
Abstract
Adequate protein consumption in amount, food sources, and meals is important to maintain muscle mass and reduce the risk of sarcopenia in older adults. This study aimed to assess protein intake in terms of the amount consumed, food sources, and meals in a sample of 295 community-dwelling older adults in a city in southeastern Brazil. Protein intake was assessed in grams/day and the amount consumed per meal and food sources were calculated using the total value and relative contribution. Adequate protein consumption was considered 0.66 g/kg/day (Estimated Average Requirement-EAR) and amount per meal 25 g, as recommended by the PROT-AGE Study Group. Descriptive analysis was based on central trend and dispersion measures. Average protein intake was 67 g and 1.05 g/kg, with an 8.5% prevalence of inadequacy. The meal that provided the largest protein contribution was lunch and 98% of the group showed insufficient intake at breakfast. Concerning food sources, the greatest contribution came from the meat group (47.3%). The results indicated that median intake was at the lower end of the range recommended by PROT-AGE, with about 50% of subjects consuming less than 1.0 g/kg/day. Protein distribution among meals showed a high prevalence of adequate consumption, breakfast being the most critical meal. Strategies to optimize protein intake should consider the amount, quality, and distribution of protein consumed at meals that form part of a balanced healthy diet, in addition to dietary techniques and supplementation, to achieve maximum protein synthesis capacity.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The ageing process is characterized by physiological changes and nutrition plays a vital role in managing complex, chronic conditions in older adults, such as sarcopenia and frailty. In this respect, adequate protein intake is important in preventing loss of muscle mass and strength (Sandoval-Insausti et al., 2016; Coelho-Junior et al., 2018; Fancelli et al., 2018).
The most widely used protein recommendation for older adults is 0.8 g/kg/day, which is the same as for adults, regardless of sex (DRI, 2005). Study groups such as the ESPEN Expert Group report that consumption between 1.0 and 1.5 g/kg/day favors anabolism and helps preserve muscle tissue in the presence of chronic conditions and inflammation though (Deutz et al., 2014; Layman et al., 2015).
In addition to daily protein intake, fractionation and the amount consumed per meal are also important because ageing compromises protein synthesis ability. When compared to young adults, older adults exhibit anabolic resistance due to the reduced availability of dietary amino acids. To optimize postprandial muscle protein synthesis, the PROT-AGE study group and other authors recommend consuming 25 to 30 g of protein in three main meals (Bauer et al., 2013; Tome, 2018). The PROT-AGE study group recommends an average daily intake of at least 1.0 to 1.2 g protein per kilogram of body weight per day, and protein quality and timing of ingestion. For timing and amount of intake, older individuals appear to have a higher per-meal protein threshold to promote anabolism (i.e., 25 to 30 g protein per meal containing about 2.5 to 2.8 g leucine).
The type of food source may influence postprandial amino acid availability and protein anabolism. Animal sources provide high-quality protein, whereas the amino acid composition of plant-based proteins needs to be balanced (van Vliet et al., 2015). To overcome the anabolic resistance, it has been suggested that 25 to 30 g of dietary protein per meal is required to allow and appropriate the stimulation of postprandial muscle protein synthesis and prevent or treat sarcopenia (Gaytán-González et al., 2020; Tieland et al., 2015).
Greater knowledge about protein intake in older adults will support nutritional strategies for preventing and treating conditions related to adequate consumption. This study aimed to assess protein intake in community-dwelling older adults in terms of the amount consumed, sources and mealtime distribution.
Methods
Type of Study and Sample
A descriptive cross-sectional study was carried out in a non-probability sample of older adults. The sample size was determined according to the method of Hair et al. (2010) which establishes the minimum number of individuals equal to five times the number of food items studied. In addition, a sample of at least 288 individuals was estimated for multivariate regression analysis with a 95% confidence level and 5% sampling error, plus 10% for possible losses.
The study was conducted between February 2014 and 2015, with 295 community-dwelling older adults of both sexes, aged 60 years or older, from a city in southeastern Brazil. The municipality studied (São Caetano do Sul) has the best Human Development Index (HDI) in Brazil, classified as high (0.862), similar to cities in the South and some Brazilian capital cities, as well as to developed countries. The present study was approved by the Research Ethics Committee of Universidade São Judas Tadeu (São Judas Tadeu University) under number 24855113.6.0000.0089.
The inclusion criteria were: (1) being aged 60 years or older; (2) not experiencing significant weight loss in the last few months; (3) not being on a diet plan for weight change; and (4) not having a disease or taking drugs that have an impact on their diet. This study was approved by the Health Municipal Foundation and São Judas Tadeu University Institutional Reviewer Boards and all participants provided written informed consent. This cross-sectional study is following the STROBE statement to provide detailed information on the study design and sample characteristics.
Data Collection
Trained researchers collected the data. Food intake was evaluated using the 24-h dietary recall method (24HR). The 24HR was conducted in an in-depth interview and detailed data about food, preparation methods, ingredients used in mixed dishes, and the brand name of commercial products. The amounts of each food consumed were estimated in relation to a common size container, standard measuring cups, and spoons, a three-dimensional food model, or two-dimensional aids such as photographs. Participants were instructed to write down all the food they consumed the day before the interview to reduce their risk of forgetting during the 24HR collection. All days of the week and months of the year were considered, in addition to the variability of dietary patterns in the different seasons. The Nutrition Data System for Research® (NDS-R) software was used to calculate energy and nutrient intake. The Multiple Source Method® (MSM) (Harttig et al., 2011) was applied to estimate habitual consumption. For this purpose, a repeated measure of the 24HR was collected (30% of the sample) within a maximum of 15 days after the first one.
Protein intake was calculated based on the total consumed per day in grams (g) and grams per kilogram of weight (g/kg). For the latter, weight was adjusted via the body mass index (BMI) (Berner et al., 2013; Mendonça et al., 2018, 2019) to minimize over or underestimation in malnourished or overweight individuals. BMI was classified according to PAHO (Pan American Health Organization) cutoff points (Lebrão et al., 2003). Inadequate protein intake was calculated based on the DRI (Dietary Reference Intake) of the Institute of Medicine/Food and Nutrition Board, considering a cutoff value of 0.66 g/kg/day for the estimated average requirement—EAR (DRI, 2005).
Protein was evaluated according to sex, age (60 to 70 years and ≥ 71 years), and meal. Meals were categorized into breakfast, lunch, dinner (main meals), and between-meal snacks (sum of all the snacks consumed throughout the day). A minimum value of 25 g was adopted to assess the adequacy of protein intake in the three main meals, in line with the PROT-AGE study group [Bauer et al., 2013).
The relative contribution (RC) of protein from the different food sources was calculated using the formula developed by Block) (Block et al., 1986) (RC = total protein (g) in the food item × 100 / total protein (g) from all the food sources). To that end, the food sources were categorized as plant or animal and into groups (subgroups): meat (red, white, processed); eggs; dairy (milk, cheese, yogurt); legumes; nuts and oilseeds; cereals (baked goods, rice and other grains, pasta); candy; fruit; vegetables and tubers; and others.
Analysis
Descriptive analysis was based on central trend and dispersion measures. The Kolmogorov–Smirnov test was applied to analyze the normality distribution of the variables and the Mann–Whitney test for group comparison and Cochran-Armitage for meals comparison. The data were submitted to statistical analysis using STATA® 12.0 software (Data Analysis and Statistical Software 12.0, Texas, USA), at a 5% significance level.
Results
Descriptive Analysis
Participants were 295 older adults, 85% of whom were women, 51.9% aged 71 years or older, 44.7% married, 74.6% living with a partner, 41.7% with up to four years of schooling, and 61.0% retired (data not shown). Table 1 shows the frequency distribution between meals and the amount of protein (> or < 25 g/meal) (p < 0.0001).
Food Intake
Consumption of all the nutrients was higher among men (p < 0.05), whereas the percentage distribution of energy, carbohydrate, fat, and protein intake was similar between the sexes. The ratio of animal to plant protein for both sexes was approximately 2:1. As shown in Table 2, protein intake (g/kg) was higher than recommended (0.8 g/kg) for the total population and both sexes from the 25th percentile onwards. 21.7% of participants exhibited lower-than-recommended protein consumption (g/kg) though, with a prevalence of 8.5%, that is, habitual consumption was below 0.66 g/kg (EAR) in 25 older adults.
Figure 1 indicates that lunch was the meal with the highest daily protein contribution. Protein distribution between meals was similar (p > 0.05) for the total population and both sexes. Animal protein accounted for approximately 75% of lunchtime intake, 65% at dinner, 55% for breakfast, and at least 45% for snacks, regardless of age or sex (data not shown).

Protein breakdown by meal, total sample
Concerning protein intake according to age, there were no differences between ranges assessed for either sex (p > 0.05). When the same age ranges were compared between the sexes though, protein intake was higher among men ≥ 71 years old in all meals and among men up to 70 years old only at dinner (Table 3). Considering the parameter of 25 g of protein per meal, almost all (98%) participants in both age groups exhibited low consumption at breakfast, with values of 29.8 and 37.5% at lunch and 66.9 and 68.4% at dinner for those up to 70 years old and ≥ 71 years, respectively (data not shown).
Table 3 shows the relative contribution (RC) of protein from different food sources. Animal proteins predominated, with meat ranked first, second, and fifth, accounting for 47.3% of daily protein intake. The dairy group was also an important source of protein, corresponding to around one-fifth (18.6%) of total consumption. The baked goods subgroup ranked third at 12.0% of daily intake, plant proteins being the most representative.
Considering frequency (number of times the food was cited) and the average portion of foods with RC > 5%, citations for the meat group (n = 425) surpassed the number of 24HRs collected, indicating that it was mentioned more than once in the same interview. Concerning dairy, although milk showed a high frequency (68% of 24HRs), the average portion of those who consumed was less than one glass (200 mL) a day. High frequency was also observed for the baked goods subgroup (75.4% of 24HRs). Despite their low RC (< 5%), legumes, rice, and other grains were mentioned in more than 57% of 24HRs (Table 4).
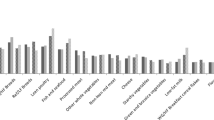
The RC values of dietary protein differed between meals, with 54% for breakfast and 44% for between-meal snacks. The highest RC was recorded for dairy, particularly milk, with a similar value obtained by the baked goods subgroup in both meals cited. The relative contribution of fruit was also representative (9.8%) for between-meal snacks. For lunch and dinner, the RC values for the meat group were 71 and 56%, respectively. Legumes and the rice and other grains subgroup were also prominent contributors for lunch (RC > 5%), and the baked goods and cheese subgroups for dinner (Fig. 2).

Relative contribution by meal, total sample
Discussion
With respect to amount, the study sample achieved the current protein recommendations in grams and g/kg from the 25th percentile onwards; the median of 1.0 g/kg demonstrates that 50% of the older adults consumed less than the minimum recommended by PROT-AGE though. Above-recommended protein intake may protect against the loss of lean muscle mass inherent to ageing. A meta-analysis by Coelho-Junior et al. (2018) and cohort study by Otsuka et al. (2019) concluded that high protein intake is inversely related to frailty in older adults, even among very old adults, as demonstrated by Mendonça et al. (2019) after a five-year follow-up.
Daily protein intake was similar to that observed in other studies with older adults from different countries (Tieland et al., 2015; Farsijani et al., 2017; Fanelli et al., 2018; ten Haafi 2018b; Ram et al., 2020), and very old adults (Mendonça et al., 2018). These findings suggest the practical viability of dietary protein intake above current recommendations, as suggested by study groups.
Despite the results cited, protein intake was below recommended levels in 21.7% (0.8 g/kg), at a prevalence of 8.5%, that is, less than 0.66 g/kg (EAR). It is important to identify the factors associated with low protein intake to promote timely interventions. A preliminary study with this same population found lower protein consumption among women and older adult individuals with a worse quality diet, who omitted one of the main meals, exhibited symptoms of dysphagia or dyslipidemia, had a lower income or schooling level, among homemakers when compared to economically active older adults, and among obese in relation to normal-weight older adults (Gaspareto et al., 2017).
Dietary protein can be either plant or animal-based, which influences amino acid composition. Animal proteins were the greatest contributor, with 69% for both sexes, higher than the values reported in other studies (50 and 65%) (Tieland et al., 2015; Huang et al., 2016; ten Haaf et al., 2018a, 2018b).
Regarding the foods that most contributed to daily protein intake, as expected, red meat ranked first (21.8%), followed by white meat (18.4%), usually chicken, and dairy (milk, cheese, and yogurt) with 18.6%, corroborating the findings reported for older adult Americans (Berner et al. 2013). The baked goods subgroup had the third-largest contribution, with 12% of total protein consumption. Tieland et al. (2012) and Tieland et al. (2015) observed a low overall contribution from meat among Dutch older adults, with a greater contribution by bread and milk, at up to 19 and 30% of their protein intake, respectively.
Animal proteins were the largest contributor in several populations; variations can be explained by the cultural and eating habits of each country. In the case of Brazil, the predominance of agriculture and size of the country, with a large amount of land available for this purpose, ensure better access to beef and other livestock.
Processed meat had the fifth-highest protein contribution (7%), with an average consumption of 45.5 g in 42% of the older adults studied. This result is worrisome given the health problems linked to excessive consumption of these products, known for their high sodium and saturated fat content. De Carvalho et al. (2014) highlighted the overconsumption of red and processed meat, with the World Cancer Research Fund recommending a maximum intake of 500 g a week to reduce the risk of cancer.
Plant-based sources usually contain less protein, meaning that larger portions are needed to achieve the same amount. In this respect, it is important to note that vegetarian diets or limited consumption of animal proteins could make it difficult to reach the required daily intake. There was no difference in muscle protein synthesis and strength among the older adults who consumed a large amount of protein though, with one group eating largely animal proteins and the other plant-based proteins (Huang et al., 2016; van Vliet et al., 2015).
The type of meal also influences the amount of animal or plant proteins consumed, as certain foods are more characteristic in specific meals. In this study, except for between-meal snacks, all meals contained at least 50% animal protein, reaching 80% at lunch and 70% at dinner. Berner et al. (2013) reported protein intake under 50% at breakfast and slightly less than 70% for lunch and dinner.
In addition to considering the amount of protein consumed per day, the amount per meal must be sufficient to ensure better metabolic functioning; the recommended intake for older adults is at least 25 g of protein in three meals (Bauer et al., 2013). The present study revealed inadequate protein distribution among the three main meals, indicating that participants may not be achieving maximum protein synthesis capacity. This scenario tends to worsen with age, as demonstrated by Mendonça et al. (2019), who found a minimum protein intake of 20 g in only 21% of the daily meals of very old adults, more frequently at lunch.
There were no differences in protein intake between participants up to 70 years old and those aged 71 or over. Krok-Schoen et al. (2019) compared these same age groups and 45 to 59-year-olds though and found a decline in protein intake at lunch and dinner with advancing age.
The main meal with the lowest protein contribution was breakfast (18%), characterized by dairy and bread, which represent more than 80% of the protein consumed at this meal. Other authors (Farsijani et al., 2017; Krok-Schoen et al., 2019; Tieland et al., 2015) also reported low protein contribution at breakfast, with around 20% of the daily total, corresponding to less than 20 g of protein, and a larger contribution for dinner (41–45%), whereas lunch accounted for the highest protein intake in our study (48%). The inadequate distribution of proteins during meals can impact protein synthesis and maintenance of muscle mass, allowing the development of sarcopenia and physical disability in older adults.
Tieland et al. (2012) recorded an average protein intake of 19 g at lunch when the meal contained bread, rising to 39 g when a “hot meal” was eaten. This indicates the extent to which dietary patterns can affect the total protein content of meals. Corroborating this finding, in the present study, lunch exhibited the highest daily protein contribution and consisted largely of the meat and legumes groups and rice and other grains subgroup, characterizing a traditional meal. When compared with dinner, there was a larger contribution from the baked goods subgroup in third place. Additionally, the number of individuals who ate legumes, rice, and other grains in this meal fell by half, demonstrating that some subjects replaced the traditional meal with a sandwich.
Replacing a traditional meal at dinner may lead to nutrient imbalance if the meal does not contain energy sources, builders, and regulators. Ferreira et al. (2017) identified three dietary patterns in this same population, the first was referred to as “Traditional” and consisted of foods usually consumed by the Brazilian population at main meals (rice, beans, vegetables, olive oil, and chicken). The second pattern was “Pasta, pork and sweets” and the third “Coffee with milk and bread and butter”, the latter likely due to the older adults' habit of eating a sandwich at dinnertime.
A diet consisting of lean and unprocessed animal proteins combined with plant-based sources to overcome the limitations of essential limiting amino acids in the latter appears to be a good strategy in complying with recommended protein intake per day and at meals, favoring maximum muscle protein synthesis capacity.
As maximum muscle protein synthesis is obtained by ingesting at least 25 g of protein per meal, it is important to increase intake at meals with a low protein contribution, particularly breakfast. This can be achieved by including or replacing foods or taking supplements (Hayashi et al., 2020; Norton et al., 2016). Other approaches to increase nutrient intake in older populations include improving oral health, enhancing the sensory attributes of food (flavor and smell) with extra seasonings, introducing a variety of food at meals and, given the heterogeneity of the older population, clinicians and dietitians may help promote higher protein intake through personalized dietary recommendations (Krok-Schoen et al., 2019).
The use of supplements is encouraged as a short to medium-term strategy, particularly for older individuals who are unable to consume the necessary food volume or when rapid recovery of nutritional status is needed. It may not be viable in the long term though due to the costs involved and the likelihood of discontinuing use and returning to old patterns. Individualized guidance is essential to maintaining a healthy dietary pattern. In this respect, it is important to encourage the inclusion of underused dietary protein sources accessible to the population, such as dairy, eggs, and oilseeds, which can be prepared in a variety of ways for any meal.
A limitation of the study was the use of a non-probabilistic sample, which prevented the extrapolation of the data to the Brazilian population. The cross-sectional design may also be a limitation in assessing consumption, as it does not take recent changes in an individual’s diet into account. As the analyses referred to the habitual consumption of a group and data collection considered all the days of the week and months of the year though, it can be inferred that the method produced a reliable dietary pattern for the group. Another important limitation of this study is that the sample is composed mostly of women, who generally consume smaller portions, however, as they are responsible for food preparation, this may also have impacted the consumption of foods and preparations that are sources of dietary protein, mostly meats.
Instructing participants to write down the food they ate on the day before the interview to prevent them from forgetting and subsequently applying the 24HR to confirm this information and correct possible inconsistencies can be considered a strength in that it improved the quality of the survey. Another noteworthy point is adjusting protein intake in g/kg with BMI to limit under and overestimation in overweight and malnourished individuals, respectively. Some authors argue that assessing g/kg protein intake in overweight individuals without adjustment results in a high prevalence of adequate consumption, which may not be accurate (Berner et al., 2013).
Conclusion
Median intake was at the lower end of the range recommended by PROT-AGE, that is, about 50% of subjects consumed less than 1.0 g/kg/day. Protein distribution among meals showed a high prevalence of adequate consumption, breakfast being the most critical meal. Our recommendation is to increase the consumption of underused foods such as dairy, eggs, and oilseeds. Strategies to optimize protein intake should consider the amount, quality, and distribution of protein consumed at meals that form part of a balanced healthy diet, in addition to dietary techniques and supplementation, to achieve maximum protein synthesis capacity.
References
Bauer, J., Biolo, G., Cederholm, T., Cesari, M., Cruz-Jentoft, M. J. E., et al. (2013). Evidence-based recommendation for optimal dietary protein intake in older people: A position paper from the PROT-AGE Study Group. Journal of the American Medical Directors Association, 14(8), 542–559. https://doi.org/10.1016/j.jamda.2013.05
Berner, L. A., Becker, G., Wise, M., & Doi, J. (2013). Characterization of dietary protein among older adults in the United States: Amount, animal sources, and meal patterns. Journal of the Academic of Nutrition and Dietetics, 113(6), 809–815. https://doi.org/10.1016/j.jand.2013.01.014
Block, G., Hartman, A. M., Dresser, C. M., Carroll, M. D., Gannon, J., & Gardner, L. (1986). A data-based approach to diet questionnaire design and testing. American Journal of Epidemiology, 124(3), 453–469.
Coelho-Junior, H. J., Rodrigues, B., Uchida, M., & Marzetti, E. (2018). Low protein intake is associated with frailty in older adults: A systematic review and meta-analysis of observational studies. Nutrients, 10(9), 1334. https://doi.org/10.3390/nu10091334
de Carvalho, A. M., César, C. L., Fisberg, R. M., & Marchioni, D. M. (2014). Meat consumption in São Paulo-Brazil: Trend in the last decade. PLoS ONE, 9(5), e96667. https://doi.org/10.1371/journal.pone.0096667
Deutz, N. E., Bauer, J. M., Barazzoni, R., Biolo, G., Boirie, Y., Bosy-Westphal, A., Cederholm, T., et al. (2014). Protein intake and exercise for optimal muscle function with aging: Recommendations from the ESPEN Expert Group. Clinical Nutrition, 33(6), 929–936. https://doi.org/10.1016/j.clnu.2014.04.007
DRI-Dietary Reference Intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein, and amino acids (2005). Institute of Medicine. National Academy Press.
Fanelli, K. M., Pohlig, R. T., Stave, S. E., Zonderman, A. B., & Evans, M. K. (2018). Dietary protein intake and overall diet quality are associated with handgrip strength in African Americans and White Adults. Journal of Nutrition Health and Aging, 22(6), 700–709. https://doi.org/10.1007/s12603-018-1006-8
Farsijani, S., Payette, H., Morais, J. A., Shatenstein, B., Gaudreau, P., & Chevalier, S. (2017). Even mealtime distribution of protein intake is associated with greater muscle strength, but not with 3-y physical function decline, in free-living older adults: The Quebec longitudinal study on nutrition as a determinant of successful aging (NuAge study). American Journal of Clinical Nutrition, 106(1), 113–124. https://doi.org/10.3945/ajcn.116.146555
Ferreira, M. P. N., Previdelli, A. N., Freitas, T. I., Marques, K. M., Goulart, R. M. M., & Aquino, R. C. (2017). Dietary patterns and associated factors among the elderly. Revista Brasileira De Geriatria e Gerontologia, 20(4), 538–549. https://doi.org/10.1590/1981-22562017020.160115
Gaspareto, N., Previdelli, A. N., & Aquino, R. C. (2017). Factors associated with protein consumption in elderly. Brazilian Journal of Nutrition, 30(6), 805–816. https://doi.org/10.1590/1678-98652017000600012
Gaytán-González, A., Ocampo-Alfaro, M. J., Torres-Naranjo, F., Arroniz-Rivera, M., González-Mendoza, R. G., Gil-Barreiro, M., & López-Taylor, J. R. (2020). The consumption of two or three meals per day with adequate protein content is associated with lower risk of physical disability in Mexican adults aged 60 years and older. Geriatrics (basel), 5(1), 1. https://doi.org/10.3390/geriatrics5010001
Hair, J. F., Black, W. C., & Anderson, R. E. (2010). Multivariate data analysis: Global edition (7th ed.). Pearson Education.
Harttig, U., Haubrock, J., Knuppel, S., & Boeing, H. (2011). EFCOVAL consortium. The MSM program: Web-based statistics package for estimating usual dietary intake using the multiple source method. European Journal of Clinical Nutrition, 65(Suppl 1), S87-91. https://doi.org/10.1038/ejcn.2011.92
Hayashi, A. P., de Capitani, M. D., Dias, S. F., et al. (2020). Number of high-protein containing meals correlates with muscle mass in pre-frail and frail elderly. European Journal of Clinical Nutrition, 74, 1047–1053. https://doi.org/10.1038/s41430-020-0618-3
Huang, R. Y., Yang, K. C., Chang, H. H., Lee, L. T., Lu, C. W., & Huang, K. C. (2016). The association between total protein and vegetable protein intake and low muscle mass among the community-dwelling elderly population in northern Taiwan. Nutrients, 8(6), E373. https://doi.org/10.3390/nu8060373
Krok-Schoen, J. L., Jonnalagadda, S. S., Luo, M., Kelly, O. J., & Taylor, C. A. (2019). Nutrient Intakes from meals and snacks differ with age in middle-aged and older Americans. Nutrients, 11(6), E1301. https://doi.org/10.3390/nu11061301
Layman, D. K., Anthony, T. G., Rasmussen, B. B., Adams, S. H., Lynch, C. J., Brinkworth, G. D., & Davis, T. A. (2015). Defining meal requirements for protein to optimize metabolic roles of amino acids. American Journal of Clinical Nutrition, 101(Suppl), 1330S-1338S. https://doi.org/10.3945/ajcn.114.084053
Lebrão M. L., Duarte Y. A. O. (org). (2003). O Projeto SABE no Município de São Paulo: uma abordagem inicial. Brasília: Organização Pan Americana de Saúde / Ministério da Saúde; 2003. Available online: http://livros01.livrosgratis.com.br/op000002.pdf. Accessed 14 January 2020.
Mendonça, N., Granic, A., Hill, T. R., Siervo, M., Mathers, J. C., Kingston, A., & Jagger, C. (2019). Protein Intake and disability trajectories in very old adults: The Newcastle 85+ Study. Journal American Geriatric Society, 67(1), 50–56. https://doi.org/10.1111/jgs.15592
Mendonça, N., Granic, A., Mathers, J. C., Hill, T. R., Siervo, M., Adamson, A. J., & Jagger, C. (2018). Prevalence and determinants of low protein intake in very old adults: Insights from the Newcastle 85+ Study. European Journal of Clinical Nutrition, 57(8), 2713–2722. https://doi.org/10.1007/s00394-017-1537-5
Norton, C., Toomey, C., McCormack, W. G., Francis, P., Saunders, J., Kerin, E., et al. (2016). Protein supplementation at breakfast and lunch for 24 weeks beyond habitual intakes increases whole-body lean tissue mass in healthy older adults. Journal of Nutrition, 146(1), 65–69. https://doi.org/10.3945/jn.115.219022
Otsuka, R., Tange, C., Tomida, M., Nishita, Y., Kato, Y., Yuki, A., Ando, F., Shimokata, H., & Arai, H. (2019). Dietary factors associated with the development of physical frailty in community-dwelling older adults. Journal of Nutrition Health and Aging, 23(1), 89–95. https://doi.org/10.1007/s12603-018-1124-3
Ram, A., Kerse, N., Moyes, S. A., Muru-Lanning, M., & Wham, C. (2020). Dietary protein intake and determinants in Māori and Non-Māori Octogenarians. Te Puāwaitanga o Ngā Tapuwae Kia Ora Tonu: Life and living in advanced age: A cohort study in New Zealand. Nutrients, 12(7), 2079. https://doi.org/10.3390/nu12072079
Sandoval-Insausti, H., Pérez-Tasigchana, R. F., López-García, E., García-Esquinas, E., Rodríguez-Artalejo, F., & Guallar-Castillón, P. (2016). Macronutrients intake and incident frailty in older adults: A prospective cohort study. Journal of Gerontology Series A Biological Sciences and Medical Sciences, 71(10), 1329–1334. https://doi.org/10.1093/gerona/glw033
ten Haaf, D. S. M., de Regt, M. F., Visser, M., Witteman, B. J. M., de Vries, J. H. M., Eijsvogels, T. M. H., & Hopman, M. T. E. (2018a). Insufficient protein intake is highly prevalent among physically active elderly. Journal of Nutrition Health and Aging, 22(9), 1112–1114. https://doi.org/10.1007/s12603-018-1075-8
ten Haaf, D. S. M., van Dongen, E. J. I., Nuijten, M. A. H., Eijsvogels, T. M. H., de Groot, L. C. P. G. M., & Hopman, M. T. E. (2018b). Protein intake and distribution in relation to physical functioning and quality of life in community-dwelling elderly people: Acknowledging the role of physical activity. Nutrients, 10(4), 506. https://doi.org/10.3390/nu10040506
Tieland, M., Borgonjen-Van den Berg, K. J., van Loon, L. J., & de Groot, L. C. (2012). Dietary protein intake in community-dwelling, frail, and institutionalized elderly people: Scope for improvement. European Journal of Clinical Nutrition, 51(2), 173–179. https://doi.org/10.1007/s00394-011-0203-6
Tieland, M., Borgonjen-Van den Berg, K. J., Van Loon, L. J., & de Groot, L. C. (2015). Dietary protein intake in dutch elderly people: A focus on protein sources. Nutrients, 7(12), 9697–9706. https://doi.org/10.3390/nu7125496
Tome, D. (2018). Protein: What’s on in research on clinical nutrition. European Journal of Clinical Nutrition, 72(9), 1215–1220. https://doi.org/10.1038/s41430-018-0240-9
van Vliet, S., Burd, N. A., & van Loon, L. J. (2015). The skeletal muscle anabolic response to plant- versus animal-based protein consumption. Journal of Nutrition, 145(9), 1981–1991. https://doi.org/10.3945/jn.114.204305
Funding
Anima Institute of São Judas Tadeu University. The founding sponsors had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, and in the decision to publish the results.
Author information
Authors and Affiliations
Contributions
Conceptualization (NG, ANP and RCA); Formal analysis (NG and ANP); Funding acquisition (RCA); Methodology (NG, ANP and GCL and RCA); Project administration (RCA); Resources (ANP and RCA); Supervision (RCA); Writing—original draft (NG); Writing—review and editing (RCA).
Corresponding author
Ethics declarations
Conflicts of interest
The authors declare no conflict of interest.
Ethical Approval
The study was approved by the Research Ethics Committee (CAAE 24855113.6.0000.0089).
Informed Consent
Informed consent was obtained from all individual participants include in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Gaspareto, N., Previdelli, Á.N., Laurentino, G.C. et al. Protein Consumption: Inadequacy in Amount, Food Sources, and Mealtime Distribution in Community-Dwelling Older Adults. Ageing Int 48, 132–145 (2023). https://doi.org/10.1007/s12126-021-09465-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12126-021-09465-3