
Abstract
Purpose
The extranodal extension (ENE) in head and neck squamous cell carcinoma (HNSCC) is a potential poor prognostic factor. Clinical ENE (cENE) was incorporated in the HNSCC staging system in the 8th edition of AJCC. There is not much evidence to support the treatment of HNSCC with cN3b with radiotherapy in radical intent. This study aims to assess the treatment outcome in patients of HNSCC with cN3b disease treated with definitive radiotherapy.
Method
Forty-five HNSCC patients with cN3b disease treated with definitive radiotherapy with or without concurrent chemotherapy between January 2018 to December 2018 were retrospectively evaluated.
Results
The median age of the study patients was 60 years (40–75years). Only 35 patients (77.8%) could complete the prescribed course of treatment, and the leading common cause of non-completion was treatment-related toxicities. After a median follow-up period of 9.3 months (range 2–33), the median OS and PFS were 22.6 months and 7.2 months, respectively. Fourteen patients (31.1%) in our study developed grade III/IV mucositis, and 11 (24.4%) developed severe grade III/IV dermatitis. The locoregional failure constituted 24 patients (53.3%).
Conclusion
The treatment outcome of HNSCC with cN3b disease is inferior. A personalized and subjective approach should be undertaken before choosing radiotherapy with a radical intent in this group of patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Head and Neck Cancer (HNC)is the seventh most common cancer worldwide, constituting 5.7% of global cancer-related mortality. Worldwide an estimated 67% of HNC cases and 82% of HNC deaths are reported from low- and middle-income countries [1, 2].
In India, HNC is the most common malignancy in males and the fifth most common in females. Northeastern states of India report a relatively higher incidence of HNC owing to higher consumption of bidis, betel quid, areca nut etc. [3, 4]. A recent report from National Cancer Registry Programme in India showed that most HNC patients (66.6%) were diagnosed in a locally advanced stage, making management strategies challenging [5].
Cervical lymph node metastases in head and neck squamous cell cancer (HNSCC) strongly indicate a poor prognosis, particularly N3 nodal disease [6]. The trend is to treat locally advanced HNSCC with N3 diseases with chemoradiation to improve tumour response, disease control, and organ preservation. However, there is an extreme paucity of data for this subgroup of patients.
One of the significant changes in HNC staging incorporated in the 8th edition of AJCC was that; N3 was divided into N3a and N3b. N3a; lymph node more than 6 cm in dimension, no extranodal extension (ENE) and N3b, any size with ENE [7].
In AJCC 7th, the presence or absence of ENE clinically, radiologically or pathologically was used as a descriptor and did not influence the nodal staging system. But the AJCC 8th edition introduced the criteria of ENE in the staging system. This pathological ENE (pENE) was defined as the extension of metastatic carcinoma from within the lymph node through the capsule and into the surrounding tissue. The minor ENE was defined as the extension of the carcinoma within 2 mm of the capsule. Major ENE was described as an extension of carcinoma cells beyond 2 mm of fibrous node capsule. But the AJCC 8th edition introduced the clinical criteria of ENE in the clinical staging system. Physical examination finding of overt tumour spread by fixation of the nodal mass to adjacent structures such as skin or muscles, dense tethering to adjacent structures, or dysfunction of a cranial nerve, the brachial plexus, the sympathetic trunk, or the phrenic nerve supported by radiological evidence, should be present to assign a status of ENE-positive. Incorporating clinical ENE (cN3b) leads to a stage migration of these advanced cancer patients to more advanced diseases with worse outcomes. Controversies exist regarding the optimum treatment of head and neck squamous cell carcinoma with cN3b disease. The variability in treatment approaches reflects the paucity of evidence to guide decision-making. No published literature is available for patients with N3b disease to establish the standard of care [8,9,10,11,12,13,14]. Evidence to support the treatment of HNSCC with cN3b patients with radiotherapy in radical intent is meagre. Therefore, this study has been undertaken to assess the treatment outcome in patients of HNSCC with cN3b disease treated with definitive radiotherapy.
Materials and Methods
This hospital-based retrospective study was carried out in compliance with the institutional policy after approval by the institutional ethical committee.
Patient Selection
All histologically proven HNC patients with N3b nodal disease as per the 8th edition of AJCC planned for definitive radiotherapy in the institutional multidisciplinary tumour board between January 2018 to December 2018 were included. Forty-five patients were eligible for the analysis during that specified period. All patient and treatment-related data were retrieved from the record of hospital files.
Diagnostic Workup
Pretreatment evaluation included a complete medical history, physical examination, and haematological and biochemical profiles. Diagnostic and staging investigations included pan endoscopy with biopsy and contrast-enhanced computed tomography (CECT) scan of the neck, thorax, and abdomen. Positron emission tomography (PET) CT scan was not mandatory. However, few patients underwent pretreatment PET-CT. Preradiotherapy dental check-up was carried out for all patients, and dental extraction, if deemed necessary, was performed. All patients underwent pretreatment speech and swallowing therapy evaluation and dietician consultation.
Treatment
The patients were immobilized in the supine position for radiotherapy using thermoplastic head-neck-shoulder mould. The radiotherapy was delivered using both conventional and three-dimensional conformal radiotherapy (3DCRT) technique using 6 MV photons. A dose of 66-70 Gy was prescribed for the primary and the gross nodal disease, and a dose of 60 Gy in 30 fractions was prescribed for the high-risk clinical target volume. Electron boost was considered for nodes that remained posteriorly out of the radiation portal after the 46 Gy when spinal cord shielding was done. Radiotherapy was delivered five fractions in a week. The patients were planned for concurrent chemotherapy either with inj Cisplatin 40 mg/m2 or with inj Carboplatin 2 AUC.
Follow-up and Assessment
During the radiotherapy treatment, patients were assessed weekly to evaluate and document acute toxicity [using Common Terminology Criteria for Adverse Events (CTCAE) v4.0]. After treatment completion, the patients were followed up every two months for one year and every three months through the first two years. During every follow-up, a complete physical examination, direct laryngoscopy and CECT of the neck were carried out.
Statistical Analysis
Baseline variables were depicted as numbers (percentage) and median. The follow-up period was measured from the day of completion of treatment to the day of the last clinic visit before analysis. The progression-free survival (PFS) and overall survival (OS) were calculated to measure treatment outcomes. Death from any cause was considered an event for calculating OS and was measured from the date of histologic diagnosis to the date of the last visit or death. PFS was calculated from the date of treatment completion to the time of disease progression, either local, regional or metastatic or death, whichever occurred earlier. Kaplan–Meir method was used to evaluate the survival rate, and the log-rank test was used to compare the survival among groups. P < 0.05 was considered as statistically significant at 95% confidence interval (CI). All the data were analyzed using IBM SPSS Statistics for Windows, version 21 (IBM Corp., Armonk, N.Y., USA).
Results
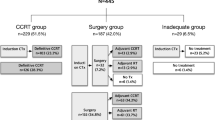
The hospital database was retrospectively reviewed between January 2018 to December 2018. Relevant clinical, pathological and cancer-specific data were reviewed. A total of 63 non-nasopharyngeal head and neck cancer patients with cN3b nodal disease were treated in the radiation oncology department during the specific period. Out of these, 45 patients planned for upfront definitive radiotherapy were included in the analysis (n = 45). The remaining 18 patients were not included as they received palliative radiotherapy as per the decision taken by the multidisciplinary tumour board.
Patient and Tumour Characteristics
Baseline patient and tumour characteristics are shown in Table 1. The median age of the study patients was 60 years (40–75years). Thirty-nine patients (86.6%) were male, and six (13.3%) were females. Most patients had a history of tobacco and beetle nut chewing (88.9%). Thirteen patients (28.9%) had a history of alcohol consumption.
The most common subsite of the primary tumour was the oropharynx (20 patients; 44.5%). It was followed by the hypopharynx (18 patients; 40%) and the larynx (4 patients; 8.8%). Three patients (6.7%) had neck nodes with unknown primary.
Moderately differentiated squamous cell carcinoma (MDSCC) was the predominant histology among the study cohort (36 patients; 80%), followed by poorly differentiated squamous cell carcinoma (PDSCC) (5 patients, 11.1%) and well-differentiated squamous cell carcinoma (WDSCC) (4 patient, 8.9%). The most common T-stage among the patients was T3 (27 patients, 60%), followed by T4a (10 patients, 22.2%).
The median nodal size of the study patients was 4 cm (range 3–10 cm). Twenty-two patients (48.9%) had a maximum nodal size between 3 and 6 cm, 14 patients (31.1%) had a nodal size of 3 cm or less, and nine patients (20%) had a node size greater than 6 cm. In 40 patients (88.9%), the nodal involvement was on one side of the neck, and five patients (11.1%) had bilateral neck nodal involvement.
Treatment Characteristics
As per the institutional multidisciplinary joint tumour board decision, all the patients in the study cohort received definitive radiotherapy with or without concurrent chemotherapy. Various treatment characteristics are shown in Table 2.
Thirty-five patients (77.8%) could complete the prescribed course of treatment, and ten patients (22.2%) could not complete the prescribed treatment. The most common cause of treatment non-completion was severe radiation-induced mucositis (6 patients). Other reasons owing to non-completion of treatment were; severe dermatitis (2 patients), progressive disease during treatment (1 patient) and defaulter (2 patients).
The median radiation dose was 66 Gy (54-70 Gy) in 2 Gy daily fractions, and the median duration of radiotherapy was 52 days (42–77 days).
Thirty-five patients (77.8%) received concurrent chemotherapy along with radiotherapy. Among these 35 patients, 12 (34.3%) received inj Cisplatin, and the remaining 23 (65.7%) received inj Carboplatin as concurrent chemotherapy.
After radiotherapy, four patients (8.8%) underwent surgery with radical neck dissection. A total of 16 patients (35.6%) received palliative chemotherapy after the completion of radiotherapy due to either residual or progressive disease.
Treatment Outcome and Prognostic Factors
After a median follow-up period of 9.3 months (range 2–33), the median overall survival (OS) was 22.6 months. The three-year overall survival of the patients was 36.90%. (Fig. 1). The median PFS of the entire patient cohort was 7.2 months, with a two-year PFS of 7.5% only.

Kaplan–Meier plot of overall survival (OS) and progression free survival (PFS)
The effect of potential prognostic factors, including gender, age, histology, T-staging, and use of chemotherapy drugs, were analyzed by the log-rank test for univariate analysis (Table 3).
There were no significant differences in OS and PFS regarding age or sex among the study patients. The PDSCC histology patients had statistically substantial improved PFS (p < 0.001) (Fig. 2). There was no difference in OS and PFS among the different subsites of the primary tumour (p = 0.8).

Comparison of OS and PFS among different histologic groups of primary tumours
The patients whose nodal size was less than 4 cm showed improved PFS at one and two years (43.5% and 8.7%, respectively) than those with nodal sizes more than 4 cm (29.4% and 5.9%, respectively). However, the difference could not reach statistical significance (p = 0.1, Fig. 3).

Comparison of OS and PFS with respect to size of the nodal mass
The primary tumour size is an important prognostic factor in the treatment outcome of head and neck cancer patients. The two-year OS of the patients T2 or less was 71.4%, followed by T3 and T4a patients (36.5% and 31.1%, respectively). The difference in OS was statistically significant (p = 0.02, Fig. 3). Similarly, the PFS at two years was also superior for small primary patients; however, the difference is not statistically significant (Fig. 4).

Comparison of OS and PFS among different T-stage groups
The use of concurrent chemotherapy and radiotherapy is the standard of care for treating locally advanced HNC unless contraindicated. The single-agent platinum drug, Cisplatin, is the cornerstone of therapy. However, Carboplatin can be used in patients with a high risk of cisplatin toxicity.
Thirty-five patients (77.8%) in our study population received concurrent chemotherapy. Table 2 shows that those receiving concurrent chemotherapy as a part of treatment had superior two-year- OS and one-year- PFS (43.7% vs. 16.7% and 40.6% and 25.5%, respectively). But the differences were not statistically significant (0.3 and 0.08, respectively, Fig. 5). Most patients in our study cohort received inj Carboplatin as concurrent chemotherapy. The OS at two years was more for patients receiving Cisplatin than those receiving Carboplatin (65.5% vs. 34.4%, respectively). However, this difference could not reach statistical significance (P = 0.08) (Fig. 5).

Comparison of OS and PFS based on concurrent chemotherapy
A radiation dose of 66 Gy or more to the gross primary and nodal disease is recommended in HNC radiotherapy. Thirty-one patients (68.9%) in our study population received a radiation dose of 66 Gy or more, and these patients had a superior OS and PFS at two- years when compared with those receiving any amount lower than 66 Gy (45.6% vs. 26.1% and 15.4% Vs 5.7% respectively). However, the differences are not statistically significant (P = 0.5 and 0.6, respectively).
Treatment-related Toxicity
Various treatment-related toxicities are depicted in Table 4. Eight patients (17.7%) developed grade III, and six (13.3%) developed grade IV oral mucositis during treatment. Grade III and IV dermatitis was reported by 11 patients (24.4%) during treatment. Eight patients (17.8%) developed grade II and III neutropenia during treatment. The patients who developed grade IV mucositis or dermatitis could not complete the prescribed radiotherapy treatment. They were managed conservatively. Xerostomia and dysphagia are two significant late complications of HNC radiotherapy. Eight patients (17.8%) reported grade III, and 19 (42.2%) reported late xerostomia during the follow-up period.
Patterns of Failure
The data retrieved from the hospital record showed that most patients had disease failure in both the primary and neck (Table 5). This locoregional failure constituted 24 patients (53.3%). Only one patient had isolated primary failure, and three patients had isolated nodal failure with controlled primary (6.7%). Five patients (11.1%) developed bone metastases, two patients (4.4%) developed lung metastases and two patients (4.4%) developed liver metastases.
Discussion
It is a well-accepted fact that the stage of nodal disease in head and neck squamous cell carcinoma is one of the most important prognostic factors in terms of local control and distant failure [15].
The factors that determine the nodal stage of N1-N3 in the AJCC 7th version, like the size, number and laterality, remained unchanged in the AJCC 8th ; however, an additional clinical criterion of extranodal extension (ENE) has been added. Earlier, ENE was a finding in postoperative specimens that carried poor HNC prognosis in published reports [16, 17]. In the newly added clinical criterion of N3b nodal disease, clinical examination findings of overt tumour spread by fixation of the nodal mass to adjacent structures like skin or muscles or evidence of nerve dysfunction suggesting nerve invasion was included. N3b nodal disease upstages the tumour to stage IVB carrying a poor prognosis. There is minimal data on treatment outcomes of HNC with N3 nodal disease; these are primarily retrospective series. However, to the best of our knowledge, this is the first of its kind to evaluate the treatment outcome of HNC patients with N3b nodal disease treated with definitive radiotherapy after introduction in AJCC 8th edition.
The present study included non-nasopharyngeal HNC patients with N3b nodes treated with definitive radiotherapy with or without concurrent chemotherapy between January 2018 to December 2018. Only 77.8% of the patients could complete the prescribed course of radiotherapy. The leading cause of treatment’s non-completion was severe toxicity like mucositis and dermatitis.
Witek M et al. evaluated the treatment outcome in 36 patients of HNC with N3 nodal disease. They found overall survival at 2 and 5 years for the entire cohort as 60% and 30%, respectively. After a median follow-up period of 9.3 months (range 2–33), the three-year overall survival of our patients was 36.90%. The two years PFS of our study patients were only 7.2%. Head to head comparison of our results with Witek M et al. can not be done as they included N3 nodes, and the N3b subset carries a worse prognosis by definition [18].
It was seen that the patients with early primary T stage had statistically significant superior OS (p = 0.02). Therefore decisions regarding HNC patients with advanced T stage with N3b node for radical treatment should be taken with caution. Andrew S. Jones and colleagues studied the role of radical intent treatment in 175 HNC patients having N3 nodal disease. They observed that the most important factor associated with the decision not to treat aggressively was advanced disease at the primary site (P = 0.0029) [19].
Those with unknown primary underwent planned neck dissection among our study patients after definitive radiotherapy. Among the different primaries, the patients with hypopharynx cancer showed superior OS and PFS at two years; however, the difference was not statistically significant. Patients with poorly differentiated squamous histology had superior OS and statistically significant improved PFS at two years (p < 0.002). Effects of other tumours and treatment-related prognostic factors affecting treatment outcomes are shown in Table 3. Like in all HNC, the patients who received concurrent chemotherapy in our cohort showed improved OS and PFS (p = 0.3 and 0.08, respectively). Although Carboplatin was used more as concurrent chemotherapy, the patients receiving Cisplatin showed superior OS at two years (65.6% vs. 34.4%).
Radiotherapy dose is an important prognostic factor in HNC patients treated with radical intent. The recommended dose should be 66 Gy or more for gross primary and nodal disease. In our cohort of patients, those receiving more than 66 Gy showed improved OS (45.6% vs. 261%) and PFS (15.4% vs. 5.7%) at two years.
The majority of the patients in our study were treated with conventional radiotherapy techniques, which is known to contribute more to acute and late toxicities. Fourteen patients (31.1%) in our study developed grade III/IV mucositis, and 11 (24.4%) developed severe grade III/IV dermatitis. Twenty-seven patients (60%) had a radiotherapy treatment duration of more than 50 days. The treatment gaps are because of various treatment-related toxicities. We understand that the treatment-related toxicities could have been lowered if intensity-modulated radiotherapy (IMRT) had been used. But in a high patient volume but resource-constrained centre like us, it is hard to treat every patient with IMRT.
Wang J et al. retrospectively evaluated 355 postoperative patients with laryngeal squamous carcinoma. Out of this, 22 patients (6.2%) had pathological ENE [20]. They have noticed that the ENE rate increased with the T-stage increase. This can be correlated with the present study, that 82.2% of patients in our study cohort had locally advanced primary tumour T3/T4. Wang et al. also concluded that the presence of ENE was associated with twice the hazards of death. But the major limitation of their results is that none of the patients received either radiotherapy or chemotherapy [17]. Dunee AA et al., in their meta-analysis of 9 studies including 2573 patients, reported that the presence of ENE had a significant negative impact on survival [21].
The presence of ENE, either radiological or clinical, is an independent prognostic factor for HNSCC. In a recent study from India, Mahajan A et al. evaluated the prognostic value of radiological extranodal extension in predicting outcomes in patients with locally advanced HNSCC treated with definitive chemoradiation. Out of 244 locally advanced HNSCC with metastatic nodes, 140 (57.3%) had radiological ENE. They reported that the radiological ENE-positive group had poor survival compared to the ENE-negative group 3-year OS (46.7% vs. 63.6%) and poor DFS (48.8% vs. 87%) [22].
Management of patients with N3b disease often reflects institutional patterns of care. In that regard, choosing the proper treatment approach that yields the highest therapeutic ratio of cure against morbidity is challenging. Historically poor response rates to bulky nodal disease in HNC treated with definitive RT led to the practice of planned neck dissection. But in our study, only four patients underwent planned neck dissection after completion of RT. On the contrary, 16 patients (35.6%) received palliative chemotherapy due to gross residual or disease progression. The lower rates of neck dissection may be attributed to increased radiation-induced morbidity. Another reason for less neck dissection is poor response at the primary site. Most of the patients (37, 82.2%) in our study cohort had locally advanced primary tumour T3/T4. Therefore care should be taken while offering radical intent radiotherapy for HNC patients with large primary tumours and cN3b disease, particularly when conventional radiotherapy techniques are planned.
This series carries several limitations inherent in retrospective analysis. Moreover, the sample size is also less, and the study population is heterogeneous. Another significant limitation of our study is that the patients were treated with conventional radiotherapy techniques. The relatively poor outcome in our group of patients may be mainly due to inadequate radiotherapy techniques. These very advanced groups of patients need more advanced conformal radiation techniques for a better outcome. However, we have tried to report the experience of treating this very advanced group of patients with definitive radiotherapy from a geographical area of relatively higher incidence but with limited resources. However, further research on homogenous patients in a prospective design with a larger sample size needs to be done.
Conclusion
The presence of ENE is widely used for predicting prognosis in HNC. A clinical terminology of cN3b was introduced in HNC staging in AJCC 8th edition. The presence of cN3b leads to clinical upstaging to stage IVb. There is an extreme paucity of data regarding the optimal management of this locally advanced disease. Very few retrospective series are available on this group of patients; however, role of radiotherapy as a prime treatment modality has not been reported so far. The survival outcome was relatively poor in this retrospective analysis of HNSCC with cN3b node treated with definitive radiotherapy. Therefore, a personalised and subjective approach should be undertaken before choosing radiotherapy with a radical intent in this group of patients. However, planned prospective research may help find the optimum management strategy for these patients.
References
Patterson R, Fischman V, Wasserman I, Siu J, Shrime M, Fagan J et al (2020) Global burden of Head and Neck Cancer: Economic Consequences, Health, and the role of surgery. Otolaryngology-Head and Neck Surgery 162(3):296–303
Global Burden of Disease Cancer Collaboration, Fitzmaurice C, Allen C et al (2017) Global, Regional, and National Cancer incidence, mortality, years of Life Lost, Years lived with disability, and disability-adjusted life-years for 32 Cancer Groups, 1990 to 2015: a systematic analysis for the global burden of Disease Study. JAMA Oncol 3:524–548
Addala L, Pentapati CK, Reddy Thavanati PK, Anjaneyulu V, Sadhnani MD (2012) Risk factor profiles of head and neck cancer patients of Andhra Pradesh, India. Indian J Cancer 49:215–219
Datta S, Chaturvedi P, Mishra A, Pawar P (2014) A review of indian literature for association of smokeless tobacco with malignant and premalignant diseases of head and neck region. Indian J Cancer 51:200–208
Mathur P, Sathishkumar K, Chaturvedi M, Das P, Sudarshan KL, Santhappan S, Nallasamy V, John A, Narasimhan S, Roselind FS, ICMR-NCDIR-NCRP Investigator Group (2020) Jul;6:1063–1075 ;. Cancer Statistics, 2020: Report From National Cancer Registry Programme, India. JCO Glob Oncol. doi: 10.1200/GO.20.00122. PMID: 32673076; PMCID: PMC7392737
Carsuzaa F, Dufour X, Gorphe P et al (2020) Locoregional control, progression-free survival and morbidity rates in N3 head and neck cancer patients with low primary tumour burden: a 301-patient study. Clin Otolaryngol 45:877–884
Amin M (2018) AJCC CANCER STAGING MANUAL, 8th edn. SPRINGER, Chicago
Edge S, Byrd D, Carducci M, Compton C (2009) AJCC Cancer staging manual, 7th edn. Springer Verlag, Berlin
Lydiatt W, Patel S, O’Sullivan B, Brandwein M, Ridge J, Migliacci J et al (2017) Head and neck cancers-major changes in the american Joint Committee on cancer eighth edition cancer staging manual. Cancer J Clin 67(2):122–137
Bernier J, Domenge C, Ozsahin M et al (2004) Postoperative irradiation with or without concomitant chemotherapy for locally advanced head and neck cancer. N Engl J Med 350(19):1945–1952
Cohen EE, Karrison TG, Kocherginsky M et al (2014) Phase III randomized trial of induction chemotherapy in patients with N2 or N3 locally advanced head and neck cancer. J Clin Oncol 32(25):2735–2743
Cooper JS, Pajak TF, Forastiere AA et al (2004) Postoperative concurrent radiotherapy and chemotherapy for high-risk squamous-cell carcinoma of the head and neck. N Engl J Med 350(19):1937–1944
Pajak KF, Trotti TF (2000) A radiation therapy oncology group (RTOG) phase III randomized study to compare hyperfractionation and two variants of accelerated fractionation to standard fractionation radiotherapy for head and neck squamous cell carcinomas: first report of RTOG 9003. Int J Radiat Oncol Biol Phys 48(1):7–16
Haddad R, O’Neill A, Rabinowits G et al (2013) Induction chemotherapy followed by concurrent chemoradiotherapy (sequential chemoradiotherapy) versus concurrent chemoradiotherapy alone in locally advanced head and neck cancer (PARADIGM): a randomized phase 3 trial. Lancet Oncol 14(3):257–264
Snow GB, Annyas AA, van Slooten EA et al (1982) Prognostic factors of neck node metastasis. Clin Otolaryngol 7:185–192
Wreesmann VB, Katabi N, Palmer FL et al (2016) Influence of extracapsular nodal spread extent on prognosis of oral squamous cell carcinoma. Head Neck 38(Suppl 1):E1192–E1199
de Juan J, García J, López M et al (2013) Inclusion of extracapsular spread in the pTNM classification system: a proposal for patients with head and neck carcinoma. JAMA Otolaryngol Head Neck Surg 139(5):483–488
Witek M, Wieland A, Chen S, Kennedy T, Hullett C, Liang E et al (2017) Outcomes for patients with head and neck squamous cell carcinoma presenting with N3 nodal disease. Cancers of the Head & Neck. ;2(1)
Jones A, Goodyear P, Ghosh S, Husband D, Helliwell T, Jones T (2010) Extensive Neck Node Metastases (N3) in Head and Neck squamous carcinoma. Otolaryngology–Head and Neck Surgery 144(1):29–35
Wang Z, Zeng Q, Li Y, Lu T, Liu C, Hu G (2020) Extranodal Extension as an independent prognostic factor in laryngeal squamous cell carcinoma patients. J Cancer 11(24):7196–7201
Dunne AA, Muller HH, Eisele DW, Kessel K, Moll R, Werner JA (1990) Meta-analysis of the prognostic significance of perinodal spread in head and neck squamous cell carcinomas (HNSCC) patients. European journal of cancer (Oxford, England: 2006; 42:1863-8
Mahajan A, Chand A, Agarwal U, Patil V, Vaish R, Noronha V et al (2022) Prognostic value of radiological extranodal extension detected by computed tomography for predicting outcomes in patients with locally advanced head and neck squamous cell cancer treated with radical concurrent chemoradiotherapy. Front Oncol. ;12
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical Approval
The study was approved by Institutional Ethics Committee; BBCI Medical Ethics Committee (Registration No: ECR/1040/Inst/AS/2018).
Conflict of Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Nath, J., Sarma, G., Samra, B. et al. Definitive Radiotherapy in Locally Advanced Head and Neck Squamous Cell Cancer with Clinical Extranodal Extension. Indian J Otolaryngol Head Neck Surg 75, 3519–3529 (2023). https://doi.org/10.1007/s12070-023-04041-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12070-023-04041-4