
Abstract
Chronic osteomyelitis resulting from foreign body entrapment in the pediatric mandible presents unique challenges in diagnosis and management. Habitual insertion of objects into the oral cavity by children can lead to serious complications such as discharging sinuses and osteomyelitis. We present a case of a 12-year-old boy with extra-oral pus discharge originating from the mandible, ultimately traced to an embedded iron nail adjacent to a carious first molar. Radiographic imaging played a crucial role in diagnosis, revealing the foreign object and. Long-term follow-up showed successful healing with prompt treatment. Prevention through parent education, meticulous examination, and interdisciplinary collaboration are emphasized to avoid such complications.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Foreign body entrapments are more common in pediatric group due to habitual behavior of placing objects in their mouth. Children usually insert objects like pencils, needles and screws. Insertion of such objects can lead to impaction of objects in teeth due to large open pulp chambers due to traumatic injury or dental caries [1]. Hence, habitual or accidental insertion coupled with long standing dental neglect of carious teeth can lead to devastating consequences. Chronic embedment of such foreign body can result in osteomyelitis with discharging sinus and localized destruction of bone [2].
In most instances, these conditions can give misleading diagnosis as the foreign object is not visible in the oral cavity. Hence, radiographic examination plays a vital role in the detection, position of such objects. The management depends on the location of foreign object, type of dentition and condition of the tooth. Hereby, we present an unusual case of foreign body impaction in tooth.
Case Report
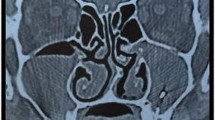
This is a case of a 12-year-old boy who was referred by dermatologist to the department of burns, plastic and maxillofacial surgery with a report of the extra-oral pus discharge from lower jaw. History revealed that the child had pain in left lower first molar 3 months back and presented with discharge for past 2 months. Medical history was unremarkable. On extra-oral examination, sinus was noticed in the left body region of mandible with pus discharge and tenderness on palpation. No inferior alveolar nerve parasthesia was present. Intraoral examination revealed a grossly carious first molar indicating the etiology for extra-oral sinus. (Fig. 1) Orthopantomogram revealed a radio-opaque object with respect to carious left lower molar and radiolucency extending up to lower border of mandible. (Fig. 2) Cone beam computed tomography was done to assess the three dimensional location, its relationship with inferior alveolar nerve and integrity of the mandible. Buccal and lingual cortices were intact with destruction of cancellous marrow and lower border of mandible. (Fig. 3).

Image showing the extraoral sinus and intraoral carious molar

Orthopantomogram showing the carious Mandibular first molar and foreign body(nail)

Coronal section of CBCT showing the position of foreign object and its relationship with buccal and lingual cortex of mandible
Retrieval of foreign body (iron nail) was done along with extraction of carious molar as the tooth was non-salvageable. (Fig. 4) Whole procedure was done under local anaesthesia Local debridement and de-epitheliasation of sinus tract was done. One year follow up revealed healed intraoral extraction site and extra-oral sinus tract. (Fig. 5)

Retrieved foreign body (nail) and extracted tooth

Image showing healed intraoral site
Discussion
Children often explore their environment through various means and inserting foreign objects in mouth is a common behavior [3]. In contrast, adolescents may engage such actions to gain attention or with intention of risk taking. These kinds of behavior are termed as self injurious behavior and pose greater risks. The present patient was ruled out of any self-injurious behavior. Prompt identification of habitual placement of foreign objects is necessary to prevent patient induced trauma to oral cavity region. When accompanied with dental neglect, particularly of carious teeth which are infection prone and can lead to severe consequences such as osteomyelitis and chronic sinus tracts. Hence, parent education is vital in preventing such situations [4]. Scrupulous case history, clinical examination and radiographic assessment are mandatory to locate the foreign body and aid in easy retrieval.
Timely diagnosis and management of foreign bodies in tooth should be done to avoid complications like osteomyelitis and chronic sinus tracts. The location and size of the object determination is important. For small objects in salvageable tooth, referral to pediatric dentist is necessary. Hedstroem Files may be used for retrieval [5], followed by calcium hydroxide dressing in order to save the tooth. Many cases have been reported with entrapment in anterior tooth, but in posterior tooth it is rare. The surgeon should be aware of such fomite or foreign body entrapment in oral cavity especially in children. Thorough debridement with de-epitheliasation and complete removal of foreign body with antibiotic coverage is the key for management. Given the complexity of cases, an interdisciplinary management is necessary.
References
Lakhani B, Garg S, Saraf BG, Tomer E, Singh N, Sheoran N (2019) Self-insertion of Foreign objects in Teeth. Int J Clin Pediatr Dentistry 12(2):145–149. https://doi.org/10.5005/jp-journals-10005-1595
Coviello V, Stevens MR (2007) Contemporary concepts in the treatment of chronic osteomyelitis. Oral Maxillofacial Surg Clin 19(4):523–534. https://doi.org/10.1016/j.coms.2007.07.001
Mahesh R, Waseem H, Siva Kumar M (2014) Unusual behavior in children–foreign object in tooth: a report of two cases. Ethiop J Health Sci 24(4):369–373. https://doi.org/10.4314/ejhs.v24i4.14
Spiller L, Lukefahr J, Kellogg N (2020) Dental Neglect. J Child Adolesc Trauma 13(3):299–303. https://doi.org/10.1007/s40653-019-0247-y
Aduri R, Reddy RE, Kiran K (2009) Foreign objects in teeth: retrieval and management. J Indian Soc Pedod Prev Dent 27(3):179–183. https://doi.org/10.4103/0970-4388.57100
Funding
None.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
Not required.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Alagarsamy, R., Kain, R., Lal, B. et al. Chronic Osteomyelitis Following Foreign Body Entrapment in Pediatric Mandible-a Case Reprt. Indian J Otolaryngol Head Neck Surg (2024). https://doi.org/10.1007/s12070-024-04904-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s12070-024-04904-4