
Abstract
This study aimed to evaluate the associations between perceived invalidating childhood environments, attachment in intimate relationships and eating psychopathology, to explore how these variables interact with each other, and to explore potential mediators to this pattern of association in a clinical eating disorder (ED) sample. One hundred thirty-seven ED outpatients were evaluated with the Invalidating Childhood Environments Scale (ICES), the Eating Disorder-15 (ED-15) and the Experiences in Close Relationships Inventory (ECR). Paternal invalidation was associated to the ED-15 total score through avoidance of proximity and anxiety over abandonment, while maternal invalidation was only associated to the ED-15 total score through avoidance of proximity. Our results highlight the potential role of the perception of an invalidating family environment in the development of eating pathology and of difficulties in intimate relationships. These results endorse the relevance of address parental invalidation and promote adequate emotion regulation strategies and interpersonal competencies in the context of intimate relationships.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Eating disorders (EDs) – anorexia nervosa (AN), bulimia nervosa (BN), binge eating disorder (BED), and related syndromes – are serious disorders characterized by severe disturbances in eating behaviours and related thoughts and emotions (American Psychiatric Association, [APA] 2013). The peak age of onset is 15–25 years old and the average illness duration is about 6 years (Schmidt et al. 2016). EDs are highly prevalent worldwide, especially among women (Galmiche et al. 2019). According to previous research, eating psychopathology may be related with invalidating childhood environments (e.g., Haslam et al. 2008; Haynos and Fruzzetti 2011) and difficulties in intimate relationships (e.g., Gander et al. 2015). The present study aimed at exploring the interaction between these variables, considering possible mediating effects that may be found in the family, in the individual and in the clinical symptomatology, potentially inter-related and applicable in the explanation of current ED symptomatology and severity.
Eating Disorders and Perceived Invalidating Childhood Environment
An invalidating childhood environment can be defined by the delegitimizing of a child’s valid emotional experience or expression (Musser et al. 2018). Three major features must be considered when describing invalidating childhood environments: (1) the existence of a poor fit between the environment and the child’s temperament; (2) a context where the child’s personal experiences are not validated by caregivers; and (3) a pattern where the communication of emotions is considered to be unsuitable, for which children are either ignored or punished (Ford et al. 2010; Linehan 1993; Mountford et al. 2007). Specifically, four primary characteristics may be found in invalidating environments: communications of inaccuracy, misattribution, discouraging negative emotional expression, and oversimplification of problem solving (Musser et al. 2018).
According to the biosocial theory of Linehan (1993), which underlies the theoretical background of the dialectical behaviour therapy (DBT) for the treatment of borderline personality disorder, the transaction between an invalidating social and family environment and a biological disposition towards emotional vulnerability may predispose individuals to cope with their negative emotional experiences via maladaptive behaviours, such as impulsive eating, restrictive diet and excessive physical exercise (Linehan 1993), which may be linked to pervasive emotion dysregulation. Briefly, emotion regulation refers to individuals’ attempts to influence the experience and expression of emotions and, alternatively, emotion dysregulation refers to deficits in the a) awareness, understanding, and acceptance of emotions; b) ability to engage in goal-directed behaviours and inhibit impulsive behaviours; c) flexible use of situationally-appropriate strategies to modulate emotions; and d) willingness to experience and accept negative emotions (Gratz and Roemer 2004).
The biosocial theory (Linehan 1993) has been applied to EDs. For instance, Safer et al. (2001a, b, 2010) adapted the DBT (Linehan 1993) to treat difficulties in emotion regulation in BN and BED with promising decreases in binge/purge behaviours. Also, Haynos and Fruzzetti (2011) posit that individuals with AN may have experienced a history of invalidating responses regarding a variety of inner experiences stemming from societal and familial interactions.
In fact, there is considerable evidence on the relationship between invalidating childhood environment, emotion dysegulation and EDs. Ford et al. (2010) found that invalidation in childhood was associated with core beliefs in women with EDs. Specifically, the experience of a chaotic family was associated with core beliefs that reflect maladaptive emotional functioning and maladaptive inter and intra-personal styles. This study replicated earlier research that concluded that an invalidating childhood environment was associated with the presence of an ED during adulthood, compared with those who reported a validating childhood environment, being the latter less likely to develop an ED (Mountford et al. 2007). Haslam et al. (2008) also found that patients with BN scored higher on levels of paternal invalidation than those with AN. On its turn, paternal invalidation was associated with vomiting, while an emotionally controlled and high achieving family style was associated with excessive exercise. Further, bingeing was less associated with maternal invalidation, leading the authors to hypothesize that maternal invalidation might be associated with food restriction.
To summarise, individuals raised in invalidating families in which the expression of negative emotions was not validated, may be predisposed to invalidate their own negative emotions, which seems to result in a pervasive pattern of emotion dysregulation in ED patients. A perceived invalidating childhood environment is also related to eating psychopathology, and bingeing and purging or restrictive eating behaviours may be related to under and over-controlled emotion regulation strategies. Therefore, our main aim in this study was to evaluate the potential mechanisms through which some patterns in the family, in the individual and in the clinical symptomatology may be inter-related and relevant in the explanation of current ED symptomatology in a clinical sample of EDs. So far, it is unclear how a perceived invalidating childhood environment might result in eating problems later in life. One possible mechanism to understand this association is through the presence of attachment avoidance and anxiety, since women with EDs report insecure romantic attachment (Evans and Wertheim 2005), and a perceived invalidating childhood environment has been associated to negative core beliefs, which reflects maladaptive emotional functioning and dysfunctional inter or intra-personal styles (Ford et al. 2010).
Eating Disorders, Intimate Relationships and Attachment
An intimate relationship has been described as a particularly close interpersonal relationship that involves physical or emotional intimacy (Miller and Perlman 2007). Research has demonstrated that patients with EDs present relationship difficulties, intimacy problems and marital dysfunction (cf. Arcelus et al. 2012, for a review). For instance, a study by Evans and Wertheim (2005) concluded that women with EDs reported insecure attachment and negative feelings towards partners. In a systematic review regarding the role of interpersonal functioning in EDs, Arcelus et al. (2013) concluded that interpersonal difficulties in patients with restrictive behaviours appear to be related to the avoidance in the expression of feelings to others and to prioritize other’s individuals’s feelings over their own, while interpersonal difficulties in patients with BN appear to be more related to distrust and negative interactions with others.
In the scope of the comprehension of intimate relationships and their potential difficulties experienced by ED patients, the attachment theory has emerged as the most suitable model (Bowlby 1969). Attachment is the mechanism by which individuals form close bonds with others (Hazan and Shaver 1987) and it seems closely related to emotion regulation and emotional reactions to stressful events, particularly perceived threats to one’ relationships. Tasca and Balfour (2014) explained that individuals with secure attachment styles are able to maintain measured approaches and respond to interpersonal stressors and/or the absence of attachment figures more adaptably. Interpersonally, these individuals can accept intimacy, express affection and support others without feeling overwhelmed, anxious, or dismissive. In this sense, attachment orientation can be assessed in terms of two orthogonal dimensions: attachment anxiety and attachment avoidance (e.g., Gander et al. 2015; Tasca et al. 2018).
In a recent meta-analysis, results showed that higher levels of attachment anxiety and avoidance were significantly associated with more unhealthy eating behaviours in community samples (Faber et al. 2018). In another review, Jewell et al. (2016) discussed the findings from longitudinal studies suggesting that insecure attachment in early childhood seems to be a distal risk factor with a relatively weak effect on the development of eating pathology during adolescence, whereas insecure attachment in pre-adolescence is more likely to predict eating pathology. Moreover, insecure attachment may be a potential risk factor for the development and maintenance of EDs (Tasca et al. 2018). In a review of the literature, Gander et al. (2015) systematized results supporting the presence of insecure attachment styles amongst adolescents and young adults with EDs, with some authors finding higher prevalence of the avoidant attachment styles, while others found higher prevalence of anxious attachment styles.
Some authors have speculated that an anxious attachment style might be associated with binge eating and purging behaviours, while an avoidant attachment style may be linked to dietary restriction. Indeed, Gander et al. (2015) acknowledge the inconsistent findings regarding this matter, stating that the diagnostic subgroup is not necessarily related to attachment insecurity dimensions. Accordingly, a recent study suggested that attachment anxiety and avoidance independently predicted EDs symptoms above-and-beyond differences between ED diagnoses (Tasca et al. 2018).
In sum, women with EDs and sub-clinical disordered eating symptoms, when compared to controls, displayed characteristics consistent with anxious and avoidant attachment styles. Therefore, women with EDs experienced vigilance and concerns about rejection and abandonment (anxiety) and discomfort with closeness in relationships (avoidance) with their intimate partners (Ward et al. 2000; Broberg et al. 2001). By considering the attachment theory, as an attempt to explain the difficulties in intimate relationships found in ED patients, and the experience of growing up in invalidating families, a better understanding of ED symptomatology and severity could be reached. Previous studies did not completely explain why growing up in invalidating families may predispose individuals to cope with negative emotional experiences via ED symptoms that, as well, may serve as inadequate strategies to regulate emotions and to deal with the experience of difficulties in intimate relationships.
Current Study
To our knowledge, there are no studies that have been conducted with clinical samples of EDs that have explored both perceived invalidating childhood environments and attachment in intimate relationships during adulthood. This study extends on a previous study by Gonçalves et al. (2018) with a non-clinical sample that found that difficulties in establishing intimate relationships, body dissatisfaction and related EDs symptoms were stronger in invalidating families.
The current study encompasses two main objectives. First, we aimed to explore the associations between perceived invalidating childhood environments, attachment in intimate relationships and eating psychopathology; and second, we aimed to explore how these variables interact between each other, and potential mediators in this association. Considering the unquestionable role of both family environment during childhood and current adult intimate relationships, we intended to deepen the knowledge about perception of invalidation during childhood, current experiences in intimate relationships in terms of difficulties in dealing with avoidance of intimacy and anxiety over abandonment, and eating psychopathology in a clinical sample of ED patients. We hypothesize that having been previously invalidated in family raises difficulties in emotion regulation and undermines current intimate adaptive functioning through anxiety and avoidance of intimacy. This may also increase EDs symptoms and maladaptive emotion regulation strategies to cope with the sense of vigilance, concerns about rejection and abandonment, and discomfort in the intimacy.
Method
Participants
The sample consisted of 137 Portuguese ED outpatients (114 adults, 21 minors), caucasian and predominantly females (n = 128, 93.4%). According to the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; APA 2013), participants met criteria for: AN, restricting type or binge eating/purging type (n = 66, 50.4%); BN (n = 26, 19.8%); BED (n = 14, 10.7%); and other specified or unspecified eating disorders (OSFED; n = 25, 19.1%). Table 1 displays the sociodemographic and clinical characteristics of the sample, according to the DSM-5 (APA 2013) diagnostic groups.
Participants were recruited through referrals by clinicians at two public psychiatric units (one included specialized consultation for the treatment of ED) and one psychological service integrated in the university. This service provides psychological counseling to the students and to the general community. Of the referred outpatients, 145 consented and participated in the study. However, seven participants did not complete most of the measures and one participant did not meet diagnostic criteria for an ED. These participants were excluded from the study. Information regarding the number of participants who were referred to the study and did not consent is not available.
Measures
Invalidating Childhood Environments Scale (ICES; Mountford et al. 2007; Portuguese Version by Vieira et al. 2018)
This self-report measure consists of 14 items that assess maternal and paternal behaviours (e.g., “My parents would become angry if I disagreed with them”; “My parents would understand and help me if I couldn’t do something straight away”). Participants rate their experiences with each parent up to the age of 18, using the first 14 items on a Likert scale ranging from 1 (never) to 5 (all the time). Items 5, 8, 12 and 14 are reverse scored. Invalidating scores are derived for each parent – paternal and maternal invalidation. Higher scores reflect a greater perception of invalidation by one’s father and mother.
On the second part of the questionnaire, four items correspond to different family types: “chaotic” (parents are often unavailable and may have substance abuse problems, mental health disorders or financial difficulties), “validating” (an emotionally supportive environment), “perfect” (focus is on hiding feelings and getting on with it), and “typical” (the focus of the family is controlling one’s emotions, achievement and success). The participants are requested to respond using a Likert scale ranging from 1 (not like my family) to 5 (like my family all of the time). Four types of families (one validating and three invalidating) are defined using a score that corresponds to the individual’s perceptions of his/her family type. An individual might identify him- or herself with more than one family type. Higher average scores denote higher levels of “chaotic”, “validating”, “perfect” and “typical” family types.
In the present study, we consider the paternal and maternal invalidation scores in the multivariate analyses of variance (MANOVA), correlational matrix and in the parallel multiple mediator models. Family types are only considered in the Spearman’s (rs) correlations. The results of the original version of the ICES (Mountford et al. 2007) suggested acceptable levels of internal consistency in terms of maternal (α = .77) and paternal invalidation (α = .80). In the study of the Portuguese version of the ICES (Vieira et al. 2018), reliability analyses also showed good internal consistency for both the paternal invalidation (α = .86) and the maternal invalidation (α = .89). The internal consistency results in this study are .89 and .86 for maternal and paternal invalidation, respectively.
Eating Disorder-15 (Tatham et al. 2015; Portuguese Version by Rodrigues et al. 2019)
This self-report measure consists of 10 items that assess eating attitudes, using a Likert scale ranging from 0 (not at all) to 6 (all the time). Two subscales are derived: eating concerns (e.g., “Worried about losing control over my eating”) and weight and shape concerns (e.g., “Avoided activities or people because of the way I look”). The total score is computed by the mean of the 10 items. Higher scores suggest greater levels of eating pathology. The last five items assess eating behaviours over the past week: binge-eating episodes, self-induced vomiting episodes, laxative misuse days, excessive exercise days and eating restraint days.
In the present study, we consider the ED-15 total score, the weight and shape concerns and eating concerns subscales in the correlational matrix and only the ED-15 total score in the parallel multiple mediator models. Eating behaviours are considered in the Spearman’s (rs) correlations. The results of the original version of the ED-15 (Tatham et al. 2015) suggested strong levels of internal consistency for the weight and shape concerns (α = .94) and for the eating concerns (α = .80) subscales. In the study of its Portuguese version, ED-15 total score revealed an excellent internal consistency in a clinical EDs sample and in a nonclinical sample (α = .93 and α = .91, respectively), temporal stability (intraclass correlation coefficient = .84; 95% CI [.72–.91]), and acceptable concurrent and convergent validity. Internal consistency values ranged from .79 to .92 in the present study.
Experiences in Close Relationships Inventory (ECR; Brennan et al. 1998; Portuguese Version by Paiva and Figueiredo 2010)
This self-report measure consists of 36 items that assess adult attachment styles, using a Likert scale ranging from 1 (strongly disagree) to 7 (strongly agree). The ECR measures individuals on two subscales of attachment: avoidance (e.g., “I find it difficult to allow myself to depend on romantic partners”) and anxiety (e.g., “I’m afraid that I will lose my partner’s love”). Higher scores suggest greater levels of avoidance of intimacy and anxiety related to abandonment. The total score is computed by the mean of both subscales.
In this study, we consider the avoidance and anxiety subscales in the MANOVA, correlational matrix and in the parallel multiple mediator models. The ECR total score is only considered in Pearson’s (r) and Spearman’s (rs) correlations. According Mikulincer and Shaver (2007), the ECR has been used in a variety of studies with high reliability (alpha coefficients were near or above .90). In the study of validation of the Portuguese version of the ECR, the total scale had good internal consistency (α = .86), as well as the avoidance (α = .88) and anxiety (α = .86) subscales. In the current study, the internal consistency for avoidance is .85, for anxiety .89 and .88 for the total score.
Procedure
This study was authorized and approved by the institutional review board committees of the institutions involved. All participants were diagnosed by their psychiatrists or psychologists with a clinical interview. At the time of the data collection, diagnoses were reviewed by clinicians and researchers according to the DSM-5 criteria. After that, researchers applied the ED-15 questionnaire to assess ED cognitions and behaviours, a measure validated for the Portuguese population with sound psychometric properties and the potential to distinguish clinical presentations of eating psychopathology from nonclinical cases (Rodrigues et al. 2019). Participants were informed about the research aims and data confidentiality was assured. Adult participants provided written informed consent and for minors written informed consent was provided by their legal tutors.
Statistical Analyses
The statistical analyses are conducted with IBM SPSS Statistics 24.0 (SPSS Inc., Chicago, IL). To describe the characteristics of intimate relationships, descriptive statistics are performed. MANOVA analyses are also conducted with the relationship status and the diagnostic group as independent variables and the perceived invalidating childhood environment (paternal and maternal invalidation) and attachment styles (anxiety and avoidance) as dependent variables. Pearson’s (r) and Spearman’s (rs) correlation coefficients were used to explore the associations between the main variables of the study: perceived invalidating childhood environment (ICES), eating psychopathology (ED-15) and adult attachment styles (ECR). We also test the role of attachment anxiety and avoidance in intimate relationships as potential mediators of the association between perceived invalidating childhood environments and ED psychopathology. These variables were first selected based on previous evidence (Evans and Wertheim 2005; Haslam et al. 2008; Ford et al. 2010).
According to Baron and Kenny (1986), a mediator is a third variable that represents the mechanism through which the independent variable may influence the dependent variable. Therefore, parallel multiple mediation analyses are conducted for the ED-15 total score as a dependent variable (Y), paternal and maternal invalidation as independent variables (X), and avoidance and anxiety styles as potential mediators (M1 and M2). In each of the mediation models, only one X affects one Y through M1 and M2. According to Hayes (2013), in a parallel multiple mediator model, no mediator causally influences another. If two mediators are correlated even after controlling for X, this suggests that one mediator affects the other. This condition was verified using a partial correlation to measure the association between two mediators while controlling for the effect of X.Footnote 1
The multiple mediation models are tested using the PROCESS macro for SPSS (Hayes 2013) that calculates unstandardized total, direct and indirect effects. The direct effect (c´) represents the relationship between X and Y when M is included in the model. The indirect effect (a1b1 or a2b2; the product of path a and path b) is the effect of X on Y through M. PROCESS gives an estimate of the indirect effects as well as a bootstrapped standard error and a 95% confidence interval (CI). A CI that does not contain zero suggests the likelihood of a genuine indirect effect. The total effect (c) is the sum of the direct and indirect effects. The total indirect effect represents the indirect effect of X on Y summed across all mediators. PROCESS also conducts pairwise comparisons, one for each possible difference between indirect effects. A CI that does not contain zero provides evidence that the indirect effects are statistically different from each other, whereas a CI that includes zero supports no difference between the indirect effects.
Results
One hundred and nine participants (79.5%) reported having a current or past intimate relationship, whereas 17 participants (12.4%) reported never having had a relationship. Among those participants who reported a relationship, 46.7% were currently in a relationship. The average length of the most recent relationship was 70.35 months (SD = 101.83).
MANOVA was conducted with the relationship status as the independent variable and the perceived invalidating childhood environment (paternal and maternal invalidation) and attachment styles (anxiety and avoidance) as dependent variables. Findings revealed no significant multivariate differences between the groups in the perceived invalidating childhood environment, Wilks’ λ = .92, F (4, 222) = 2.23, p = .07, as well as in attachment styles, Wilks’ λ = .95, F (4, 242) = 1.54, p = .19. MANOVA analyses were also conducted with the diagnostic group (AN, BN, BED and OSFED) as the independent variable and the perceived invalidating childhood environment (paternal and maternal invalidation) and attachment styles (anxiety and avoidance) as dependent variables. Findings revealed no significant multivariate differences between the groups in the perceived invalidating childhood environment, Wilks’ λ = .92, F (6, 228) = 1.57, p = .16, as well as in attachment styles, Wilks’ λ = .95, F (6, 250) = 1.15, p = .33.
There were no significant differences between adults and minors regarding the ED-15 total score, t (133) = −.53, p = .60, paternal invalidation, t (12) = −.61, p = .54, maternal invalidation t (126) = .09, p = .93, avoidance of proximity, t (132) = .85, p = .40 and anxiety related to abandonment, t (133) = −1.17, p = .24.
Associations Among Perceived Invalidating Childhood Environment, Eating Psychopathology and Attachment in Intimate Relationships
The correlational matrix showed that the perception of paternal invalidation was weakly, significantly and positively correlated with weight and shape concerns and with the ED-15 total score. Paternal invalidation was also weakly and significantly correlated with attachment dimensions of ECR: avoidance and anxiety, and moderately correlated with the ECR total score. On the other hand, maternal invalidation was weakly and positively associated with avoidance and ERC total scores. Higher levels of weight and shape concerns were moderately associated with higher levels of avoidance, anxiety and with the ECR total scores. More eating concerns were also weakly, significantly and positively correlated with avoidance, and moderately associated with anxiety and ECR total scores. Finally, higher ED-15 total scores were weakly associated with higher levels of avoidance and moderately correlated with anxiety and higher ECR total scores.
Regarding the styles of invalidating environment, higher scores in the chaotic family were weakly correlated with more avoidance in intimate relationships and higher ECR total scores. A typical family was weakly and positively correlated with anxious attachment while a validating family was weakly and negatively correlated with avoidance and ECR total scores. Regarding disordered eating behaviours, binge-eating episodes were weakly associated with paternal and maternal invalidation. More laxative misuse days were weakly associated with more avoidance in intimate relationships and higher ECR total scores. Finally, eating restraint days were also weakly and positively correlated with attachment dimensions: avoidance, anxiety and total score. The results of correlation analyses are presented in Table 2.
Parallel Multiple Mediator Models
Two parallel multiple mediator models were conducted. In the first one, the ED-15 total score was defined as Y, paternal invalidation as X, and anxiety and avoidance in intimate relationships were entered as M1 and M2, respectively. A second model was tested in which the ED-15 total score was defined as Y, maternal invalidation as X, and anxiety and avoidance in close relationships were entered as M1 and M2, respectively. A direct path linking paternal invalidation to eating psychopathology was also included in the models.
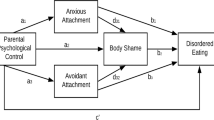
As seen in Fig. 1 and Table 3, the total effect of paternal invalidation on the ED-15 total score was significant, c = .027, t = 2.128, p = .035. Paternal invalidation was also related to ED-15 total score through avoidance of proximity, a1b1 = .010, CI [.002, .023], and anxiety related to abandonment, a2b2 = .008, CI [.0002, .018], as both CIs did not include zero. The difference between the indirect effects was .003, but a 95% CI included zero (−.008 to .016). Therefore, the indirect effect of paternal invalidation on ED-15 total score through avoidance was no different than the indirect effect through anxiety. The total indirect effect of paternal invalidation through both mediators simultaneously was between .005 and .036. Paternal invalidation was not significantly associated with the ED-15 total score after controlling for anxiety and avoidance in intimate relationships, c´ = .009, t = .706, p = .481. The model accounted for 19% of the variance of the ED-15 total score.

Statistical diagram for the parallel multiple mediator model with both anxiety and avoidance in intimate relationships as potential mediators of the relationship between paternal invalidation and ED-15 total score. a1 = the coefficient of the X - > the mediator 1 (M1), a2 = the coefficient of the X - > the mediator 2 (M2), b1 = the coefficient of M1 - > Y, b2 = the coefficient of M2 - > Y, c´ = the direct effect of X on Y. All endogenous variables were associated with errors which, for the sake of simplicity, are not shown in this figure. *p < .05, **p < .01, ***p < .001
In the model related to maternal invalidation, considering the ED-15 total score as a dependent variable (Fig. 2, Table 3), the total effect of maternal invalidation on ED-15 total score was not significant, c = .019, t = 1.531, p = .128. On the other hand, maternal invalidation was related to the ED-15 total score through avoidance of proximity, a1b1 = .007, CI [.0003, .016], but CIs of the indirect effect of maternal invalidation on ED-15 total score through anxiety related to abandonment included zero, a2b2 = .005, CI [−.004, .014]. Thus, it is not likely a genuine indirect effect. The difference between the indirect effects was .002, but a 95% CI included zero (−.008 to .013). Therefore, the indirect effect of maternal invalidation on ED-15 total score through avoidance was no different than the indirect effect through anxiety. The total indirect effect of maternal invalidation through both mediators simultaneously was between −.001 and .026. Maternal invalidation was also not associated with the ED-15 total score after controlling for anxiety and avoidance in intimate relationships, c´ = .007, t = .605, p = .546. The model accounted for 19% of the variance in ED-15 total score.

Statistical diagram for the parallel multiple mediator model with both anxiety and avoidance in intimate relationships as potential mediators of the relationship between maternal invalidation and ED-15 total score. a1 = the coefficient of the X - > the mediator 1 (M1), a2 = the coefficient of the X - > the mediator 2 (M2), b1 = the coefficient of M1 - > Y, b2 = the coefficient of M2 - > Y, c´ = the direct effect of X on Y. All endogenous variables are associated with errors which, for the sake of simplicity, are not shown in this figure. *p < .05, **p < .01, ***p < .001
Discussion
This study aimed to evaluate the association between perceived invalidating childhood environments, attachment in intimate relationships during adulthood and eating psychopathology in a clinical sample of ED patients. Our particular interest, rather than focusing on a specific pattern of family relationships during early experiences, emerged from the relevance of considering the potential mechanisms through which some patterns in the family, in the individual and in the clinical symptomatology, may be inter-related and can be relevant in the explanation of current ED symptomatology. Paternal invalidation was related to the ED-15 total score through avoidance of proximity and anxiety over abandonment, while maternal invalidation was only related to the ED-15 total score through avoidance of proximity. In general, these results are in line with previous studies (e.g., Mountfort et al., 2007; Ford et al. 2010) that showed that invalidation environments were related to eating psychopathology, emotional difficulties and interpersonal difficulties, and to Linehan’s biosocial theory (1993) that postulates that growing up in invalidating families might predispose individuals to cope with negative emotional experiences via maladaptive behaviours such as eating-related symptomatology.
Providing more detail by looking at the severity and frequency of eating psychopathology in our sample, we also found that binge-eating episodes were associated with higher paternal and maternal emotional invalidation. High laxative misuse frequency was related with higher avoidance over intimacy and ECR total scores. Moreover, a higher eating restraint frequency was also associated with avoidance over intimacy and anxiety over abandonment. Previously, Arcelus et al. (2013) proposed a model of the interpersonal functioning in EDs suggesting that interpersonal difficulties in patients with restrictive and bulimic behaviours might be related to the avoidance in expressing feelings, distrust and negative interaction with others. Therefore, and according to our results, eating symptomatology may serve as an inadequate strategy to regulate emotions and to deal with difficulties in intimate relationships in the context of invalidating family environments. These results are in line with those found in a community sample of college women (Gonçalves et al. 2018), in which associations between perceived invalidating childhood experiences and greater body dissatisfaction and eating disordered behaviours were found to be mediated by avoidance over intimacy and abandonment-related anxiety.
In accordance with other studies (e.g., Gander et al. 2015; Jewell et al. 2016; Tasca et al. 2018), our results showed that higher eating psychopathology scores were associated with higher avoidance over intimacy, anxiety over abandonment and difficulties in the experience of intimate relationships in a clinical sample of patients with EDs. As Hartmann et al. (2010) already discussed, it seems that a more pronounced interpersonal pattern of intimate relationships might reflect a severer level of overall disturbance in ED patients.
More specifically our results highlight the role of father’s invalidation in the EDs spectrum. Thus, participants who perceived their fathers as invalidating presented higher eating psychopathology and difficulties in the experience of intimate relationships expressed by anxiety over abandonment and avoidance over intimacy. The perception of paternal invalidation during childhood and current ED symptomatology and severity were associated with and mediated by current difficulties in establishing intimate relationships characterized by higher avoidance over intimacy and anxiety over abandonment. Despite the small effects observed, these results are in line with previous research had showed the importance of paternal invalidation in ED patients. Mountford et al. (2007) already discussed that, in women with EDs, it appears that perceived paternal invalidation is a key factor in the explanation of childhood invalidation. Haslam et al. (2008) also found that patients with binge eating and vomiting scored higher on paternal invalidation. Moreover, when testing a mediation analysis, bootstrap confidence intervals are the better approach to inference (Hayes 2013). Thus, we mainly considered these intervals to confirm the possible mediating role. If future empirical research supports the potential mediator role of attachment in the association between invalidation during childhood and ED psychopathology, this would indicate the importance of including parental emotional invalidation, particularly paternal, as a target in early prevention and intervention efforts in EDs, as well as the individual internal working models.
Moreover, in our study, no differences between ED’s diagnosis and maternal and paternal invalidation, and between ED’s diagnosis and anxiety over abandonment and avoidance of intimacy were found. Our results are in agreement with those found by Tasca et al. (2018), since attachment anxiety and attachment avoidance independently predicted ED symptoms above-and-beyond differences between ED diagnoses. In addition, considering the fact that all the three major diagnoses of EDs were measured in the present study, we were also able to sustain a transdiagnostic perspective in agreement with previous reviews that concluded that types of attachment insecurity may not be inevitably related to specific ED diagnoses (cf., Tasca and Balfour 2014).
As expected, chaotic family was associated with avoidance and higher ECR total scores, typical family was associated with anxiety and, on the contrary, validating family was associated with lower levels of avoidance and difficulties in intimate relationships. These results are in line with previous studies (e.g., Ford et al. 2010) that showed that invalidation in childhood undermines emotional functioning and, more specifically, a chaotic family was related to interpersonal difficulties.
In sum, it seems that a childhood family environment, when perceived as invalidating, may be considered in the association with current ED symptomatology, if we also consider current difficulties in intimate relationships in the sense of dealing with the fear of abandonment and intimacy. In that sense, eating pathology may be understood as an inadequate strategy to regulate emotions such as fear of abandonment and anxiety. This relationship seems to emerge in the context of childhood paternal invalidation.
Our results extend the literature on our understanding on the role of invalidating environments in EDs and adult attachment. As Tasca and Balfour (2014) suggested, clinicians may consider assessing attachment insecurity through self-report questionnaires or interviews, since individuals with EDs and insecure attachment styles have differing affect regulation approaches and interpersonal styles that may affect their interactions with treatment providers and their behaviours in therapy. Additionally, and since insecure attachment in childhood seems to predict higher eating pathology (cf., Jewell et al. 2016), treatment programmes should promote emotion regulation strategies and interpersonal competencies as key intervention goals in EDs.
Our study has some limitations. The sample consisted predominantly of women recruited from a specialized clinical ED setting. Although men are being increasingly diagnosed (e.g., Micali et al. 2013; Mitchison and Mond 2015; Raevuori et al. 2014), they were under-represented in this study. This may limit the generalization of the present results to males. Future studies assessing a more diverse demographic sample may provide greater insight into the mechanisms underlying family invalidation, ED psychopathology and attachment in intimate relationships during adulthood. Additionally, the AN diagnose was overrepresented as the remaining diagnostic categories contained significantly fewer participants. In the future, efforts should be made to obtain more balanced sample sizes within each diagnostic group. Further limitations are related to the use of self-report measures. According to Tasca et al. (2018), these types of measures are only able to capture consciously available information with regard to attachment. Additionally, we must also consider that it is possible that ED psychopathology also increases the likelihood that a person would perceive others’ behaviours as emotionally invalidating. According to Ambwani et al. (2016), there may be disruptions in AN patient’s ability to detect and interpret warmth from others. Somehow, we may consider this potential impact when assessing childhood invalidation in ED patients and be moderated considering the results found by self-report measures. We must not forget that we evaluated childhood invalidating environment using only as basis the participant’s perception. Moreover, when a .05 level of significance is used, the chance of making a Type I error (the incorrect rejection of a true null hypothesis) is 5% for each statistical test. However, we used more than a single test. Across a group of tests, the probability of making a Type I error increases. On the other hand, a lower level is vulnerable to type II errors (the failure to reject a false null hypothesis), and typically, in psychology, an α-level of .05 is used, based on Fisher’s criterion (Field 2009). Thus, as in previous studies (e.g., Mountford et al. 2007), we used a .05 level of significance. Finally, present results must be interpreted with caution given the small indirect effects from the mediation analyses and the cross-sectional design of this study, which limits the inference on causality, for such, future studies should prospectively examine these variables. On the positive side, as far as our knowledge, this is the first study conducted with a large clinical sample of EDs, in which perceived invalidating childhood environments and attachment in intimate relationships during adulthood were combinedly explored.
Notes
We considered other parallel multiple mediation models with ED-15 total score as dependent variables, avoidance of proximity/anxiety related to abandonment as independent variables, and paternal and maternal invalidation as potential mediators. However, a condition for a parallel multiple mediation analysis is that no mediator causally influences another (Hayes 2013). In these cases, mediators (paternal and maternal invalidation) are correlated even after controlling for independent variables. Thus, it was not possible to test these mediation models.
References
Ambwani, S., Berenson, K. R., Simms, L., Li, A., Corfield, F., & Treasure, J. (2016). Seeing things differently: An experimental investigation of social cognition and interpersonal behavior in anorexia nervosa. International Journal of Eating Disorders, 49(5), 499–506. https://doi.org/10.1002/eat.22498.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington, DC: American Psychiatric Association.
Arcelus, J., Yates, A., & Whiteley, R. (2012). Romantic relationships, clinical and sub-clinical eating disorders: A review of the literature. Sexual and Relationship Therapy, 27(2), 147–161. https://doi.org/10.1080/14681994.2012.696095.
Arcelus, J., Haslam, M., Farrow, C., & Meyer, C. (2013). The role of interpersonal functioning in the maintenance of eating psychopathology: A systematic review and testable model. Clinical Psychology Review, 33(1), 156–167. https://doi.org/10.1016/j.cpr.2012.10.009.
Baron, R. M., & Kenny, D. A. (1986). The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology, 51, 1173–1182. https://doi.org/10.1037/0022-3514.51.6.1173.
Bowlby, J. (1969). Attachment and loss, Vol. 1: Attachment. New York: Basic Books.
Brennan, K. A., Clark, C. L., & Shaver, P. R. (1998). Self-report measurement of adult attachment: An integrative overview. In J. A. Simpson & W. S. Rholes (Eds.), Attachment theory and close relationships (pp. 46–76). New York: Guilford Press.
Broberg, A., Hjalmers, I., & Nevonen, L. (2001). Eating disorders, attachment and interpersonal difficulties: A comparison between 18- to 24-year-old patients and normal controls. European Eating Disorders Review, 9(6), 381–396. https://doi.org/10.1002/erv.421.
Evans, L., & Wertheim, E. (2005). Attachment styles in adult intimate relationships: Comparing women with bulimia nervosa symptoms, women with depression and women with no clinical symptoms. European Eating Disorders Review, 13(4), 285–293. https://doi.org/10.1002/erv.621.
Faber, A., Dubé, L., & Knäuper, B. (2018). Attachment and eating: A meta-analytic review of the relevance of attachment for unhealthy and healthy eating behaviors in the general population. Appetite, 123(1), 410–438. https://doi.org/10.1016/j.appet.2017.10.043.
Field, A. P. (2009). Discovering statistics using SPSS. London, England: SAGE.
Ford, G., Waller, G., & Mountford, V. (2010). Invalidating childhood environments and Core beliefs in women with eating disorders. European Eating Disorders Review, 19, 316–321. https://doi.org/10.1002/erv.1053.
Galmiche, M., Déchelotte, P., Lambert, G., & Tavolacci, M. P. (2019). Prevalence of eating disorders over the 2000–2018 period: A systematic literature review. The American Journal of Clinical Nutrition, 109(5), 1402–1413. https://doi.org/10.1093/ajcn/nqy342.
Gander, M., Sevecke, K., & Buchheim, A. (2015). Eating disorders in adolescence: Attachment issues from a developmental perspective. Frontiers in Psychology, 6, 1–12. https://doi.org/10.3389/fpsyg.2015.01136.
Gonçalves, S., Moreira, C., Gonçalves, M., Vieira, A. I., & Machado, B. (2018). The role of the perception of family environment in relation to body dissatisfaction, disordered eating and difficulties in close relationship. Eating and Weight Disorders – Studies on Anorexia, Bulimia and Obesity, 1–9. https://doi.org/10.1007/s40519-108-0551-9.
Gratz, K. L., & Roemer, L. (2004). Multidimensional assessment of emotion regulation and dysregulation. Journal of Psychopathology and Behavioral Assessment, 26(1), 41–54. https://doi.org/10.1023/B:JOBA.0000007455.08539.94.
Hartmann, A. S., Czaja, J., Rief, W., & Hilbert, A. (2010). Personality and psychopathology in children with and without loss of control over eating. Comprehensive Psychiatry, 51, 572–578. https://doi.org/10.1016/j.comppsych.2010.03.001.
Haslam, M., Mountford, V., Meyer, C., & Waller, G. (2008). Invalidating childhood environments in anorexia and bulimia nervosa. Eating Behaviours, 9, 313–318. https://doi.org/10.1016/j.eatbeh.2007.10.005.
Hayes, A. F. (2013). Introduction to mediation, moderation, and conditional process analysis. New York: The Guilford Press.
Haynos, A., & Fruzzetti, A. (2011). Anorexia nervosa as a disorder of emotion dysregulation: Evidence and treatment implications. Clinical Psychology: Science and Practice, 18(3), 183–202. https://doi.org/10.1111/j.1468-2850.2011.01250.x.
Hazan, C., & Shaver, P. (1987). Romantic love conceptualized as an attachment process. Journal of Personality and Social Psychology, 52(3), 511–524. https://doi.org/10.1037/0022-3514.52.3.511.
Jewell, T., Collyer, H., Gardner, T., Tchanturia, K., Simic, M., Fonagy, P., & Eisler, I. (2016). Attachment and mentalization and their association with child and adolescent eating pathology: A systematic review. International Journal of Eating Disorders, 49(4), 354–373. https://doi.org/10.1002/eat.22473.
Linehan, M. M. (1993). Cognitive-behavioral treatment of borderline personality disorder. New York: Guildford Press.
Micali, N., Hagberg, K. W., Petersen, I., & Treasure, J. L. (2013). The incidence of eating disorders in the UK in 2000–2009: findings from the General Practice Research Database. BMJ Open, 3–10. https://doi.org/10.1136/bmjopen-2013-002646.
Mikulincer, M., & Shaver, P. R. (2007). Attachment in adulthood: Structure, dynamics, and change. New York: Guilford Press.
Miller, R. S., & Perlman, D. (2007). Intimate relationships. Boston: McGraw-Hill Higher Education.
Mitchison, D., & Mond, J. (2015). Epidemiology of eating disorders, eating disordered behaviour, and body image disturbance in males: A narrative review. Journal of Eating Disorders, 3(20), 1–9. https://doi.org/10.1186/s40337-015-0058-y.
Mountford, V., Corstorphine, E., Tomlinson, S., & Waller, G. (2007). Development of a measure to assess invalidating childhood environments in the eating disorders. Eating Behaviours, 8, 48–58. https://doi.org/10.1016/j.eatbeh.2006.01.003.
Musser, N., Zalewski, M., Stepp, S., & Lewis, J. (2018). A systematic review of negative parenting practices predicting borderline personality disorder: Are we measuring biosocial theory’s “invalidating environment”? Clinical Psychology Review, 65, 1–16. https://doi.org/10.1016/j.cpr.2018.06.003.
Paiva, C., & Figueiredo, B. (2010). Validation of the “experiences in close relationships” – Portuguese version. Interpersona, 4(4), 237–270. https://doi.org/10.5964/ijpr.v4i2.51.
Raevuori, A., Keski-Rahkonen, A., & Hoek, H. (2014). A review of eating disorders in males. Current Opinion in Psychiatry, 27(6), 426–430. https://doi.org/10.1097/YCO.0000000000000113.
Rodrigues, T, Vaz, AR., Silva, C., Conceição, E., Machado, P. P. P. (2019). Eating disorder-15 (ED-15): Factor structure, psychometric properties, and clinical validation. European Eating Disorders Review, 1–10. https://doi.org/10.1002/erv.2694
Safer, D. L., Telch, C. F., & Agras, W. S. (2001a). Dialectical behavior therapy for bulimia nervosa: A case study. International Journal of Eating Disorders, 30, 101–106. https://doi.org/10.1002/eat.1059.
Safer, D. L., Telch, C. F., & Agras, W. S. (2001b). Dialectical behavior therapy for bulimia nervosa. American Journal of Psychiatry, 158, 632–634. https://doi.org/10.1176/appi.ajp.158.4.632.
Safer, D. L., Robinson, A. H., & Jo, B. (2010). Outcome from a randomized controlled trial of group therapy for binge eating disorder: Comparing dialectical behavior therapy adapted for binge eating to an active comparison group therapy. Behavior Therapy, 41(1), 106–120. https://doi.org/10.1016/j.beth.2009.01.006.
Schmidt, U., Adan, R., Böhm, I., Campbell, I. C., Dingemans, A., Ehrlich, S., Elzakkers, I., Favaro, A., Giel, K., Harrison, A., Himmerich, H., Hoek, H. W., Herpertz-Dahlmann, B., Kas, M. J., Seitz, J., Smeets, P., Sternheim, L., Tenconi, E., van Elburg, A., van Furth, E., & Zipfel, S. (2016). Eating disorders: The big issue. Lancet Psychiatry, 3(4), 313–315. https://doi.org/10.1016/S2215-0366(16)00081-X.
Tasca, G. A., & Balfour, L. (2014). Attachment and eating disorders: A review of current research. International Journal of Eating Disorders, 6, 1–12. https://doi.org/10.1002/eat.22302.
Tasca, G. A., Brugnera, A., Ba, D. B., Carlucci, S., Angelo, B. A., Louise, C., et al. (2018). Reliability and validity of the experiences in close relationships Scale-12: Attachment dimensions in a clinical sample with eating disorders. International Journal of Eating Disorders, 51, 18–27. https://doi.org/10.1002/eat.22807.
Tatham, M., Turner, H., Mountford, V., Tritt, A., Dyas, R., & Waller, G. (2015). Development, psychometric properties and preliminary clinical validation of a brief, session-by-session measure of eating disorder cognitions and behaviors: The ED-15. International Journal of Eating Disorders, 48, 1005–1015. https://doi.org/10.1002/eat.22430.
Vieira, A. I., Gonçalves, M., Machado, B. C., Rodrigues, T., Machado, P. P. P., Brandão, I., et al. (2018). Psychometric properties of the Portuguese version of the invalidating childhood environment scale. Eating and Weight Disorders - Studies on Anorexia, Bulimia and Obesity, 23, 1–9. https://doi.org/10.1007/s40519-018-0550-x.
Ward, A., Ramsay, R., & Treasure, J. (2000). Attachment research in eating disorders. British Journal of Medical Psychology, 73(1), 35–51.
Acknowledgments
This study was authorized and approved by the institutional review board committee of the São João Hospital Center (Number 188-17) and the Ethic Committee for Human and Social Sciences of the University of Minho (Number 006/2017).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Gonçalves, S., Vieira, A.I., Rodrigues, T. et al. Adult attachment in eating disorders mediates the association between perceived invalidating childhood environments and eating psychopathology. Curr Psychol 40, 5478–5488 (2021). https://doi.org/10.1007/s12144-019-00524-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12144-019-00524-2