
Abstract
The psychosocial model of social exclusion postulates that age identity of older persons induce and sustain perceived and enacted discrimination, resulting in psychosocial disability and social exclusion. These propositions were tested by using a cross-sectional survey of 573 older persons, aged 65 years and above. The variables were measured by standardized rating scales. The results reveal age identity significantly influenced perceived (β = .762; p < .001), enacted discrimination (β = .514; p < .001), psychosocial disability (β = .588; p < .001) and social exclusion (β = .389; p < .001). Perceived discrimination significantly increased enacted discrimination (β = .314; p < .001) and enacted discrimination influenced psychosocial disability (β = .279; p < .001) and psychosocial disability increased social exclusion (β = .090; p < .05). Perceived discrimination significantly mediated the negative effect of age identity on enacted discrimination (b = .211; p < .001), psychosocial disability (b = .219; p < .001) and social exclusion (b = .073; p < .05). The conceptual model showed good data model-fit, giving evidence to conclude that this model was useful in explaining process and outcomes of social exclusion of older persons.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Identity theories in social and behavioural sciences posits that identities are embedded in social structures (Barrett, 2005, 2009; Holstein & Gubrium, 2000) and evolve through life course over historical periods (Settersten & Mayer, 1997) and emphasised the longitudinal formation of identities (Howard, 2000). The important proposition is that people have multiple intersecting identities (e.g., social, ethnic, gender, sexual, age) which are socially constructed and attached meaning to relative positions people hold in society (Turner & Stets, 2006; Howard, 2000; Tajfel & Turner, 1986; Barrett, 2005). Identity helps individuals to define themselves as a member of (age) group, which distinguish themselves from others and gives a sense of self-worth and generate awareness of self-identity as (aged) social categories (Turner & Stet, 2006).
Identities are turned negative and devalued when others challenge and reject them (e.g., age identity of older adults) results in identity threat (Schmitt et al., 2002; Stagnor et al., 2002; Steele et al., 2002). Stigmatization and discrimination are mechanisms by which identities are often devalued, challenged and distanced in social interactional milieu (Jose et al., 2016b; Varghese, 2011). The stigma disposes individuals vulnerable to identity threat and inversely influences both individual and collective self-esteem (Crocker et al., 1998). Steele (1997) posits that cultural knowledge or situational cues indicate that one’s group is devalued, marginalized and of low status, which leads to identity threats. Such threat to self is derived from the membership in such devalued groups (Tajfel & Turner, 1986).
In a seminal review of stigma, Major and O’ Brian (2005) developed an identity threat model of stigma, which postulates that owning a consensually devalued social identity itself is a stigma. It increases one’s risk of exposure to potentially stressful situations. Collective representations, situational cues and personal characteristics affect people’s appraisal of the significance of those events for their wellbeing. Identity threats occur when one appraises stigma inducing situations are potentially harmful and as exceeding the coping ability of the situational demands. It results in both voluntary (coping efforts) and involuntary (anxiety, increased vigilance and working memory loaded) responses. These responses lead to negative outcomes such as reduced self-esteem, poor health and academic under achievements.
Invariably, Varghese (2011) proposed a conceptual model on psychosocial aspects of social exclusion of dalits. The model posits that caste as a stigmatizing and discriminating social identity of dalits. Stigma has two dimensions viz., perceived and enacted. Social interactional milieu is characterized through perceived and enacted stigma that induces and sustains perceived and enacted discrimination. Persistent experience of discrimination results in a psychosocial disability, which is self-perceived by individuals and groups or ascribed to members of marginalized social groups by society and disposes its targets to social exclusion.
Locating within these premises (see Fig. 1), age identity is conceptualized as identity attached with societal stereotypes and negative socio-cultural images in older persons, thus stigmatized in itself (Major & O’ Brien, 2005; Mariyam & Jose, 2014; Jose & Meena, 2015). These stigmatized age identities are evolved through life course, through which individuals internalize the socio-cultural stereotypes and images associated with ageing and older persons and then directed to themselves when they are aged (Levy et al., 2002). Evidently, some older people who view themselves positively ironically develop a negative and stigma inducing outlook to other older persons (Barrett, 2005; Blau, 1973). Hence, we argue that age identity outweighs the positive ageing experiences to negative ageing experiences therefore, it is predominantly negative due to its stigmatized status. This study attempts to examine complex interactions of stigmatized age identity, perceived and enacted discrimination, psychosocial disability and social exclusion as shown in Fig. 1, and reflected in the guiding hypotheses in this study.
Brief Review of Literature
Ageing Self-images
Ageing self-image refers to an ageing person’s knowledge of chronological and subjective ageing (how person feel about the broad age group he/she belongs to). Ageing self-image occurs at two levels viz., personal and social images. Self-image of the aged refers to the self-attribution while social image refers to older persons’ idea about how society perceives ageing persons, especially societal attitudes, social stereotypes and cultural images (Sijuwade, 2009). The nature of self and social attitudes, social stereotypes and socio-cultural images significantly determine the quality of self and social image. The negative social images of the older persons were typically a set of behavioural prescriptions and expectations. These included older persons as forgetful, intellectually rigid, unproductive and asexual (Sijuwade, 2009). Older persons’ responses to these negative societal prescriptions were predominantly depicted in four ways: acceptance, denial, avoidance or reform (Palmore, 2003). The older persons who internalized the negative social prescriptions accept the negative self-image and act as aged. If it is contrary to their personality, the person denies their age (telling a lie about one’s age, cosmetic, use of anti-ageing products), while these may not appear useful, they erode the morale. The avoidance may result in self-imposed isolation. Hence, all these responses produce harmful effects on older persons.
The studies suggest that people of 60 to 65 years of age do not necessarily feel that they were aged but society ascribes to them the ageing status. It brings discrepancy to the self and social images of older persons. The younger people have negative image of ageing, but all ageing persons do not necessarily have negative self-image. Nonetheless, some ageing persons who view themselves positively ironically develop negative attitude to other aged persons (Blau, 1973; Kwak et al., 2014). The phenomenon of ageing is a culture sensitive since criteria for ageing vary substantially across different societies and cultures. Transition to old age is therefore identified with several factors namely chronological age, ill health, retirement, physical and mental deterioration, death of spouse, changes in social roles and grant parenthood (Sijuwade, 2009).
Older persons personalize self and social images as ageing persons and attach less importance to age identity; thus form negative age identity (Jose & Meena, 2015). Considering the critical role of age identity on successful ageing (Logan et al., 1992; Montepare & Lachman, 1989; Demo, 1992; Howard, 2000) and ongoing demographic transition due to rapidly ageing societies (Rajan, 2001; Rajan, 2006; Mandal, 2011; Agewell Foundation, 2014), we need advanced research on age identity and its influence on discrimination, psychosocial disability and social exclusion of older persons.
Discrimination
To discriminate is the innate ability of humans, which serve many psychological functions to those who discriminate (e.g., feeling superior, healthy self-esteem, and enjoying wellbeing) and the target of discrimination. When a group or individual discriminate others, it serves as a sense of personal or group identity different and superior from the discriminated, which in turn increases the sense of control over the discriminated, resulting deprivations and constraining resource access (Varghese, 2011; Jose et al., 2016a). Besides, discrimination is also used as a mechanism to punish deviant members within a social group or even a group altogether due to their stigmatized or devalued status. This discrimination is an instrument to keep away the discriminated from scare resources (Paradies, 2006; Williams et al., 1997). On the other hand, those who are discriminated face multiple forms of marginalization and deprivations, which have potential negative effect on reducing wellbeing, health and quality of life (Jose & Cherayi, 2016). This is because the discriminated are often constrained from strategic life choices, deprived from critical resources, perspectives and worldviews necessary for self expansions most fulfilling to individuals and groups (Jose et al., 2016b).
Older persons are discriminated on three important grounds viz., protection, participation and image. Protection refers to securing physical, psychological and emotional safety of older persons with regard to their unique vulnerability to abuse and ill-treatment (Agewell Foundation, 2014). Elder abuse, mistreatment and torture are the manifestation of the interpersonal violence against older persons (Jose & Cherayi, 2014). Because of discrimination at households, older persons are often gets ignored, abused and denied food and medication (Sredhanya, 2014; Mandal, 2011; Agewell Foundation, 2014). Critical factors disposing older persons to abuse and neglect at households are sometimes pathology of the abuser and/or abused (e.g., mental health issues, substance dependence), dependence of the abused upon the abuser for caring related stress (Mandal, 2011; Sredhanya, 2014).
Psychosocial Disability
The construct psychosocial disability in the context of social marginalization is defined as “individual or/and collective sense of psychosocial incompetence that restricts optimal use of individual and collective human agency to influence out-groups favourably to achieve self expansion and/or collective self expansion most fulfilling to individuals and groups” (Jose et al., 2016b). The studies that connect some aspects of psychosocial disability such as components of social integration (e.g., social relations, social ties, social cohesion etc.) and self-concept and (collective) self-esteem of older persons are associated with social exclusion (Evandrou & Glaser, 2004; Lee & Powers, 2002; Thomas, 2011). Older persons are faced with familial and social neglect (Sredhanya, 2014) and experienced exclusion when accessing services (Hoff, 2008; Jose & Cherayi, 2016, 2017), restricted physical mobility (Diener & Lucas, 1999; Shields & Wooden, 2003) increased dependence on others and cognitive decline (e.g., Abbott & Sapsford, 2005; Scharf et al., 2005; Victor et al., 2003). Hence, older persons are susceptible to develop psychosocial disability.
Social Exclusion
Social exclusion has increasingly been used in academic and policy literature to designate the multi-dimensional disadvantage (Levitas et al., 2007) faced by people at the social margins (Jose, 2014; Cherayi, Jose, & Sudhakar, 2019). Older persons are an especially at risk group for social exclusion. Age itself is not a dimension of social exclusion rather it is regarded as a risk factor for reduced income with advancement in age (Agulnik et al., 2002). Social exclusion research on older persons is relatively less, except a few in international literatures (Levitas et al., 2007). The dimensions of social exclusion for older people are poverty, health, life expectancy, fear of crime, poor housing and lack of independence, which mirrors recent analyses of social exclusion in older people (Aldridge et al., 2011). The indicators used to operationalize and measure social exclusion in older persons often results from the loss of independence viz., lack of pension, public transport, housing and promoting the need for state interventions.
Some scholars argue that age in itself is not a dimension of social exclusion; rather it acts as a risk factor for reduced income, which increases with advancing age (Agulnik et al., 2002). Age related characteristics such as disability, cognitive decline, low income and widowhood, labour market characteristics, economic decline and crime in local areas and age-based discrimination dispose older persons at risk of social exclusion (Phillipson & Scharf, 2004). Advancing age is further associated with decreasing social relationships, restricted access to service provisions and material consumption, thus age is associated with greater risk for social exclusion (Jose & Cherayi, 2016). Older persons are less likely to live with their partners, more likely to be widowed, live alone and face exclusion from civic and cultural activities. They are likely to report poor health that further restricted their independence. Older persons are likely to spend more time at home and relay more on immediate environment (Popay et al., 2008; Burns et al., 2012). Nonetheless, the studies on social exclusion in India is emerging but such studies on older people is scant (Jose & Meena, 2015; Mariyam & Jose, 2014).
Method
Using a cross sectional survey design, this study examined the suitability of psychosocial model to explain negative age identity induced discrimination, psychosocial disability and social exclusion in older persons. The universe constituted the older persons aged 65 years and more who live in the southern state of Kerala in India. The sample was defined as ‘an older person, aged 65 years and more, presently living either with family or in an institutional care from the selected districts, namely Kannur, Ernakulam and Pathanamthitta’. The study has chosen 65 years as the minimum age to participate in this study, since older persons in their 60 s were likely to be economically active and engage in familial and social roles. Therefore, such persons may not experience severe social isolation and exclusion (Cornwell & Waite, 2009).
Sample Size Estimate
To estimate the sample size for the survey, we used the following formula:
The formula is \({\text{n}}=\frac{\widehat{\text{p}}\left(1-\widehat{\text{p}}\right){\text{z}}^{2}}{{\text{ME}}^{2}}\)
Where, n is the sample size, \(\widehat{\text{p}}\) is the prior judgment of the correct value of p, which means the percentage of older people to general population. M.E is the desired margin of error. We need a margin of error less than 2.5%. Therefore, we assumed a margin of error at 2.4%. The z is the confidence interval; we have selected 90% confidence interval, which means the z score is 1.645. Where \(\widehat{\text{p}}=0.105\) (10.5%); 1-\(\widehat{\text{p}}=0.895\); z = 1.645; ME = 0.024. Thus, the calculated sample size is 507, which is rounded up into 600 for ensuring the equal proportion of sample size from three selected districts. However, the final sample size for analysis was 573 as showed in Table 1. This was because we have excluded the incomplete interviews, interviews with significant amount of missing responses (more than 5%) and outlier cases.
Sample Selection Procedure
We used multi-stage sampling procedure for this study (Bordens & Abbott, 2011; Bryman, 2008). Using this sampling procedure, two to three administrative blocks were selected from each selected district randomly as clusters. We divided these clusters into different village panchayats. About 50 per cent of the village panchayats were randomly selected by using lottery technique. We selected 50 per cent of the wards from each selected village panchayat from where we selected older persons for structured interview.
In order to operationalize the sampling procedure in detail, we divided Kerala into three geographic divisions, viz., the north, the central and the south. All districts (i.e., 14) were listed out at each division. We selected three districts one each from three geographic divisions using lottery method. The selected district from the northern division was Kannur; Ernakulam district was from the central and Pathanamthitta district was from the south. Using the state and district level database on Panchayats from the ministry of Panchayat Raj Affairs, Government of India, we developed a sampling frame through engaging multiple levels of sample selections (Polit & Hungler, 1995).
In the north zone, there were 11 block panchayats in Kannur district, which contained 81 village panchayats. From this district, we randomly selected two block Panchayats namely Edakkadu (consists of 8 village panchayats) and Peravoor block (with 7 village panchayats) constituting 15 panchayats. We selected 8 village panchayats (more than 50% representation) as the final units for the study. In the central zone, we randomly selected Ernakulam district with 14 block panchayats with 84 village panchayats. We selected 3 block panchayats namely Vypin (5 village panchayats), Kothamangalam (10 village panchayats) and Parakadave (6 village panchayats) constituting 21 village panchayats. From these 21 village panchayats, we randomly selected 10 village panchayats as the final units for the study.
In the south zone, we randomly selected Pathanamthitta district, which has 8 block panchayats. For this study, we randomly selected Ranni (9 village panchayats) and Pandalam (6 village panchayats) constituting 14 village panchayats. Among these 14 village panchayats, we randomly selected 8 village panchayats (50% representation) as the final administrative units. From such selected village panchayats, we listed out all wards (smallest units of administration).
A ward typically includes 300–500 households, thus we selected one ward randomly from the list of wards from each selected panchayat. These wards deemed as primary sampling unit where our research team has conducted a mapping exercise to identify all eligible households with older persons. In addition, we also made a list of old age homes in these selected Panchayats. This has helped us to develop an extensive ward specific sampling frame. Using a lottery technique, we selected 25–30 study participants who were contacted for interviews at their residence. Thus, this study sampled 573 older persons from three districts namely Kannur (n = 200), Ernakulam (n = 200) and Pathanamthitta (n = 173).
Measures
We used a structured interview schedule, which contained a socio-demographic profile, Age Identity Measurement Scale, Stigma and Discrimination Scale, Everyday Life Discrimination Scale, Psychosocial Disability Scale and Social Exclusion Scale for interviewers.
-
1.
Socio-demographic Profile In socio-demographic profile of older persons, we collected age in years, gender, social group affiliation, religious affiliation, education, marital status and whether older persons were economically active or not at the time of interview.
-
2.
Age Identity Measurement Scale It is a 24-item scale measures negative age identity in older persons upon four subscales using 4-point Likert type rating scale: The responses are ‘1 = strongly disagree; 2 = disagree; 3 = agree; 4 = strongly agree.’ First subscale was personalized social image, which consists of 9-items that measured collective representation of older persons in society. Second subscale was on age identity importance, which contains four items followed by relative self-image, which measure one’s own comparison of self-in relation to other age groups with four items. The last subscale is on personalized self-image, which measures internalization of social prescriptions of ageing. It consists of 7-items. Internal consistency reliability ranged from 0.72 to 0.92 with an overall coefficient alpha of 0.91. Test-re-test reliability over four-week interval ranged from IC = 0.514 to IC = 0.851 with an overall inter-class correlation coefficient of IC = 0.831. It yields evidence for construct validity with self-esteem (r = -.437) (Rosenberg, 1965), Loneliness (r = .603), Social Integration (r = -.537), Discrimination (r = .690) and Wellbeing (r = -.319).
-
3.
Stigma and Discrimination Scale We used a modified version of AIDS Stigma and Discrimination Scale (Genberg et al., 2008) to measure aspects of stigma and discrimination. It is a 22-item Likert type rating scale based on three-component model of stigmatization and discrimination (viz., shame, blame and social isolation, perceived discrimination and equity) with a high internal consistency reliability and good divergent validity. Third subscale was modified i.e., perceived discrimination to capture the study context and subsequently used. It consisted of five items with factor loadings ranging from 0.46 to 0.73 (Genberg et al., 2008) and tapped attitude to freedom and need for equal and fair treatments in society. It has an internal consistency reliability of .71. In our sample, reliability coefficient was .78. The perceived and enacted discrimination (r = .676; p < .001) were significantly correlated yielding evidence for construct validity (Berger et al., 2001; Nunnally & Bernstein, 1994).
-
4.
Everyday Life Discrimination We used a 9-item scale (Williams et al., 1997) to measure frequency of disrespects faced by older persons in everyday life. This scale included statements to which older persons were asked to indicate response with a 4-point scale ranging from 1 (strongly disagree) to 4 (Strongly agree). Total scores need to be computed, with higher scores indicating severity of discrimination. Internal consistency was 0.93. Internal reliability our sample was .88. The correlation coefficient showed a strong positive correlation between the everyday life discrimination with perceived and enacted discrimination (r = .676; p < .001) which implied evidence for construct validity.
-
5.
Psychosocial Disability Scale (Jose & Meena, 2015) A 37-item 4-point rating scale measures psychosocial disability on five sub-scales namely psychological disability, autonomy, social support, social integration and spouse support. The responses ranged from ‘strongly disagree = 01 to strongly agree = 04′. First subscale was psychological disability with 19 items that measured a range of concerns like feel shame, public attitude, feeling less good, feel isolated, feel bad, feel useless and less important due to ageing with internal consistency reliability of 0.92 (Gutman Split Half r = 0.89). In second subscale, 6-items measured freedom in terms of physical mobility, spending money for self and health for enjoying independence. Internal reliability was .86 (Guttman Split Half r = 0.76). In subscale 5-items, we measured social support with an internal reliability of .79 (Guttman Split Half r = .63). In fourth subscale, we measured social integration on five items. The items tape the aspects of feeling proud of being an older person, satisfaction with life, attitude to life and felt loved and wanted. Internal reliability was .57. In final subscale, two items measured older persons’ sense of opening up self to spouse and level of reliability on spouse in time of needs. It has internal reliability of .94 (Guttman Split Half r = 0.94).
-
6.
Social Exclusion Scale (Jehoel-Gijsbers & Vrooman, 2007) It is a 15-item instrument to measure social exclusion with 4 subscales namely material deprivation, access to social rights, normative integration and social participation. The responses were rated on a five-point Likert type rating scale with never (1) to always (5). High scores on scale indicate high level of social exclusion. Material deprivation showed a reliability coefficient of .79, access to social rights showed a reliability coefficient of .82, social participation had a reliability coefficient of .77 and normative integration was with .67. The reliability coefficient of the overall scale was .85.
Data Analysis
Analysis progressed through several progressive steps as follows: First, we edited the data, processed and transformed based on the factors of the standardized scales. Missing responses were dealt either with deletion of interviews (more than 5% responses missing) or mean substitution (if 5 percent or less). We deleted 27 cases due to significant missing responses, which represent 4.5% of the total 600 interviews. We used mean substitution upon 2–5 variables in four cases. Secondly, we followed three methods to assess the normal distribution of both test and control variables viz., Kolmogorov–Smirnov and Shapiro–Wilk tests and individually assessing QQ Plot. Both tests of normality showed non-significant values at p < .05, indicating both test and control variables were approximately normally distributed. Then we analysed socio-demographic data by using frequency, percentile, mean and SD. The structural relationships between measured variables (MVs) in the model were tested after controlling for socio-demographic variables namely age, gender (1 = female), caste (1 = high caste), education and marital status (married = 1).
Fourthly, we used ‘maximum likelihood method’ for structural modelling and used R matrix (R) due to two important reasons. In this structural modelling, we used measured variables (MVs) instead of latent variables (LVs) for path analysis and the data were produced through cross-sectional design. Thus, the analysis does not address variances in variables over time. If latent variables were standardized and model was fit to R-matrix, then the parameter estimates can be interpreted as standardized variables (MacCallum & Austin, 2000).
We anticipated our own probable prejudice to confirm the model being evaluated or the confirmation bias (Greenwald et al., 1986). In order to control this, we considered specifying alternate explanations of data through developing equivalent models (Macallum et al., 1993) since we believed that ruling out the existence or meaningfulness of such equivalent models strengthen the support of a favoured model (MacCallum & Austin, 2000). Hence, we examined the reverse causality in the relationship between negative age identity and social exclusion, by considering social exclusion as independent variable discrimination and psychosocial disability leading to negative age identity as cross-lagged model (Gollob & Reichardt, 1991; Lin & Wu, 2011). Nonetheless, these reverse relationships were not significant, therefore the specified model with two additions of (perceived discrimination to enacted discrimination, age identity and social exclusion) were accepted as final model.
Finally, we used three criteria to assess the data-model fits for this analysis. These were Chi-square test, Comparative Fit Index (CFI), the root means square error of approximation (RMSEA). A non-significant Chi-square test (p > .05) implies good model fit. CFI values greater than .9 indicates an acceptable fit as do RMSEA of less than .06 (Tabachinck & Fidell, 2007; MacCallum et al., 1996).
Ethical Considerations
Informed oral consent was obtained from each study participant with a view to protect their rights either to participate or to decline participation after informing the study purpose and nature of participation.
Results
Sample Characteristics
Table 2 shows the socio-demographic characteristics of older persons. Out of 573 older persons, 61.2% were women, mean age was 75.5 years with SD of 7.6 years. Nearly 87% were from forward castes and 57.5% were Hindus. The mean years of education was 4.3 years with SD of 3.1 years. Nearly 57% were previously married and 13.6% were economically active at the time of interview. In older persons’ living status, 87.5% were living either with spouses or children, 6.2% were living alone and 6.2% were living in care facilities.
Testing the Structural Model
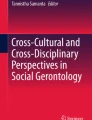
Figure 2 and Table 3 show parameter estimates with standardized path coefficients. The overall conceptual model was tested for data model-fit (X2(689, N = 573; df 2, p = .709). GFI = 0.999, AGFI = 0.995 and CFI = 0.999 with RMSEA = 0.001. Figure 1 and Table 3 show standardized path coefficients in final model. Parameter estimates show that negative age identity significantly increased perceived discrimination (β = .762; p < .001) and enacted discrimination (β = .514; p < .001). Negative age identity significantly increased psychosocial disability (β = .588; p < .001) and social exclusion (β = .389; p < .001). Perceived discrimination significantly increased enacted discrimination (β = .314; p < .001) but shows a non-significant effect on psychosocial disability (β = .025; p > .05). Enacted discrimination significantly increased psychosocial disability (β = .279; p < .001) whereas psychosocial disability increases social exclusion (β = .090; p < .05).

shows psychosocial model of social exclusion

Structural equation modelling. All coefficients are standardized *p < .05, **p < .01, and ***p < .001
In short, age identity acts as a significant source of perceived and enacted discrimination, psychosocial disability and social exclusion. Perceived discrimination intensified enacted discrimination, although it did not directly severe psychosocial disability. Nonetheless, enacted discrimination intensified psychosocial disability and social exclusion.
The analysis of mediated effect reveals (not shown in table) that perceived discrimination significantly mediated effect of age identity on enacted discrimination (b = .211; p < .001) and psychosocial disability (b = .219; p < .001). Invariably, perceived discrimination significantly mediated effect of age identity on social exclusion (b = .073; p < .05). The enacted discrimination significantly mediated effect of perceived discrimination on psychosocial disability in older persons (b = .088; p < .05). Nevertheless, psychosocial disability did not significantly mediate the effect of perceived discrimination on social exclusion (b = .010; p > .05). In short, negative indirect effect of age identity was significant upon enacted discrimination and psychosocial disability, whereas enacted discrimination significantly mediates an increasing effect of perceived discrimination on psychosocial disability.
Table 3 shows that some controlled variables were significantly associated to dependent variables. Interestingly, advancing age was inversely associated to perceived discrimination (β = -.084; p < .05) but increasing psychosocial disability (β = .046; p < .05). As expected, caste showed a significant inverse association to social exclusion (β = -.144; p < .01). All these associations were consistent with previous study findings (Jose & Cherayi, 2014; Kwak et al., 2014; Levy et al., 2002).
Discussion
Precisely, after controlling for age, gender, education, caste and marital status of older persons, age identity acted as a significant source of perceived and enacted discrimination. Age identity significantly increased perceived and enacted discrimination, psychosocial disability and social exclusion. Perceived discrimination significantly increased enacted discrimination but did not show such influence on psychosocial disability. Enacted discrimination significantly increased psychosocial disability whereas psychosocial disability directly increased social exclusion in older persons.
Enacted discrimination significantly mediated the negative effect of age identity on psychosocial disability. Age identity increased perceived discrimination but perceived discrimination in turn did not significantly explain psychosocial disability. Nonetheless, perceived discrimination significantly increased enacted discrimination, which has a significant worsening effect on psychosocial disability. Psychosocial disability significantly mediated the negative effect of age identity upon social exclusion. The perceived discrimination significantly mediated negative effect of age identity on enacted discrimination, psychosocial disability and social exclusion. Enacted discrimination significantly mediated the effect of perceived discrimination on psychosocial disability but psychosocial disability did not mediate the effect of perceived discrimination on social exclusion.
We tested the indirect effect of age identity through perceived and enacted discrimination upon psychosocial disability. The modelling suggests that the enacted discrimination significantly mediated effect of age identity upon psychosocial disability, which further worsened social exclusion in older persons. Nonetheless, perceived discrimination did not significantly mediate the effect of age identity upon psychosocial disability, despite the fact that the age identity significantly increased perceived discrimination in older persons. Studies using multivariate regression analyses explained an increasing effect of age identity upon stigma and discrimination (Jose & Meena, 2015; Mariyam & Jose, 2014; Varghese, 2011). Hence, these findings advance literature since relatively little was systematically studied about the pathway interactions of age identity, discrimination and psychosocial disability upon social exclusion.
Age identity’s mediating effect on psychosocial disability through enacted discrimination reduced older persons’ agency and ability to access necessary resources within families, communities and in larger society. These findings were consistent with the theoretical argument that identity threat (Major & O’ Brien, 2005) negative identity substantially disable its targets psychosocially, which in turn resulted in compromised agency and ability for collective self-expansion (Jose et al., 2016b). In addition, discrimination disposes older persons vulnerable to perceived and ascribed rejection, distancing and social disconnections that further aggravate the psychosocial incompetence either individually or collectively or both, which significantly disabled older persons’ ability to mobilize and acquire critical resources and support from others (Jose et al., 2016b).
Hence, psychosocial disability act as a critical barrier restricting older person from social inclusion with respect to accessing necessary resources such as material, emotional and social for their wellbeing. For instance, having developed a poor self-concept and resultant poor evaluation of self in the context of ageing self limit older persons from approaching others, acquiring support (social and emotional) which was important for wellbeing (Jose et al., 2016b). Plausibly, this belief is mediated by negative ageing experience and resultant age identity that influence older persons to self-perceive that they are bad, useless and inadequate just because they are aged. In order to address this psychosocial disability in older persons, we need comprehensive psychosocial care provisions for older persons since they were systematically incapacitated to influence resourceful others.
Situating within the present findings, we argued that negative age identity substantially shaped social exclusion in older persons. Invariably, Jose and Meena (2015) argued that poor self-concept, self-esteem and sense of control over self and environment, were likely to be associated with negative evaluation of one’s own identity. Such negative self-evaluations were likely to result in poor social integration, restricted social participation and constrained social engagement, especially outside one’ own family and age groups. Invariably, the results suggest that psychosocial disability significantly shaped social exclusion in older persons while it also mediated the negative effect of age identity on social exclusion. Age identity significantly worsen older persons’ psychosocial disability which in turn significantly incapacitated them from influencing others in favour for securing social support, much needed psychosocial and material resources, knowledge, perspectives and worldviews that help self-expansions and to remain normatively integrated, socially participating and enjoying basic social rights and material wellbeing; therefore, social inclusion.
In the present analysis, we controlled socio-demographic characteristics of older persons namely age, gender, caste, education and marital status. Among these variables, age was inversely associated with perceived discrimination. It indicated that as age advanced, older persons tend to reduce perceptions of discrimination. In line with Mariyam and Jose (2017), this study yielded a similar inverse association between advancing age and perceived discrimination. Invariably, advancing age was associated with increasing psychosocial disability. It was consistent with theoretical arguments (Jose et al., 2016b). Also, we found significant association between castes and social exclusion (Jose & Cherayi, 2016; Jose & Meena, 2015).
Internalization of ageing and ageing related socio-cultural expectations, including negative stereotypes and cultural images considerably reduced older persons’ personal autonomy and sense of freedom. As a result, the older persons perceived that they were less effective to take care of themselves, which resulted in increased dependence on others for everyday life needs. Poor social support and integration alongside frequent conflicts in social relationships at homes and in community considerably reduced older persons’ social participation and engagement. They were with special care and support needs, for which social care interventions may specifically be designed. Such interventions should include connecting especially vulnerable older persons to psychosocial care counselling services, local NGOs/social security and welfare benefits.
Improving social participations, facilitating access to basic social rights, adequate material wellbeing, reducing conflicts in social relations, loneliness, freedom and autonomy are critical for wellbeing in older persons. Thus, state funded psychosocial care provisions for older persons should include social support groups for older persons that break their loneliness, ensure mutual support among the group members, to integrate older people with society, improved social relations through meaningful participation and engagement in social activities. Further, connecting older persons with existing social security and welfare benefits, civil, health, justice and other important services provisions are critical where state and non-state actors interested in the welfare and wellbeing of older persons, needs to engage in. In addition, we need carefully planned strategies for improving intergenerational interactions and engagement between younger and older adults within and outside families, whereas our children, adolescents and youth are sensitized for meeting inclusion needs of older persons in familial and public spaces.
The National Policy on Senior Citizens (2011) envisages an ‘age integrated society’ through promoting the concept of ‘ageing in place.’ It is committed to age inclusive, barrier-free and age-friendly society. The Maintenance and Welfare of Parents and Senior Citizens Act, 2007 envisages to addresses the maintenance and welfare needs of the older persons including provisions for alternate care as a last resort. Reiterating these legislative as well as policy measures, the present study evidenced that age identity is inherently associated with perceived and enacted discrimination, worsening psychosocial disability and increasing social exclusion. Existing legislations and policy practices need to address the issues of stigmatized age identity through planned policy responses. It is critical to address concerns in the dominant social construction of ageing and age identity that negatively portrayed ageing and older persons. The need for positive ageing experience to older persons through positive social reframing of ageing may help in detaching perceptions and experience of stigma and discrimination associated with age identity. Nonetheless, such efforts demand multipronged policy responses to challenge existing negative socio-cultural stereotypes of ageing. We need participatory and emancipative researches within the right based framework to generate discussions in the public domain, aiming at positive portrayal of age identity and older persons.
Limitations
This model testing is based on randomly selected 573 samples, which reasonably represent social group patterns in Kerala society. However, the sample is over-represented by Christians while Muslim gets under-represented due to the concentration of the Christian religious groups in the selected study area. Since the study included older population within Kerala, the generalizability of the results may be limited to Kerala; therefore, results may be considered for this limitation. We acknowledge that age identity does not evolve all of a sudden rather it evolves over life course therefore, studying age identity and its complex interactions with other psychosocial variables, using cross-sectional data and design pose multiple limitations. We further understand and acknowledge the existence of complex intersections of multiple identities evolved over life course such as gender, caste, ethnicity and sexual identities, which may interact with age identity with unique opportunities and vulnerabilities to ageing persons. Nonetheless, using cross-sectional design allowed the evaluation of relationships between data at one point in time while it did not allow to capture auto-regressive effect as well as time lag, which poses difficulties to infer causality of the parameter estimates. In our model, we used measurement variables (instead of latent variable) of modelling in the premises that constructs are measured using standardized rating scales with established reliability and validity. This study did not examine the moderator effect of class and caste advantage, which may be examined in future studies.
Conclusion
The study evidence that negative age identity significantly shapes social exclusion of older persons with respect of increased material deprivation, poor social participation and normative integration and limited access to social rights, through complex interactions of multiple variables like mediating role of discrimination upon psychosocial disability and social exclusion. Therefore, this study concludes that the psychosocial model of social exclusion is useful to explain the complex interactions of identity, discrimination, psychosocial disability and social exclusion in older persons.
References
Abbott, P., & Sapsford, R. (2005). Living on the margins: Older people, place and social exclusion. Policy Studies, 26(1), 29–46.
Agewell Foundation. (2014). Human rights of older persons in India: a reality check. New Delhi: Agewell Foundation.
Agulnik, P., Burchardt, T., & Evans, M. (2002). Response and prevention in the British Welfare State. In J. Hills, J. Le Grande, & D. Piachaud (Eds.). Understanding Social Exclusion. Oxford: Oxford University Press.
Aldridge, H., Parekh, A., MacInnes, T. and Kenway, P. (2011). Monitoring Poverty and Social Exclusion. York: Joseph Rowntree Foundation.
Barrett, A. E. (2005). Gendered experiences in midlife: Implications for age identity. Journal of Aging Studies, 19, 163–183.
Barrett, R. W. (2009). Against All England: Regional Identity and Cheshire Writing, 1195–1656. University of Notre Dame Press.
Berger, B., Ferrans, C. E., & Lashley, F. R. (2001). Measuring stigma in people with HIV: Psychometric assessment of the HIV stigma scale. Research in Nursing and Health, 2, 518–529.
Blau, Z. S. (1973). Old age in a changing society. New View Point.
Bordens, K., & Abbott, B. B. (2011). Research Design and Methods: A Process Approach (8th ed.). McGraw Hill.
Bryman, A. (2008). Why do researchers integrate/combine/mesh/blend/mix/merge/fuse quantitative and qualitative research. Advances in mixed methods research, 87–100.
Burns, F.V., Lavoie, J, P., Rose, D. (2012). Revisiting the Role of Neighbourhood Change in Social Exclusion and Inclusion of Older People. Journal of Aging Research, vol. 2012. https://doi.org/10.1155/2012/148287
Cherayi, S., Jose, J. P., & Sudhakar, S. (2019). Children of Tribal Unwed Mothers and Their Non-Legitimate Origin: A Social Exclusion Perspective. SAGE Open, 9(2), 2158244019850041.
Cornwell, E. Y., & Waite, L. J. (2009). Measuring social isolation among older adults using multiple indicators from the NSHAP Study. Journal of Gerontology: Social Sciences, 64B(S1), i38–i46.
Crocker, J., Major, B., & Steele, C. (1998). Social stigma. In S. Fiske., D. Gilbert., G. Lindzey (Eds.), Handbook of Social Psychology, l (2) (pp-504–53), Boston, MA: McGraw-Hill.
Demo, D. H. (1992). The self-concept over time: Research issues and directions. Annual Review of Sociology, 18, 303–326.
Diener, E., & Lucas, R. E. (1999). 11 Personality and Subjective Well-Being. Well-Being: Foundations of Hedonic Psychology: Foundations of Hedonic Psychology, 213.
Evandrou, M., & Glaser, K. (2004). Family, work and quality of life: changing economic and social roles through the life course. Ageing & Society, 24, 771–791.
Genberg, B. L., Kawichai, S., Chingono, A., Sendah, M., Chariyalertsak, S., Konda, K. A., & Celentano, D. D. (2008). Assessing HIV/AIDS stigma and discrimination in developing countries. AIDS and Behavior, 12(5), 772–780.
Gollob, H. F., & Reichardt, C. S. (1991). Best methods for the analysis of change: Recent advances, unanswered questions, future directions.
Greenwald, A. G., Pratkanis, A. R., Leippe, M. R., & Baumgardner, M. H. (1986). Under what conditions does theory obstruct research progress? Psychological Review, 93, 216–229.
Hoff, A. (2008). Tackling poverty and social exclusion of older people: Lessons from Europe. Oxford Institute of Ageing Working Papers, 308: www.ageing.ox.ac.uk
Holstein, J. A., & Gubrium, J. F. (2000). The self we live by: Narrative identity in a postmodern world. Oxford University Press.
Howard, J. A. (2000). Social psychology of identities. Annual Review of Sociology, 26, 367–393.
Jehoel-Gijsbers, G., & Vrooman, C. (2007). Explaining social exclusion: A theoretical model explaining social exclusion tested in the Netherlands. The Netherlands Institute for Social Research SCP: The Hague.
Jose, J. P., Cherayi, S., & Vinod, C. (2016a). Age identity, stigma and discrimination in older persons. The Indian Journal of Social Work, 77(2), 135-160.
Jose, J. P., & Cherayi, S. (2014). Psychosocial determinants of dalit identity: Evidence from women of Tamilnadu in South India. Voice of Dalits, 7(2), 163–185.
Jose, J. P., & Cherayi, S. (2016). Age Identity, Social Exclusion and Wellbeing: Implications for Elder Inclusive Societies. Indian Journal of Gerontology, 30(2).
Jose, J. P., & Meena, K. S. (2015). An Explanatory enquiry into the ageing induced social exclusion of older persons in Kerala: Empirical validation of a psychosocial model of social exclusion: Research report submitted to Indian Council of Social Science Research. New Delhi: Dharmagiri Jeevas Social Centre: Kannur.
Jose, J. P., & Cherayi, S. (2017). Social Exclusion of Older Persons: The Role of Socio-Demographic Characteristics. Ageing International, 42(4), 447–465.
Jose, J. P. (2014). Women with non-dominant identities in India: Validation of a psychosocial model of social exclusion. PhD thesis submitted to Pondicherry University: Puducherry.
Jose, J. P., Cherayi, S., & Sadath, A. (2016b) Conceptualizing psychosocial disability in social exclusion: A Preliminary Discourse. Contemporary Voice of Dalit, 8(1), 1-14, 2016.
Kwak, M., Imgersoll-Bayton, B., & Burgard, S. (2014). Receipt of care and depressive symptoms in later life: importance of self perceptions of ageing. Journals of Gerontology, Series B: Psychological Sciences and Social Science, 69(2), 325–335.
Lee, C. L., & Powers, J. R. (2002). Number of social roles, health, and well-being in three generations of Australian women. International Journal of Behavioural Medicine, 9(3), 195–215.
Levitas, R., Pantazis, C., Fahmy, E., Gordon, D., Lloyd, E., & Patsios, D. (2007). The multi-dimensional analysis of social exclusion. University of Bristol.
Levy, B. R., Slade, M. D., Kunkel, S. R., & Kasl, S. V. (2002). Longevity increased by positive self-perceptions of aging. Journal of Personality and Social Psychology, 83, 261–270. https://doi.org/10.1037/0022-3514.83.2.261
Lin, J. S. C., & Wu, C. Y. (2011). The role of expected future use in relationship-based service retention. Managing Service Quality, 21(5), 535–551.
Logan, J. R., Ward, R., & Spitze, G. (1992). As old as you feel: Age identity in middle and later life. Social Forces, 71(2), 451–467. https://doi.org/10.1093/sf/71.2.451
MacCallum, R. C., Wegener, D. T., Uchino, B. N., & Fabrigar, L. R. (1993). The problem of equivalent models in applications of covariance structure analysis. Psychological Bulletin, 114, 185–199.
MacCallum, R. C., Browne, M. W., & Sugawara, H. M. (1996). Power analysis and determination of sample size for covariance structure modeling. Psychological Met.
MacCallum, R. C., & Austin, J. T. (2000). Applications of structural equation modeling in psychological research. Annual review of psychology, 51(1), 201–226.
Major, B., & O’Brien, L. T. (2005). Social psychology of stigma. Annual Review of Psychology, 56, 393–421.
Mariyam, S., & Jose, J. P. (2014). Age identity and social exclusion of elderly persons in Kozhikode district, Kerala: a cross sectional study. Paper presented at an ICSSR sponsored International Conference on Social Exclusion, at Mysure University, Nov 2014.
Mariyam, S., & Jose, J. P. (2017). Age Identity and Social Exclusion of Elderly Persons: A Cross Sectional Study. International Journal of Social Science, 6(3), 191-198.
Mandal, S. N. (2011). Protection of rights of oldage persons in India: A challenging facet of human rights. Global Journal of Human Social Sciences, 11(5), 1–11.
Montepare, J. M., & Lachman, M. E. (1989). You’re only as old as you feel: Self-perceptions of age, fears of aging, and life satisfaction from adolescence to old age. Psychology and Aging, 4, 73–78.
National Policy on Senior Citizens (2011).Press Information Bureau, Government of India, Ministry of Social Justice & Empowerment.
Nunnally, J. C., & Bernstein, I. H. (1994). Psychometric theory (3rd ed.). McGraw-Hill Inc.
Palmore, E. (2003). Ageism comes of age: Review Essay. The Gerontologist, 43, 418–420.
Paradies, Y. (2006). A systematic review of empirical research on self-reported racism and health, International Journal of Epidemiology, 35 (4), 888–901. https://doi.org/10.1093/ije/dyl056
Phillipson, C., & Scharf, T. (2004). The impact of government policy on social exclusion among older people. London: Social Exclusion Unit, Office of the Deputy Prime Minister.
Polit, D. F., & Hungler, B. P. (1995). Nursing research: Principles and methods (5th ed.). Lippincott.
Popay, J., Escorel, S., Hernández, M., Johnston, H., Mathieson, J., & Rispel, L. (2008). Understanding and tackling social exclusion. Final report to the WHO commission on social determinants of health from the social exclusion knowledge network.
Rajan, S. I. (2001). Social assistance for Poor Elderly: How Effective? Economic and Political Weekly, 36, 613–617.
Rajan, I. S. (2006). Kerala aging survey among old age homes. Centre for Development Studies.
Rosenberg, M. (1965). Society and the Adolescent Self-Image. Princeton, NJ: Princeton University Press.
Scharf, T., Phillipson, C., & Smith, A. (2005). Social exclusion of older people in deprived urban communities of England. European Journal of Ageing, 2(2), 76–87.
Schmitt, M. T., Branscombe, N. R., Kobrynowicz, D., & Owen, S. (2002). Perceiving discrimination against one’s gender group has different implications for well-being in women and men. Personality and Social Psychology Bulletin, 28(2), 197–210.
Settersten, Jr, R. A., & Mayer, K. U. (1997). The measurement of age, age structuring, and the life course. Annual review of sociology, 233–261.
Shields, M., & Wooden, M. (2003). Marriage, children and subjective well-being. Paper presented at the 8th Australian Institute of Family Studies Conference. http://www.melbourneinstitute.com/hilda/Biblio/hbibliocq.html
Sijuwade, P. O. (2009). Attitudes towards old age: a study of the self-image of aged. Studies on Home and Community Science, 3(1), 1–5.
Sredhanya. (2014). Abuse and neglect of elder women in Kerala: A mixed method study. PhD thesis submitted to Mahatma Gandhi University, Kerala.
Stangor, C., Swim, J. K., Van Allen, K. L., & Sechrist, G. B. (2002). Reporting discrimination in public and private contexts. Journal of Personality and Social Psychology, 82(1), 69.
Steele, C. M. (1997). A threat in the air: how stereotypes shape intellectual identity and performance. American Psychologist, 52, 613–629.
Steele CM, Spencer, S. J., & Aronson, J. (2002). Contending with group image: the psychology of stereotype and social identity threat. In M. P Zanna (Ed.). Advances in Experimental Social Psychology (Vol. 34, pp. 379–440). San Diego, CA: Academic Press.
Turner, J. H., & Stets, J. E. (2006). Sociological theories of human emotions. Annual Review of Sociology, 25–52.
Tabachnick, B. G., & Fidell, L. S. (2007). Using Multivariate Statistics (5th ed.). Allyn and Bacon.
Tajfel, H, & Turner, J. C. (1986). The social identity theory of intergroup behavior. In S. Worchel, & W. G. Austin (Ed.). The Psychology of Intergroup Relations, 7–24.
Thomas, P. A. (2011). Gender, social engagement, and limitations in late life. Social Science & Medicine, 73, 1428–1435.
Varghese, C. V. (2011). Socio-economic and cultural conditions of Dalit Christians: A case study of Chengalpattu and Trichy Taluks of Tamilnadu. PhD thesis submitted to Jamia Millia Islamia University: New Delhi.
Victor, C., Bowling, A., Bond, J., & Scambler, S. (2003). Loneliness, social isolation and living alone in later life, Research Findings 17 from the Growing Older Program. UK.
Williams, D., Yu, Y., Jackson, J., & Anderson, N. (1997). Racial differences in physical and mental health: Socio-economic status, stress and discrimination. Journal of Health Psychology, 2, 335–351.
Acknowledgment
This paper is part of a state level study funded by Indian Council of Social Science Research (ICSSR), New Delhi, with the grant ID no: 02/54/2014-15/RPR.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors have no conflict of interest to declare.
Ethical Treatment of Experimental Subjects (Animal and Human)
The project received ethical clearance from Institutional Review Board (IRB) of the Dharmagiri Jeevas Social Centre (implementing agency) specially constituted for the study.
Informed Consent
All participants were informed about the purpose of the study and oral consent was obtained from each study participants with prior to the data collection.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Jose, J.P., Cherayi, S.J. & Sudhakar, S. Age Identity and Social Exclusion of Older Persons: A Psychosocial Perspective. Ageing Int 47, 115–133 (2022). https://doi.org/10.1007/s12126-021-09409-x
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12126-021-09409-x