
Abstract
Defensive Responding is a term to describe strategies used to control the perceptions others have of oneself. The attempt to control information in an effort to influences another’s opinion can serve as a personal or social goal-directed behavior. This behavior has implications for how others perceive, evaluate, and treat them. There is a wealth of research on parental characteristics that can influence responding about children, and there is literature showing that certain motives, goals, and personality characteristics, such as defensive responding, can affect caregiver’s self-report. However, research has yet to bridge these lines of research and examine whether defensive responding impacts parents’ responding about their children. The current study explored differences in responding between mothers who do and do not engage in defensive responding on a widely-used measure of child psychopathology: the Child-Behavior Checklist, while controlling for maternal psychopathology, child race, age, and gender. Results indicated that mothers who engaged in defensive responding responded more defensively about their children on the Total score of the Child-Behavior Checklist. Specifically, mothers reported reduced internalizing, anxiety/depression, withdrawal/depression, externalizing, inattention, delinquency, and aggression symptoms. Exploratory analyses indicated that the relationship between maternal depressive symptoms and child psychopathology was mediated by maternal defensive responding.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Defensive responding (DR) is a term used to describe strategies to control the perceptions others form (Leary and Kowalski 1990). The impressions people make of others have implications for how others perceive, evaluate, and treat them. Furthermore, others’ impressions can influence their own views of themselves. For instance, DR has been shown to mediate the relationship between emotion regulation and anxiety in a large sample of college students (Arndt et al. 2013), suggesting it may be a useful emotion regulation strategy. Research on DR has spanned many fields from marketing (McFarland et al. 2006), to romantic relationships (Howard et al. 1986; Pontari and Schlenker 2004), to politics (Schütz 1995). However, the focus of the current study is to explore whether maternal DR influences mother-reported child psychopathology.
Interest in DR began when Schlenker (1980, 1985), Jones and Pittman (1982), Hogan (1982), and Baumeister (1982, 1986) provided conceptual analysis of DR as a fundamental interpersonal process. Research has linked DR to psychotic symptoms (Braginsky et al. 1966), attitude change (Tedeschi et al. 1971), aggression (Tedeschi et al. 1974), self-serving attributions (Weary and Arkin 1981), social facilitations (Bond 1982), social anxiety (Schlenker and Leary 1982), self-handicapping (Kolditz and Arkin 1982), and the counseling process (Friedlander and Schwartz 1985). A recent article by Frühauf et al. (2015) explored DR as it pertains to an intake interview. They defined 12 DR tactics defined on theoretical conceptions of the therapeutic alliance and rated 60 videotaped intake interviews. DR influence was observed in roughly 30% of all patients, and they found patients could be classified as negative self-presenters, positive self-presenters, or response provokers. There have been a number of reviews of the literature (e.g., Baumeister 1982; Leary and Kowalski 1990; Schlenker 1980; Tedeschi 1981), however, a more recent review is needed.
DR has been part of the literature for nearly 60 years (e.g., Goffman 1959), yet the role DR has on a mother’s report of their child’s mental health has largely been ignored. Thus, background literature for this study has relied on studies exploring DR in reporting on their own symptoms. There has been a consistent link between parenting stress and DR (Copeland and Harbaugh 2005; MacCallum et al. 2007; McMahon et al. 2003). Overall, these studies specifically explored the effect DR has on maternal self-reporting; demonstrating that there are elevated levels of DR in families that have undergone a stressful event. Taken together with findings that suggest parenting a child with a mental illness increases maternal stress (Donenberg and Baker 1993), it follows that DR may play a role in maternally reported child psychopathology. DR has generally focused on self-reports with only two studies (described below) connecting DR to maternally reported child psychopathology.
All the research on DR to date has been conducted on self-perception in the adult population. However, applying DR to multi-informant child assessments has intuitive appeal. The assessment of child psychopathology has been known to require multi-informant data (Achenbach et al. 2005). However, reports from different informants have been shown to be only moderately correlated (Achenbach et al. 1987; De Los Reyes and Kazdin 2005;). Additionally, it is not uncommon for parent report methods to have low convergence with naturalistic observations and/or teacher reports (e.g., Seifer et al. 1994). Furthermore, Mesman and Koot (2000) found that they have weaker predictive validity for later psychological functioning than do teacher reports.
Low informant agreement among multiple informants regarding a wide range of child psychopathologies has long been a methodological challenge (see De Los Reyes and Kazdin 2005 for a review). There is a great deal of evidence that a wide range of parental characteristics influences responding. Specifically, maternal depression/anxiety, (Boyle and Pickles 1997; Chi and Hinshaw 2002; Gartstein et al. 2009; Najman et al. 2000; Richters 1992; Youngstrom et al. 1999) parental/family stress (Foley et al. 2005; Youngstrom et al. 2000), maternal alcoholism (Foley et al. 2005), marital discard (Christensen et al. 1992; Webster-Stratton and Hammond 1988), and low socioeconomic status (Duhig et al. 2000) have been linked to biased reporting. Additionally, a recent article by Müller and Furniss (2013) found that maternal reports of child psychopathology are influenced by general maternal psychopathology using structural equation modeling.
Many researchers have suggested various guidelines to clinicians and researchers to ameliorate the multi-informant discrepancy (Carlson and Youngstrom 2011; Smith 2016). For example, it has been suggested to use a combination of ratings to improve predictability and validity or decide which informant rating would be preferred in practice or research (e.g., Shemmassian and Lee 2012). Often times the preferred informant is the mother; thus, maternally reported child psychopathology has been heavily relied on in clinical practice and research.
However, the validity of maternal-reported child psychopathology outside of maternal psychopathology and stress, such has DR, has yet to be explored.
Of the variables that influence maternal responding, maternal depression/anxiety has the most robust support (Boyle and Pickles 1997; Chi and Hinshaw 2002; Gartstein et al. 2009; Najman et al. 2000; Richters 1992; Youngstrom et al. 1999). A recent meta-analytic review of 193 studies (Goodman et al. 2011) found a strong relationship between mothers’ depressive symptoms and their reporting of their children’s psychopathology. Maternal depression was related to higher levels of reporting of child internalizing, externalizing, and overall psychopathology. These associations were moderated by a number of demographic variables such as the child’s age and gender. Understandably, maternal DR was not inspected as a moderator or mediator of this relationship; however, given the link between maternal depressive symptoms and maternal DR, and association between maternal depressive symptoms and maternal report of child psychopathology, it is hypothesized that the relationship between maternal depressive symptoms and child psychopathology is mediated by maternal DR.
There is some research demonstrating a relationship between social desirability and mother reported parenting, such as level of self-efficacy (Lovejoy et al. 1997). Similarly, Marachi et al. (1999) examined mother social desirability and a number of mother-report, teacher-report, and observational measures of parenting and child behavioral problems. Although the focus of the study was not on social desirability (it was included as a covariate), the results indicated that mothers responded in a socially desirable manner when reporting their child’s externalizing behaviors and discipline style. These results continued to be significant even while controlling for the effects of maternal depression. Johnston et al. (2004) examined similar variables when exploring the validity of mothers’ reports of their parenting behavior and their child’s ADHD symptoms. Mothers’ DR significantly influenced their reports of over-reactive and lax parenting strategy on the Patenting Scale. However, controlling for DR did not alter the relationships between self-reported parenting and measures of maternal or child ADHD symptomology. These researchers did not explore how DR influenced the validity of maternally reported ADHD symptomology independent from parenting style.
There are several methodological issues with the literature relating DR (or social desirability) and mother-reported parenting style and child externalizing disorders. First, two of the three studies (i.e., Lovejoy et al. 1997; Marachi et al. 1999) were conducted with community samples. These samples had low levels of parenting problems and subsequently it may be inferred that they had reduced DR motives. Second, the measures used to assess DR or social desirability did not control for stress. The Marlowe-Crowne Social Desirability Scale (Lovejoy et al. 1997; Marachi et al. 1999) and the Balanced Inventory of Desirable Responding (Johnston et al. 2004) are frequently used and well-respected measures of social desirability and DR, but they do not control for maternal stress, a possible confound. Finally, Johnston et al. (2004) used a clinical sample, but explored a sample of mother-child dyads of children already diagnosed with ADHD, leaving it unlikely that DR would influence maternally reported ADHD symptomatology.
Current Study
Overall, the literature on maternal DR as related to child psychopathology is ambiguous and under-developed. The purpose of the current study was to explore the relationship DR has on maternally reported child psychopathology while controlling for important variables. More specifically, a group of mothers who did and did not engage in DR were compared on their reporting of psychopathology on one of the most widely used measures of child psychopathology: the Child-Behavior Checklist (CBCL; Achenbach and Rescorla 2001), while controlling for maternal psychopathology, child age, gender, and race. The decision to explore this relationship through a group analysis was made to increase the ecological validity of the current study. In practice, a clinician needs to make a decision on whether to categorize a client as engaging in DR, utilizing criteria outlined in the measure’s manual (e.g., <11; Abidin 1990). Therefore, the current study, using a group analysis, provides a clinician with information on the degree to which a mother may be under- or over-reporting of their child’s psychopathology, as well as any domain specificity (e.g., under-reporting of one psychopathological domain), if they meet criteria for engaging in DR. In addition, the decision to control for child age, gender and race was made due to previous literature linking differences in the assessment of child psychopathology based on these demographic factors (Twenge and Nolen-Hoeksema 2002). Moreover, age and race differences were examined between girls and boys in the current sample, and therefore, these effects were held constant throughout all analyses.
Although dimensional analyses would not allow for this translational information to be delineated, loss of information can occur with dichotomizing continuous variables (MacCallum et al. 2002); thus, the relationship between dimensional maternal DR and CBCL total score was determined utilizing a linear multiple regression, again controlling for maternal psychopathology, child age, gender, and race. Finally, given the robust literature linking maternal depressive symptoms specifically (Boyle and Pickles 1997; Chi and Hinshaw 2002; Gartstein et al. 2009; Goodman et al. 2011; Najman et al. 2000; Richters 1992; Youngstrom et al. 1999), an exploratory mediation analysis was conducted to determine whether maternal DR mediates the relationship between maternal depressive symptomatology and child psychopathology (i.e., total score of the CBCL), while controlling for child age, gender, and race.
Method
Participants
Participants included in the study were selected from a larger dataset of 387 participants who had previously sought services at an outpatient, community clinic. Participants completed several clinical and research measures, including the Parenting Stress Index/Short form (PSI/SF), Child Behavior Checklist (CBCL), and Symptom Checklist-90-Revised (SCL-90-R) (see measures section). From the dataset, 162 mothers and their children had completed all study-relevant measures and were therefore included in the study. Children and adolescents were between 6 and 16 years of age (M = 10.01, SD = 2.75), whereas mothers were between 25 to 71 years of age (M = 39.90, SD = 6.92). Children and adolescents were predominantly male (n = 94, 58%), with 84.6% of the entire sample identifying as White (Non-Hispanic), 10.5% identifying as Black, 2.5% identifying as Hispanic, 1.2% identifying as Asian, and 1.2% identifying as Mixed Race/Other. See Table 1. Males in the sample, specifically, were between 6 and 15 years of age (M = 9.73, SD = 2.67) and identified predominantly as White, Non-Hispanic (77.7%), with 16% identifying as Black, 4.3% identified as Hispanic, and 2.1% identified as Asian. Females in the sample were between 6 and 16 years of age (M = 10.38, SD = 2.83) and identified predominately as White, Non-Hispanic (n = 64; 94.1%), with 2.9% identifying as Black, and 2.9% Mixed Race/Other. Given these qualitative differences in demographic variables between boys and girls, all analyses were controlled for gender, age, and ethnicity.
Measures
The Parenting Stress Index/Short Form (PSI/SF; Abidin 1990) is a 36-item parent-report questionnaire assessing indicators of stress within the parent and child relationship. Endorsement patterns provide information on three scales: Parental Distress, Parent-Child Dysfunctional Interaction, and Difficult Child (Castaldi 1988; Hauenstein 1990). Overall, the PSI/SF has been found to have high internal consistency, convergent validity, and discriminate validity (Reitman et al. 2002; Whiteside-Mansell et al. 2007). The PSI/SF also provides a defensive responding scale that is based off of the Marlowe-Crowne Social Desirability Scale (Crowne and Marlowe 1960). This scale assists the clinician in determining whether parents are attempting to represent themselves more favorably and has demonstrated convergent validity (Castaldi 1988; LaFiosca and Loyd 1986). The defensive responding scale is indicated by low scores on seven items from the parental distress scale and indicates the degree to which parents may deny or minimize problems. The rate of defensive responding in the general population is estimated at 5 to 8% (Parkes et al. 2011). Test-retest and alpha reliabilities for the PSI/SF total score are .84 and .91, respectively (Abidin, 1995). Normative data were derived for each PSI scale from the raw score frequency distribution of scores (n = 800) from the mothers in the normative sample (Abidin 1990). The PSI/SF manual advises that scores greater than 11 on the defensive responding scale are clinically significant and responding may be biased in which the parent-child relationship is intended to provide a favorable impression. The Cronbach’s alpha of the PSI/SF in the current study was within the acceptable range (α = .75).
Child Behavior Checklist (CBCL; Achenbach and Rescorla 2001)
The CBCL is a 113-item parent-report screening measure for emotional and behavioral problems in children between the ages of 6 and 16 years of age. Computer scoring provides information on a Total Problems scale, indicating overall psychopathology, and on two broadband scales: Internalizing and Externalizing scales. For these scales, scores between the 84th and 90th percentile (i.e., T scores ranging between 60 and 63) are considered borderline significant, and scores above the 92nd percentile (i.e., T score of 64 or above) are considered clinically significant. Furthermore, endorsement patterns provide information on six DSM-oriented scales (Depressive Problems, Anxiety Problems, Somatic Problems, Attention Deficit/Hyperactivity Problems, Oppositional Defiant Problems, and Conduct Problems) and eight empirically derived syndrome scales (Anxious/Depressed, Withdrawn/Depressed, Somatic Complaints, Social Problems, Thought Problems, Attention problems, Rule-Breaking Behavior, and Aggressive Behavior). On these scales, scores between the 93rd and 97th percentile rank (i.e., T scores between 65 and 69) are within borderline significant range, whereas scores above the 98th percentile (i.e., T scores of 70 or above) are within the clinically significant range. The Cronbach’s alpha of the CBCL total score in the current study was within the acceptable range (α = .84).
The Symptoms Checklist-90-Revised (SCL-90-R)
The SCL-90-R (Derogatis 1994) is a 90-item adult self-report measure. The measure was administered to all mothers in the current sample. On a 5-point scale, ranging from “not at all” to “extremely”, mothers rated the severity of psychopathological symptoms they experienced over the past 7 days. Endorsement patterns provided information on the following scales: depression, obsessive-compulsive disorder, anxiety, phobias, psychoticism, interpersonal sensitivity, somatization, and paranoia. Reliability for this measure is high (Cronbach’s α: 0.75–0.91; Reuterskiöld et al. 2008). The Cronbach’s alpha of the SCL-90-R depression scale in the current study was within the good range (α = .86).
Procedure
Youth and their parent(s) presented at an outpatient, community clinic in a large, southern university for either a psychoeducational assessment or treatment (for treatment instruments were completed as part of the intake process prior to intervention). Children were referrals from community pediatricians, schools, mental health professionals, and self-referrals. Therapists were trained doctoral student clinicians practicing under the supervision of a licensed psychologist with more than 15 years experience. Families all agreed to let their de-identified data be used for research purposes. No specific inclusion criteria were used for assessment participation. Institutional Review Board approval, child assent, and parent consent were obtained prior to the start of their first session. Psychoeducational testing lasted for three, 2–3-h sessions.
Mother-child dyads were assigned to one of two groups based on maternal item endorsement on the PSI-SF. The clinically significant cut-off score for the defensing responding scale, used for the creation of groups, was < 11 (Abidin 1990). Dyads in which mother’s scores were significantly elevated on the defensive responding scale were assigned to the defensive group. Subsequently, dyads in which mother’s scores were not significantly elevated on the defensive responding scale were assigned to the nondefensive responding group. The defensive group consisted of 65 mother-child dyads and the nondefensive group consisted of 97 mother-child dyads.
Results
Statistical Approach
To determine the relationship between DR and maternally reported child psychopathology, while controlling for maternal psychopathology, child age, gender, and race, a single 2-way analysis of covariance (ANCOVA) was conducted. This decision was made to increase the ecological validity of the study; the results have the potential to provide a clinician with information on the degree to which a mother may be under- or over-reporting of their child’s psychopathology, as well as any domain specificity (e.g., under-reporting of one psychopathological domain), if they meet criteria for engaging in DR. However, given the loss of information that occurs with dichotomization of continuous variables (MacCallum et al. 2002), the relationship between dimensional maternal DR and CBCL total score was determined utilizing a linear multiple regression, again controlling for maternal psychopathology, child age, gender, and race. Our final mediational analysis was conducted utilizing a linear multiple regression because of the robust literature linking maternal depressive symptoms, specifically, child psychopathology (with child age, gender, and race as covariates).
Missing Data, Normality, and Descriptive Statistics
In each analysis, for participants administered the measures included in the study, there was very little missing data (<5% of the total samples). In addition, missing data was found to be missing at random (i.e., missing data was unrelated to the dependent variables in the analyses), and therefore deletion was list-wise for group analyses, given the statistical technique used, and pair-wise for dimensional analyses. Normality was examined through kurtosis and skewness values, as well as visual inspection of histograms. All variables were found to be approximately normally distributed, and therefore no transformations were applied (Tabachnick & Fidell, 2013). Means and standard deviations of all measured variables are presented in Table 2.
Group Analyses and Considerations
An ANCOVA was used to explore the differences between mothers’ reporting about their child’s psychopathology on a widely-used measure of child psychopathology (i.e., CBCL) depending on whether they engage in defensive responding (DR; n = 65) or do not (n = 97). Child’s age, race, gender, and maternal psychopathology were entered into the model as covariates. The effects of child’s age, race, and maternal psychopathology were not significant on any of the CBCL scales (all p > .05). Child’s gender had a significant effect on somatic symptoms (t(161) = 2.066, p < .05), but all other subscales were not significant (see Tables 3 and 4).
Box’s test of equality of covariance matrices proved significant (Box’s M = 131.48, F(45, 62,373.49) = 2.74, p < .001) suggesting unequal distribution of variance across the two groups. This is likely influenced by the unequal sample sizes in the current study. Therefore, Pillai’s Trace was used throughout all analyses (Tabachnick & Fidell 2013). Levene’s Test of Equality of Error Variances was violated for the Anxiety/Depression, F(1, 160) = 19.30, p < .001, Withdrawn, F(1, 160) = 29.53, p < .001, Delinquent, F(1, 160) = 15.95, p < .001, and Aggressive, F(1, 160) = 17.73, p < .001, subscales. Because of the large number of dependent variables, the consequent number of significance tests, and the increased likelihood of making a Type I error, a Bonferroni correction was applied. Nine subscales were examined, therefore, only results significant at the p < .0055 were reported (i.e., .05/9).
A single 2-way MANCOVA was used to explore the differences between mothers’ reporting on the CBCL depending on whether they engaged in DR (n = 60) or did not (n = 84). The dependent variables were the CBCL total score and subscales. Child’s age, race, gender, and maternal psychopathology were entered into the model as covariates. Among all CBCL subscales, the groups (i.e., DR versus control) demonstrated a statistically significant difference, F (9, 148) = 2.76, p < .001; Pillai’s Trace = .144, partial η2 = .14. Differences in reporting between the group of mothers’ that engage in DR and control mothers was explored for each subscale of the CBCL. The total score on the CBCL significantly differed between groups, t (1, 156) = 19.41, p < .0001, partial η2 = .11 (see Table 3). The mean Total score was 59.59 (SD = 1.0) for the nondefensive group and 53.47 (SD = 1.2) for the DR group, suggesting that mothers who engaged in DR were more likely to report that their children had fewer symptoms than the nondefensive group. The remaining subscale mean differences between groups show the same directionality and similar magnitudes (see Table 2).
There was a significant difference between mothers who engage in DR and the nondefensive group on how they reported their child’s internalizing, t (1, 156) = 13.75, p < .001, partial η2 = .08, anxiety/depression, t (1, 156) = 13.62, p < .001, partial η2 = .08, withdrawal, t (1, 156) = 13.90, p < .001, partial η2 = .08, externalizing t (1, 156) = 17.56, p < .0001, partial η2 = .10, inattention, t (1, 156) = 9.02, p < .01, partial η2 = .06, delinquency, t (1, 156) = 10.47, p < .01, partial η2 = .06, and aggression, t (1, 156) = 13.09, p < .001, partial η2 = .08, symptoms (see Tables 3 and 4).
Dimensional Analysis
All variables were mean-centered and included as continuous variables. A linear multiple regression was conducted predicting mother reported child psychopathology (i.e., CBCL total score), with maternal DR as the primary predictor in step two. Child age, gender, race, ethnicity, and mother psychopathology were included as covariates within step one. In the model, the first step, including only covariates, was not significant, F(4, 157) = .48, p > .05. The second step that introduces maternal DR into the model was significant, F(4, 157) = 9.46, p < .001, Adjusted R2 = .17. Within the second step, only maternal DR significantly contributed to the model (β = .45, t(161) = 6.01, p < .0001) in significantly predicting child psychopathology.
Exploratory Mediation Analysis
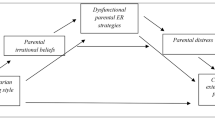
A mediation model was examined with dimensional maternal DR as a potential mediator of the relationship between dimensional maternal depressive symptoms and child psychopathology (i.e., CBCL total score). Analyses were done a linear multiple regression where the first step included relevant covariates (i.e., child age, gender, race, and ethnicity), the second step includes maternal depressive symptoms, and the final, third step, includes maternal DR. In this model (see Fig. 1), covariates within step one were not significant (p’s > .05). Within step two, increased depressive symptoms predicted more child psychopathology (B = .26, p < .001; F (3, 135) = 3.74, p < .001, R2 = .06), and maternal DR (B = .31, p < .001). The addition of maternal DR significantly predicted less child psychopathology in step three (B = −.34, p < .0001; F (4, 134) = 7.21, p < .001, R2 = .15). With the addition of maternal DR, maternal depressive symptoms no longer predicted child psychopathology (B = .15, p > .05), with a large indirect effect (Z = 2.73, p < .01).

Mediation analysis: maternal defensive responding mediates the relationship between maternal depressive symptoms and child psychopathology, while controlling for child age, gender, race and ethnicity. p < .01 = *
Discussion
We hypothesized that mothers who have a defensive manner of responding (i.e., engage in defensive responding) would significantly underreport their child’s psychopathology, despite seeking mental health services for their child. The current results provided support for our hypothesis on one of the most common measures of childhood psychopathology, the Child-Behavior Checklist. On average, results showed discrepancies on the CBCL between mothers who engage in defensive responding (DR) and a nondefensive group who did not, where mothers in the DR group reported significantly lower CBCL total score and internalizing, anxiety/depression, withdrawal, externalizing, and aggression symptom subscale scores. Since children are often seen as unreliable reporters, even of their own symptomatology, there is heavy reliance upon parents, particularly mothers, to serve as key informants in psychological assessment. A wealth of past research has shown parents are often influenced by their own symptomatology (e.g., major depression disorder) as well as external factors (e.g., family stressors); nevertheless, parents are still one of the primary informants for childhood psychopathology. Therefore, mothers’ DR can potentially exclude these children from receiving accommodations or services at a critical point in their development. If not treated, childhood psychopathology can result in significant impairment, persist into adulthood, and increase a child’s risk of developing substance use disorders later in life (Kendall and Kessler 2002). Furthermore, untreated mental disorders in youth are predictors of school failure (Kessler et al. 1995), teen childbearing (Kessler et al. 1997), adult relationship violence (Kessler et al. 2001), early marriage and divorce (Kessler et al. 1998), and adult economic instability (Ettner et al. 1997). Thus, early detection and treatment of child psychopathology is vital.
In order to control for the past research showing parental psychopathology may influence response patterns on their child’s assessments, analyses were conducted using the SCL-90-R and showed no significant difference on all CBCL scales, (all p > .05). These results serve as a primary indication that a parent’s report of their child’s symptomology may be less influenced by their own psychopathology as previously believed and the differences in reporting may in fact be due to a parent’s defensive responding. Conversely, it may be that the total SCL-90-R score used as a covariate was too general and a more specific maternal psychopathology measure (e.g., depression subscale) would have demonstrated significant differences. Support for this comes from the significant mediation model, where maternal depressive symptoms were significantly related to maternal-reported child psychopathology, though fully mediated by maternal DR.
As well, research studies of child psychopathology and their treatment require strict inclusion guidelines which may exclude certain children from analysis and therefore introduce a potentially confounding variable into studies of childhood psychopathology. The CBCL is one of the most widely used measure of child symptomatology; with dimensions that "correspond to current conceptualizations of child symptomatology," (Achenbach, 1991; pg. 695) embodied in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5; 5th ed., American Psychiatric Association, 2013). Therefore, the identification of the role DR has on the possibility of underreporting on the CBCL has important research and clinical implications. Given evidence based assessment is crucial to psychological interventions, finding evidence of this finding should inform future researchers and clinicians of the dangers of weighing parental ratings too highly. Moreover, this research has the potential to aid clinicians in understanding the degree of under-reporting of maternal-reported child psychopathology if a mother meets the cuff-off score for engaging in DR.
While this study was able to identify the presence of a subset of parents engaging in DR, information on the motivations behind this response style are unknown. Although it may be hypothesized that the DR group is underreporting their children’s psychopathology it is possible that an unknown third variable is involved. Moreover, this third variable may provide evidence that the significantly lower scores reported by mothers’ who engage in DR were accurate reports of their child’s psychopathology. However, given the effects’ ubiquity across subscales and previous research on DR, it is likely that mothers who engage in DR are underreporting their children’s psychopathology. This interpretation of the results is corroborated by the mediation analysis; maternal depressive symptoms was significantly related to mother-reported child psychopathology (i.e., total score of the CBCL); however, when maternal DR was fully mediated this relationship. Overall, this suggests that the third variable involved is the role maternal depressive symptoms has on increasing their use of DR, possibly as an emotion regulation technique (e.g., Arndt et al. 2013).
Previous research examining the influence of motivators for inaccurate responding have found greater discrepancies when there was a potential for significant gain (Rogers et al. 1996). For instance, adults have an increased probability of inaccurate response patterns when seeking forensic evaluations or when they are attempting to gain access to specific medications. In contrast, the current sample was seen at an outpatient mental health facility, where the parental responders mostly self-referred their children for evaluation, which would presume a desire for accurate assessment of their child’s psychopathology. Thus, the current findings may seem counterintuitive; mothers’ who are seeking treatment for their children are underreporting their children’s psychopathology.
Additionally, by utilizing a broad measure of child psychopathology, this study was able to analyze the differences between both internalizing and externalizing disorders. Statistically significant differences, after a conservative Bonferroni correction, between the groups were found for the total score and nearly all subscales, with the exception of Somatic Symptoms (p = .053). An examination of the means indicated mothers’ who engage in DR reported total scores that were over seven points lower than mothers who did not have that style of responding. The pervasive nature of this effect was unexpected given some behaviors having higher visibility (e.g., externalizing symptomology). Overall, results confirmed the hypothesis that a subset of parents engaged in a response style that would serve to minimize their child’s dysfunction. Future research should examine the potential motivations behind parents’ desire to respond in a defensive manner. Our mediation analysis suggests that specifically exploring the role of maternal depressive symptoms may be fruitful, though more research is clearly needed. External motivations seem minimal in this setting, so future study should focus on whether the responders are engaging in self-deception in an attempt to convince themselves that the problems are less severe or interfering. It is possible that social stereotypes that place the blame for childhood psychopathology on the parent may be one motivator to engage in defensive responding (i.e., stigma).
The current study, however, does have a number of limitations that should be addressed. First, the sample sizes of our groups (n = 65 and 97) were relatively small and came from a larger clinical sample. Second, our sample was racially homogenous; including mostly Caucasian children and parents. Additionally, the cross-sectional methodology does not allow for inferences to be made regarding temporal precedence. Finally, DR was measured only in mothers, thus not providing any information on the effect DR has on father reported child psychopathology. Even so, the reliance on maternally reported child psychopathology in the field of clinical psychology highlights the importance of future research on this relationship. Overall, the present study is the first of its kind to demonstrate that mothers’ reporting of their children’s psychopathology may be confounded by a defensive response style, despite referring their children for psychological services. Mothers’ who engage in DR reported significantly less symptomatology in their children suggesting that this may be an important variable to consider when interpreting mother-reported symptomatology in children.
References
Abidin, R. R. (1990). Parenting stress index (PSI). Atlanta: Pediatric Psychology Press.
Abidin, R. R. (1995). Manual for the parenting stress index. Odessa: Psychological Assessment Resources.
Achenbach, T. M. (1991). Integrative guide for the 1991 CBCL/4-18, YSR, and TRF profiles. Burlington: Department of Psychiatry, University of Vermont.
Achenbach, T., & Rescorla, L. (2001). The manual for the ASEBA school age forms & profiles. Burlington: University of Vermont, Research Center for Children, Youth, and Families.
Achenbach, T.M., Krukowski, R.A., Dumenci, L., & Ivanova, M.Y. (2005). Assessment of adult psychopathology: Meta-analyses and implications of cross-informant correlations. Psychological Bulletin, 131, 361-382.
Achenbach, T. M., McConaughy, S. H., & Howell, C. T. (1987). Child/adolescent behavioral and emotional problems: Implications of cross-informant correlations for situational specificity. Psychological Bulletin, 101(2), 213–232.
Arndt, J. E., Hoglund, W. L., & Fujiwara, E. (2013). Desirable responding mediates the relationship between emotion regulation and anxiety. Personality and Individual Differences, 55(2), 147–151.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (DSM-5®). Washington: American Psychiatric Publications.
Baumeister, R. F. (1982). A self-presentational view of social phenomena. Psychological Bulletin, 91, 3–26.
Baumeister, R. F. (Ed.). (1986). Public self and private self. New York: Springer.
Bond, C. F. (1982). Social facilitation: A self-presentational view. Journal of Personality and Social Psychology, 42, 1042–1050.
Boyle, M. H., & Pickles, A. R. (1997). Influence of maternal depressive symptoms on ratings of childhood behavior. Journal of Abnormal Child Psychology, 25(5), 399–412.
Braginsky, B. M., Grosse, M., & Ring, K. (1966). Controlling outcomes through impression-management: An experimental study of the manipulative tactics of mental patients. Journal of Consulting Psychology, 30, 295–300.
Carlson, G. A., & Youngstrom, E. A. (2011). Two opinions about one child—what's the clinician to do? Journal of Child and Adolescent Psychopharmacology, 21, 385–387.
Castaldi, J. (1988). The relationship of maternal defensiveness to reported levels of parenting stress (Doctoral dissertation).
Chi, T. C., & Hinshaw, S. P. (2002). Mother–child relationships of children with ADHD: The role of maternal depressive symptoms and depression-related distortions. Journal of Abnormal Child Psychology, 30(4), 387–400.
Christensen, A., Margolin, G., & Sullaway, M. (1992). Interparental agreement on child behavior problems. Psychological Assessment, 4(4), 419–425.
Copeland, D., & Harbaugh, B. L. (2005). Differences in parenting stress between married and single first time mothers at six to eight weeks after birth. Issues in Comprehensive Pediatric Nursing, 28(3), 139–152.
Crowne, D. P., & Marlowe, D. (1960). A new scale of social desirability independent of psychopathology. Journal of Consulting Psychology, 24(4), 349–354.
De Los Reyes, A., & Kazdin, A. E. (2005). Informant discrepancies in the assessment of childhood psychopathology: A critical review, theoretical framework, and recommendations for further study. Psychological Bulletin, 131(4), 483–509.
Derogatis, L. R. (1994). Symptom Checklist-90-R: Administration, scoring, and procedures manual. Minneapolis: National Computer Systems Inc.
Donenberg, G., & Baker, B. L. (1993). The impact of young children with externalizing behaviors on their families. Journal of Abnormal Child Psychology, 21(2), 179–198.
Duhig, A. M., Renk, K., Epstein, M. K., & Phares, V. (2000). Interparental agreement on internalizing, externalizing, and total behavior problems: A meta-analysis. Clinical Psychology: Science and Practice, 7(4), 435–453.
Ettner, S. L., Frank, R. G., & Kessler, R. C. (1997). The impact of psychiatric disorders on labor market outcomes. Industrial and Labor Relations Review, 51, 64–81.
Foley, D. L., Rutter, M., Angold, A., Pickles, A., Maes, H. M., Silberg, J. L., & Eaves, L. J. (2005). Making sense of informant disagreement for overanxious disorder. Journal of Anxiety Disorders, 19(2), 193–210.
Friedlander, M. L., & Schwartz, G. S. (1985). Toward a theory of strategic self-presentation in counseling and psychotherapy. Journal of Counseling Psychology, 32(4), 483–501.
Frühauf, S., Figlioli, P., Oehler, D., & Caspar, F. (2015). What to expect in the intake interview? Impression management tactics of psychotherapy patients. Journal of Social and Clinical Psychology, 34(1), 28–49.
Gartstein, M. A., Bridgett, D. J., Dishion, T. J., & Kaufman, N. K. (2009). Depressed mood and maternal report of child behavior problems: Another look at the depression–distortion hypothesis. Journal of Applied Developmental Psychology, 30, 149–160.
Goffman, E. (1959). The presentation of self in everyday life. New York: Doubleday and Company.
Goodman, S. H., Rouse, M. H., Connell, A. M., Broth, M. R., Hall, C. M., & Heyward, D. (2011). Maternal depression and child psychopathology: A meta-analytic review. Clinical Child and Family Psychology Review, 14(1), 1–27.
Hauenstein, E. J. (1990). The experience of distress in parents of chronically ill children: Potential or likely outcome? Journal of Clinical Child Psychology, 19(4), 356–364.
Hogan, R. (1982). A socioanalytic theory of personality. In M. Page (Ed.), Nebraska symposium on motivation (pp. 55–89). Lincoln: University of Nebraska Press.
Howard, J. A., Blumstein, P., & Schwartz, P. (1986). Sex, power, and influence tactics in intimate relationships. Journal of Personality and Social Psychology, 51(1), 102–109.
Johnston, C., Scoular, D. J., & Ohan, J. L. (2004). Mothers' reports of parenting in families of children with symptoms of attention-deficit/hyperactivity disorder: Relations to impression management. Child & Family Behavior Therapy, 26(1), 45–61.
Jones, E. E., & Pittman, T. S. (1982). Toward a general theory of strategic self-presentation. Psychological Perspectives on the Self, 1, 231–262.
Kendall, P. C., & Kessler, R. C. (2002). The impact of childhood psychopathology interventions on subsequent substance abuse: Policy implications, comments, and recommendations. Journal of Consulting and Clinical Psychology, 70(6), 1303–1306.
Kessler, R. C., Foster, C. L., Saunders, W. B., & Stang, P. E. (1995). Social consequences of psychiatric disorders: I. Educational attainment. American Journal of Psychiatry, 152, 1026–1032.
Kessler, R. C., Berglund, P. A., Foster, C. L., Saunders, W. B., Stang, P. E., & Walters, E. E. (1997). Social consequences of psychiatric disorders: II. Teenage parenthood. American Journal of Psychiatry, 154, 1405–1411.
Kessler, R. C., Walters, E. E., & Forthofer, M. S. (1998). The social consequences of psychiatric disorders: III. Probability of marital stability. American Journal of Psychiatry, 155, 1092–1096.
Kessler, R. C., Monar, B., Feurer, I. D., & Applebaum, M. (2001). Patterns and mental health predictors of domestic violence in the United States: Results from the National Comorbidity Society. International Journal of Law and Psychiatry, 24, 487–508.
Kolditz, T. A., & Arkin, R. M. (1982). An impression management interpretation of the self-handicapping strategy. Journal of Personality and Social Psychology, 43(3), 492–502.
LaFiosca, T., & Loyd, B. H. (1986). Defensiveness and the assessment of parental stress and anxiety. Journal of Clinical Child Psychology, 15(3), 254–259.
Leary, M. R., & Kowalski, R. M. (1990). Impression management: A literature review and two-component model. Psychological Bulletin, 107(1), 34–47.
Lovejoy, M. C., Verda, M. R., & Hays, C. E. (1997). Convergent and discriminant validity of measures of parenting efficacy and control. Journal of Clinical Child Psychology, 26(4), 366–376.
MacCallum, R. C., Zhang, S., Preacher, K. J., & Rucker, D. D. (2002). On the practice of dichotomization of quantitative variables. Psychological Methods, 7(1), 19–40.
MacCallum, F., Golombok, S., & Brinsden, P. (2007). Parenting and child development in families with a child conceived through embryo donation. Journal of Family Psychology, 21(2), 278–287.
Marachi, R., McMahon, R. J., Spieker, S. J., & Munson, J. A. (1999). Longitudinal assessment of the low-end specificity of maternal reports of depressive symptoms. Behaviour Research and Therapy, 37(5), 483–501.
McFarland, R. G., Challagalla, G. N., & Shervani, T. A. (2006). Influence tactics for effective adaptive selling. Journal of Marketing, 70(4), 103–117.
McMahon, C. A., Gibson, F., Leslie, G., Cohen, J., & Tennant, C. (2003). Parents of 5-year-old in vitro fertilization children: Psychological adjustment, parenting stress and the influence of subsequent in vitro fertilization treatment. Journal of Family Psychology, 17(3), 361–369.
Mesman, J., & Koot, H. M. (2000). Child-reported depression and anxiety in preadolescence: I. Associations with parent-and teacher-reported problems. Journal of the American Academy of Child & Adolescent Psychiatry, 39(11), 1371–1378.
Müller, J. M., & Furniss, T. (2013). Correction of distortions in distressed mothers' ratings of their preschool children's psychopathology. Psychiatry Research, 210(1), 294–301.
Najman, J. M., Williams, G. M., Nikles, J., Spence, S. H., Bor, W., O'Callaghan, M., et al. (2000). Mothers' mental illness and child behavior problems: Cause-effect association or observation bias. Journal of the American Academy of Child and Adolescent Psychiatry, 39(5), 592–602.
Parkes, J., Caravale, B., Marcelli, M., Franco, F., & Colver, A. (2011). Parenting stress and children with cerebral palsy: A European cross-sectional survey. Developmental Medicine and Child Neurology, 53(9), 815–821.
Pontari, B. A., & Schlenker, B. R. (2004). Providing and withholding impression management support for romantic partners: Gender of the audience matters. Journal of Experimental Social Psychology, 40(1), 41–51.
Reitman, D., Currier, R. O., & Stickle, T. R. (2002). A critical evaluation of the parenting stress index-short form (PSI-SF) in a head start population. Journal of Clinical Child and Adolescent Psychology, 31(3), 384–392.
Reuterskiöld, L., Öst, L. G., & Ollendick, T. (2008). Exploring child and parent factors in the diagnostic agreement on the anxiety disorders interview schedule. Journal of Psychopathology and Behavioral Assessment, 30(4), 279–290.
Richters, J. E. (1992). Depressed mothers as informants about their children: A critical review of the evidence for distortion. Psychological Bulletin, 112, 485–499.
Rogers, R., Sewell, K. W., Morey, L. C., & Ulstad, K. L. (1996). Detection of feigned mental disorders on the personality assessment inventory: A discriminant analysis. Journal of Personality Assessment, 67(3), 629–640.
Schlenker, B. R. (1980). Impression management: The self-concept, social identity, and interpersonal relations. Monterey: Brooks/Cole.
Schlenker, B. R. (1985). Identity and self-identification. In B. R. Schlenker (Ed.), The self and social life (pp. 65–99). New York: McGraw-Hill.
Schlenker, B. R., & Leary, M. R. (1982). Social anxiety and self-presentation: A conceptualization model. Psychological Bulletin, 92(3), 641–669.
Schütz, A. (1995). Entertainers, experts, or public servants? Politicians' self-presentation on television talk shows. Political Communication, 12(2), 211–221.
Seifer, R., Sameroff, A. J., Barrett, L. C., & Krafchuk, E. (1994). Infant temperament measured by multiple observations and mother report. Child Development, 65(5), 1478–1490.
Shemmassian, S. K., & Lee, S. S. (2012). Comparing four methods of integrating parent and teacher symptom ratings of attention-deficit/hyperactivity disorder (ADHD). Journal of Psychopathology and Behavioral Assessment, 34(1), 1–10.
Smith SR (2016) Making Sense of Multiple Informants in Child and Adolescent Psychopathology. Journal of Psychoeducational Assessment 25(2):139–149
Tabachnick, L. B. G. Fidell S. (2013). Using Multivariate Statistics (Sixth Ed.) Pearson.
Tedeschi, J. T. (Ed.). (1981). Impression management theory and social psychological research. New York: Academic Press.
Tedeschi, J. T., Schlenker, B. R., & Bonoma, T. V. (1971). Cognitive dissonance: Private ratiocination or public spectacle? American Psychologist, 26(8), 685–695.
Tedeschi, J. T., Smith, R. B., & Brown, R. C. (1974). A reinterpretation of research on aggression. Psychological Bulletin, 81(9), 540–562.
Twenge, J. M., & Nolen-Hoeksema, S. (2002). Age, gender, race, socioeconomic status, and birth cohort differences on the children's depression inventory: A meta-analysis. Journal of Abnormal Psychology, 111(4), 578–588.
Weary, G., & Arkin, R. M. (1981). Attributional self-presentation. New Directions in Attribution Research, 3, 223–246.
Webster-Stratton, C., & Hammond, M. (1988). Maternal depression and its relationship to life stress, perceptions of child behavior problems, parenting behaviors, and child conduct problems. Journal of Abnormal Child Psychology, 16(3), 299–315.
Whiteside-Mansell, L., Ayoub, C., McKelvey, L., Faldowski, R. A., Hart, A., & Shears, J. (2007). Parenting stress of low-income parents of toddlers and preschoolers: Psychometric properties of a short form of the parenting stress index. Parenting: Science and Practice, 7(1), 26–56.
Youngstrom, E., Izard, C., & Ackerman, B. (1999). Dysphoria-related bias in maternal ratings of children. Journal of Consulting and Clinical Psychology, 67(6), 905.
Youngstrom, E., Loeber, R., & Stouthamer-Loeber, M. (2000). Patterns and correlates of agreement between parent, teacher, and male adolescent ratings of externalizing and internalizing problems. Journal of Consulting and Clinical Psychology, 68(6), 1038–1050.
Funding
There is no funding to report.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Conflict of Interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Rights and permissions
About this article

Cite this article
Castagna, P.J., Lilly, M.E. & Davis, T.E. Maternal reporting of child psychopathology: The effect of defensive responding. Curr Psychol 39, 315–324 (2020). https://doi.org/10.1007/s12144-017-9765-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12144-017-9765-7