
Abstract
Head and neck cancers are fairly common in India due to the widespread consumption of tobacco and neck dissection is a major component in the surgical management. The objective of this study is to analyze the effect of MRND and SND on shoulder function and quality of life in patients of head and neck cancer. Our study is a prospective comparative study on 65 head and neck cancer patients divided into 2 groups—33 in group A (MRND group) and 32 in group B (SND group). Clinical evaluation of shoulder function was done pre-operatively, 1 week, 1 month, 3 month and 6 month post-operatively using arm abduction scores (AAS) and shoulder pain and disability index (SPADI). Nerve-conduction study (NCS) was done pre-operatively and 3 months post-operatively for assessment of SAN. Neck dissection quality of life questionnaire (NDQOL) was used as a quality-of-life measure. A total of 65 neck dissections were included in the analysis (33 in group A and 32 in group B) out of which 53 were males and 12 were females. The mean AAS on the 6th post-operative month in group A was significantly lower than that of group B (p = 0.01). The mean SPADI scores on the 6th post-operative month was significantly worse in group A than group B (p value 0.01). On NCS, a significant decrease in amplitude was seen in group A (p = 0.02) and a significant increase in latency was noted in group B (p = 0.005). Quality of life score on 6th post-operative month showed no significant difference between both the groups (p > 0.05). Level V dissection in MRND is associated with higher incidence and greater severity of shoulder dysfunction. AAS and SPADI score are useful tools in post operative follow up of shoulder dysfunction. NCS helps in the detection of neuropathy and to determine its severity. Early rehabilitation promotes long term recovery.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Head and neck malignancies are the commonest malignancies in Indian men and 3rd most common cancer in women as per population based cancer registries [1]. This is because of extensive use of tobacco in various forms-chewing, topical application on gums and smoking. Oral cancers are the most common among head and neck cancer [2].
Treatment modalities for head and neck cancers include surgical resection, chemoradiation or a combination of both. Neck dissection is a part of standard surgical treatment in head and neck cancers for diagnosis and treatment of metastasis to cervical lymph nodes. The extent of neck dissection depends on the “N” staging of the neck based on TNM classification [3]. Neck dissection can either be therapeutic or elective. Therapeutic neck dissection is performed in a case of clinically palpable or radiologically detectable nodal metastasis. Elective neck dissection is performed in cases where there is no evidence of nodal metastasis but the likelihood of microscopic lymphatic metastasis is high.
In modified radical neck dissection removal of nodal levels, I–V with preservation of accessory nerve [SAN] (type I), SAN with internal jugular vein [IJV] (type II) or SAN with IJV with sternocleidomastoid [SCM] (type III) is done. In Selective neck dissection (SND) preservation of one or more levels of lymph node is done [4].
Out of various complications of neck dissection, shoulder dysfunction is quite troublesome for the patient. Ewing and Martin first described “shoulder dysfunction following neck dissection” in 1952 [5]. It is mainly due to decreased trapezius function due to varying grades of injury to the SAN. Signs and symptoms are—atrophy of the trapezius muscle, loss of shoulder abduction, shoulder droop, pain in shoulder and neck and scapular dyskinesia [5,6,7].
The purpose of this study is to compare the shoulder function in patients undergoing modified radical neck dissection with those undergoing selective neck dissection and to assess the quality of life in both groups. We conducted this study as there is paucity of similar studies comparing outcomes of neck dissection in Indian subcontinent.
Materials and Methods
This prospective longitudinal comparative study was conducted in the Department of Otolaryngology and Head and Neck surgery at a tertiary care hospital from June 2020 to November 2021 after approval of the Institutional Ethics Committee (IEC). Patients with biopsy/FNAC proven head and neck malignancies undergoing neck dissection (modified radical or selective) were included in the study.
Patients with prior neck dissection, recurrent malignancy, prior chemo/radiotherapy, myopathy or neuropathy, uncontrolled diabetes mellitus or hypertension, pregnancy and coagulation abnormalities were excluded.
Patients fulfilling the inclusion and exclusion criteria were recruited in the outpatient setting. A detailed history, clinical examination and radiological investigation in the form of contrast enhanced CT and/or MRI were done to assess the site and size of the primary malignant lesion, cervical lymph nodal status and systemic metastasis. Clinical staging was done according to the 8th edition AJCC TNM staging system. Operability of the lesion was confirmed and surgical management i.e. primary resection, type of neck dissection (MRND or SND) and reconstruction options were planned in the Cancer clinic of the department. N + patients were planned for MRND (group A) and N0 patients were planned for SND (group B). Postero-lateral neck dissection cases were excluded.
Intraoperatively, SAN was identified in the anterior triangle and was traced till its insertion into the trapezius in case of MRND (Fig. 1). In SND, it was traced till its insertion into the SCM (Fig. 2). After surgery, specimens were sent for detailed histopathological evaluation. Post-operatively, patients were managed with intravenous antibiotics and analgesics according to the institutional protocols.

A Relation of SAN with the Erb’s Point (black arrow—Erb’s point; Blue arrow—SAN); note that the SAN lies nearly 1 cm above the Erb’s point; B Isolation of the SAN in the posterior triangle of the left side; the nerve can be seen entering the anterior border of the trapezius muscle

Submuscular recess area after dissection of level II lymph nodes of the left side (white arrowhead—SAN, blue arrowhead—IJV, yellow arrowhead-posterior belly of digastric)
Besides the routine investigations, the assessment of shoulder function was also done preoperatively and on subsequent follow-up using clinical and electrophysiological methods.
In Arm abduction test/score (AAS), the patient is asked to raise the arm and a score is given according to the angle up to which the patient can abduct his arm [8] [Appendix 1]. Ranges of shoulder abduction in various patients is shown in Fig. 3.

A Arm abduction score of 3(> 150° but < 180°) on 3rd post-operative month in a group A patient; B note that there is drooping of shoulder on the left side; C Arm Abduction score of 4(180° with pain) on 7th postoperative day in a patient of Group B; D Arm abduction score of 5(180° without pain) on 3rd post-operative month in another patient of Group B
The Shoulder pain and disability index (SPADI) was used to measure the shoulder pain and disability in outpatient setting. It contains 13 questions divided into 2 domains: pain score which contains 5 questions and disability score which contains 8 questions (Appendix 1) (12). AAS and SPADI scoring were recorded before surgery, at 1-week, 1 month, 3 months and 6 months post-operatively. Electroneurography (evoked electromyography) of the spinal accessory nerve of both sides was performed using NIHON KOHDEN electromyogram with software MEB-23 v 4.05 before surgery and on 3rd post-operative month by a single examiner who was unaware of the neck dissection type (Fig. 4).

A Stimulation of the SAN adjacent to the postero-superior part of SCM; B Biphasic compound muscle action potential waveform (blue arrow- stimulus artefact, black double headed arrow—latency, orange double headed arrow-amplitude)
Post operatively, all patients were referred to department of Physical medicine and rehabilitation for demonstration of shoulder exercises to be performed at home for at least 6 weeks. The physical treatment was directed at (1) pain relief (2) strengthening exercises and (3) range of motion exercises. The rehabilitation techniques used were gentle shoulder mobilisation exercises (pendulum exercise, passive forward flexion and external rotation and active assisted range of motion exercises). Before the start of these exercises, the patient was advised to apply a heat or ice pack to relieve pain.
Quality of life assessment was done using a questionnaire(NDQOL) based on the one used by Giordano et al. [8]. It consists of 7 questions each with a value between 1 and 5 with 1 being normal and 5 being severe impairment. The questionnaire was administered at 3rd and 6th post-operative month. (Refer to Appendix 1).
Statistical analysis was carried out using SPSS version 25. Descriptive analysis (age and gender) was done using Fischer exact test. For analysis of scores (Arm Abduction Scores and SPADI scores), intragroup analysis was done using Friedman’s 2-way analysis of variance and intergroup analysis using Kruskall–Wallis test. For analysis of continuous data (latency and amplitude on NCS) paired and unpaired t-test was applied. Correlation between clinical and electrophysiological data was analysed using Spearman correlation coefficient. P value of < 0.05 was considered to be significant.
Results
Out of 65 patients, 53 were male (82%) and 12 were female (18%). The mean age of patients in group A was 48 years (± 12.22) and in group B was 52 years (± 11). Smokeless tobacco was the most common risk factor (46%). pN0 was found in 37 patients (57%) and pN + in 28 patients (43%) out of which 19 were N1, 5 were N2 and 4 were N3. Oral cavity was found to be the most common site of malignancy (77%) (Table 1).
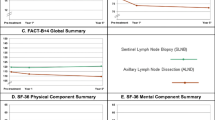
AAS was recorded in all the patients by clinically evaluating the angle of shoulder abduction using a goniometer. Mean pre-operative arm abduction score in both the groups was 5 as none of the patients had any shoulder joint pathology. In group A the decrease in abduction angle was significant till 3 months post-operatively when compared to baseline (p = 0.01) while in group B the same finding was noted till 1 month. There was a significant decrease in the arm abduction angle in group A as compared to group B at 1 week, 1-month and 6 months post-operatively (p = 0.01, 0.02 and 0.01 respectively). The proportion of patients having active shoulder abduction angle up to 180° without pain at 6th post-operative month was significantly higher in SND group [29(90.6%)-patients in SND-group vs. 21 patients (63.3%)-in MRND-group] (Table 5). Lowest AAS was seen 1 week post-operatively in both groups (mean score = 3.09 in group A and 3.63 in group B) following which there was improvement on subsequent follow-up visits (Table 2). The trend of AAS in both groups is shown in Fig. 5.

Line diagram showing the serial Arm Abduction scores in both groups
SPADI scores were significantly worse at 1 week, 1 month and 3 months post-operatively than the baseline values in both groups (Tables 2, 3 and 4). Worst mean score was seen 1 week post-operatively in both groups (88.39 in group A and 72.84 in group B). Intergroup comparison showed Group B patients having significantly better SPADI scores at 1 week, 1 month, 3 month and 6 month post-operatively than group A (p = 0.01 in all). (Fig. 6).

Line diagram showing average total scores in group A and B
In nerve conduction study, both the groups showed an overall decrease in amplitude and prolongation in latency at 3 months. In MRND group the decrease in amplitude and in SND group the prolongation in latency at 3 months post-operatively were significant (p = 0.02 and 0.005 respectively). On intergroup analysis, there was no significant difference in either the latency (p = 0.17) or the amplitude (p = 0.56) at 3rd post-operative month Tables 2, 3 and 4.
For NDQOL, intergroup analysis showed no significant difference in either the 3 months (p = 0.32) or the 6 months post operative score (p = 0.44) between the two groups. However, there was a significant improvement at 6th post-operative month in both the groups (p = 0.01 in both) Tables 2, 3 and 4, 5.
In group A there was a statistically significant correlation between arm abduction score and post operative amplitude and post-operative latency with a correlation coefficient of 0.43 and − 0.35 respectively (p = 0.01and 0.04 respectively). In group B, no significant correlation was found between clinical and electrophysiological parameters Table 6.
Discussion
The SAN after exiting from the jugular foramen, enters the anterior triangle either medial or lateral to the IJV the latter being more common [9, 10]. The styloid process, stylohyoid and digastric are lateral to the nerve. It then passes into (70–80%) or under (20–30%) the SCM. Within the muscle it forms the ansa of Maubrac with the cervical plexus (C2 and C3).
The nerve then exits through the posterior border of the SCM at the junction of upper 1/3rd and lower 2/3rd of the muscle. Erb’s point (also called the greater auricular point) is the point at which the greater auricular nerve (GAN) turns around the posterior border of the SCM. The SAN exits the SCM 1–2 cm above this point and then passes in a postero-inferior direction across the posterior triangle deep to the investing layer (Fig. 1). It is somewhat superficial in this position and is prone to injury during surgical manipulation. It then innervates the trapezius at the junction of middle and lower thirds of the muscle [11].
In modified neck dissection, SAN is skeletonized and isolated in its extracranial course starting from the jugular foramen till its entry into the anterior border of trapezius. This leads to traction injury and devascularization of the SAN although there is no gross injury to the nerve [12].
Selective neck dissection involves dissection in the submuscular recess which corresponds to level IIB lymph node. It is a relatively narrow area and dissection is this region can lead to traction injury and devascularization of the SAN due to inadvertent stretching. Therefore, both the types of neck dissection are reported to be associated with shoulder dysfunction in the post-operative period [13].
The low scores at 1-week can be explained by the post operative pain and inflammation following surgery and neuropraxia of the SAN. Another possible reason can be restriction of movement because of the presence of surgical drain and the pain associated with the stretching of the surgical wound. The improving trend in the AAS in subsequent follow-up can be attributed to the rehabilitation regime continued for a period of at least 6 weeks.
Group B patients had significantly better abduction scores at 6th post-operative month despite no significant difference at 3rd month between both groups. This highlights the need for longer follow-up periods to appreciate clinical improvement in such patients. Similar findings were reported by Imai et al. in their study from 2017 where significant improvement in active shoulder abduction was noted at 6 months as compared to 1 month. They also reported level V dissection and head and neck irradiation to be significant risk factors for shoulder dysfunction [14].
Previous studies from Cappiello et al. [8] and Giordano et al. [15] using various clinical and electrodiagnostic tests concluded that dissection of level V and sublevel IIB hampers the shoulder function to a greater extent even with preservation of SAN.
SPADI scores had the highest average value at 1-week post-op and then declined over a period of 6 months. It is noted that at the end of 6 months both groups had no significant difference in total scores compared to the baseline. However, it was also seen that group B have significantly lower total scores (lower means better) than group A at each of the post-op evaluation (1 week, 1 month, 3 months and 6 months). SPADI scoring acts as a handy tool and helps in early detection of any shoulder impairment, planning of a rehabilitation program for the patients and to record the response to the said rehabilitation program [16]. Initiating an appropriate physical therapy before the onset of fibrosis of the glenohumeral joint can greatly reduce shoulder impairment following surgery [17].The fragmentation of the total score into pain and disability scores gives a much more detailed analysis as compared to other questionnaires.
The decrease in post-operative amplitude in group A denotes axon loss in the SAN which is usually characterized by reduced or absent CMAP amplitudes [18]. When a nerve is infarcted or severely injured, Wallerian degeneration starts in the nerve segment distal to the lesion in anterograde direction. The amplitude decline starts after day 3 and is completed by day 5–8 [19]. Prolongation of latency is not commonly seen unless there is severe axon loss so as to involve the fastest nerve fibers [18].
In group B, there was significant increase in the post-operative latency values with non-significant difference in amplitude. This can be explained by the phenomenon of demyelination of the SAN. In case of uniform demyelination there is a decrease in conduction velocities without any change in amplitude whereas in nonuniform demyelination there is a decrease in amplitude. However, on NCS it is traditionally manifested as normal amplitude distal to the lesion and decreased amplitude proximal to the lesion [18]. The criteria for defining peripheral nerve demyelination include latency prolongation > 125% and slowing of conduction velocity to < 80% of normal values [20].
Our study showed a higher mean value in group B at both 3 and 6 months postoperatively than group A. This is despite the fact that group B patients have lower incidence of shoulder dysfunction and better recovery than group A. Also, there was no significant difference in the QOL scores between the 2 groups. This goes on to show that quality of life following neck dissection depends on multiple factors including the patient’s expectations as it is a purely subjective scale.
Significant improvement in NDQOL scores at 6 months provides us with a hope that post operative quality of life can be improved with proper rehabilitation and reassurance to the patient.
Conclusion
At the end of 6 month follow up of 65 patients undergoing neck dissection for head and neck cancers, we can conclude that there is greater degree of shoulder impairment after MRND owing to level V dissection. SND patients have early and sustained recovery in shoulder function with early rehabilitation. Despite early rehabilitation, the recovery might take months before being clinically detectable. The patients should be counselled regarding the same pre-operatively and motivated to continue the therapy with regular follow-up. Arm abduction scores act as a reliable clinical tool for evaluation and prognostication in patients.
Questionnaires like SPADI prove to be a reliable and simple tool for quick assessment of the shoulder function and to analyze the response to therapy. However, as it is a subjective test, should always be correlated with the clinical findings.
Nerve conduction study helps in diagnosing, localizing and also the grading the severity of the pathology. It is highly sensitive can aid in planning of rehabilitation and prognostication. It should be combined with needle electromyogram wherever possible to give a holistic idea about the status of the nerve and muscles.
Quality of life is a multifactorial entity and one should always try and maintain a balance between the oncological clearance and the functional outcome in head and neck cancer patients.
Limitations and Recommendation
In this study we have not taken into account certain risk factors like post operative radiotherapy and the type of reconstruction done. An analysis with taking these into consideration would provide a better knowledge about the associated factors of shoulder impairment. Further subdivision of groups based on level IIB dissection could be done for a deeper understanding. Homogenous groups compared according to primary subsite involved would also provide a more detailed analysis. A longer follow up period would also add more value to the study in terms of assessing the recovery of function and quality of life in the such patients.
References
Asthana S, Patil RS, Labani S (2016) Tobacco-related cancers in India: A review of incidence reported from population-based cancer registries. Indian J Med Paediatr Oncol 37(3):152–157
Dandekar M, Tuljapurkar V, Dhar H, Panwar A, DCruz AK (2017) Head and neck cancers in India. J Surg Oncol 115(5):555–63
Amin MB, Edge S, Greene F, Byrd DR, Brookland RK, Washington MK, Gershenwald JE (2018) AJCC cancer staging form supplement. Ajcc cancer staging manual, 8th edn. Springer, Berlin, pp 303–10
Robbins KT, Clayman G, Levine PA, Medina J, Sessions R, Shaha A et al (2002) Neck dissection classification update: revisions proposed by the American Head and Neck Society and the American Academy of otolaryngology-head and neck surgery. Arch Otolaryngol Head Neck Surg 128(7):751–758
Ewing MR, Martin H (1952) Disability following “radical neck dissection” An assessment based on the postoperative evaluation of 100 patients. Cancer 5:873
Cheng A, Schmidt BL (2008) Management of the N0 neck in oral squamous cell carcinoma. Oral Maxillof Surg Clin North Am. https://doi.org/10.1016/j.coms.2008.02.002
Bradley PJ, Ferlito A, Silver CE, Takes RP, Woolgar JA, Strojan P et al (2011) Neck treatment and shoulder morbidity: still a challenge. Head and Neck. https://doi.org/10.1002/hed.21495
Giordano L, Sarandria D, Fabiano B, Bussi M, Del Carro U (2012) Shoulder function after selective and superselective neck dissections: clinical and functional outcomes. Acta Otorhinolaryngol Ital 32(6):376–379
Rhoton ALJ, Buza R (1975) Microsurgical anatomy of the jugular foramen. J Neurosurg 42(5):541–550
Soo KC, Hamlyn PJ, Pegington J, Westbury G (1986) Anatomy of the accessory nerve and its cervical contributions in the neck. Head Neck Surg 9(2):111–115
Lloyd S (2007) Accessory nerve: anatomy and surgical identification. J Laryngol Otol 121(12):1118–1125
Popovski V, Benedetti A, Popovic-Monevska D, Grcev A, Stamatoski A, Zhivadinovik J (2017) Preservazione del nervo accessorio spinale nelle dissezioni del collo: Outcomes chirurgici e funzionali. Acta Otorhinolaryngol Ital 37(5):368–374
Giordano L, Sarandria D, Fabiano B, Del Carro U, Bussi M (2012) Shoulder function after selective and superselective neck dissections: clinical and functional outcomes. Acta Otorhinolaryngol Ital. 32(6):376–9
Imai T, Sato Y, Abe J, Kumagai J, Morita S, Saijo S et al (2021) Shoulder function after neck dissection: assessment via a shoulder-specific quality-of-life questionnaire and active shoulder abduction. Auris Nasus Larynx 48(1):138–47. https://doi.org/10.1016/j.anl.2020.06.013
Cappiello J, Piazza C, Giudice M, De Maria G, Nicolai P (2005) Shoulder disability after different selective neck dissections (levels II–IV versus levels II–V): a comparative study. Laryngoscope 115(2):259–263
Breckenridge JD, McAuley JH (2011) Shoulder pain and disability index (SPADI). J Physiother 57(3):197. https://doi.org/10.1016/S1836-9553(11)70045-5
Chaplin JM, Morton RP (1999) A prospective, longitudinal study of pain in head and neck cancer patients. Head Neck 21(6):531–537
Tavee J (2019) Nerve conduction studies: basic concepts. In: Levin KH, Chauvel P (eds) Clinical neurophysiology: basis and technical aspects, 1st edn. Elsevier, Amsterdam, pp 217–224. https://doi.org/10.1016/B978-0-444-64032-1.00014-X
Chaudhry V, Cornblath DR (1992) Wallerian degeneration in human nerves: serial electrophysiological studies. Muscle Nerve 15(6):687–693
Dimachkie MM, Barohn RJ (2013) Chronic inflammatory demyelinating polyneuropathy. Curr Treat Options Neurol 15(3):350–366
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendices
Appendix 1
Arm abduction score
Abduction angle | Score |
|---|---|
• Can raise up to 180° without pain/effort | 5 |
• Can raise up to 180° with pain/effort | 4 |
• Can raise up to > 150° but < 180° | 3 |
• Can raise up to > 90° but < 150° | 2 |
• Can raise up to < 90° | 1 |
Shoulder Pain and Disability Index (SPADI)
Please place a mark on the line that best represents your experience during the last week attributable to your shoulder problem.
Pain Scale
How Severe is your Pain?
Circle the number that best describes your pain where: 0 = no pain and 10 = the worst pain imaginable.
At its worst? | 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
When lying on the involved side: | 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
Reaching for something on a high shelf? | 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
Touching the back of your neck? | 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
Pushing with invoved arm? | 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
Disability Scale
How Much Difficulity do you Have?
Circle the number that best describes your pain where: 0 = no pain and 10 = so difficulty it requires help.
Washing your hair? | 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
Washing your back? | 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
Putting on an undershirt or jumper? | 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
Putting on a shirt that button down the front? | 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
Putting on your pants? | 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
Placing an object on the high shelf? | 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
Carrying a heavy object of 10 pounds (4.5 km) | 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
Removing something from your back pocket | 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
Neck Dissection Quality of Life Questionnaire (NDQOL)
Questions | Score |
|---|---|
• Are you bothered by neck or shoulder stiffness? | 1–5 |
• Are you bothered by tightness in your neck? | 1–5 |
• Are you bothered by pain in neck or shoulder? | 1–5 |
• Are you bothered by numbness of your neck? | 1–5 |
• Do you think your shoulder is dropped? | 1–5 |
• Have you been limited in your ability to reach above for objects because of your shoulder or neck? | 1–5 |
• Are you bothered by the appearance of your neck? | 1–5 |
• Total score | 7–35 |
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Mishra, A.K., Parida, P.K., Bhoi, S.K. et al. Shoulder Dysfunction and Quality of Life Following Modified Radical and Selective Neck Dissection: A Prospective Comparative Study. Indian J Otolaryngol Head Neck Surg 76, 3245–3255 (2024). https://doi.org/10.1007/s12070-024-04659-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12070-024-04659-y