/10.1157/13127277.
García-Altés, A., Peiró, M., & Artells, J. J. (2019). Priorización de medidas para la consolidación de la toma de decisiones compartidas en las prestaciones del Sistema Nacional de Salud español. Gaceta Sanitaria, 33(5), 408–414. https://doi.org/10.1016/j.gaceta.2018.04.017.
Garcia-Campayo, J., Navarro-Gil, M., Andrés, E., Montero-Marin, J., López-Artal, L., & Demarzo, M. M. P. (2014). Validation of the Spanish versions of the long (26 items) and short (12 items) forms of the Self-Compassion Scale (SCS). Health and Quality of Life Outcomes, 12(4), 1–9. https://doi.org/10.1186/1477-7525-12-4.
García-Campayo, J., Cebolla, A., & Demarzo, M. M. (2016a). La ciencia de la compasión. Alianza Editorial.
García-Campayo, J., Navarro-Gil, M., & Demarzo, M. (2016b). Attachment-based compassion therapy. Mindfulness & Compassion, 1(2), 68–74. https://doi.org/10.1016/j.mincom.2016.10.004.
Garcia-Esteve, L., Ascaso, C., Ojuel, J., & Navarro, P. (2003). Validation of the Edinburgh postnatal depression scale (EPDS) in Spanish mothers. Journal of Affective Disorders, 75(1), 71–76. https://doi.org/10.1016/S0165-0327(02)00020-4.
Garner, D. M., Olmsted, M. P., Bohr, Y., & Garfinkel, P. E. (1982). The eating attitudes test: Psychometric features and clinical correlates. Psychological Medicine, 12, 871–878.
Gilbert, P., Clarke, M., Hemel, S., Miles, J. N. V., & Irons, C. (2004). Criticizing and reassuring oneself: And exploration of forms, style and reasons in female students. British Journal of Clinical Psychology, 43, 31–35. https://doi.org/10.1348/014466504772812959.
Gonzalez-Hernández, E., Romero, R., Campos, D., Burychka, D., Diego-Pedro, R., Baños, R., et al. (2018). Cognitively-based compassion training (CBCT®) in breast cancer survivors: A randomized clinical trial study. Integrative Cancer Therapies, 17(3), 684–696. https://doi.org/10.1177/1534735418772095.
Hays, R. D., Brown, J. A., Spritzer, K. L., Dixon, W. J., & Brook, R. H. (1998). Member ratings of health care provided by 48 physician groups. Archives of Internal Medicine, 158(7), 785–790. https://doi.org/10.1001/archinte.158.7.785.
Hernández-Nieto, H. (2002). Contribuciones al análisis estadístico: sensibilidad estabilidad y consistencia de varios coeficientes de variabilidad relativa y el coeficiente de variación proporcional cvp el coeficiente. CreateSpace Independent Publishing Platform.
Hojat, M. (2016). Empathy in health professions education and patient care. Springer.
Hojat, M., Mangione, S., Nasca, T. J., Cohen, M. J., Gonnella, J. S., Erdmann, J. B., Velosky, J., & Magee, M. (2001). The Jefferson Scale of Physician Empathy: Development and preliminary psychometric data. Educational and Psychological Measurement, 61(2), 349–365. https://doi.org/10.1177/00131640121971158.
*Horcajo, L., Quiles, Y., & Quiles, M. J. (2019). Aplicación de la terapia centrada en la compasión en pacientes con un trastorno de la conducta alimentaria: un estudio piloto. Psicología Conductual, 27(2), 295–309.
Jáuregui, I., & Bolaños, P. (2011). Body image and quality of life in a Spanish population. International Journal of General Medicine, 4, 63–72. https://doi.org/10.2147/IJGM.S16201.
*Julliard, K., Vivar, J., Delgado, C., Cruz, E., Kabak, J., & Sabers, H. (2008). What Latina patients don’t tell their doctors: A qualitative study. The Annals of Family Medicine, 6(6), 543–549. https://doi.org/10.1370/afm.912.
Klein, C. F. (2008). Escala de evaluación parental (EEP): desarrollo, propiedades psicométricas y aplicaciones. Universitas Psychologica, 7(2), 468–468.
Klimecki, O. M., Leiberg, S., Ricard, M., & Singer, T. (2014). Differential pattern of functional brain plasticity after compassion and empathy training. Social cognitive and affective neuroscience, 9(6), 873–879. https://doi.org/10.1093/scan/nst060.
*Klos, M. C., & Lemos, V. N. (2018). Adaptación y validación de un instrumento para evaluar el constructo compasión. Revista Evaluar, 18(2), 31–44. https://doi.org/10.35670/1667-4545.v18.n2.20801.
*Melgar-Moran, C. C., Fajardo, E., & Gómez-Luján, M. D. P. (2018). El amor, resonancia esencial del cuidado para la vida, desde la experiencia del familiar donante renal vivo. Lima (Perú). Revista Salud Uninorte, 34(3), 687–695.
Mercadillo, R. E., Barrios, F. A., & Diaz, J. L. (2007). Definition of compassion-evoking images in a Mexican sample. Perceptual and Motor Skills, 105(2), 661–676.
Minayo, M. (2003). Investigación Social. Teoría, métodos y creatividad. Lugar Editorial.
Moher, D., Shamseer, L., Clarke, M., Ghersi, D., Liberati, A., Petticrew, M., et al. (2015). Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Systematic Reviews, 4(1), 1–9. https://doi.org/10.1186/2046-4053-4-1.
*Molinier, P. (2008). Trabajo y compasión en el mundo hospitalario. Una aproximación a través de la psicodinámica del trabajo. Cuadernos de relaciones laborales, 26(2), 121–138.
Montero-Marín, J., & García-Campayo, J. (2010). A newer and broader definition of burnout: Validation of the “Burnout Clinical Subtype Questionnaire (BCSQ-36)”. BMC Public Health, 10(302), 1–9. https://doi.org/10.1186/1471-2458-10-302.
*Montero-Marin, J., Zubiaga, F., Cereceda, M., Piva Demarzo, M. M., Trenc, P., & Garcia-Campayo, J. (2016). Burnout subtypes and absence of self-compassion in primary healthcare professionals: A cross-sectional study. PloS ONE, 11(6), Artículo e0157499. https://doi.org/10.1371/journal.pone.0157499.
*Montero-Marín, J., Navarro-Gil, M., Puebla-Guedea, M., Luciano, J. V., Van Gordon, W., Shonin, E., & García-Campayo, J. (2018). Efficacy of “attachment-based compassion therapy” in the treatment of fibromyalgia: A randomized controlled trial. Frontiers in Psychiatry, 8, 307–318. https://doi.org/10.3389/fpsyt.2017.00307.
*Montero-Marin, J., Collado-Navarro, C., Navarro-Gil, M., Lopez-Montoyo, A., Demarzo, M., Herrera-Mercadal, P., et al. (2019). Attachment-based compassion therapy and adapted mindfulness-based stress reduction for the treatment of depressive, anxious and adjustment disorders in mental health settings: a randomised controlled clinical trial protocol. BMJ Open, 9(10), Artículo e029909. https://doi.org/10.1136/bmjopen-2019-029909.
Montón, C., Pérez, M. E., Campos, R., García, J. C., & Lobo, A. (1993). Anxiety scales and Goldberg’s depression: An efficient interview guide for the detection of psychologic distress. Atención primaria, 12(6), 345–349.
Nápoles, A. M., Gregorich, S. E., Santoyo‐Olsson, J., O'Brien, H. & Stewart, A. L. (2009). Interpersonal processes of care and patient satisfaction: do associations differ by race, ethnicity, and language?. Health Services Research, 44(4), 1326–1344. https://doi.org/10.1111/j.1475-6773.2009.00965.x.
Nunberg, G., & Newman, E. (2011). The American heritage dictionary of the English language (5th ed.). Houghton Mifflin Harcourt.
*Ortega-Barco, M. A., & Muñoz de Rodríguez, L. (2018). Evaluation of the nursing care offered during the parturition process. Controlled clinical trial of an intervention based on Swanson’s theory of caring versus conventional care. Investigación y Educación en Enfermería, 36(1), 50–61. https://doi.org/10.17533/udea.iee.v36n1e05.
Orwin, R.G. (1994). Evaluating coding decisions. En H. Cooper y L. V. Hedges (Eds.), The handbook of research synthesis (p. 139–162). Russell Sage Foundation.
Paterson, R. (2011). Can we mandate compassion?. The Hastings Center Report, 41(2), 20–23.
Pommier, E., Neff, K. D., & Tóth-Király, I. (2020). The development and validation of the compassion scale. Assessment, 27(1), 21–39. https://doi.org/10.1177/1073191119874108.
Preckel, K., Kanske, P., & Singer, T. (2018). On the interaction of social affect and cognition: Empathy, compassion and theory of mind. Current Opinion in Behavioral Sciences, 19, 1–6. https://doi.org/10.1016/j.cobeha.2017.07.010.
Ques, Á. A. M. (2019). La ética de la compasión en el cuidado de otros. Ética de los Cuidados, 12, Artículo e90865.
Remor, E. (2006). Psychometric properties of a European Spanish version of the Perceived Stress Scale (PSS). The Spanish Journal of Psychology, 9(1), 86–93. https://doi.org/10.1017/S1138741600006004.
Riggs, J. S., Woodby, L. L., Burgio, K. L., Amos Bailey, F., & Williams, B. R. (2014). “Don’t get weak in your compassion”: Bereaved next of Kin’s suggestions for improving end-of-life care in Veterans Affairs Medical Centers. Journal of the American Geriatrics Society, 62(4), 642–648. https://doi.org/10.1111/jgs.12764.
Rivera, J., & González, T. (2004). The fibromyalgia impact questionnaire: A validated Spanish version to assess the health status in women with fibromyalgia. Clinical and Experimental Rheumatology, 22, 554–560.
Ruiz, F. J., Luciano, C., Cangas, A. J., & Beltrán, I. (2013). Measuring experiential avoidance and psychological inflexibility: The Spanish version of the acceptance and action questionnaire-II. Psicothema, 25(1), 123–129. https://doi.org/10.7334/psicothema2011.239.
Sackett, D. L., Rosenberg, W. M., Gray, J. A., Haynes, R. B., & Richardson, W. S. (1996). Evidence based medicine: What it is and what it isn't. BMJ (Clinical Research Ed.), 312(7023), 71–72. https://doi.org/10.1136/bmj.312.7023.71.
*Sacristán-Martin, O., Santed, M. A., Garcia-Campayo, J., Duncan, L. G., Bardacke, N., Fernandez-Alonso, C., et al. (2019). A mindfulness and compassion-based program applied to pregnant women and their partners to decrease depression symptoms during pregnancy and postpartum: Study protocol for a randomized controlled trial. Trials, 20(1), 654–668. https://doi.org/10.1186/s13063-019-3739-z.
Sandín, B., Chorot, P., Lostao, L., Joiner, T. E., Santed, M. A., & Valiente, R. M. (1999). Escalas PANAS de afecto positivo y negativo: validación factorial y convergencia transcultural. Psicothema, 11(1), 37–51.
Sankar, P., & Jones, N. L. (2005). To tell or not to tell: Primary care patients’ disclosure deliberations. Archives of Internal Medicine, 165(20), 2378–2383. https://doi.org/10.1001/archinte.165.20.2378.
Schaufeli, W. B., Salanova, M., González-Romá, V., & Bakker, A. B. (2002). The measurement of engagement and burnout: A two sample confirmatory factor analytic approach. Journal of Happiness Studies, 3(1), 71–92. https://doi.org/10.1023/A:1015630930326.
Seppala, E. M., Hutcherson, C. A., Nguyen, D. T., Doty, J. R., & Gross, J. J. (2014). Loving-kindness meditation: A tool to improve healthcare provider compassion, resilience, and patient care. Journal of Compassionate Health Care, 1(1), 1–9. https://doi.org/10.1186/s40639-014-0005-9.
Silva, M. G., Castillo, J. A. & Narváez, V. P. D. (2014). Empathic orientation observed in medical students at one university in the Dominican Republic. Revista Cubana de Educación Médica Superior, 28(1), 74–83.
Simard, S., & Savard, J. (2009). Fear of Cancer recurrence inventory: Development and initial validation of a multidimensional measure of fear of cancer recurrence. Supportive Care in Cancer, 17(3), 241–251. https://doi.org/10.1007/s00520-008-0444-y.
Sinclair, S., Beamer, K., Hack, T. F., McClement, S., Raffin Bouchal, S., Chochinov, H. M., & Hagen, N. A. (2016a). Sympathy, empathy, and compassion: A grounded theory study of palliative care patients’ understandings, experiences, and preferences. Palliative Medicine, 31(5), 437–447. https://doi.org/10.1177/0269216316663499.
Sinclair, S., McClement, S., Raffin-Bouchal, S., Hack, T. F., Hagen, N. A., McConnell, S., & Chochinov, H. M. (2016b). Compassion in health care: An empirical model. Journal of Pain and Symptom Management, 51(2), 193–203. https://doi.org/10.1016/j.jpainsymman.2015.10.009.
Sinclair, S., Norris, J. M., McConnell, S. J., Chochinov, H. M., Hack, T. F., Hagen, N. A., McClement, S., & Bouchal, S. R. (2016c). Compassion: A scoping review of the healthcare literature. BMC Palliative Care, 15(1), 6–20. https://doi.org/10.1186/s12904-016-0080-0.
Sinclair, S., Kondejewski, J., Raffin-Bouchal, S., King-Shier, K. M., & Singh, P. (2017a). Can self-compassion promote healthcare provider well-being and compassionate care to others? Results of a systematic review. Applied Psychology: Health and Well-Being, 9(2), 168–206. https://doi.org/10.1111/aphw.12086.
Sinclair, S., Russell, L. B., Hack, T. F., Kondejewski, J., & Sawatzky, R. (2017b). Measuring compassion in healthcare: A comprehensive and critical review. The Patient-Patient-Centered Outcomes Research, 10(4), 389–405. https://doi.org/10.1007/s40271-016-0209-5.
Sinclair, S., Hack, T. F., Raffin-Bouchal, S., McClement, S., Stajduhar, K., Singh, P., & Chochinov, H. M. (2018). What are healthcare providers’ understandings and experiences of compassion? The healthcare compassion model: A grounded theory study of healthcare providers in Canada. BMJ Open, 8(3), Artículo e019701. https://doi.org/10.1136/bmjopen-2017-019701.
Soler, J., Vega, D., Feliu-Soler, A., Trujols, J., Soto, Á., Elices, M., Ortiz, C., Pérez, V., Bohus, M., & Pascual, J. C. (2013). Validation of the Spanish version of the Borderline Symptom List, short form (BSL-23). BMC Psychiatry, 13(139), 1–7. https://doi.org/10.1186/1471-244X-13-139.
Soler, M. I., Meseguer, M., & García, M. (2016). Psychometric properties of the Spanish version of the 10-item Connor-Davidson resilience scale (10-item CD-RISC) in a sample of workers. Revista Latinoamericana de Psicología, 48(3), 159–166.
Stewart, A. L., Nápoles-Springer, A. M., Gregorich, S. E., & Santoyo-Olsson, J. (2007). Interpersonal processes of care survey: Patient-reported measures for diverse groups. Health Services Research, 42(31), 1235–1256. https://doi.org/10.1111/j.1475-6773.2006.00637.x.
Strauss, C., Taylor, B. L., Gu, J., Kuyken, W., Baer, R., Jones, F., & Cavanagh, K. (2016). What is compassion and how can we measure it? A review of definitions and measures. Clinical Psychology Review, 47, 15–27. https://doi.org/10.1016/j.cpr.2016.05.004.
Sultana, J., Trotta, F., Addis, A., Brown, J. S., Gil, M., Menniti-Ippolito, F., Milozzi, F., Suissa, S., & Trifirò, G. (2020). Healthcare database networks for drug regulatory policies: International workshop on the Canadian, US and Spanish experience and future steps for Italy. Drug Safety, 43, 1–5. https://doi.org/10.1007/s40264-019-00871-w.
Taylor, A., Hodgson, D., Gee, M., & Collins, K. (2017). Compassion in healthcare: A concept analysis. Journal of Radiotherapy in Practice, 16(4), 350–360. https://doi.org/10.1017/S1460396917000322.
*Tejada-Pérez, I. I. (2017). “No es fácil estar 24 horas en una cama”: confort del paciente con sedación en una unidad de cuidado intensivo. Aquichan, 17(4), 380–389.
Tejedor, R., Feliu-Soler, A., Pascual, J. C., Cebolla, A., Portella, M. J., Trujols, J., Soriano, J., Pérez, V., & Soler, J. (2014). Psychometric properties of the Spanish version of the Philadelphia mindfulness scale. Revista de Psiquiatría y Salud Mental (English Edition), 7(4), 157–165. https://doi.org/10.1016/j.rpsmen.2014.10.002.
*Ulloque, M. J., Villalba, S., Varela, T., Fantini, A., Quinteros, S., & Díaz-Narváez, V. P. (2019). Empathy in medical students of Córdoba, Argentina. Archivos Argentinos Pediatría, 117(2), 81–86.
*Valentín, M. J. D., Abejar, M. G., Chacón, R. M. F., Parra, M. D. S., Rubio, M. E. L., & Jiménez, S. Y. (2019). Validation to the Spanish of the Jefferson empathy scale health professions students version and its psychometric properties in nursing students. Nurse Education in Practice, 40, Artículo e102629. https://doi.org/10.1016/j.nepr.2019.102629.
Vallejo, M. A., Rivera, J., Esteve-Vives, J., & Rodríguez-Muñoz, M. F. (2012). Use of the Hospital Anxiety and Depression Scale (HADS) to evaluate anxiety and depression in fibromyalgia patients. Revista de Psiquiatría y Salud Mental (English Edition), 5(2), 107–114. https://doi.org/10.1016/j.rpsmen.2012.01.004.
Varela, T. B., Villalba, R. H., Gargantini, P., Quinteros, S., Villalba, S. B., & Díaz Narváez, V. P. (2012). Niveles de orientación empática en estudiantes de odontología de la Universdidad Católica de Córdoba, Argentina (UCC). Claves Odontol, 19(70), 15–22. https://doi.org/10.5546/aap.2019.81.
Vázquez-Barquero, J. L., Gaite, L., Cuesta, M. J., Garcia, E., Knapp, M., & Beecham, J. (1997). Spanish version of the CSRI: A mental health cost evaluation interview. Archivos de Neurobiologiá, 60, 171–184.
Vera, C. (2014). Empathetic Orientation in Dentistry students from Latin America. Literature review. Journal of Oral Research, 3(2), 123–127. https://doi.org/10.17126/joralres.2014.029.
Vesga Gualdrón, L. M., & Ruiz de Cárdenas, C. H. (2016). Validez y confiabilidad de una escala de cuidado profesional en español. Avances en Enfermería, 34(1), 69–78. https://doi.org/10.15446/av.enferm.v34n1.44488.
Watson, D., Clark, L. A., & Tellegen, A. (1988). Development and validation of brief measures of positive and negative affect: The PANAS scales. Journal of Personality and Social Psychology, 54(6), 1063–1070. https://doi.org/10.1037/0022-3514.54.6.1063.
Authors’ Contributions (Optional: Please Review the Submission Guidelines from the Journal whether Statements are Mandatory)
All authors contributed to the study conception and design. The selection of the key words and the initial searches were carried out among all the researchers. The final searches, screening and elaboration of the collection protocol were carried out by Andrea Zaragozá and Marián Pérez-Marín. The first draft of the manuscript was written by Andrea Zaragozá. The following versions were reviewed by Ana Soto-Rubio and Laura Lacomba-Trejo, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding (Information that Explains whether and by whom the Research was Supported)
Andrea Zaragozá Salvador is a beneficiary of Beca de Colaboración (2019/2020) of Ministerio de Educación y Formación Profesional of Gobierno de España and Laura Lacomba-Trejo is a beneficiary of the “Talent Attraction” pre-doctoral research staff training grant from the University of Valencia (0113/2018).
Data Availability (Data Transparency)
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Code Availability (Software Application or Custom Code)
not applicable.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics Approval (Include Appropriate Approvals or Waivers)
this study was performed in line with the principles of the Declaration of Helsinki.
Consent to Participate (Include Appropriate Statements)
not applicable.
Consent for Publication (Include Appropriate Statements)
not applicable.
Conflicts of Interest/Competing Interests (Include Appropriate Disclosures)
the authors declare that they have not conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Salvador Zaragozá, A., Soto-Rubio, A., Lacomba-Trejo, L. et al. Compassion in Spanish-speaking health care: A systematic review. Curr Psychol 42, 6732–6751 (2023). https://doi.org/10.1007/s12144-021-01994-z
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12144-021-01994-z