
Abstract
This study was conducted to determine whether there is an association between cigarette smoking, alcohol consumption and self-reported health status among older persons and how sociodemographic and socio-economic factors mediate the association between these lifestyle behaviours and health in old age. Data from wave 7 of the English Longitudinal Study of Ageing (ELSA) were analysed using bivariate and logistic regression method. Self-reported health status was assessed as a binary variable; cigarette smoking and alcohol consumption as independent variables; and age, sex, marital status, education, employment as well as financial status were assessed as covariates. Smoking had a significant inverse association with reported health status and the odds of reporting good health status versus bad health status was 59% and 38% times less for former and current smokers respectively compared with those that never smoked. However, mild alcohol consumption seemed to have a significant positive association with health status, while a negative association existed between heavy alcohol consumption and health. Sociodemographic and economic factors did not appear to mediate the effects of smoking and alcohol consumption on health status. This study provided evidence that it is important to consider interventions on smoking and heavy alcohol drinking behaviours on good health status of older adults.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Tobacco use has been closely associated with alcohol misuse and both have significant impact on the health of older adults (Schulte and Hser 2014). The health effects of heavy alcohol consumption in the context of smoking increases the risks of a person suffering greater harm. Thus, there is a synergy of effects from cigarette smoking and alcohol consumption. Research has shown that people who smoked, and consumed alcohol heavily had a cognitive decline 36% faster than people who drank alcohol moderately without smoking(Hagger-Johnson et al. 2013). Overall cigarette smoking and alcohol intake have been shown to be significantly associated with deteriorating health status and premature mortality in the general population(Scott and Happell 2011; Whitfield et al. 2018). However, there is a gap in knowledge about the extent to which these factors are associated with health in old age. Previous research show that alcohol consumption and cigarette smoking are major risk factors for admission to hospitals and chronic illness among older persons. For example, data from the United Kingdom (UK) show that alcohol-related harm is increasing among older persons and that they are more likely to exceed the recommended drink limits when compared with younger adults (Office For National Statistics 2014). Findings from other countries also indicate that heavy alcohol consumption may be a significant problem among older adults(Artaud et al. 2013; Chhatre et al. 2017; Selivanova and Cramm 2014). This tendency to engage in excessive drinking could be because they are likely to drink alone without family and friends checking on them. Also, cigarette smoking and alcohol consumption are prevalent habits among older persons in the UK despite the adverse health implications associated with these habits. The number of alcohol-related hospital admissions of older persons increased significantly between 2002 and 2010 and deaths as a result of excessive alcohol intake remains a huge problem in the UK (Office For National Statistics 2014). Smoking is also associated with an accumulation of adverse health issues that subside with smoking cessation(Mons et al. 2013).
Research has indicated that certain social, demographic and economic factors are likely to influence cigarette smoking and alcohol consumption. For example, finding from in Health Survey for England (Hiscock et al. 2012) showed that the prevalence of smoking reduced among the affluent while it remained remarkably high among the economically less privileged. Income has been shown to be positively associated with harmful alcohol intake for women but not for men whereas education is positively associated with harmful alcohol intake for both sexes in England (Iparraguirre 2015). However, a longitudinal study in the US showed that over time, affluent and highly educated people were more likely to have increasing alcohol consumption in later life, and the increasing alcohol consumers usually had a problem-drinking history and were more likely to be male, White, unmarried and less religious (Platt et al. 2010).
In addition, while studies have been undertaken on the effects of smoking and alcohol intake on the health of older persons, minimal focus have been placed on the possible mediating effects of sociodemographic and economic status. Little is known about how sociodemographic factors such as age, sex, religion, educational status, and employment as well as financial factors mediate the effects of cigarette smoking and alcohol consumption on health.
This study aims to investigate whether sociodemographic and financial factors mediate the association between these lifestyle behaviours and health among older persons who are 50 and over. Findings from this study can be helpful for policy makers and health care professionals to understand how sociodemographic and economic factors can affect any associations between cigarette smoking, alcohol intake, and health status among older adults. An understanding of these associations and effects can assist in designing preventive treatments and rehabilitative measures. This is therefore an important research focus due to the prevalence of chronic illnesses in old age and their association with smoking, alcohol intake, and overall health status.
Methods
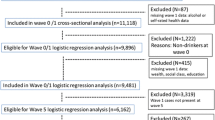
This research utilises the most recent English Longitudinal Study of Ageing (ELSA) data which is representative of the English population 50 years and over (Steptoe et al. 2013). Beginning in 2002, data collection is conducted every 2 years with self-completion questionnaires and computer-assisted personal interviews. Nurse visits are carried out every 4 years to assess biomarkers. The original sample consisted of 11,391 participants and the data set is made available to researchers on request, soon after collection (Steptoe et al. 2013). There were 9491 respondents aged 50 and above included in this study from the wave 7 of ELSA.
Health status (which is measured by ‘Hehelf’ in ELSA) was the dependent variable. It was the self-reported general health measured in an ordinal scale of five categories, which are: excellent, very good, good, fair and poor. Self-reported health has been found to be a very good predictor for an individual’s health in studies conducted in different countries (Bopp et al. 2012; Buman et al. 2010; Moreno et al. 2014). In our analysis, “excellent, very good and good” were recoded to “good health”, and “fair and poor” was recoded to “poor health”. The self-reported health was further recoded into two categories because research has shown that “fair” and “poor” responses on self-rated health can be categorized together for effective analyses (Elliott et al. 2015; Reyes-Gibby et al. 2002; Stone et al. 2015; Veenstra 2011). In addition, alternative analysis showed that grouping fair to the good health category would change the interpretation of significance of the regression results. Therefore, we decided that fair should be grouped into poor health.
Cigarette smoking and alcohol consumption were the independent variables. Smoking variable reflect on the current and retrospective smoking habit and is measured as an ordinal variable with three categories (never smoked, ever smoked and current smoker). Alcohol drinking was assessed based on the frequency of drinking during the last 12 months, i.e. almost every day, five or six days a week, three or four days a week, once or twice a week, once or twice a month, once every couple of months, once or twice a year and not at all in the last 12 months. The responses on alcohol consumption were recoded into three categories: almost every day to once a week, once a month to once a year (including any categories between “five or six days a week” to “once or twice a year”), and not at all in the last 12 months. Furthermore, individual characteristics such as age, gender, race and economic status have been found to influence cigarette smoking and the consumption of alcohol. These sociodemographic and economic variables were therefore introduced as covariates in order to assess how they influence the association between smoking, alcohol consumption and health status. There are few missing data due to some participants not providing responses to some questions.
In the bivariate analysis Chi-Square tests of the association between alcohol intake and health status as well as between smoking and health status were conducted. Kendall’s Tau was used to assess associations involving ordinal variables to determine if it was a better test of association than Chi-square.
The mediating effects of sociodemographic and economic factors on the relationship between alcohol intake, smoking and health status were assessed by bivariate and multivariate regression models. In the multivariate regression models, independent variables measuring smoking status and alcohol consumption were entered in block one; age, sex, marital status in block two; religion and ethnicity in block three; education and work status (in paid employment or not) in block four; and financial status in block five. These variables were entered into blocks in this manner in order to assess the effects of sociodemographic and economic factors on the relationship between smoking status, alcohol consumption, and health. Logistic regression method was used as the dependent variable is binary where 1 represents good health status and 0 represents poor health status.
The data were analysed using SPSS version 21 and the level of statistical significance was determined at 0.05 for all analyses. The secondary data used for this study had been anonymized, eliminating the chances of direct harm to research participants and ethical approval was obtained from the Ethics Committee of the University of Southampton.
Results
There is a high level of literacy among the respondents and almost two-third of them had at least secondary education (Table 1). Up to one-third of them were still in employment and 52.5% indicated that they ever found they have too little money to spend on their needs. Furthermore, 70.7% of the respondents had reported good to excellent health, 35.3% had never smoked, while 13.2% had not taken alcohol at all in the last 12 months. About half of the respondents were previous smokers while about a tenth were current smokers. A slightly higher proportion of the male than female participants were current smokers and similarly more men than women were former smokers. In addition, about a tenth of all respondents were daily alcohol consumers while another tenth had not taken alcohol in the preceding 12 months.
Table 2 shows the association between cigarette smoking and health status as well as between alcohol consumption and health status. About two-fifth (40.6%) of current smokers reported poor to fair general health compared to 27.6% of former smokers and 20.1% of those who had never smoked cigarettes. Also, fewer smokers had good general health as 26.8% of current smokers had very good to excellent general health compared to 38.7% of former smokers and 47.7% of those who had never smoked cigarettes. Cigarette smoking is therefore significantly associated with health status (p < 0.001).
The increase in frequency of alcohol intake appears to be associated with better self-reported general health. Almost half (46.3%) of participants who had not taken alcohol in the last 12 months compared with 28.7% of those who had alcohol once a month to once a year and 17.3% of those who consumed it once a week to almost every day had poor to fair general health. On the other hand, 22.9% of participants who had not taken alcohol in the last 12 months, 36.9% of those who had alcohol once a month to once a year and 49.2% of those who consumed it almost every day to once a week have very good to excellent general health. Alcohol consumption is also significantly associated with health status (p < 0.001).
Smoking has a significant inverse association with health status and the odds of reporting good versus poor health status is 0.593 and 0.376 times less for former and current smokers respectively (p < 0.001) compared with those that never smoked (Table 3). However, alcohol consumption seems to have a significant positive association with health status. The odds of having good health status is 2.197 times higher for those who take alcohol once a month to once a year and 4.209 times higher for those who took alcohol once a week to almost every day (p < 0.001) compared with those who had not taken any alcohol in the last 12 months. The effects of smoking and alcohol intake on health remain statistically significant all through the five models (p < 0.001).
Advancing age and male gender have a significant negative association with health status, while being married increases the odds of having good health by a factor of 1.452. Furthermore, adding the variables in this block slightly increases the odds by which smoking affected health status (OR = 0.629 for former smokers and 0.392 for current smokers) but slightly reduces the odds of alcohol consumption on health. Nevertheless, the odds remain significant. Furthermore, the odds of having good health status is 2.748 times higher for those who had a paid job while the odds of having good health is 0.574 times less for those who ever found they had too little money to spend on their needs (p < 0.001).
Discussion
More than half of the respondents (about 53.5%) have ever smoked, 11.2% are still currently smoking, and 58.2% consume alcohol almost every day to once a week; showing the prevalence of smoking and alcohol consumption in the English population aged 50 years and older. This finding is similar to what has been reported in previous studies in the UK and other countries (Allender et al. 2009; Britton et al. 2015; Chhatre et al. 2017). However, mild to moderate alcohol consumption was associated with good self-reported health. Comparably, studies previously carried out in the UK have shown that older adults who are mild to moderate consumers of alcohol tend to have less symptoms and diseases compared to their counterparts who consume heavy amounts of alcohol (Howie et al. 2011).
The younger subgroup of respondents in this study reported better health status than their older counterparts. It is possible that oldest old reported poorer health due to the increased risk of multi-morbidity, frailty and disability related to ageing (Aarts et al. 2015). Also, a significantly higher number of older adults who never lacked money and those who were employed had higher odds of reporting better health compared to those who were unemployed or retired. This may be related to the satisfaction of being engaged in stimulating activities, more physical activity which promotes good health. Employment also serve as a source of income that may help improve financial status, which has been shown to have a correlation with good health (Arber et al. 2014). In Europe, preventable causes of mortality such as cigarette smoking and alcohol have been shown to be more prevalent among people of lower education status and education-related health inequalities associated with smoking are larger among men than women (Mackenbach et al. 2015). This supports the link between low educational level, male gender and cigarette smoking, all of which have been associated with poor self-reported health. Likewise, it has been estimated that more men than women smoke cigarettes (Peters et al. 2015) and conditions associated with excess hospitalizations and mortality in men tend to be smoking-related (Case and Paxson 2005). However, education status does not significantly influence to health status in our analysis and this may be due to a high proportion of educated participants in the current study.
Cigarette smoking is significantly associated with poor self-reported health, a finding that is supported by previous research in which cigarette smoking has been associated with a higher rate of diseases and mortality (Carter et al. 2015). Even among former smokers, the risk continues to be apparent due to permanent damage to the internal organs such as the lungs. This risk in former smokers may depend on the duration of smoking and the quantity of cigarette smoked per time. The quantity and duration of cigarette smoked was not covered by any of the variables used in this study. Nevertheless, the results suggested that older adults who were current smokers had a higher risk of reporting poor health than former smokers; additionally, former smokers had a significantly higher risk compared to older adults who never smoked.
Multivariate analysis showed that a higher frequency of alcohol intake was associated with better self-reported general health. These results indicated that the frequency of alcohol consumption might have protective effect on health, which is similar to findings of previous research in England (Frisher et al. 2015) and other countries (Hamaguchi et al. 2012; Plunk et al. 2014; Scott et al. 2013). After controlling for the effects of age, sex, religion, ethnicity, education, employment, and financial status, there was no marked change in the effects of smoking and alcohol intake on self-reported health status. Therefore, there were no indications from the analysis carried out in this study that these sociodemographic and economic factors medicated the effects of smoking and alcohol consumption on self-reported health.
Although this was a cross-sectional study that do not establish causality, these results have policy implications in terms of targeting at-risk groups with specific health promotion strategies. Such strategies should be directed at lifestyle and behaviours at younger age, especially at smoking behaviours as it has destructive effects on health. In addition, since low socioeconomic status is a determinant of poor health and smoking status (Hiscock et al. 2012), it is important for policy makers to lower poverty rates among older adults. It is also relevant to consider implementing tax programs on tobacco purchase or strengthening tobacco consumer tax where they exist. Furthermore, future research can evaluate the relative efficacy of smoking cessation programs and provide guidance on the amount of alcohol consumption that imply safe drinking for older adults.
References
Aarts, S., Patel, K. V., Garcia, M. E., Van den Akker, M., Verhey, F. R. J., Metsemakers, J. F. M., Van Boxtel, M. P. J., Gudnason, V., Jonsdottir, M. K., Siggeirsdottir, K., Jonsson, P. V., Harris, T. B., & Launer, L. J. (2015). Co-presence of multimorbidity and disability with frailty: An examination of heterogeneity in the frail older population. The Journal of Frailty & Aging, 4(3), 131–138.
Allender, S., Balakrishnan, R., Scarborough, P., Webster, P., & Rayner, M. (2009). The burden of smoking-related ill health in the UK. Tobacco Control, 18(4), 262–267.
Arber, S., Fenn, K., & Meadows, R. (2014). Subjective financial well-being, income and health inequalities in mid and later life in Britain. Social Science and Medicine, 100(October), 12–20.
Artaud, F., Dugravot, A., Sabia, S., Singh-Manoux, A., Tzourio, C., & Elbaz, A. (2013). Unhealthy Behaviours and disability in older adults: Three-City Dijon cohort study. BMJ (Online), 347, f4240.
Bopp, M., Braun, J., Gutzwiller, F., & Faeh, D. (2012). Health risk or resource? Gradual and independent association between self-rated health and mortality persists over 30 years. PLoS One, 7(2), e30795.
Britton, A., Ben-Shlomo, Y., Benzeval, M., Kuh, D., & Bell, S. (2015). Life course trajectories of alcohol consumption in the United Kingdom using longitudinal data from nine cohort studies. BMC Medicine, 13(47), 47.
Buman, M. P., Hekler, E. B., Haskell, W. L., Pruitt, L., Conway, T. L., Cain, K. L., Sallis, J. F., Saelens, B. E., Frank, L. D., & King, A. C. (2010). Objective light-intensity physical activity associations with rated health in older adults. American Journal of Epidemiology, 172(10), 1155–1165.
Carter, B. D., Abnet, C. C., Feskanich, D., Freedman, N. D., Hartge, P., Lewis, C. E., Ockene, J. K., Prentice, R. L., Speizer, F. E., Thun, M. J., & Jacobs, E. J. (2015). Smoking and mortality — Beyond established causes. New England Journal of Medicine, 372(7), 631–640.
Case, A., & Paxson, C. (2005). Sex differences in morbidity and mortality. Demography, 42(2), 189–214.
Chhatre, S., Cook, R., Mallik, E., & Jayadevappa, R. (2017). Trends in substance use admissions among older adults. BMC Health Services Research, 17(584), 1–8.
Elliott, M. N., Kanouse, D. E., Burkhart, Q., Abel, G. A., Lyratzopoulos, G., Beckett, M. K., Schuster, M. A., & Roland, M. (2015). Sexual minorities in England have poorer health and worse health care experiences: A National Survey. Journal of General Internal Medicine, 30, 9–16.
Frisher, M., Mendonca, M., Shelton, N., Pikhart, H., de Oliveira, C., & Holdsworth, C. (2015). Is alcohol consumption in older adults associated with poor self-rated health? Cross-sectional and longitudinal analyses from the English longitudinal study of ageing. BMC Public Health, 15, 703.
Hagger-Johnson, G., Sabia, S., Brunner, E. J., Shipley, M., Bobak, M., Marmot, M., Kivimaki, M., & Singh-Manoux, A. (2013). Combined impact of smoking and heavy alcohol use on cognitive decline in early old age: Whitehall II prospective cohort study. The British Journal of Psychiatry, 203(2), 120–125.
Hamaguchi, M., Kojima, T., Ohbora, A., Takeda, N., Fukui, M., & Kato, T. (2012). Protective effect of alcohol consumption for fatty liver but not metabolic syndrome. World Journal of Gastroenterology, 18(2), 156–167.
Hiscock, R., Bauld, L., Amos, A., & Platt, S. (2012). Smoking and socioeconomic status in England: The rise of the never smoker and the disadvantaged smoker. Journal of Public Health (United Kingdom), 34(3), 390–396.
Howie, E. K., Sui, X., Lee, D.-c., Hooker, S. P., Hébert, J. R., & Blair, S. N. (2011). Alcohol consumption and risk of all-cause and cardiovascular disease mortality in men. Journal of Aging Research, 2011, 1–10.
Iparraguirre, J. (2015). Socioeconomic determinants of risk of harmful alcohol drinking among people aged 50 or over in England. BMJ Open, 5(7), e007684.
Mackenbach, J. P., Kulhánová, I., Bopp, M., Deboosere, P., Eikemo, T. A., Hoffmann, R., Kulik, M., Leinsalu, M., Martikainen, P., Menvielle, G., & Regidor, E. (2015). Variations in the relation between education and cause-specific mortality in 19 European populations: A test of the ‘fundamental causes’ theory of social inequalities in health. Social Science & Medicine, 127, 51–62.
Mons, U., Schöttker, B., Müller, H., Kliegel, M., & Brenner, H. (2013). History of lifetime smoking, smoking cessation and cognitive function in the elderly population. European Journal of Epidemiology, 28, 823–831.
Moreno, X., Huerta, M., & Albala, C. (2014). Global self-rated health and mortality in older people. Gaceta Sanitaria, 28(3), 246–252.
Office For National Statistics. 2014. Alcohol-Related Deaths in the United Kingdom , Registered in 2012. Office for National Statistics Statistical Bulletin (February):1–26.
Peters, S. A. E., Huxley, R. R., & Woodward, M. (2015). Do smoking habits differ between women and men in contemporary Western populations? Evidence from half a million people in the Uk biobank study. BMJ Open, 4(12), e005663.
Platt, A., Sloan, F. A., & Costanzo, P. (2010). Alcohol-consumption trajectories and associated characteristics among adults older than age 50. Journal of Studies on Alcohol and Drugs, 71(2), 169–179.
Plunk, A. D., Syed-Mohammed, H., Cavazos-Rehg, P., Bierut, L. J., & Grucza, R. A. (2014). Alcohol consumption, heavy drinking and mortality: Re- thinking the J-shaped curve. Alcoholism, Clinical and Experimental Research, 38(2), 471–478.
Reyes-Gibby, C. C., Aday, L. A., & Cleeland, C. (2002). Impact of pain on self-rated health in the community-dwelling older adults. Pain, 95(1–2), 75–82.
Schulte, M. T., & Hser, Y. I. (2014). Substance use and associated health conditions throughout the lifespan. Public Health Reviews, 35, 2.
Scott, D., & Happell, B. (2011). The high prevalence of poor physical health and unhealthy lifestyle Behaviours in individuals with severe mental illness. Issues in Mental Health Nursing, 32(9), 589–597.
Scott, I. C., Tan, R., Stahl, D., Steer, S., Lewis, C. M., & Cope, A. P. (2013). The protective effect of alcohol on developing rheumatoid arthritis: A systematic review and meta-analysis. Rheumatology (United Kingdom), 52, 856–867.
Selivanova, A., & Cramm, J. M. (2014). The relationship between healthy behaviors and health outcomes among older adults in Russia. BMC Public Health, 14(1183), 1–13.
Steptoe, A., Breeze, E., Banks, J., & Nazroo, J. (2013). Cohort profile: The English longitudinal study of ageing. International Journal of Epidemiology, 42(6), 1640–1648.
Stone, J., Evandrou, M., Falkingham, J., & Vlachantoni, A. (2015). Women’s economic activity trajectories over the life course: Implications for the self-rated health of women aged 64+ in England. Journal of Epidemiology and Community Health., 69, 873–879.
Veenstra, G. (2011). Race, gender, class, and sexual orientation: Intersecting axes of inequality and self-rated health in Canada. International Journal for Equity in Health, 10(1), 3.
Whitfield, J. B., Heath, A. C., Madden, P. A. F., Landers, J. G., & Martin, N. G. (2018). Effects of high alcohol intake, alcohol-related symptoms and smoking on mortality. Addiction, 113(1), 158–166.
Funding
This research didn’t receive grants from any funding agency in the public, commercial or not-for-profit sectors.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
All the authors declare no conflict of interests.
Informed Consent
Not applicable
Ethical Treatment of Experimental Subjects (Animals and Humans)
No experimental treatment was conducted on either human or animal subjects in this study
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Atoyebi, O.A., Langat, G.C. & Xiong, Q. Cigarette Smoking, Alcohol Intake and Health Status of Older Persons in England: the Mediating Effects of Sociodemographic and Economic Factors. Ageing Int 45, 380–392 (2020). https://doi.org/10.1007/s12126-020-09395-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12126-020-09395-6