
Abstract
Tinnitus represents one of the most common and distressing otologic problems, and it causes various somatic and psychological disorders that interfere with the quality of life. This study aimed to compare the outcome of music therapy, tinnitus maskers and pharmacotherapy on patients with chronic tinnitus, to observe and analyse the etiological factors of tinnitus and to find out whether music can be used as an active listening mode by which tinnitus perception can be decreased. This was a comparative longitudinal study involving 90 patients with chronic tinnitus who were randomly assigned to 3 groups of 30 each: Group A (Music therapy), Group B (Pharmacotherapy) and Group C (Tinnitus masker). After a detailed clinical history and examination, Tinnitus Handicap Inventory and Visual Analogue Scores were recorded both prior to and following therapy, and patient were followed up monthly up to 2 months. There is a significant difference in the mean THI score (p = 0.002) and mean VAS(p = 0.0006) at 2 months follow up in patients treated with Music therapy and patients had a satisfactory outcome after music therapy and did not require any further treatment. Patients in pharmacotherapy and hearing aid group had a good clinical improvement but mean THI and mean VAS score was not statically significant. It was also noticed that loud noise exposure and hypertension were main etiological factors in 37.77% and 26% of patients respectively. Music therapy appears to be an effective and cost-efficient mode of therapy for chronic tinnitus and could be suitable for widespread implementation for patients with tinnitus of varying severity. Pharmacotherapy and hearing aid application in the treatment of tinnitus has good outcome in our study but requires long term treatment and follow up.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Tinnitus is the perception of sound in the absence of an actual external sound, and represents a symptom of an underlying condition rather than a single disease. It represents one of the most common and distressing otologic problems, and it causes various somatic and psychological disorders that interfere with the quality of life [1]. A population based study of hearing loss in adults aged 48–92 years found that tinnitus had a prevalence of 8.2% at baseline and an incidence of 5.7% during a 5 year follow-up [2].
Tinnitus has been treated in a number of different ways, including tinnitus masking, counselling, tinnitus retraining therapy, pharmacotherapy and more recently, music therapy. The Tinnitus Retraining Therapy (TRT) proposed by Jastreboff and colleagues is an approach to the treatment of tinnitus through two main stages- psychological counselling and sound therapy, which is aimed at decreasing the strength of the abnormal neural activity involved in tinnitus [3]. The music therapy approach is a more recent development, and is a modification of the TRT in which music is applied to the patient’s therapy routine. This therapy includes counselling (to decrease negative feelings towards one’s own tinnitus), singing (especially in frequencies near or at that of the tinnitus), listening to music (as a means of distraction from the tinnitus) and awareness of one’s own body is encouraged through music [4].
The pharmacological treatment of tinnitus remains a subject of much debate as currently, no drug exists with an indication for tinnitus. Extensive reviews of randomized clinical trials have revealed that usage of Gingko biloba and antioxidants are more beneficial than placebo. Gingko biloba extract has been shown to have therapeutic effects on symptoms of cerebral insufficiency including memory disturbances and other cognitive defects, such as tinnitus [5].
The fitting of masking devices plays an important part in the management of many different forms of tinnitus. Tinnitus maskers are small devices worn like hearing aids. They give relief from tinnitus by giving out a “white noise” or ultrasonic signal, to cover up the internal sounds heard [6].
This study attempted to compare the outcome of music therapy, tinnitus maskers and pharmacotherapy on patients with chronic tinnitus and to find out whether music could be used as an active listening mode by which tinnitus perception could be decreased.
Materials and Methods
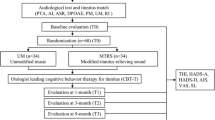
This was a comparative longitudinal study, which was conducted at a rural tertiary care hospital over a period of 18 months. The Institutional Medical Ethics Committee approval was obtained for this study. From January 2015 until June 2016, 90 patients aged 18 years and older with complaints of chronic tinnitus presenting to the Outpatient Department of Otorhinolaryngology and Head and Neck Surgery were enrolled in the study after obtaining written informed consent from the patients. The inclusion criteria included patients with chronic subjective tinnitus for 3 months or more and with normal hearing or mild/moderate hearing loss. Patients excluded from the study included patients with severe or profound hearing loss, severe or acute neurological or medical or psychiatric conditions, obvious pathological causes of tinnitus, objective tinnitus and history of current alcohol or drug abuse.
The patients underwent a thorough history taking and clinical examination, the findings of which were recorded in a structured proforma. Next, the pre-treatment Tinnitus Handicap Inventory (THI) scores and Visual Analogue Scale (VAS) scores were recorded. The patients were then subjected to Pure Tone Audiometry and Impedance audiometry. Following this, the patients were assigned to three groups by a computer-generated table of random numbers, with 30 patients in each group: Group A- Music therapy, Group B- Pharmacotherapy and Group C- Tinnitus maskers. The patients received their assigned mode of therapy for a period of one month, following which, the patients were reviewed at the end of the 1st and 2nd months. At each review, the post-treatment THI and VAS scores were recorded. The results obtained were statistically analysed.
Patients in the music therapy group received counselling on the first day, followed by 50 min-long sessions of pleasant relaxing music of the patients’ choice on alternate days from Monday to Saturday, for one month. The music was delivered to the ears via high quality Phillips headphones and a Walkman mp3 music player. The volume was adjusted by the patient until a suitable volume was achieved which just masked the tinnitus.
Patients in Group B (pharmacotherapy) received Gingko biloba in doses of 25–100 mg/kg/day, along with antioxidants. Patients were monitored for the development of adverse reactions. Patients in Group C received a consultation with the audiologist and were then prescribed tinnitus maskers to the affected ears, depending on the amount of hearing loss for a period of one month. The patients were then taught the proper method of use and maintenance of the tinnitus maskers and were advised to report back in the eventuality of any discomfort or complications.
In order to avoid bias, all cases were followed up and scored by the principal investigator. Statistical analysis was carried out using SPSS version 19.0 (IBM SPSS, US) software with Regression Modules installed. Descriptive analyses were reported as mean and standard deviation of continuous variables. Statistical comparison between the groups was performed using Chi-square analysis for categorical variables and t-test and ANOVA for continuous variables. All tests were two-tailed and significance level was set at p < 0.05.
Results
90 patients were included in the study over a period of 18 months. The majority of patients (26.67%) were in the 61–70 years age group, while a minimum of 4.4% patients were below 30 years. The overall mean age was found to be 47.5 ± 14.71 years (Range 22–80 years, Median 47.5 years). There was a male preponderance (60%) as compared to females (40%) (Male to female ratio = 1.5:1).
We studied the characteristics of tinnitus in the study population in terms of intensity, volume, onset, description, influence and fluctuation. (Table 1) Across the three groups, a majority patients (53.3%) had chronic tinnitus of intermittent intensity. A majority of patients in Groups B (66.7%) and C (53.3%) suffered fluctuating tinnitus, while most patients in Group A (66.7%) had a constant tinnitus. Most patients in the study population have a history of gradual onset of tinnitus, with the majority having a tonal type of tinnitus. The major factors influencing the onset of tinnitus were found to be stress, sleeplessness and smoking. Perception of tinnitus was found to be more in the morning (20%) in Group A, more in the evening (20%) in Group B and more at night (30%) in Group C.
The major outcome measures for this study were pre- and post-intervention Tinnitus Handicap Index (THI) scores and pre- and post-intervention VAS scores. On analysis of THI scores, patients across the three groups showed gradual and steady improvement in their symptoms, although patients in Groups B and C did not show statistically significant changes in index scores at the end of the 2nd month of the intervention, as compared to Group A patients which showed a statistically significant improvement in index scores, thereby demonstrating a slight advantage of music therapy over pharmacotherapy and tinnitus maskers in the relief of chronic subjective tinnitus over a short time interval. (p = 0.02) (Table 2).
The VAS scoring was done at the initial assessment, 1st follow up at the end of 1 month and at 2nd follow up at the end of second month. Similar to the findings of THI scores, a considerable relief of perception of tinnitus was found in patients who underwent music therapy as opposed to the other two modalities of therapy, and this difference was found to be statistically very significant. (p = 0.0069) (Table 3).
Discussion
In this study carried out in a rural tertiary care hospital, the total study group consisted of 90 patients in which, a clear male preponderance was seen. The range of age group with maximum susceptibility to disease was found to be between 41 and 70 years (66.66%). According to an epidemiological analysis in patients with tinnitus by Aage Moller et al [7] , tinnitus is common in the elderly over the age group of 65–74 years. The overall male to female ratio in our study was found to be 1.5:1 which agrees with the findings of Morgenstern and Biermann et al [8] who found a male preponderance in tinnitus patients.
A study conducted by Fukuda et al [9] showed intermittent tinnitus in most of the patients, while a study conducted by Miriam Grapp et al [10] for assessing Music therapy as an early intervention to prevent chronification of tinnitus showed that 52% patient had a clear tonal tinnitus and 34.8% patients categorized their tinnitus as noise like. These findings were similar to those of the present study. Goebel G et al [11] showed that 10–20% of patients’ tinnitus is not influenced by any environmental factors which was reflected in our study with (27%). Stouffer JL et al [12] showed that common detrimental activities and/or conditions like noise exposure, being located in a quiet place, emotional stress, loss of sleep, and physical exhaustion are commonly associated with tinnitus, whereas our study showed a relationship with stress and emotional states (12%), sleeplessness (17%), smoking (15%) and occupational noise exposure (10%). Tinnitus was reported to be louder upon awakening by Levin RA et al [13] who suggested the involvement of somatic factors, such as bruxism. He also reported that tinnitus vanishes during sleep but returns within few hours, further suggesting that psychosomatic factors, such as neck muscle contractions occurring in an upright position or jaw clenching, play etiological roles.
Music therapy is a recent addition to the treatment options for chronic subjective tinnitus. A study by Heike Argstatter et al [14] on long term benefits of music therapy in tinnitus revealed that 87% of patients had a satisfactory outcome and 71% did not undergo any further treatment. In the present study, music therapy showed statistically significant reduction in THI scores (p = 0.02) and VAS scores (p = 0.006). Music therapy employs specific musical elements such as sound, rhythm, melody, harmony and tempo to mask tinnitus levels and thereby reduces perception of tinnitus. Santiago et al [15] found that music therapy facilitates positive interaction and has been found to reduce anxiety levels and facilitates relaxation by acting on the autonomic nervous system. Reduction of perception of tinnitus further promotes reduction in anxiety and stress levels.
Malcolm P Hilton et al [16] showed that pharmacotherapy with Ginkgo biloba had a good outcome in a majority of patients with chronic tinnitus. While the results of our study did show that pharmacotherapy was associated with some relief of symptoms, this change was not statistically significant. Similarly, outcome after the use of tinnitus maskers was not statically significant on assessing the patients with THI and VAS score for 2 months post-intervention. These findings may be explained by the short duration of follow up post-intervention. A long-term community cohort study may help crystallize the long term therapeutic effects of music therapy in the treatment of chronic tinnitus. A study by Elisabeth Peltier et al [17] on long term tinnitus suppression with hearing aids concluded that hearing aids can be used for a long term benefits.
References
Han BI, Lee HW, Kim TY, Lim JS, Shin KS (2009) Tinnitus: characteristics, causes, mechanisms and treatments. J Clin Neurol 5(1):9–11
Nondahl DM, Cruickshanks KJ, Wiley TL, Klein R, Klein BE, Tweed TS (2002) The role of zinc in management of tinnitus. Auris Nasus Larynx 29:329–333
Jastreboff PJ (2007) Tinnitus retraining therapy. In: Langguth, B.; Hajak, G.; Kleinjung, T.; Cacase, A.; Moller, AR., editors. Progress in Brain Research. Vol. 166. Elsevier Science; Oxford, UK:2007.Pp.415–423
Nickel AK, Hillecke T, Argsttater H, Bolay HV (2005) Outcome research in music therapy. Ann N Y Acad Sci 1060:283–293
Murai K, Tyler RS, Harker LA, Stouffer JL (1992) Review of pharmacological treatment of tinnitus. Am J Otol 13:454–464
Hazell JWP, Wood SM, Cooper HR, Stephens SDG, Corcoran AL, Coles RRA, Baskill JL, Sheldrake JB (1985) A clinical study of tinnitus maskers. Br J Audiol 19:65–146
Aage Moller (2011) Epidemiology of Tinnitus in Adults. Chapter 5. Textbook of Tinnitus. Doi: https://doi.org/10.1007/978-1-60761-145-5_5
Morgenstern C, Biermann E (1997) Long term therapy of tinnitus with Ginkgo biloba extract EGb 761®. Fortschr Med Orig 115(4):57–58
Shargorodsky Josef et al (2010) Prevalence and characteristics of tinnitus among US Adults. Am J Med 123(8):711–718
Grapp M et al (2013) Music therapy as an early intervention to prevent chronification of tinnitus. Int J Clin Exp Med 6(7):589–593
Goebel G, Buettner U (2004) Basics of tinnitus: diagnostics and therapy. Psychoneuro 30(6):322–329
Stouffer JL, Tyler RS, Kileny PR, Dalzell LE (1991) Tinnitus as a function of duration and etiology: counselling implications. Am J Otol 12:188–194
Levin RA (2004) Somatic tinnitus. In: Snow JB (ed) Tinnitus: theory and management. BC Decker Inc., Ontario, pp 108–124
Argstatter H et al (2012) Long term effects of the “Heidelberg model of music therapy” in patients with chronic tinnitus. Int J Clin Exp Med 5(4):273–288
Pérez-Lloret S, Diez J, Domé MN, Delvenne AA, Braidot N, Cardinali DP, Vigo DE (2014) Effects of different “relaxing” music styles on the autonomic nervous system. Noise Health 16:279–284
Hilton MP, Zimmermann EF, Hilton Hunt WT (2013) Ginkgo biloba for tinnitus. Cochrane Database Syst Rev. https://doi.org/10.1002/14651858.CD003852.pub3
Elisabeth Peltier et al. (2012) Long-term tinnitus suppression with linear octave frequency transposition hearing aids. PLOS ONE. 7 (12): e51915
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The author declared that there is no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Sruthi, N., Venkataramanujam, N.C., Karthikeyan, P. et al. A Comparative Study of Treatment Outcomes of Music Therapy, Tinnitus Maskers and Pharmacotherpy in Chronic Subjective Tinnitus. Indian J Otolaryngol Head Neck Surg 74, 185–189 (2022). https://doi.org/10.1007/s12070-021-02799-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12070-021-02799-z