
Abstract
The purpose of this research was to examine reports of and pathways to posttraumatic growth (PTG) by emerging adults who have experienced trauma during adolescence compared with a comparison group recruited from the same sample frame. The sample consisted of 546 college students; 359 reported having experienced a traumatic event during adolescence, and 187 college students reporting no such trauma made up the comparison group. Independent t-tests revealed that the comparison group reported more growth in the domain of new possibilities; whereas, the trauma group reported more growth in the domains of spiritual change and appreciation for life. Structural equation modelling revealed no differences in factor loadings or path regression weights between the groups, suggesting that there was consistency in the influence that attachment, social support, and coping had on reports of PTG. However, constraining the intercepts did result in a poorer model fit; specifically, scores of growth in new possibilities and engagement in intrapersonal coping strategies (active, positive reframing, planning) were higher for the comparison group. Because these coping strategies also had the strongest path coefficient to PTG across groups, engagement in intrapersonal coping strategies appears to be a pathway to realizing growth, which is more likely to be experienced by college students but less likely to be achieved by emerging adults of adolescent trauma.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Posttraumatic growth (PTG) does not represent a single dimension of growth but can be realized in one or more of five domains: relating to others, new possibilities, personal strength, spiritual growth, and appreciation for life (Tedeschi and Calhoun 1996). Several groups of researchers (e.g., Park 2009; Tedeschi and Calhoun 1996, 2004) outline the base theoretical model of PTG as starting with exposure to a traumatic event, which must be accompanied by or followed with a perceived threat of significant loss, physical impairment, or death. According to this approach, it is this perceived threat related to the trauma that is the trigger required for PTG to develop. In response to these threats, individuals often modify personal belief systems in order to accommodate the meaning of the trauma into new or restructured personal views of and assumptions about life and the world. However, as described later, the development and modifications of personal worldviews are also part of adolescent and emerging adult development, and these developmental processes can confound results and lead to problematic interpretations of findings when investigating PTG in adolescents and emerging adults.
Factors Related to Posttraumatic Growth
Two of the more commonly cited psychosocial factors found to be associated with PTG are coping (e.g., Bellizzi and Blank 2006) and social support (e.g., Park et al. 1996). The coping strategies most commonly associated with reports of growth are positive reappraisal (e.g., Morris et al. 2007; Schmidt et al. 2012) and use of support coping (e.g., Swickert and Hittner 2009; Thornton and Perez 2006). In a meta-analysis on factors contributing to PTG, reappraisal coping (r = .36) and support coping (r = .25) had small to moderate effect sizes (Prati and Pietrantoni 2009). Some researchers (e.g., Bellizzi and Blank 2006; Park et al. 2008) have found similar effects using composite measures of adaptive or positive coping strategies. In addition to the use of social support as a coping strategy, perceived availability and satisfaction with social support have been identified as positively related to reports of PTG (e.g., Cadell et al. 2003; Park et al. 1996). In their meta-analysis, Prati and Pietrantoni (2009) combined various types of support (received, availability, satisfaction) and included multiple dimensions of support (e.g., emotional, instrumental), and they found an overall small but positive effect size of the association between support and PTG (r = .26).
Attachment style is another potentially important factor to consider. Literature on attachment style and coping strategies in adults indicates that attachment style can dictate the development and use of appropriate coping strategies for individuals who are dealing with stressful or traumatic events (Mikulincer and Florian 1995; Ognibene and Collins 1998). This body of research has further shown that secure attachment style is often associated with the use of more positive reframing and acceptance coping strategies; whereas, insecure attachment style is often associated with the use of avoidant coping strategies such as substance use and disengagement. Also, in several studies of adjustment to stressful events, securely attached adults sought more social support as a way of coping; however, insecurely attached adults either tended to not seek out support or engaged in avoidant coping strategies (Mikulincer and Florian 1995; Ognibene and Collins 1998). The research on attachment and PTG further suggests a positive relationship between secure attachment and PTG (Salo et al. 2005; Schmidt et al. 2012).
There has been relatively little research on PTG with survivors of traumas experienced during adolescence and emerging adulthood. Events experienced during adolescence will likely have lasting effects into emerging adulthood, which has been defined as a transition stage of the life course (typically 18–25 years) during which people explore options available to them as they transition from late adolescence (being dependent) to young adulthood (being independent) (Arnett 2000; Gottlieb et al. 2007). Thus, factors that influence how adolescents and emerging adults respond to traumatic events and the psychological outcomes related to the trauma exposure during these early life stages are likely to differ compared with exposure to traumatic events during adulthood. Accordingly, expanded research is needed on PTG and its correlates with people who have been exposed to traumatic events during adolescence to better understand how emerging adults adjust to traumatic events and what factors are associated with these responses.
Life Transitions as Sources of Growth
Researchers (Aldwin and Levenson 2004; Anderson and Lopez-Baez 2008, 2011; Gottlieb et al. 2007) have shown that growth is also likely to result from other experiences not normally considered to be traumatic but, instead, regarded as positive events (e.g., college entrance and graduation, marriage, becoming a parent). Tedeschi and Calhoun (2004), too, acknowledge that growth can be realized through other maturational processes, including college and other positive experiences, especially when these experiences are transformative enough to impact worldviews and personal schemas.
Particularly relevant to the current study, worldviews are likely to vary and fluctuate as cognitive development continues into the early- to mid-twenties. This is especially true for college students who are regularly exposed to new perspectives and theories as part of their education. Thus, there is a confounding factor influencing reports of posttraumatic growth with younger adult populations in that worldviews are typically fluid during this life stage but are also often modifiable in response to traumatic or life transition events. In fact, Gottlieb et al. (2007) found that reports of growth by college students exceeded reports of decline, and the majority of changes were triggered by events related to the transition to college life and were not necessarily traumatic in nature. Moreover, growth in the PTG domains of relating to others, new possibilities, and personal strength was experienced by the majority of participants. However, the differences in levels of specific types of growth reported between trauma and comparison groups have not been reported in the scientific literature.
If there are aspects of growth that are uniquely reported by trauma survivors, then understanding how these types of growth differ from growth commonly associated with expected developmental tasks and life transitions may result in a deeper and more comprehensive understanding of PTG, which can inform clinical approaches to working with adolescent and emerging adult survivors of trauma.
Present Study
The main purpose of this research is to examine reports of PTG by emerging adults who have experienced trauma during adolescence compared with a comparison group recruited from the same sample frame. Specifically, the goals are to compare the levels and types of reported growth and examine the differential contributions that attachment, coping, and social support play in reports of PTG (directly and indirectly) between these two groups. This design will allow for a better understanding of the ways that growth is commonly experienced by emerging adults without prior exposure to trauma and how the experiences of growth may differ for those who have experienced a traumatic event during adolescence.
The theoretical model to be tested includes the relationships among PTG, attachment style, coping, and perceived social support (Fig. 1). Using this model as a guide, the present research design will examine the relationships among these variables, including exploratory structural model comparisons between the trauma and comparison groups. It is hypothesized that the comparison group will report higher levels of PTG in the domains of relating to others and new possibilities; whereas, the trauma group will report higher levels of appreciation for life. In addition, this design will attempt to identify any differences between the groups in regard to the structural pathways leading to PTG.

Theoretical model of attachment, social support, coping, and posttraumatic growth
Method
Procedure
Undergraduate students at a large New England university were recruited through a listserv announcement. Incentive for participation was a chance to receive one of eleven $10 Starbucks gift cards. Participants were organized into two groups: those who had experienced a trauma as an adolescent (trauma group) and those who had had not experienced a traumatic event during high school (comparison group). All participants were between the ages of 18 and 23, currently enrolled at the university where recruitment took place, and had either experienced a traumatic event during high school (trauma group) or had not experienced a traumatic event during high school (comparison group).
This research was approved by the university Institutional Review Board. Participants completed an online survey, and after agreeing to participate, they were asked to respond yes or no to “Did you experience any of the following events during the years you were in high school?”
-
1)
diagnosed with a life-threatening health condition
-
2)
a life-threatening injury or accident
-
3)
the death of a close family member or friend
-
4)
victim or witness of a violent crime or assault
-
5)
victim or witness of physical or sexual abuse
-
6)
loss of your home
-
7)
terrorist attack
-
8)
natural or manmade disaster
-
9)
unexpected pregnancy or miscarriage
These nine categories were selected based on a review of the events used in the Diagnostic and Statistical Manual of Mental Disorders-IV (American Psychiatric Association 2005) to define a traumatic event and items included on the Traumatic Life Events Questionnaire (TLEQ, Kubany et al. 2000). Because the specific trauma is not germane to the aims of this study, indication of the specific trauma(s) experienced was not collected; however, the list of events was included in order to minimize subjectivity of a traumatic event and to create a clear delineation between the trauma and comparison groups.
Participants who responded “yes” to the initial question regarding trauma experienced during high school (trauma group) were then instructed “if you experienced more than one of the above events during high school, please focus on the one that you believe has had the greatest impact on you for the remainder of this survey.” Participants in the trauma groups were then presented with questions worded in regard to the “traumatic event” they reported; participants in the comparison group answered the same survey items except they were worded in regard to their “transition to college.”
Participants completed quantitative measures assessing posttraumatic growth, attachment style, coping strategies, and social support. Counterbalancing of these measures was used to control for order effects. Participants were also asked to provide demographic information including age, gender, race/ethnicity, major, and class year.
Measures
Posttraumatic Growth
The Posttraumatic Growth Inventory (PTGI, Tedeschi and Calhoun 1996) is a widely used measure of perceptions of positive changes experienced by individuals following traumatic events. This scale consists of 21 items representing five subscales: relating to others, new possibilities, personal strength/growth, spirituality, and appreciation for life. Tedeschi and Calhoun reported high internal consistency (α = .90) and test-retest reliability (r = .71) as well as good discriminant and construct validity. Cronbach’s alpha in this study was .93, and subscale alphas ranged from .73 to .88. The measure instructs participants to indicate the degree to which each item occurred in their life as a result of their identified trauma (or transition to college). Responses are scored on a 6-point Likert scale ranging from 0 (I did not experience this change as a result of my [traumatic event/transition to college]) to 5 (I experienced this change to a very great degree as a result of my [traumatic event/transition to college]) and higher scores indicate a greater amount of growth experienced.
Attachment Style
The Measure of Attachment Qualities (MAQ; Carver 1997a) consists of 14 items measuring four aspects of adult attachment: avoidance, ambivalence-worry, ambivalence-merger, and secure. Item responses are ratings of attachment attitudes and feelings in general and are not specific to the participants’ experiences or specific types of relationships. Items are scored on a 4-point Likert scale from 1 (I disagree with this statement a lot) to 4 (I agree with this statement a lot). Carver (1997a) reported good convergent validity with other measures of attachment and test-retest reliabilities for the subscales have ranged from .61 to .80. Cronbach’s alpha for the subscales in this study ranged from .67 to .78. Higher subscale scores indicate greater adherence to the corresponding dimension of attachment.
Coping
Coping strategies were assessed using the Brief COPE (Carver 1997b). This scale is an abbreviated version of the original COPE and consists of 14 types of coping, each measured with two items. Participants respond to items regarding how they have coped with their traumatic event (or transition to college) since its occurrence. In order to measure coping strategies used in response to the traumatic event (or transition to college), the original scales’ use of present perfect tense was changed to include past tense. Participants were instructed to respond to each item on a 4-point Likert scale ranging from 1 (I didn’t or don’t do this at all) to 4 (I did or do this a lot) in regards to the reported trauma (or transition to college). Higher scores indicate more frequent use of that corresponding strategy. Carver reported adequate test-retest reliability (r ranges from .42–.89) of the subscales, and Cronbach’s alphas for the subscales in this study ranged from .54 to .93.
Social Support
The Medical Outcomes Study Social Support Survey (MOS-SS) is a 19 item measure of functional social support that includes four subscales of emotional / informational, tangible, affectionate, and positive social interaction (Sherbourne and Stewart 1991). Participants respond to: “People sometimes look to others for companionship, assistance, or other types of support. How often has each of the following kinds of support been available to you if you needed it since your traumatic event?” Responses are scored on a 5-point Likert scale from 1 (none of the time) to 5 (all of the time) with higher scores indicating a greater level of perceived support. Discriminant, convergent, and construct validity have been previously demonstrated (Sherbourne and Stewart), and in the current study, subscale Cronbach’s alpha ranged from .89 to .94.
Data Analysis
SPSS version 19 and AMOS version 20 were used for statistical analyses. Descriptive statistics and t-tests were run to test the differences in variable means between the two groups, and bivariate correlations were run to test the relationships of attachment, social support, and coping with PTG. Structural equation modeling was used to test for model invariance of the factor loadings, paths, and intercepts across groups. Chi square (χ2), comparative fit index (CFI), root mean square error of approximation (RMSEA), and probability of close fit (PCLOSE) were used to test for goodness-of-fit.
Results
Overall, 546 college students were enrolled in the study. The trauma group was comprised of 359 students who reported having experienced one of the nine preselected traumatic events during adolescence, and 187 students made up the comparison group. The average age of the sample was 19.7, Caucasian (75.6%) was the most common race reported, females made up 81.2% of the sample, and class year was approximately evenly represented. There were no differences in these demographic characteristics between the trauma group and the comparison group. As a precursor to the SEM analyses, Table 1 displays the descriptive statistics of study variables by group including the results of independent sample t-tests. Of note, partial support for the study hypothesis was found in the significantly higher scores in the domain of new possibilities for the comparison group and significantly higher scores in the domain of appreciation for life for the trauma group. However, contrary to the study hypothesis, relating to others did not significantly vary across groups. Of particular interest, individuals in the trauma group reported engaging in more avoidant coping strategies (self-distraction, denial, behavioral disengagement, acceptance); whereas, those in the comparison group reported using more approach-oriented coping strategies (active, use of instrumental support, positive reframing, planning). Table 2 shows the bivariate correlation coefficients of the domains of social support, attachment, and coping with overall posttraumatic growth. The strongest correlates with PTG were approach-oriented coping strategies (active coping, use of emotional and instrumental support, positive reframing, planning, and turning to religion). Coefficients were compared between the trauma and comparison group using the Fisher z-transformation, and no differences were found to be statistically significant.
Model Development
Measurement Models
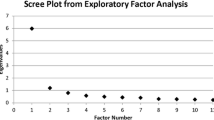
The measurement model of the PTGI as a five factor model was subjected to goodness of fit test. The initial analysis revealed the model to be a less than adequate fit of the data (χ2(184) = 789.985, p < .001; CFI = .892; RMSEA = .078; PCLOSE < .001). The spiritual change subscale loading on the PTGI was only .45, and considering that the subscale score was positively skewed, it was removed from analyses. Modification indices, standard residual covariances, and item cross-loadings were analyzed. As a result and based on empirical and theoretical justifications, four items were dropped. Specifically, three items from the relating to others subscale (I more clearly see that I can count on people in times of trouble, I have more compassion for others, I put more effort into my relationships) and one item from the new possibilities subscale (I developed new interests) loaded on multiple domains of the PTGI and were found to have problematic (> 1.96) standardized residual covariances with multiple other items.
The coping measurement models were constructed based on bivariate correlations between the Brief COPE subscales and PTGI scores. These analyses revealed six correlation coefficients greater than r = .30; however, one of those was turning to religion which no longer had a strong correlation with PTG after the spiritual change subscale was removed. Of the remaining five factors, three loaded onto one latent variable labeled intrapersonal coping: active coping (r = .36), positive reframing (r = .39), and planning (r = .34). Two loaded onto a second latent variable labeled interpersonal coping: use of emotional support (r = .36) and use of instrumental support (r = .37). Follow-up tests of reliability were conducted on these two custom subscales, and the Cronbach’s alphas were .90 for the intrapersonal items and .81 for the interpersonal items.
No significant modifications were made to the MOS-SS or MAQ measures because their baseline analyses demonstrated adequate goodness of fit. The final overall sample size of 546 was adequate for SEM analyses, but the size of the comparison group (187) was found to be inadequate (resulting in Heywood cases) when all individual measurement items were included in the initial models. Thus, the initial measurement model included the observed overall scores of support and secure and avoidant attachment; the latent variables of PTG, interpersonal coping, and intrapersonal coping were defined with parcels (observed composite subscale scores derived from individual measurement items with identical Likert-scale responses; Kline 2011).
Structural Model
Based on the theoretical and empirical research reviewed, the measurement model was transformed to a structural model by removing the correlational relationships among the six primary variables of interest and adding directional arrows indicating causal relationships based on the current literature (see Fig. 2). These include:
-
secure and avoidant attachment ➔ interpersonal and intrapersonal coping
-
secure and avoidant attachment ➔ social support
-
secure and avoidant attachment ➔ posttraumatic growth
-
interpersonal and intrapersonal coping ➔ posttraumatic growth
-
social support ➔ posttraumatic growth

Conceptual path diagram of secure attachment, avoidant attachment, social support, intrapersonal coping, interpersonal coping, and posttraumatic growth. Dotted lines represent constructs and paths excluded from final model
Modification indices were reviewed, and several correlation paths were added. The pooled sample data were then split into the trauma and comparison groups so assessments could be made. Regression weights of the paths were examined for nonsignificance across groups; paths that were not significant in both groups were trimmed from the model for parsimony. As a result, several paths were removed from the structural model (see Fig. 2):
-
interpersonal coping ➔ posttraumatic growth
-
secure attachment ➔ posttraumatic growth
-
avoidant attachment ➔ posttraumatic growth
-
secure attachment ➔ interpersonal coping
-
avoidant attachment ➔ interpersonal coping
-
avoidant attachment ➔ intrapersonal coping
Because the latent variable of interpersonal coping did not contribute significantly to this model for both the trauma group and the comparison group, it was excluded from further analysis. The direct paths of secure and avoidant attachment to PTG were also found to be nonsignificant, and those paths were removed from the analyses; however, the two attachment constructs were kept in the model because of their indirect influence on PTG through pathways with the intrapersonal coping and social support. The resulting model (see Fig. 3) was a good-fitting model: (χ2(58) = 128.999, p < .001; CFI = .966; RMSEA = .047; PCLOSE = .634).

Final path diagram and standardized coefficients of fully saturated model fit to the data representing attachment, support, intrapersonal coping, and posttraumatic growth (n = 546)
Structural Equation Model Results
The total variance of PTGI that was explained by the factors in the baseline model was 24.7% in the trauma group and 20.3% in the comparison group. The direct and indirect effects of attachment, support, and coping on PTG and the PTGI subscales are presented in Table 3. Across both groups, only the effect of intrapersonal coping was greater than .30 in magnitude as a contributor to the variance in PTGI scores.
The summary of the structural equation multi-group analyses for the model is shown in Table 4. There were nonsignificant changes in model fit when the factor loadings and paths were constrained to be equal across groups. However, significant differences between groups were found in the third step when the intercepts of the variables were constrained; the differences from the baseline model (Δχ2 = 207.420 Δdf = 20, p < .001) and the model with constrained factor loadings and paths (Δχ2 = 201.952 Δdf = 10, p < .001) resulted in a fit of the model that was significantly worse. This finding is interpreted as a difference between groups on the mean scores of one or more of the items constrained.
To identify which specific mean(s) varied across groups, intercepts were constrained one at a time. This closer investigation of the intercepts revealed all three factors of intrapersonal coping (active ΔX2 = 18.68, p < .001, positive reframing ΔX2 = 14.41, p < .001, and planning ΔX2 = 39.67, p < .001) and the PTGI domain of new possibilities (ΔX2 = 65.65, p < .001) to be significantly higher in the comparison group.
Discussion
This study of a theoretical model of posttraumatic growth is innovative in both the population of interest and the methodological design. The design reported here allowed for an evaluation of PTG by comparing a group of emerging adults who reported on a traumatic event that was experienced during adolescence (trauma group) with a group of emerging adults who reported on their transition from high school to college (comparison group). This design allowed for an analysis of growth and the factors commonly associated with reports of growth across groups in order to better understand how growth that results from exposure to a traumatic event during adolescence differs from growth that results from a life transition during later adolescence.
The first two goals of this study were to compare the levels of and types of reported growth between these two groups. Emerging adults who responded to survey items in regard to their transition from high school to college reported higher levels of overall growth compared with those emerging adults who reported on growth as an outcome related to their exposure to a traumatic event during adolescence. This difference in overall growth was found to be at least partly accounted for in the domain of new possibilities and may result from the fact that college is a time of intellectual growth. By taking classes, making new acquaintances, interacting with peers and professors, and exploring career interests, these emerging adults are exposed to a wealth of new opportunities to explore. Whereas new opportunities such as career exploration are commonly pursued by high school and college students, such opportunities for this type of growth may be less commonly realized for survivors of traumatic events experienced during adolescence possibly due to a different focus of attention (on the trauma rather than developmental tasks) and the disruption of typical development during the critical years of adolescence.
What carries particular weight, however, when considering potential clinical implications is the lower level of reported growth in the domain of new possibilities for the trauma group (this was the largest effect found). Adolescent and emerging adult years are regarded as development stages of growth and exploration. The fact that the trauma group reported such lower levels of growth in new possibilities than the comparison group could inform and be a focal point of clinical approaches to working with young trauma survivors. Although one cannot ascertain that these experiences during high school years caused this difference in reporting growth in the domain of new possibilities, the possibility that trauma at this life stage can impede the recognition of growth from more expected and non-traumatic life events (i.e., transitioning to college) warrants further investigation. It is also unclear if the exposure to these events had an adverse effect on the adolescent’s ability/opportunity to recognize new possibilities or if they actually experienced two distinct forms of growth: one reported here from exposure to trauma and one (not collected here) resulting from their transition to college.
Another goal of this study was to examine the differential contributions that attachment, coping, and social support play in reports of PTG (directly and indirectly) between these two groups. The influence of these factors on PTG did not differ across groups. This suggests that the pathways to PTG are similar for these two groups, and the sources examined in this study (traumatic event and transition to college) do not change how attachment, support, and coping influence PTG. However, an important finding regarding the mean group differences of these independent variables comes from the analyses of the COPE domains. The scores of the three intrapersonal coping strategies (positive reframing, planning, and active coping) were all significantly higher for the comparison group than the trauma group. This suggests that individuals exposed to trauma during adolescence are less likely to engage in approach-oriented coping strategies, which appears to be one pathway to recognizing growth. It may be the independent nature of being a college student that fosters the use of these intrapersonal coping strategies, or it may be the emotionally distressful nature of trauma that interferes with the ability to engage in such coping strategies. This study, however, was unable to tease out whether these differences in coping are more strongly related to the events being coped with or the age and life stage of the individuals who experienced these events.
Intrapersonal coping was the strongest predictor of PTG for both groups, which supports the body of research on PTG (Prati and Pietrantoni 2009). However, none of the weights of the paths to overall PTG differed significantly across models, suggesting that the processes to experiencing growth appear to be independent of the triggering events. What did differ, though, were the paths taken across groups. The comparison group engaged in more intrapersonal coping strategies (the strongest correlate with PTG) and was, thus, more likely to report higher levels of overall growth.
It is not uncommon for adolescents to feel a sense of isolation or alienation as they struggle with the physiological, social, and cognitive changes experienced during adolescence. However, when trauma exposure is added to these stressors to be managed, the resulting withdrawal can be potentially disruptive developmentally if the trauma is not managed appropriately in order to minimize the impact of the trauma on developmental tasks. Valuable implications arise from these findings in regard to clinical approaches to working with adolescents exposed to traumatic events. Focusing on mutable factors, such as active coping strategies when dealing with significant stressors, appears to be a critical area that can benefit adolescents.
These findings need to be evaluated under the conditions of the study’s limitations. One limitation is the timing of the events reported on. The trauma group reported on an event that happened during high school (approximate ages 14–17); whereas, the comparison group reported on their transition from high school to college (approximate ages 18–19). This also meant that the trauma group was subjected to a greater potential for recall bias regarding the retrospective nature of the wording of the survey items, but more importantly, this time frame difference also includes a number of years in which cognitive development is still a significant process (adolescence). As a result, it is impossible to tease out if the findings are a direct result of the differential nature of the events being reported on or the different ages/developmental stages of the participants in which these events occurred. Additionally, an important consideration of all cross-sectional studies is that they cannot identify causal relationships or explain the structural pathways in a causal context. Finally, generalization of these findings beyond the sample frame from which the participants were recruited is not possible.
These findings have potential clinical implications for those working with adolescent and emerging adult survivors of trauma exposure. Recognizing that vulnerable areas of adolescent development, such as new possibilities, can be interrupted following exposure to a traumatic event can inform assessment and intervention designs aimed at facilitating adaptive adjustment and growth in the adolescent and emerging adult years. There are opportunities from this study to better inform clinical approaches and future studies aimed at understanding the transformative potential of mutable health behaviors (e.g., coping skills) that may foster growth. There is no question that, despite the limitations of this research design, there are clear differences in the coping processes related to traumatic experiences during adolescence compared with life transitions during emerging adulthood, and focusing on these mutable coping strategies may be a critical first component to positioning adolescents exposed to trauma to be able to experience some sense of growth from their experiences.
References
Aldwin, C. M., & Levenson, M. R. (2004). Posttraumatic growth: A developmental perspective. Psychological Inquiry, 15, 19–22.
American Psychiatric Association. (2005). Diagnostic and statistical manual of mental disorders (4th ed. Text Revision). Washington, DC: American Psychiatric Association.
Anderson, W. R., & Lopez-Baez, S. I. (2008). Measuring growth with the posttraumatic growth inventory. Measurement and Evaluation in Counseling and Development, 40, 215–227.
Anderson, W. R., & Lopez-Baez, S. I. (2011). Measuring personal growth attributed to a semester of college life using the posttraumatic growth inventory. Counseling and Values, 56, 73–82.
Arnett, J. J. (2000). Emerging adulthood: A theory of development from the late teens through the twenties. American Psychologist, 55, 469–480.
Bellizzi, K. M., & Blank, T. O. (2006). Predicting posttraumatic growth in breast cancer survivors. Health Psychology, 25, 47–56.
Cadell, S., Regehr, C., & Hemsworth, D. (2003). Factors contributing to posttraumatic growth: A proposed structural equation model. American Journal of Orthopsychiatry, 73, 279–287.
Carver, C. (1997a). Adult attachment and personality: Converging evidence and a new measure. Personality and Social Psychology Bulletin, 23, 865–883.
Carver, C. (1997b). You want to measure coping but your protocol's too long: Consider the brief COPE. International Journal of Behavioral Medicine, 4, 92–100.
Gottlieb, B. H., Still, E., & Newby-Clark, I. R. (2007). Types and precipitants of growth and decline in emerging adulthood. Journal of Adolescent Research, 22, 132–155.
Kline, R. B. (2011). Principles and practice of structural equation modeling. New York: Guilford Press.
Kubany, E. S., Leisen, M., Kaplan, A. S., Watson, S. B., Haynes, S. N., Owens, J. A., & Burns, K. (2000). Development and preliminary validation of a brief broad-spectrum measure of trauma exposure: The traumatic life events questionnaire. Psychological Assessment, 12, 210–224.
Mikulincer, M., & Florian, V. (1995). Appraisal of and coping with a real-life stressful situation: The contribution of attachment styles. Personality and Social Psychology Bulletin, 21, 406–414.
Morris, B. A., Shakespeare-Finch, J., & Scott, J. L. (2007). Coping processes and dimensions of posttraumatic growth. The Australasian Journal of Disaster and Trauma Studies, 1, 1–10.
Ognibene, T. C., & Collins, N. L. (1998). Adult attachment styles, perceived social support and coping strategies. Journal of Social and Personal Relationships, 15, 323–345.
Park, C. L. (2009). Overview of theoretical perspectives. In C. Park, S. Lechner, M. Antoni, & A. Stanton (Eds.), Medical illness and positive life change: Can crisis lead to personal transformation? (pp. 11–30). Washington, DC: American Psychological Association.
Park, C., Cohen, L., & Murch, R. (1996). Assessment and prediction of stress-related growth. Journal of Personality, 64, 71–105.
Park, C. L., Aldwin, C. M., Fenster, J. R., & Snyder, L. B. (2008). Pathways to posttraumatic growth versus posttraumatic stress: Coping and emotional reactions following the September 11, 2001, terrorist attacks. The American Journal of Orthopsychiatry, 78, 300–312.
Prati, G., & Pietrantoni, L. (2009). Optimism, social support, and coping strategies as factors contributing to posttraumatic growth: A meta-analysis. Journal of Loss and Trauma, 14, 364–388.
Salo, J. A., Qouta, S., & Punamäki, R. (2005). Adult attachment, posttraumatic growth and negative emotions among former political prisoners. Anxiety, Stress & Coping: An International Journal, 18(4), 361–378.
Schmidt, S. D., Blank, T. O., Bellizzi, K. M., & Park, C. L. (2012). The relationship of coping strategies, social support, and attachment style with posttraumatic growth in cancer survivors. Journal of Health Psychology, 17, 1033–1040.
Sherbourne, C., & Stewart, A. (1991). The MOS social support survey. Social Science & Medicine, 32, 705–714.
Swickert, R., & Hittner, J. (2009). Social support coping mediates the relationship between gender and posttraumatic growth. Journal of Health Psychology, 14, 387–393.
Tedeschi, R. G., & Calhoun, L. G. (1996). The posttraumatic growth inventory: Measuring the positive legacy of trauma. Journal of Traumatic Stress, 9, 455–471.
Tedeschi, R. G., & Calhoun, L. G. (2004). Posttraumatic growth: Conceptual foundations and empirical evidence. Psychological Inquiry, 15, 1–18.
Thornton, A. A., & Perez, M. A. (2006). Posttraumatic growth in prostate cancer survivors and their partners. Psycho-Oncology, 15, 285–296.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Schmidt, S.D., Blank, T.O., Bellizzi, K.M. et al. Posttraumatic Growth Reported by Emerging Adults: a Multigroup Analysis of the Roles of Attachment, Support, and Coping. Curr Psychol 38, 1225–1234 (2019). https://doi.org/10.1007/s12144-017-9670-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12144-017-9670-0