
Abstract
Although there are data on the psychometric properties of the Client Satisfaction Questionnaire (CSQ-8) in the United States Hispanic population, there are no data about the suitability of the questionnaire in Spanish-speaking populations in Spain. Trained and independent interviewers administered a Castilian Spanish translation of the CSQ-8 to 205 subjects (86.3% women, mean age 55.6 years) with subclinical depressive symptoms who participated in brief cognitive-behavioral group therapy interventions in Spain to treat subclinical depression. The internal consistency of the scale was satisfactory (α = .80). A single factor was identified that aggregated all eight items with high loadings in this global factor, which accounted for 43.5% of total variance. Differences in satisfaction were found based on the patients’ education level (p = .038) and post-treatment depressive symptoms (p = .021). There were no differences in level of satisfaction based on sex, age, marital status, social class, pre-treatment depressive symptoms or the number of sessions attended. The results indicate that the Castilian Spanish CSQ-8 has adequate psychometric properties and maintains those of the original questionnaire; therefore, it is suitable for use in Spain for assessment of satisfaction with services received.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Measurement of patient satisfaction with service received has become an important aspect in the assessment of human and health services (Rosenblatt and Attkisson 1993). In general terms, patient satisfaction information is valuable because it provides a consumer viewpoint that is necessary for a complete, unbiased assessment of intervention programs (Pascoe and Attkisson 1983) and is commonly used as a component of the assessment of quality of services (Säilä et al. 2008).
From the patient’s viewpoint, assessment of satisfaction is the only available method to express his/her concerns about the services received and to express his/her opinion about new services he/she needs (World Health Organization 2000). From the professionals’ viewpoint, the assessment of patient satisfaction can be seen as an opportunity to obtain feedback that can be very useful to those responsible for health policy in order to improve the offered services (European Foundation for Quality Management 2013). For example, service managers and designers of interventions and clinicians can critically review the quality of intervention programs implemented and services offered, as well as introduce improvements to them based on patient satisfaction feedback. Furthermore, assessment of patient satisfaction is important for all health facilities because it is a predictor of patients’ reactions and behaviors. In fact, it has been found that low satisfaction is related to bad word-of-mouth communications about the center (Zemke 1999) and with a greater likelihood of a change in service provider (Marquis et al. 1983).
However, previous studies have acknowledged that there are various factors outside of the service provided associated with patients’ level of satisfaction, such as their sociodemographic characteristics like their sex, age or education level (Hall and Dornan 1990; Larsen et al. 1979), their health status (Hall et al. 1993) or the results obtained from the treatment (Attkisson and Zwick 1982). In addition, studies about patient satisfaction with health services have been limited to date by methodological aspects such as low response rate, assessment of satisfaction in only an individual intervention format and the lack of validated assessment tools.
In fact, although a variety of tools have been developed to assess patient satisfaction in various programs and health care services (e.g., Barker et al. 1996; Varela et al. 2003), few have examined their psychometric properties. A review of 195 studies about data of patient satisfaction with health services found that only 46% of studies provided some validity or reliability data, and that those that used a validated instrument showed a greater validity and reliability than those that used new or modified tools (Sitzia 1999).
Among the validated tools, the Client Satisfaction Questionnaire, in its 8-item version (CSQ-8; Larsen et al. 1979), has been used most commonly to assess satisfaction in mental health services (Sitzia 1999). This tool includes a brief standardized scale with good psychometric properties that provides an overall assessment of satisfaction (Rush et al. 2008). The original version of this questionnaire is in English, but CSQ-8 is currently available in more than 30 languages, including Spanish (Attkisson 2015). However, simply translating the items on the questionnaire does not guarantee that the items have the same significance in all cultures (Attkisson and Greenfield 1994). Although there are data about the CSQ-8 in different cultural contexts, including United States Hispanics (Roberts and Attkisson 1983; Roberts et al. 1984), there are no data about the suitability of the scale in Spanish-speaking populations in Spain. This is of major importance, because measures validated in one culture may not be appropriate in others. Furthermore, although there is a Castilian Spanish translation of the CSQ-8 (Vázquez et al. 2009), its psychometric properties have not been evaluated.
In the current study, the psychometric properties of the Castilian Spanish version of the CSQ-8 were analyzed in a sample of people with subclinical symptoms of depression who participated in a group therapy intervention. The primary objective was to examine the internal consistency and factorial structure of the CSQ-8. The second objective was to analyze the differences in satisfaction with the service received based on the patients’ sociodemographic characteristics, the number of sessions of the intervention attended and the results obtained with the intervention. Specifically, it is expected that the Castilian Spanish translation of the CSQ-8 has adequate psychometric properties consistent with the original version of the questionnaire, and that patient variables such as age or education level and post-treatment depressive symptoms are related to the level of satisfaction achieved.
Method
Sample
The data for this study were extracted from 209 patients who underwent brief cognitive-behavioral group therapy interventions (maximum 5 sessions) to treat subclinical depression at the Depressive Disorders Unit (DDU) of the Faculty of Psychology of University of Santiago de Compostela (Spain) from September 2011 to December 2014. The patients were referred by health centers and by previous patients.
All participants had a score equal to or greater than 16 on the Center for Epidemiologic Studies Depression Scale (Radloff 1977; Spanish version of Vázquez et al. 2007). None of them met the diagnostic criteria for a major depressive episode. They also did not present with suicidal ideation or any of the following mental disorders: dysthymia, bipolar I and II disorders, panic disorder, obsessive-compulsive disorder, cyclothymia, anorexia, bulimia, psychotic disorders, alcohol dependence or dependence on other substances, somatization disorder, hypochondriasis, undifferentiated somatoform disorder.
Of the total 209 patients treated, 4 did not complete psychological intervention and did not fill out the final questionnaires. The reasons for not continuing the intervention were health problems, lack of time and an inability to locate the person. Therefore, the final sample was comprised of 205 participants with a mean age of 55.6 years, obtaining a response rate of 98.1% for the CSQ-8. No significant differences were found among those who stopped the intervention and those who continued until the end of the intervention based on sex (p = .452), age (U = 408.5, z = −0.013, p =.990), marital status (p = 1.000), social class (p =.134), education level (p =.463), or initial depressive symptoms (U = 344.0, z = −0.553, p =.580).
In addition, all of the participants included in this study were informed of the nature of the study and gave their informed consent to make use of the data analyzed in this study. Participation was voluntary; none of the participants received financial compensation or incentive of any type.
Instruments
Sociodemographic Data
The sex, age, marital status, self-perceived social class and education level of all subjects were recorded in an ad hoc questionnaire designed for this study.
Center for Epidemiological Studies Depression Scale
(CES-D; Radloff 1977; Spanish version of Vázquez et al. 2007). This is a self-report scale of 20 items that provides a continuous score that reflects the level of depressive symptoms during the last week. Each of the 20 items is assessed on a Likert-type scale of four possible answers ranging from 0 (rarely or none of the time) to 3 (most of the time). Therefore, the range of the scale is 0 to 60, where a higher score corresponds to greater depressive symptoms. The internal consistency is .89.
Structured Clinical Interview for DSM-IV Axis I Disorders Clinician Version
(SCID-CV; First et al. 1997/ 1999). This is a semi-structured interview that provides Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM-IV) diagnoses and must be administered by a clinician. It is comprised of 6 modules: mood disorder episodes, psychotic symptoms, psychotic disorders, mood disorders, substance use disorders, anxiety and other disorders. The reliability between interviewers (kappa) is .61.
Record of Sessions
For each participant, the number of sessions that he/she attended during the intervention was computed.
Client Satisfaction Questionnaire
(CSQ-8, Larsen et al. 1979; Castilian Spanish translation from Vázquez et al. 2009). The CSQ-8 is a self-report questionnaire that assesses the general level of satisfaction with the service received. It is comprised of eight items that is scored on a scale, ranging from 1 to 4. The total score varies from 8 to 32, where a higher score indicates greater satisfaction with the service received. The internal consistency of the original English version scale ranges from .83 to .93 (Attkisson and Greenfield 2004).
Procedure
We produced a new Spanish-language version (Castilian) more suitable for use in Spain. We followed the general recommendations of Guillemin et al. (1993), and included back-translation (Brislin et al. 1973). The CSQ-8 was translated into Castilian Spanish by two researchers (both of them Spanish native hispanophones familiar with English), and was then back-translated by an independent translator, whose mother tongue is English and who had not been exposed to the English version of the CSQ-8. This back-translation was used by a bilingual expert panel to identify and resolve flaws in the Castilian version; the new Castilian version was back-translated once more, and the new back-translation was re-evaluated by the panel. The process was repeated until the panel was satisfied that the Castilian Spanish and English versions were equivalent (Vázquez et al. 2009).
Following the recommendations of Attkisson and Greenfield (2004) to implement the CSQ-8, a system for collecting information on patient satisfaction was implemented. A waiting room survey was administered by independent administrators trained in the procedures for systematically soliciting voluntary participation from patients. The administrators requested that patients filled out the questionnaire at the end of the last session of the intervention, gave the patients the questionnaire to fill out on-site and responded any questions. Questionnaires were self-administered by all participants and were completed in about 5–10 min.
Data Analysis
All calculations were performed using SPSS statistical software (version 20.0). Calculations were done for the frequencies, percentages, means and standard deviations of the sociodemographic variables, the score in depressive symptoms and the number of sessions attended, as well as the satisfaction score and the score of each of the items of the CSQ-8. There were few participants who did not continue the intervention until the end and therefore did not fill out the final assessment tools, so they were not taken into account in the statistical analyses.
To analyze the internal consistency of the Castilian Spanish CSQ-8, the Pearson correlations between its items and between the scores on each one of the items and the total corrected score (i.e., the total score without taking that item into account), as well as Cronbach’s α coefficient, were calculated.
To explore the underlying dimensions of the CSQ-8, a factor analysis was performed with extraction of factors using the principal components extraction method. To determine the number of factors that should be extracted, the number of items with an eigenvalue greater than 1 was used. Subsequently, in a second phase, a varimax orthogonal rotation was performed to try to minimize the number of items that had a great weight in one factor. The measure of adequacy of the sample was performed using the Kaiser-Meyer-Olkin index and the identity correlation matrix was tested through Bartlett’s sphericity test.
To assess the possible relationship between the characteristics of the sample at baseline and post-treatment satisfaction, the Student’s t-test, ANOVA and Pearson’s correlation coefficient were used depending on the characteristics of the variables involved and the number of groups used. Pearson’s correlation coefficients were used to analyze the relationship between the number of sessions attended, pre- and post-treatment depressive symptoms and CSQ-8 satisfaction.
Results
Sample Profile
Of the participants, 86.3% were women, their ages ranged from 31 to 79 years, with a mean of 55.6 years (SD = 10.1), 73.2% had a partner, 55.6% stated that they belonged to a low or lower-middle class, 55.6% had completed a primary education. The mean depressive symptoms score before the intervention was 24.0 (SD = 7.1). Participants attended a mean of 4.2 sessions (SD = 0.9), and had a mean score of 11.8 (SD = 8.7) in depressive symptoms after the intervention (see Table 4).
Measurement Adequacy
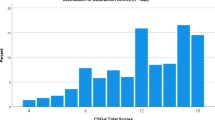
Table 1 shows the distribution of scores in the Castilian Spanish CSQ-8. Mean CSQ-8 score was 29.2 (SD = 2.6; range 21–32) and neither the peak index nor the symmetry of the distribution curve of the scores exceeded values of ±1 (kurtosis = −0.17 and symmetry = −0.88). Among the responses of all subjects, 0.2% of items were scored as 1, 1.7% as 2, 31.6% as 3 and 66.5% as 4. Mean-over-subjects item ratings ranged from 3.32 for the Needs item to 3.85 for Recommended (Table 2; see Table 3 for item names). Item-total correlation coefficients ranged from .43 for Needs to .60 for Amount of help, and all were significant (p < .001). The mean inter-item correlation coefficient was .351, with a minimum of .19 and a maximum of .47, and Cronbach’s α = .80.
Factor Structure
A principal components factor analysis with varimax rotation identified one primary factor with eigenvalue greater than unity which accounted for 43.5% of total variance. This factor (eigenvalue = 3.48) aggregated all eight items: three with factor loadings > .7 (the Amount of help, Satisfied and Quality items), four with loadings between .6 and .7 (Come back, Recommended, Wanted and Effectively), and one with a loading between .5 and .6 (Needs). In Table 3, factor loadings of the eight items are presented.
Patient Characteristics vs. CSQ-8 Satisfaction
As can be seen in Table 4, there were no significant differences in satisfaction with services received based on participants’ sex, age, marital status or social class. However, significant differences were found in the satisfaction scores based on their education level, F (2, 202) = 3.39, p = .036, ηp2 = 0.03. Post hoc Scheffé’s tests showed that there was a significantly greater satisfaction (p =.038) in literate participants who had just learned to read and write (M = 29.8; SD = 2.4) than in individuals with secondary or university studies (M = 28.3; SD = 3.2).
Moreover, there were no significant differences in satisfaction based on the level of pre-treatment depressive symptoms or the number of sessions attended. However, there was a significant negative correlation between satisfaction with the services received and the depressive symptoms score at the end of the intervention (r = −.16, p = .021).
Discussion
This study evaluated the psychometric properties of the Castilian Spanish translation of the CSQ-8 in a sample of patients with subclinical depressive symptoms who received brief group therapy intervention and analyzed the factors associated with patient satisfaction.
The distribution of scores did not differ considerably from the normal curve, though there was an inclination toward a negative distribution due to the high levels of reported satisfaction found in the CSQ-8 (Nguyen et al. 1983). The total mean score of 29.2 and the per-item mean score of 3.6 found in this study were slightly higher than those found in the primary normative sample (Nguyen et al. 1983) and in Spanish-speaking populations (Roberts and Attkisson 1983; Roberts et al. 1984). This fact is of great importance because the evidence supports that intention to use the same facility again is directly affected by satisfaction (Gotlieb et al. 1994).
The internal consistency of the Castilian Spanish CSQ-8 was satisfactory, with a Cronbach’s α of .80, a mean inter-item correlation coefficient of .351 and corrected item-total correlations ≥ .43. Although this Cronbach’s α is lower than the Cronbach’s α of .93 found by Larsen et al. (1979), it is similar to that found in the English-speaking group in the study of Roberts et al. (1984). Furthermore, the item-total and mean inter-item correlations satisfy the criteria recommended by Briggs and Cheek (1986) to reach an acceptable balance between the internal consistency and the amplitude of the measurement.
Our factor analysis showed a single general factor of satisfaction. All of the items had high loadings in this factor, which indicates an adequate factorial validity and a great conceptual consistency that confirms the findings of the original CSQ-8 of a global and one-dimensional measure of satisfaction (Larsen et al. 1979).
In regard to the analysis of sociodemographic characteristics and pre-treatment clinical characteristics associated with satisfaction level, differences were found only in patients’ education level; that is, those who had only learned to read and write demonstrated greater satisfaction than those who had secondary or higher education. This is consistent with the findings of previous studies (Roberts and Attkisson 1983; Roberts et al. 1984), and may be due to the fact that individuals with a higher education level had a greater likelihood of feeling that the intervention did not fit their education level as it was designed to be understood by patients of all educational levels. However, no significant differences were found based on patients’ sex, age, marital status, social class, pre-treatment depressive symptoms, or the number of sessions attended. This suggests, in general terms, a great homogeneity and robustness in the CSQ-8 as a tool for measuring satisfaction with the intervention. Furthermore, these results are along the same line as those found in the original scale, except for sex differences found previously in which women were more polarized than men in their responses (Larsen et al. 1979), and are consistent with those found in the Spanish version of the scale conducted with a sample of Spanish speakers (Hispanics) residing in the United States (Roberts and Attkisson 1983; Roberts et al. 1984).
Moreover, an association was found between patients’ satisfaction and their post-treatment depressive symptoms; those who had fewer depressive symptoms after the intervention expressed greater satisfaction. Although both depressive symptoms and satisfaction were assessed at post-treatment and this concurrence may have increased their association, this finding suggests adequate convergent validity of the Castilian Spanish translation of the CSQ-8 regarding patient improvement because of the value in positive changes (Attkisson and Greenfield 2004). Furthermore, this result is consistent with the finding of Larsen et al. (1979) and suggests a modest influence of the benefits obtained with therapy on the patients’ perceived satisfaction. Nevertheless, this interpretation should be taken with caution because association is not synonymous with causality, and the opposite could also occur, i.e., individuals who were more satisfied with the intervention were more likely to participate more actively in it and, therefore, obtain better results.
This study should be interpreted in light of its limitations. No data were obtained about the degree of satisfaction of patients who did not continue with the intervention until the end. This could limit the generalization of the results because there are data that indicate that satisfaction negatively correlates with early treatment dropout (Larsen et al. 1979). However, the scope of this limitation in this study is minimal due to the low percentage of patients who did not finished the intervention (only 1.9%), the fact that the reasons given for the discontinuation were not related to patient dissatisfaction and the lack of significant differences in the sociodemographic and clinical characteristics at baseline between patients who left the intervention and those who completed it. All of these questions eliminate bias attributable to nonresponse. Future studies in which the subjects who leave the intervention can express their level of satisfaction with the intervention received thus far are recommended. Moreover, new studies to analyze whether these results are consistent with clinical samples or with various mental disorders are suggested.
This study provides important lessons for research and clinical practice. It offers data about the reliability and validity of the Castilian Spanish translation of the CSQ-8 after group therapy intervention, presenting acceptable psychometric properties in line with the original questionnaire. This questionnaire can be used with confidence by clinics and investigators in Spain to evaluate the satisfaction of their patients with the services received within the context of our cultural context. The results provided by this questionnaire are of great relevance for the assessment of psychological programs, as well as planning and improvement of programs implemented due to their useful feedback; therefore, they are fundamental for evaluators and planners to improve the practice of their professions. In addition, they allow valid comparisons of patient satisfaction to be made between different health facilities, intervention programs and samples. Having indicators of client satisfaction available is essential to improving the competitiveness of organizations (European Foundation for Quality Management 2013) and to achieve a complete evaluation since when the patient’s perspective is not taken into account the evaluation of services is biased toward the provider’s or evaluator’s perspective. The Castilian CSQ-8 provides a valid and reliable tool for assessment of this measure in our country. Moreover, the results found in this study recommend the need to control the educational level and results of the intervention when analyzing data on patients’ satisfaction with the service received.
References
Attkisson, C. C. (2015). The Client Satisfaction Questionnaire (CSQ). Retrieved from http://www.csqscales.com/. Archived at http://www.webcitation.org/6hJGeESXS on 6 May 2016.
Attkisson, C. C., & Greenfield, T. K. (1994). The Client Satisfaction Questionnaire-8 and the Service Satisfaction Questionnaire-30. In M. E. Maruish (Ed.), The use of psychological testing for treatment planning and outcomes assessment (pp. 402–420). Hillsdale: Lawrence Erlbaum Associates.
Attkisson, C. C., & Greenfield, T. K. (2004). The UCSF Client Satisfaction Scales: I. The Client Satisfaction Questionnaire-8. In M. E. Maruish (Ed.), The use of psychological testing for treatment planning and outcomes assessment (Vol. 3, 3rd ed., pp. 799–811). Mahwah: Lawrence Erlbaum Associates.
Attkisson, C. C., & Zwick, R. (1982). The Client Satisfaction Questionnaire: Psychometric properties and correlations with service utilization and psychotherapy outcome. Evaluation and Program Planning, 5, 233–237. doi:10.1016/0149-7189(82)90074-X.
Barker, D. A., Shergill, S. S., Higginson, I., & Orrell, M. W. (1996). Patients’ views towards care received from psychiatrists. British Journal of Psychiatry, 168, 641–646. doi:10.1192/bjp.168.5.641.
Briggs, S. R., & Cheek, J. M. (1986). The role of factor analysis in the development and evaluation of personality scales. Journal of Personality, 54, 106–148. doi:10.1111/j.1467-6494.1986.tb00391.x.
Brislin, R. W., Lonner, W. J., & Thorndike, E. M. (1973). Cross-cultural research methods. New York: Wiley.
European Foundation for Quality Management. (2013). EFQM Excelence Model 2013. Brussels: EFQM.
First, M. B., Spitzer, R. L., Gibbon, M., & Williams, J. B. W. (1999). Entrevista Clínica Estructurada para los Trastornos del Eje I del DSM-IV- Versión Clínica (SCID-CV). [Structured Clinical Interview for DSM-IV Axis I Disorders, Clinician Version (SCID-CV)]. Barcelona: Masson (Original published in 1997).
Gotlieb, J. B., Grewal, D., & Brown, S. W. (1994). Consumer satisfaction and perceived quality: Complementary or divergent constructs? Journal of Applied Psychology, 79, 875–885. doi:10.1037/0021-9010.79.6.875.
Guillemin, F., Bombardier, C., & Beaton, D. (1993). Cross-cultural adaptation of health-related quality of life measures: Literature review and proposed guidelines. Journal of Clinical Epidemiology, 46, 1417–1432. doi:10.1016/0895-4356(93)90142-N.
Hall, J. A., & Dornan, M. C. (1990). Patient sociodemographic characteristics as predictors of satisfaction with medical care: A meta-analysis. Social Science and Medicine, 30, 811–818. doi:10.1016/0277-9536(90)90205-7.
Hall, J. A., Milburn, M. A., & Epstein, A. M. (1993). A causal model of health status and satisfaction with medical care. Medical Care, 31, 84–94. doi:10.1097/00005650-199301000-00007.
Larsen, D. L., Attkisson, C. C., Hargreaves, W. A., & Nguyen, T. D. (1979). Assessment of client/patient satisfaction: Development of a general scale. Evaluation and Program Planning, 2, 197–207. doi:10.1016/0149-7189(79)90094-6.
Marquis, M. S., Davies, A. R., & Ware, J. E. (1983). Patient satisfaction and change in medical care provider: A longitudinal study. Medical Care, 21, 821–829. doi:10.1097/00005650-198308000-00006.
Nguyen, T. D., Attkisson, C. C., & Stegner, B. L. (1983). Assessment of patient satisfaction: Development and refinement of a Service Evaluation Questionnaire. Evaluation and Program Planning, 6, 299–314. doi:10.1016/0149-7189(83)90010-1.
Pascoe, G. C., & Attkisson, C. C. (1983). The evaluation ranking scale: A new methodology for assessing satisfaction. Evaluation and Program Planning, 6, 335–347. doi:10.1016/0149-7189(83)90013-7.
Radloff, L. S. (1977). The CES-D Scale: A self-report depression scale for research in the general population. Applied Psychological Measurement, 1, 385–401. doi:10.1177/014662167700100306.
Roberts, R. E., & Attkisson, C. C. (1983). Assessing client satisfaction among Hispanics. Evaluation and Program Planning, 6, 401–413. doi:10.1016/0149-7189(83)90019-8.
Roberts, R. E., Attkisson, C. C., & Mendias, R. M. (1984). Assessing the Client Satisfaction Questionnaire in English and Spanish. Hispanic Journal of Behavioral Sciences, 6, 385–396. doi:10.1177/07399863840064004.
Rosenblatt, A., & Attkisson, C. C. (1993). Assesssing outcomes for sufferers of severe mental disorders: A conceptual framework and review. Evaluation and Program Planning, 16, 347–363. doi:10.1016/0149-7189(93)90049-E.
Rush, A. J., First, M. B., & Blacker, D. (2008). Handbook of psychiatric measures (2nd ed.). Washington, DC: American Psychiatric Publishing.
Säilä, T., Mattila, E., Kaila, M., Aalto, P., & Kaunonen, M. (2008). Measuring patient assessments of the quality of outpatient care: A systematic review. Journal of Evaluation in Clinical Practice, 14, 148–154. doi:10.1111/j.1365-2753.2007.00824.x.
Sitzia, J. (1999). How valid and reliable are patient satisfaction data? An analysis of 195 studies. International Journal of Quality in Health Care, 11, 319–328. doi:10.1093/intqhc/11.4.319.
Varela, J., Rial, A., & García, E. (2003). Presentation of a satisfaction scale with primary care services. Psicothema, 15, 656–661.
Vázquez, F.L., Blanco, V., & López, M. (2007). An adaptation of the Center for Epidemiologic Studies Depression Scale for use in non-psychiatric Spanish populations. Psychiatry Research, 149, 247-252. doi:10.1016/j.psychres.2006.03.004
Vázquez, F.L., Torres, A., & Otero, P. (2009). CSQ-8 Castilian (TMS.110). Retrieved from http://www.csqscales.com/
World Health Organization (2000). Evaluation of psychoactive substance use disorder treatment. Workbook series. Workbook 6: Client satisfaction evaluations. Retrieved from http://www.who.int/substance_abuse/publications/psychoactives/en/. Archived at http://www.webcitation.org/6hJHR7BsS on 6 May 2016.
Zemke, R. (1999). Service recovery: Turning oops into opportunity. In R. Zemke & J. A. Woods (Eds.), Best Practices in Customer Service (pp. 279–288). New York: AMA Publications.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The author declared no conflicts of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Vázquez, F.L., Torres, Á., Otero, P. et al. Psychometric Properties of the Castilian Spanish Version of the Client Satisfaction Questionnaire (CSQ-8). Curr Psychol 38, 829–835 (2019). https://doi.org/10.1007/s12144-017-9659-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12144-017-9659-8