
Abstract
Japan has one of the highest longevity rates and the second highest average effective age of retirement within the OECD. To face declining birth-rates and growing labour shortage, the Japanese government made the choice to postpone retirement ages. However, an important part of the ageing workforce is in non-standard employment such as part-time, temporary or contract work. The potential health impact of such transitions has not been analysed so far. Using four waves from the Japanese Study of Aging and Retirement (JSTAR), this article assesses, using a latent growth curve method, the impact of moving to non-standard employment in late career on general and mental health for the population aged 50 to 75 after controlling for fixed and time-varying covariates. Analyses are replicated separately by gender. Mixed results flow from the study. Those keeping being in non-standard employment have a better health than those working in full-time employment. However, moving from full-time employment to non-standard employment has negative effects on mental health, particularly for women.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Background
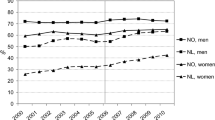
The age at which the older workforce leaves the labour market has drastically increased over the past twenty years in most OECD (Organisation for Cooperation and Development Economics) countries. In 1997, the average effective age of retirement was 63.2 years old for men and 61.3 for women within the OECD. Twenty years later, it is respectively 65.3 and 63.6 (for the calculation detail, please see Keese n.d.; Wels 2016). Nevertheless, important differences are observed across countries. For instance, in 2017, the male average age of retirement was 60.5 years old in France, 65 in the United Kingdom and 70.6 in Japan. In comparison, women were leaving the labour market respectively at 60.6, 63.9 and 69.3 years old. In other words, there is a gap of about ten years between OECD countries and important national differences between men and women. Increasing the age at which workers leave the labour market is not without consequences, particularly regarding the health of the older workforce. This raises concerns about the potential effects postponing the retirement age would have on older workers’ health. An extensive amount of research was recently carried out on this topic, particularly using longitudinal methods that are suitable for assessing such an association, but a consensual view on this matter has not been reached yet (Hashimoto, 2015): results vary from one study to another, from one country to another and show a huge heterogeneity depending on the types of variables that are taken into account.
The Impact of Late Career Transitions on Health
The impact of late career transitions on health is subject to a considerable – but still relatively new – amount of research using longitudinal methods. Among the different possible transitions, many studies have focused on the impact of the transition from work to retirement, unemployment and inactivity on health (Bell & Jones, 2015; Graetz, 1993; Rice, Lang, Henley, & Melzer, 2011; Waddell & Burton, 2006) but also on work or family care histories (Benson et al., 2017; Corna & Sacker, 2013; Wahrendorf, 2015). So far, a consensual view on this matter has not been reached (Hashimoto, 2015). Some research has found a negative association between retirement transitions and post-retirement health (see for instance: Alavinia and Burdorf 2008; Moon et al. 2012; Di Gessa and Grundy 2014; Wahrendorf et al. 2015; Voss et al. 2018; Wahrendorf et al. 2018) while some other studies have demonstrated the health benefits of retiring (see, for instance: Westerlund et al. 2009; Wels 2018) .
For instance, Di Gessa and Grundy (2014) have demonstrated that engagement in paid work contributes to maintain health in later life compared to people leaving the labour market. Similarly, using cross-sectional data Siegrist and Wahrendorf (2009) have shown that continued participation in socially productive activities improves prospective quality of life in early old age and Alavinia and Burdof (2008) have demonstrated that poor health, chronic diseases, and lifestyle factors are associated with being out of the labor market. Similarly, looking at full-time workers aged 50 and over, Moon et al. (2012) show that retirement is associated with elevated odds of having cardiovascular disease. Using the Health and Retirement Survey, Voss et al. (2018) found that late-career unemployment has no significant effect on self-reported physical health but is associated with lower levels of mental health. Similarly, taking a life-course perspective, Wahrendorf et al. (2018) have shown, for France, that adverse employment histories and years out of work are associated with poor health at the old age. Conversely, a certain number of studies have underlined the positive impact of retiring, particularly for those working in poor work environment. Using the French GASEL dataset, Westerlund et al. (2009) have shown that workers’ self-perceived health is substantially relieved by retirement for all groups of workers (apart from those with ideal working conditions). Similarly, focusing on sleep disturbance, Vahtera et al. (2009) provide strong evidence for a substantial and sustained post-retirement decrease in sleep disturbances. Using Belgian data from the SHARE, I found that respondents moving to retirement are more likely to present a better self-perceived health, depression level and quality of life compared to people increasing or keeping the same working-time level, after controlling for the age and other socio-economic variables (Wels 2018).
As a matter of fact, the association between retirement transitions and health needs to be nuanced and to account for factors that affect the retirement decision. For instance, Schuring et al. (2015) show that the level of education plays a role in explaining both early retirement decision and post-retirement health. While the health of low-educated workers partly prompts early retirement and economic inactivity, these exit routes prevent further deterioration of their health. The opposite relation is observed for high educated workers as early retirement has an adverse effect on self-reported health. Slightly different finding was reported by König et al. (2018) using Swedish data: as lower educated retirees are more likely to stop working for physical reasons, this leads to poor post-retirement health. The same kind of result is observed when looking at the occupational class (see, for instance, Virtanen et al., 2017). But other factors can be taken into consideration. For instance, the generosity of the Welfare State plays a role in explaining the change in health following work exit. Comparing 16 European countries, Richardson et al. (2019) found that national expenditure on in-kind benefits is associated with more favourable wellbeing change outcomes after leaving the labour market. The nature of the transition, whether voluntary or involuntary, also affects health. Using the Swedish Longitudinal Occupational Survey of Health, Hyde et al. (2015) show that, compared to voluntary employment exit, involuntary exit is associated with a higher risk of reporting major depression and becoming newly prescribed anti-depressant medication. Finally, collective bargaining and trade union membership may also play a role in explaining older workers’ health variations. Using the Health and Retirement Study for the United States, I have shown that unionized workers are less likely than non-unionized workers to experience a negative change in self-perceived health and depression level during the different types of late career transitions (Wels 2018). Unionized workers are also more likely to retire earlier compared with non-unionized workers. In essence, it can be assumed that working life prolongation may have both adverse and beneficial effects.
Late Career Transitions in Japan
The retirement age in Japan is high when compared to other industrial countries. Statistics show that the labor participation rate for men aged 65 and over in Japan is much higher than in North America and EU countriesFootnote 1 (JILPT, 2019). In response to population decline and labor shortage, recent political discussion focused on providing an environment that allows elderly workers to continue working. Japan’s employment policy for the elderly has been a subject of great debate in recent years. Since the 1980s, the debate on extending retirement age has continued, and a law change in 2012 has imposed an employment obligation from the retirement age of 60 to the age of 65. The current law requires companies to continue working until the age of 65, such as by setting a 65-year retirement age. The current policy debate is about securing employment opportunities until the age of 70.
Studies looking specifically at Japan are few in number and estimates are still contradictory. Okamoto et al. (2018) find that remaining in employment has positive effect on life expectancy, reduces cognitive decline and reduces the risk of early diabetes and stroke. Similarly, using data from the Japan Gerontological Evaluation Study, Shiba et al. (Shiba et al., 2017) find that respondents who transitioned to retirement experience increased depressive symptoms. Men who were continuously retired report increased depressive symptoms whereas moving back to work is associated with reduced depressive symptoms. Using the same dataset, Amemiya et al. (2019) demonstrate that a high level of education (13 years or more) is associated with functional ability improvement, both for men and women. Using the JSTAR-RIETI dataset, Hashimoto (2015) finds limited impact of transitioning from paid work to retirement and underlines the need to account for the heterogeneity of the population. The common feature of these studies is to look at retirement as a process (Atchley, 1982) and therefore to assess the health variations resulting from this process. But such a perspective raises an issue: does retirement explain post-retirement health or, conversely, it is the health that explains the retirement decision and reflects in post-retirement health? Causation is a key point when analyzing the health effects of late career transitions, particularly when using longitudinal data.
The major issue of the Japanese employment system lies in the features of employment trajectories. Over the past two decades, non-standard forms of employment have flourished in Japan with consequences on health. For instance, Nishikitani et al. (2012) have shown that the increase in precarious non-regular employment has been on the main factor that has caused a deterioration in workers’ health between 2001 and 2007. More globally, non-standard forms of employment are clearly associated with lower health outcomes (Sirviö et al., 2012). The question is worth asking in the case of the older Japanese workforce as it has been observed that older workers are more likely to work in non-regular employment – particularly part-time and contract work – than the rest of the working population: non-regular forms of employment are more often observed after 60 than before (Cabinet Office, 2019). One of the factors explaining this is the companies’ ‘employment extension practices’. Under the current law, companies are required to hire up to 65 years of age. Under these conditions, many companies have adopted a reemployment scheme instead of setting retirement age to 65. The common reemployment scheme is to have employees retire once at retirement age set by company (e.g. 60 years old) and sign a reemployment contract in a non-regular employment form such as on a contract employee. This type of employment form is called ‘Shokutaku’ (i.e. entrusted employee). The reason why this reemployment practice is common in Japan is that under the seniority-based wage system, extending the retirement age of the elderly increases the labour costs for the company. For this reason, companies are likely to take measures to reduce salaries of re-employed elderly to near productivity levels. For elderly people, however, wages have dropped significantly, and motivation has been a major problem. It has also been pointed out that the content of work has changed drastically, such as being removed from management positions, and that skills and experience cannot be used. Therefore, older Japanese workers might face a so-called downward mobility (Osako, 1988) towards retirement.
However, the relationship between change in health outcomes and late career employment transitions has not been assessed so far in Japan. The negative effects of precarious employment on well-being and health conditions have been discussed in previous studies (Benavides et al., 2000; Nishikitani et al., 2012; Sirviö et al., 2012). The specific case of Japan where non-standard forms of employment are widespread in late career bring new light on this perspective. First, the impact of employment forms on well-being needs to be considered not only with the low working conditions, but also with the elderlies’ motivations to work and the relationship with the labor market they face. A survey of elderlies’ motivations to work shows that many continue to work because of financial needs (JILPT, 2020). Second, there is a strong desire among elderly women to work in shorter working hours than full time (JILPT, 2020). On the other hand, in the current labor market, there are not enough regular employment opportunities in line with the wishes of workers, and there are few options other than working in non-standard employment, which has far worse working conditions. Since such a working style does not match the wishes of the workers, there is a possibility that health conditions such as mental health may be deteriorated. Finally, when considering the labor market in Japan, gender differences cannot be ignored. Under Japanese-style employment system, it is pointed out that women have difficulty forming careers and skills (Takahashi, 2018), but the poorer the skills, the more likely they are to face difficulties in the elderly labor market. Under these labor markets and the employment system, workers who have no choice but to shift to non-standard employment may experience adverse effects in terms of well-being and self-reported health. This is the hypothesis that is test in this study.
Data and Methods
JSTAR-RIETI
JSTAR is a longitudinal dataset that currently contains four waves released every two years (currently: 2007, 2009, 2011, 2013). The original sample strategy is described in Ichimura et al. (2009). One its specificities is that the survey takes the municipality as a “cluster of sampling, instead of adopting nationwide probabilistic sampling” (p.44). At baseline (2007), JSTAR contains respondents aged 50 to 75 living in five municipalities in eastern area of Japan (Ichimura et al., 2009): Takikawa in Hokkaido, Sendai in the Tohoku area, Adachi Ward within Tokyo, Kanazawa in Hokuriki and Shirakawa in the Chubu area. Some efforts have been made to increase the number of cities. The 2011 wave includes two additional cities (Tosu and Naha) and there are ten cities in the 2013 wave (Chofu, Hiroshima and Tondabayashi). The original sample was composed of 4163 respondents. The attrition rate was 25.8% between wave 1 and wave 2, 19.8% between wave 2 and wave 3 and 13.1% between wave 3 and wave 4. JSTAR-RIETI provides a country-level sample weight that is based on census data and accounts for age and household composition, the type of employment and regional attributes (information about the municipality level are not publicly available). In this study we select the population that is in employment at first wave (N = 1267). As for the original sample, the highest attrition rate is observed between the baseline (2007) and the second wave (2009) with 911 respondents alive and who were able to answer (attrition accounts for 28% of the original sample). The retention rate is then 724 and 647 respondents respectively in the third (2011) and fourth waves (2013) which correspond to a retention rate of respectively 20.5 and 10.6% from waves 2 to 3 and from waves 3 to 4. Information about the reasons for the missingness were collected but with a very high non-response rate. The dataset raises several issues. First, the 2007 sample is relatively big (4200) but about half of the population that was included in the original survey was already out of work (mainly retired). Looking at the older workforce and, particularly, at non-standard employment drastically reduces the size of the sample and attrition in the following waves makes it even more complex (about 20% of the working sample dropped out between wave 2007 and wave 2009). Second, as the baseline sample was collected in five municipalities, it does not represent accurately the situation of the full Japanese workforce and this is a limitation it is hard to deal with. The current study only focuses on data collected in 2007 in the five municipalities. By doing so, one calculates a slope (for the three subsequent waves, i.e. 2009, 2011, 2013) that accounts for the long term change in health over a period of four years.
Dependent Variables
Two dependent variables are used in this study: the general health and the mental health. The general health (also called self-perceived health or self-rated health) is the answer to the question ‘How is your health in general?” and contains five answer modalities coded from very positive (1) to very negative (5). It is a very common variable that can be found in most sureveys looking at the older population, such as the Survey of Health, Ageing and Retirement in Europe (SHARE) (Fujii et al. 2012). Mental health sums up information about week frequency (1: Not at all; 2: 1 ~ 2 days; 3: 3 ~ 4 days; 4: 5 days or more) of several mental health conditions such as feeling unusual in some way, having no appetite, feeling depressed, feeling sad, feeling lonely, etc. Both variables are used a numeric in further analysis. The normal distributiveness of the original variables and post-transformed variables was tested using a Kurtosis coefficient (see Table 1). The Kurtosis for general health was calculated for the original variable distribution (n), le natural logarithm (n(log)) and a reduced version of the variable that combines modalities 4 and 5 into one modality (h). The Kurtosis for mental health was calculated for the original variable (n), the natural logarithm (n(log)) and the Anscombe transformation (15 modalities) of the natural logarithm.Footnote 2
Further analyses use the original distribution of general health (n) and the Anscombe transformation of mental health (h). In both cases, estimates can be interpreted as follow: a positive coefficient indicates a negative impact on health (the value of the dependent variable tend to be higher) whilst a negative coefficient indicates a positive impact on health.
Variable of Interest
The variable of interest is ‘T’, that is the type of professional transition between wave 1 (2007) and wave 2 (2009). Only the population declaring being employed in wave 1 is selected. Wave 1 contains three modalities: ‘full-time employment’, ‘non-standard employment’ and ‘other’. Data are collected on a declarative basis. ‘Non-standard employment’ combines information about part-time employment, contract work and temporary work. The category ‘other’ refers to respondents who answered being in the category ‘other’ within the questionnaire (only five respondents in wave 1). Conversely, wave 2 accounts for the full set of possible transitions and contains five modalities: full-time employment, non-standard employment, retirement and self-employment. Therefore, the study focuses on a set of fifteen possible transitions from wave 1 to wave 2.
Covariates
The paper controls for a set of fixed covariates measured at the baseline year of the observation period (2007): a quadratic function of the age at the baseline, the highest level of education achieved (Elementary to middle school, High School, Junior college, Vocational school, University, Master, PhD), the seniority (i.e. the number of years since the current position started), the martial status, the number of children, the type of business (18 types), the type of employment (Full-time employee, Part-time employee, Temporary worker, contract worker, own or dependent business, Helping in dependent business, side job at home, or other) and the post calculated weekly working time and incomes. The study also controls for an index of job dissatisfaction that sums up information collected on a Likert scale ((1) strongly agree, (2) somewhat agree, (3) don’t really agree, (4) strongly disagree) on whether or not the job includes physical labour, workload and time pressure, job discretion, colleague support, appropriate evaluation by manager and pay satisfaction. The natural logarithm of the index is used to ensure that the variable is normally distributed. Finally, two dummy variables are included to control for the exact year when respondents retired (2008 versus 2007, and 2009 versus 2007). The study also controls for time-varying covariates looking at the change in employment status in subsequent waves (2011 and 2013).
Propensity Scores
Propensity scores were calculated using a binary logit model to assess the potential impact of individual characteristics on the types of transitions that occur from wave 1 to wave 2.
Latent Growth Modeling (LGM)
We use a latent growth modeling (LGM) to examine the association between SPH and MHI and employment status between wave 1 and wave 2. This is a multivariate approach (Masyn et al., 2013) in which intra individual change is captured by the measurement model for the growth factors, and interindividual differences are captured by the structural model (i.e. the mean and variance/covariance structure of the growth factors). The linear latent growth curve contains two latent factors, an intercept and a slope. The dependent variable (Yti) is the observed outcome Y for individual i (from 1 to n) at time t (T is the number of waves). The intercept (random intercept factor) is the expected outcome on y for respondent i at time score 0 (i.e. the first wave). The slope (random linear slope factor) is the change in the expected outcome on the dependent variable for respondent i for one-unit increase in time so that the slope can be interpreted as the linear rate of change in the dependent variable. In this study, we select only the population in employment in wave 2007 (N = 893, excluding attrition) and pick up wave 2007 as the baseline to assess for the change in employment status between 2007 and 2009. The model controls for covariates at the baseline and time-changing covariates in order to control for change in employment status in waves 2011 and 2013. Attrition is controlled using maximum likelihood estimations.
Figure 1 summarizes the model. ‘C’ represents the set of fixed covariates that affect both the intercept and the slope. ‘H1’ to ‘H4’ are the longitudinal health outcomes respectively from wave 1 (2007) to wave 4 (2013). ‘V’ are the time-varying co-variates. ‘T’ is the transition that is observed from wave 1 to wave 2 and is used as a fixed covariate that affects both the intercept and the latent slope. The LGM was performed using weighted data as JSTAR provides a specific weight that accounts for the age, the household type (man alone, woman alone, married couple alone, married couple and the others, man and the others, woman and the others), the type of employment (full time worker, part time worker, self-employed, unemployed or not in labour force, executive) and some regional attributes.

Model specifications
Results
Descriptive Results
Table 2 exhibits some descriptive statistics about the type of employment transitions that are observed between wave 1 and wave 2. As in most longitudinal studies, it can be observed that stability is the norm: 37% (i.e. 329) of the sample was declaring being in full-time employment in waves 1 and 2 and 33% (i.e. 293) of the sample declared being in non-standard employment in waves 1 and 2. 69 respondents moved from full-time employment to non-standard employment (8% of the sample) and 22 respondents moved from non-standard to full-time employment (2% of the sample).
Looking at the ratio between men and women (in parentheses), it can be observed that there are 3.27 men remaining in full-time employment for one woman. Conversely, there is a ratio of 0.67 for those remaining in non-standard employment: women are more likely than men to be in non-standard employment at the baseline and to remain in non-standard employment in wave 2. Interestingly, men are more likely than women to move from full-time employment to non-standard employment (5.9 men for one woman).
Propensity Scores
All categories of workers are not affected by non-standard employment the same way. Consequently, a bias could arise because the impact of non-standard employment on health may be cause by the factors that predicts non-standard employment rather than by non-standard employment itself. Some preliminary analyses are therefore needed to tackle such a bias. To do so, we used propensity scores to estimate the differences in mean between each independent variable (predicting non-standard employment) within the original dataset on the log odds (logit) of transitioning from full-time to non-standard employment versus the other types of transitions.
Propensity scores presented in Table 3 are in logits. They show that four variables might be of particular significance when looking at the transition from full-time employment to non-standard employment. The logarithm of the incomes has a positive (but barely statistically significant) impact. Put in another way, the probabilities for the ageing workforce to move from full-time employment to non-standard employment are higher for those having higher incomes. Another variable of interest is the number of children: a high number of children is associated with lower probabilities (by about 5 percentage points – significant at 95%) to move to non-standard employment. The type of sector of activity (business type) could also play a part in explaining such a transition; that is particularly the case of the education and learning support sector. Finally, a strong cofounder in explaining transition from full-time to non-standard employment is gender. Women have very little probability to move to non-standard employment (statistically significant at 95%). Three main reasons could explain this finding. First, the proportion of women still in professional activity after 50 is low. Second, Japanese female workers tend to retire slightly before Japanese male workers. Finally, and more importantly, female workers are more likely to be already in non-standard employment prior the selected sequence than me. Unfortunately, the original sample is small, and the matched dataset following propensity score matching reduces drastically the number of cases, reducing the number of available independent variables as well. That is the reason for why further analyses are calculated based on the original dataset but results for the latent growth modelling are replicated separately for male and female.
Missing Data
Attrition and missing data can lead to misleading estimates if data are not missing completely at random (MCAR), i.e. if there is no relationship between the propensity for missingness and any values in the dataset, missing or observed. Yet, this case is rare and most of the time missing data are missing at random (MAR) or missing not at random (MNAR). When missing data are missing at random, the propensity of a data to be missing is not related to missing data as such but to some of the observed data: observed data could predict the missingness, there is a conditionality in it. Conversely, in the case of data that are missing not at random, there is a relationship between the propensity of missingness, on the one hand, and its values, on the other hand.
To assess the nature of the missingness in the dataset, we have performed a binary logistic regression using general and mental health in waves 2, 3 and 4 (coded ‘1’ when the value is missing and ‘0’ when the value is not missing due to attrition). Therefore, the model estimates the reasons leading to attrition in waves 2, 3 and 4 using the health indicators (H) prior the transition as the variable of interest (to detect for missingness not at random – MNAR) and other covariates such as gender, sector of activity or business type at the baseline to detect data that are missing at random (MAR). Table 4 shows the estimates (in log odds) as well as the significance levels.
Table 4 does not show any association between attrition patterns and mental health in waves 2 to 4 – logit coefficients are near zero and not significant. However, there is a positive association between the general health level in wave 1 and whether data are missing in wave 2 (by 0.182, significant at 95%). In other words, an increase of one unit in general health at the baseline is associated with an increased logit (by 0.182 units) to be missing in wave 2, which indicates a potential MNAR pattern, at least from wave 1 to wave 2 (which also contains the highest attrition rate). But other variables contribute to explain attrition such as seniority (with a very low impact from waves 1 to wave 2), the type of business or the level of education (junior high school education is associated with higher attrition rates from wave 3 to wave 4). The C-statistics (concordance statistics) is a useful measurement to evaluate the fit of logistic regression models (Westreich et al., 2011). It ranges from the minimum value of 0.5 to the maximum one of 1. The c-statistics of the logit model is 0.622, 0.643 and 0.762 for waves 2, 3 and 4 respectively, which indicate the intermediary levels about predicting the propensity of retention or attrition.
Latent Growth Curve
Tables 5 and 6 exabit the results of the LGM calculated for both general health and mental health (after the Anscombe transformation of the natural logarithm). The transition from full-time employment to full-time employment was selected as the reference category as it is the one that occurred the most. Therefore, both the intercepts and the slopes for each transition is compared with the reference category. The model is replicated using full-information likelihood estimation for attrition in Table 5 and the original dataset excluding sample attrition (i.e. treated as missing data) in Table 6, with no significant difference between the observed estimates. Both models include fixed and time-varying covariates. Three main findings flow from Table 5. First, those who keep working in non-standard employment over the sequence have a more positive change in general and mental health than those who keep working full-time (slopes are respectively −0.071 and − 0.048, significant at 95 and 90% which indicates an average difference in the dependent variable scales). Second, those who move from full-time employment to non-standard employment have a poorer mental health than those who keep working full-time (0.030 units, significant at 95%). Finally, those who move to retirement after working full-time have a poorer baseline general and mental health (intercept) compared with those who keep working full-time, but with low statistical significance in the case of general health (0.10). Interestingly, those who move from non-standard employment to full-time employment have a positive change in mental health (−0.123, significant at 95%).
Reflecting the results that were found in the propensity scores, Table 7 decomposes the estimates separately by gender. Four main conclusions flow from the table. First, men are more likely to move from full-time employment to non-standard employment but women moving from full-time to non-standard employment have a much poorer mental health than women remaining in full-time employment. Second, men moving from full-time employment to self-employment have a much better general health than men remaining in full-time job. Third, men who keep working in non-standard employment (i.e. those who do not experience a change in employment status over the sequence) have a better health than those who keep working full-time. Men who move from non-standard employment to full-time employment also have a better health than those working in full-time employment over the sequence. Finally, both men and women moving from non-standard employment to retirement have a better health than respondents remaining in full-time employment.
Limitations
This article contains many limitations that should be addressed in further studies using the JSTAR dataset or focusing on the same issue.
Firstly, the small sample size does not allow to perform a proper propensity score matching that would neutralise the effect of covariates on the type of transition. This is a major issue as variables such a gender or level of education are associated both with health and with the type of transition that is observed over the sequence. Therefore, this might lead to some spurious associations in which we assess the impact of labour market transitions on health whereas external variables explain both the type of transition and health. Though, to tackle such an issue, we have performed analyses separately for men and women (gender being a major cofounder).
Secondly, attrition is controlled using maximum likelihood estimations, but attrition rates vary drastically from one area to another, potentially due to issues in reaching back some populations in rural areas. To keep the dataset anonymous, JSTAR does not provide an individualized variable distinguishing area and, consequently, the paper does not control for such a potential issue.Footnote 3
Thirdly, JSTAR does not contain any information about whether the transition towards retirement is voluntary or not. That is an important issue. As demonstrated by Hyde et al. (2015), involuntary transitions may have adverse effects on health that voluntary transitions do not have.
Discussion
Assessing the impact of late career transitions requires to look in-depth at the set of arrangements that are implemented for the older workforce among which non-standard employment plays an important role, particularly in Japan where the use of non-standard forms of employment after 60 is not negligible. One cannot assess such an impact without understanding the policy backgrounds that shape late career transitions and a clear understanding of employment configurations. This study particularly emphases the dual nature of non-standard employment. On the one hand, respondent who were in non-standard employment throughout the sequence do not experience a negative change in health (the intercept is not significant, but the slope indicates a positive change). On the other hand, the study shows that moving to non-standard employment after being a full-time employee does have adverse effects on health. This is a key point when looking at the relationship between non-standard employment trajectories and health: that is indeed the change in status and, more specifically, moving to more flexible statuses that has an impact on health, not the type of status as such. According to the study, transitioning from full-time to non-standard deteriorates health but moving from non-standard employment to full-time employment improves health. Japan’s employment system may lead to poor health for the elderly. Similarly, the article particularly shows that older female workers are more vulnerable to changing employment status and that self-employed workers constitute a large part of the older employment workforce about which little is known.
The study shows the necessity to distinguish the respective effects of work and employment when assessing – particularly using longitudinal data – change in health over the working life course. Further research should look at this direction. The current study focuses on the role of employment transitions (i.e. the change in employment status) after controlling for job quality at the baseline (i.e. the working conditions). By doing so, the study catches up the changes that occurred because of the transition from one type of status to another independently from the content of the job (i.e. the tasks and responsibilities). Research on this matter is indeed often decontextualized, giving little space for national regulations, types of employment schemes or working conditions (see, for instance, Giorgio Di Gessa et al., 2016) even if there is a recent growing attention for the role played precarious employment and welfare coverage in explaining older workers’ health (Lain et al. 2018). That is the direction that this study is taking.
For the specific case of Japan, the study points out the necessity to open up a debate about what would be the accurate policy reforms to implement to achieve sustainable transitions towards retirement in Japan. An important issue is about the use of the re-employment system for the older employed workforce. Contract work is often imposed in late career due to legislations regarding the legal retirement age. In contrast to other liberal countries such as the United States, New Zealand or the United Kingdom that have abolished the legal retirement age, Japan still has a retirement age (and so does most European countries). However, one major obstacle in extending working lives lies within the costs related to labour. So far, current policies impose such a cost to workers rather than to employers and this has negative consequence on workers’ health. One needs to find a fairer system that secures older workers’ employment, on the one hand, and does not discourage employers, on the other hand. There are three ways to do so. First, it would be possible to limit through legislation the use of reemployment system but with the risk of discouraging companies to hire older workers. Another solution would be to force companies to set up retirement ages that correspond to the one that is fixed by the state to avoid such a gap, but this would also have adverse effects. Finally, a last solution – that is promoted by the OECD – would be to abolish the retirement age and to implement an ‘equal work, equal pay principle’ (OECD, 2019) but with other types of adverse effects such as, for instance, low incomes for so-called low qualified jobs (Wels, 2019a) and a difficulty in some companies to receive the information about the age at which one can actually move to retirement.
A more suitable solution might lie in the implementation of gradual retirement schemes in Japan. So far, Japan has not systematically implemented working time schemes that would allow workers to reduce working time in a move towards retirement. Such an issue is complex (Wels 2020, 2019b, 2019c) as working time reduction is often associated with income loss and the question is to know whether it would be equitably affordable to reduce working time in the lead up to retirement and to what extent the welfare state could financially support such a reduction to avoid discrepancies. If working time reductions do not guarantee better health and wellbeing outcomes (Wels 2020) they could nevertheless enhance healthier late career transitions for low-paid workers (Wels 2019c). The potential benefits of such schemes are still to evaluate.
Notes
In 2018, the percentage in Japan is 33.9.
Mental health has a typical Poisson Distribution with a large part of the sample declaring not having any mental health conditions. The Anscombe transformation is particularly suitable for transforming a random variable with a Poisson distribution into an approximately standard Gaussian distribution.
n.b. Approved JSTAR users can used a Very High (VH) confidentiality dataset but are required to access the datasets via the RIETI remote control system (SACSES).
References
Alavinia, S., & Burdorf, A. (2008). Unemployment and retirement and ill-health: a cross-sectional analysis across European countries. International Archives of Occupational and Environmental Health, 82(1), 39–45.
Amemiya, A., Kondo, N., Saito, J., Saito, M., Takagi, D., Haseda, M., Tani, Y. & Kondo, K. (2019). Socioeconomic status and improvement in functional ability among older adults in Japan : a longitudinal study. BMC Public Health, 19(209), 1–8.
Atchley, R. (1982). Retirement as a social institution. Annual Review of Sociology, 8(1982), 263–287 Retrieved from http://www.jstor.org/stable/2945996.
Bell, A., & Jones, K. (2015). Age, period and cohort processes in longitudinal and life course analysis: A multilevel perspective. In C. Burton-Jeangros, S. Cullati, A. Sacker, & D. Blane (Eds.), A life course perspective on health trajectories and transitions (Vol. 4, pp. 39–61). London: Springer. https://doi.org/10.1007/978-3-319-20484-0.
Benavides, F. G., Benach, J., & Diez-Roux, a V, & Roman, C. (2000). How do types of employment relate to health indicators? Findings from the second European survey on working conditions. Journal of Epidemiology and Community Health, 54(7), 494–501. https://doi.org/10.1136/jech.54.7.494.
Benson, R., Glaser, K., Corna, L. M., Platts, L. G., Gessa, G. Di, Worts, D., … Sacker, A. (2017). Do work and family care histories predict health in older women? European Journal of Public Health, online(October), 1–6. https://doi.org/10.1093/eurpub/ckx128
Cabinet Office. (2019). Annual report on the ageing society. Cabinet Office Japan, (June 2019), 11. Retrieved from https://www8.cao.go.jp/kourei/whitepaper/w-2019/gaiyou/pdf/1s1s.pdf
Corna, L. M., & Sacker, A. (2013). A lifetime of experience : Modeling the labour market and family histories of older adults in Britain. Longitudinal and Life Course Studies, 4(1), 33–56.
Di Gessa, G., & Grundy, E. (2014). The relationship between active ageing and health using longitudinal data from Denmark, France, Italy and England. Journal of Epidemiology & Community Health, 68(3), 261–267. https://doi.org/10.1136/jech-2013-202820.
Di Gessa G, Corna LM, Platts LG, Worts D, McDonough P, Sacker A, … Glaser K (2016). Is being in paid work beyond state pension age beneficial for health? Evidence from England using a life-course approach. Journal of Epidemiology and Community Health, onlinefirs, jech-2016-208086. https://doi.org/10.1136/jech-2016-208086
Fujii, M., Oshio, T., Shimizutani, S. (2012). Self-Rated Health Status of the Japanese and Europeans in Later Life : Evidence from JSTAR and SHARE. RIETI Discussion Paper Series, 12-E-061, 27.
Graetz, B. (1993). Health consequences of employment and unemployment: Longitudinal evidence for young men and women. Social Science & Medicine, 36(6), 715–724. https://doi.org/10.1016/0277-9536(93)90032-Y.
Hashimoto, H. (2015). Impacts of leaving paid work on health, functions, and lifestyle behavior: Evidence from JSTAR panel data. RIETI Discussion Paper Series 15-E-114, 17.
Hyde, M., Hanson, L. M., Chungkham, H. S., Leineweber, C., & Westerlund, H. (2015). The impact of involuntary exit from employment in later life on the risk of major depression and being prescribed anti-depressant medication. Aging and Mental Health, 19(5), 381–389. https://doi.org/10.1080/13607863.2014.927821.
Ichimura, H., Shimizutani, S., & Hashimoto, H. (2009). JSTAR first results 2009 report: Japanese study of aging and retirement. REITI Discussion Paper Series, 09-E-047, 305. Retrieved from http://www.rieti.go.jp/jp/publications/dp/09e047.pdf
JILPT (Japan Institute for Labour Policy and Training). (2019). Databook of international labour statistics. Tokyo: JILPT.
JILPT (Japan Institute for Labour Policy and Training). (2020). Survey on employment and life in 60s. JILPT Research Series, n°199.
Keese, M. (n.d.). A method for calculating the average effective age of retirement. OCDE, 1–3.
König, S., Lindwall, M., & Johansson, B. (2018). Involuntary and delayed retirement as a possible health risk for lower educated retirees. Journal of Population Ageing., 12, 475–489. https://doi.org/10.1007/s12062-018-9234-6.
Lain, D., Airey, L., Loretto, W., & Vickerstaff, S. (2018). Understanding older worker precarity: The intersecting domains of jobs, households and the welfare state. Ageing and Society, (October), 1–23. https://doi.org/10.1017/S0144686X18001253.
Masyn, K. E., Petras, H., & Liu, W. (2013). Growth curve models with categorical outcomes. Encyclopedia of Criminology and Criminal Justice, 2013–2025. https://doi.org/10.1007/978-1-4614-5690-2_404.
Moon, J. R., Glymour, M. M., Subramanian, S. V, Avendaño, M., & Kawachi, I. (2012). Transition to retirement and risk of cardiovascular disease: Prospective analysis of the US health and retirement study. Social Science & Medicine (1982), 75(3), 526–530. https://doi.org/10.1016/j.socscimed.2012.04.004.
Nishikitani, M., Tsurugano, S., Inoue, M., & Yano, E. (2012). Effect of unequal employment status on workers’ health: Results from a Japanese national survey. Social Science and Medicine, 75(3), 439–451. https://doi.org/10.1016/j.socscimed.2011.11.039.
OECD. (2019). Working better with age: Japan. Paris: OECD. https://doi.org/10.1787/9789264201996-en.
Okamoto, S., Okamura, T., & Komamura, K. (2018). Employment and health after retirement in Japanese men. Bulletin of the World Health Organization, 96(12), 826–833. https://doi.org/10.2471/BLT.18.215764.
Osako, M. M. (1988). “Downward mobility” as a form of phased retirement in Japan. Ageing International, 15(2), 19–22. https://doi.org/10.1007/BF03002119.
Rice, N. E., Lang, I. A., Henley, W., & Melzer, D. (2011). Common health predictors of early retirement: Findings from the English longitudinal study of ageing. Age and Ageing, 40(1), 54–61. https://doi.org/10.1093/ageing/afq153.
Richardson, S., Carr, E., Netuveli, G., & Sacker, A. (2019). Country-level welfare-state measures and change in wellbeing following work exit in early old age: Evidence from 16 European countries. International Journal of Epidemiology, 48(2), 389–401. https://doi.org/10.1093/ije/dyy205.
Schuring, M., Robroek, S. J. W., Lingsma, H. F., & Burdorf, A. (2015). Educational differences in trajectories of self-rated health before, during, and after entering or leaving paid employment in the european workforce. Scandinavian Journal of Work, Environment and Health, 41(5), 441–450. https://doi.org/10.5271/sjweh.3514.
Shiba, K., Kondo, N., Kondo, K., & Kawachi, I. (2017). Retirement and mental health: Dose social participation mitigate the association? A fixed-effects longitudinal analysis. BMC Public Health, 17(526), 0–10. https://doi.org/10.1186/s12889-017-4427-0.
Siegrist J., Wahrendorf M., (2009). Participation in socially productive activities and quality of life in early old age: findings from SHARE. Journal of European Social Policy, 19(4), 317–326
Sirviö, A., Ek, E., Jokelainen, J., Koiranen, M., Järvikoski, T., & Taanila, A. (2012). Precariousness and discontinuous work history in association with health. Scandinavian Journal of Public Health, 40(4), 360–367. https://doi.org/10.1177/1403494812450092.
Takahashi, K. (2018). The future of the Japanese-style employment system - continued long-term employment and the challenges it faces. Japan Labor Issues, 6(2). Retrieved from http://www.jil.go.jp/english/researcheye/bn/REtakahashi.html
Vahtera, J., Westerlund, H., Hall, M., Sjösten, N., Kivimäki, M., Salo, P., & Ferrie, J. E. (2009). Effect of retirement on sleep disturbances : The GAZEL prospective cohort study. Sleep, 32(11), 1459–1466.
Virtanen, M., Oksanen, T., Pentti, J., Ervasti, J., Head, J., Stenholm, S., et al. (2017). Occupational class and working beyond the retirement age: A cohort study. Scandinavian Journal of Work, Environment and Health, 43(5), 426–435. https://doi.org/10.5271/sjweh.3645.
Voss, M. W., Wadsworth, L. L., Birmingham, W., Merryman, M. B., Crabtree, L., Subasic, K., & Hung, M. (2018). Health effects of late-career unemployment. Journal of Aging and Health, 32, 1–21. https://doi.org/10.1177/0898264318806792.
Waddell, G., & Burton, a K. (2006). Is work good for your health and well-being? The stationery office, United Kingdom. London: TSO.
Wahrendorf, M. (2015). Previous employment histories and quality of life in older ages: Sequence analyses using SHARELIFE. Ageing and Society, 35(9), 1928–1959. https://doi.org/10.1017/S0144686X14000713.
Wahrendorf, M., Hoven, H., Goldberg, M., Zins, M., & Siegrist, J. (2018). Adverse employment histories and health functioning: The CONSTANCES study. International Journal of Epidemiology, 48(2), 402–414. https://doi.org/10.1093/ije/dyy235.
Westerlund, H., Kivimäki, M., Singh-Manoux, A., Melchior, M., Ferrie, J. E., Pentti, J., Jokela, M., Leineweber, C., Goldberg, M., Zins, M., & Vahtera, J. (2009). Self-rated health before and after retirement in France (GAZEL): a cohort study. The Lancet, 374(9705), 1889–1896. https://doi.org/10.1016/S0140-6736(09)61570-1.
Westreich, D., Cole, S. R., Funk, M. J., & Brookhart, M. A. (2011). The role of the c-statistic in variable selection for propensity score models. Pharmacoepidemiol Drug, 20(3), 317–320. https://doi.org/10.1002/pds.2074.The.
Wels, J. (2016). The Statistical Analysis of End of Working Life: Methodological and Sociological Issues Raised by the Average Effective Age of Retirement. Social Indicators Research, 129(1), 291–315. https://doi.org/10.1007/s11205-015-1103-6
Wels, J. (2018). Are there health benefits of being unionized in late career? A longitudinal approach using HRS. American Journal of Industrial Medicine, 61(9), 751–761. https://doi.org/10.1002/ajim.22877
Wels, J. (2020). Assessing the impact of partial early retirement on self-perceived health , depression level and quality of life in Belgium : a longitudinal perspective using the Survey of Health , Ageing and Retirement in Europe (SHARE). Ageing & Society, 40(3), 512–536. https://doi.org/10.1017/S0144686X18001149
Wels, J. (2019a). État des lieux de l’emploi des travailleurs âgés en Belgique. Pyramides, 31/32, 261–283.
Wels, J. (2019b). Structural and Individual Barriers to Progressive Retirement . A European comparison using SHARE. SHARE Working Paper Series, 38, 19. http://www.share-project.org/uploads/tx_sharepublications/WP_Series_38_2019_Wels.pdf
Wels, J. (2019c). Wels, J. (2019c). The association between self-reported health, late career transitions and working time modulation in England. International Journal of Workplace Health Management, 12(6), 424–440. https://doi.org/10.1108/IJWHM-04-2019-0056
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interests
All the authors declare no conflict of interests.
Informed Consent
None.
Ethical Treatment of Experimental Subjects (Animals and Humans)
No experimental treatment was conducted on either human or animal subjects in this study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Wels, J., Takami, T. The Impact of Transitioning to Non-Standard Employment on Older Workers’ Self-Reported and Mental Health in Japan. A Longitudinal Perspective Using the Japanese Study of Aging and Retirement. Ageing Int 46, 363–382 (2021). https://doi.org/10.1007/s12126-020-09392-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12126-020-09392-9