
Abstract
Dermoid cysts of the head and neck are a rare entity. These cysts are benign cystic malformations and histologically composed of tissues originating from ectoderm and mesoderm. Dermoid cysts usually presents as midline neck mass and rarely appear in lateral region. These are extremely rare in parotid gland, however should be considered as a differential in the list of parotid mass. There are a few cases published till date. Superficial parotidectomy is suggested as surgical treatment, however sometimes enucleation is also sufficient. There are only very few case reports published on dermoid cysts in parotid glands. We present a rare case of this entity and the challenges faced in making diagnosis with a short review of the literature.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Dermoid cysts of the head and neck are rare benign lesions accounting for about 7% of all such cysts [1]. Dermoid cysts usually presents as midline neck mass and rarely appear in lateral region. Only a few cases involving parotid glands has been reported so far. These cysts can be congenital or acquired. Congenital cysts arise from a rest of embryonic epithelium whereas acquired cysts are a result of traumatic implanted skin in deeper layers [2]. Histologically, it is composed of tissues originating from ectoderm and mesoderm. These are lined by stratified squamous epithelium with variable amount of pilosebaceous units and sweat glands supported by a fibrous connective tissue wall.
The incidence of dermoid cyst in parotid gland is very low. 7% of all dermoid cysts are seen in head and neck region and 80% of them predominantly occur in the orbit, floor of mouth and nose [3,4,5]. More than 50% of these in head and neck region cases are detected by the age of 6, though approximately one-third are present at birth [6]. These cysts are generally asymptomatic unless they grow enough to be conspicuous, causing cosmetic problems or compressive effects.
In this article, we describe about a mystical case of dermoid cyst of parotid gland, and discuss its management.
Case Report
37 years old lady with no known co-morbidities presented with complaints of swelling in the (R) parotid region for the last 8 years. It was insidious in onset and progressively increasing in size which made the patient to seek consultation. There is no history of pain associated with swelling and facial weakness of the right side of the face.
On examination there was 3 cm × 3 cm mobile, soft, non-tender, smooth globular swelling involving the parotid. Overlying skin was normal. There were no palpable neck nodes and rest of the ENT examination was essentially normal (Fig. 1).

Swelling involving Rt parotid
MRI of the neck revealed a well-defined, non-enhancing, homogenous, smooth and lobulated mass involving the superficial lobe. Fat planes were preserved all around the mass. The superficial lobe was pushed anterolaterally and retromandibular vein was pushed medially (Fig. 2). USG parotid revealed the mass to be cystic and there were no intraparotid lymph nodes or internal vascularity in the mass. FNAC of the mass was suggestive of a lipoma. There was no evidence of any malignancy.

Hypointense mass on T1 image and hyperintense on T2
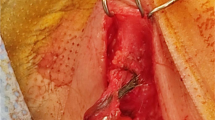
On the basis of above findings patient was planned for superficial parotidectomy. Intraoperatively, the facial nerve trunk was identified. The cystic lesion was seen in the region of tail parotid and extending between superficial and deep lobe, cranial and extending deep to main facial nerve trunk. Trans parotid excision of cyst was done by gently dissecting superficial lobe from deep lobe preserving facial nerve branches. Superficial lobe was reflected caudally and cystic mass was excised thereby saving the parotid tissue (Figs. 3, 4). Postoperatively patient developed paresis of the marginal mandibular branch and temporal branch of facial nerve which recovered completely after 2 weeks (Fig. 5). Histopathological examination of the excised mass was consistent with dermoid cyst.

Cystic mass noticed extending in between superficial and deep lobe (white arrow); superficial lobe retracted caudally (yellow arrow)

Excised cyst

Post-operative pic; no facial paresis
Discussion
The dermoid cyst is a rare, congenital, epithelial lined, cystic cavity that contains tissues of both mesodermal and ectodermal origin. Most dermoid cysts in the head and neck region occur around the orbital, oral and nasal regions (80%). Out of these, orbital dermoids are 49.5%, nasal dermoids 12.6%, submental and submaxillary dermoids account for 23% and the remainder 14.6% [2].These locations are the fusion sites of many embryonic structures and hence prone for dermoid cyst formation [7]. Dermoid cyst in parotid gland is rare and only few case reports are available in literature. Cystic lesions account for 2–5% of all parotid gland lesions [8].
Dermoid cysts generally are painless swellings without infiltration into surrounding important structures like facial nerve or skin. These cystic lesions are either congenital or acquired. The congenital lesions are most often ectodermal in origin and they include branchial cleft cysts/lymphoepithelial cysts. The acquired cysts can be due to obstructions, neoplasms, calculi and traumatic implantation of epithelium [9].
Clinico-radiological evaluation is often ambiguous which makes pre-operative diagnosis difficult. A large number of differential diagnosis includes mucous retention cyst, unilateral blockage of the parotid duct, benign mesenchymal tumors like lipoma, fibroma, hemangioma or neurofibroma, branchial cleft cyst, benign salivary gland tumors like pleomorphic adenoma, Warthin’s tumor and malignant salivary gland tumor like muco-epidermoid tumor [7, 8]. Ultrasonography, CT, MRI, and FNAB can be performed. Ultrasound is able to differentiate between solid, vascular and cystic lesions. MRI and CT may give an idea about the location and relation of mass with the surrounding tissue, but cannot give a final preoperative diagnosis.
MRI of a dermoid cyst typically depicts a cystic mass, hypointense on T1-weighted images and hyperintense on T2-weighted ones with peripheral enhancement on contrast. Some dermoid cysts have variable signal intensity on T1 weighted images which may be hyperintense because of the presence of sebaceous lipid [9].
FNAC may provide reliable information on cystic lesions if there are supporting radiologic findings, but can also be misleading because some well-differentiated squamous cell carcinomas and malignant lesions showing squamous metaplasia may share the benign-looking cytologic features with dermoid cysts. Hence the definitive diagnosis should always be made by histopathologic examination [2]. Similarly Baschinsky et al. [10] also did not consider the FNAC as a definitive diagnostic modality.
New and Erich [4], on the basis of hypothesized pathogenesis and microscopic appearance classified these cysts into three following categories:
1. Congenital dermoid cysts of teratoma type: they arise from the embryonic germinal layers. Depending on the dormant layer, they can contain skin, hair or teeth etc. They are almost always limited to the ovaries and testes. 2. Acquired dermoid cysts: they are inclusion cysts as a result of traumatically implanted skin in the deeper tissues. They occur on the hands and the other exposed parts of the body. 3. Congenital inclusion dermoid cysts: these develop from inclusions of displaced dermal cells along the lines of embryologic fusion. This category is subdivided into four subgroups: (a) cysts around the eyes and orbits, originating along the nasooptic groove, (b) those around the nose, resulting from intrusion of the frontonasal plate, (c) those around the floor of the mouth, and in submental and submaxillary regions, originating from the 1st and 2nd branchial arches, (d) those around the suprasternal, suboccipital, thyroidal, lower lip and palate, most of which occur along the mid-ventral or mid-dorsal lines of the body.
Dermoid cysts are treated by surgical removal. Since, they are generally encapsulated and therefore dissection is simple. Superficial parotidectomy is generally performed for treatment of the parotid dermoid cyst. In our case, however, we did not perform superficial parotidectomy as the mass could be dissected in toto without sacrificing the superficial lobe. In all kinds of surgical intervention, careful dissection of the nerves from the cyst wall is paramount to prevent damage which may potentially cause neurologic deficits [11].
In our case, on the basis of FNAC and MRI findings preoperative diagnosis of lipoma had been made. In view of available diagnosis, it was decided that the mass be excised trans parotid after lifting the superficial lobe and preserving all branches of facial nerve. The soft cystic mass was identified in between superficial and deep lobe, the mass was dissected free of salivary gland tissue and excised in toto without any evidence of residual or satellite mass. There is no evidence of recurrence after 06 months of follow up.
Conclusion
Dermoid cysts of the parotid gland are rare benign lesions, with only few cases having been reported in the literature. Dermoid cysts can be considered as a differential diagnosis in cases with a recurrent, painless enlargement of the parotid gland which has a soft consistency. Pre-operative diagnostic work up is important, this helps in formulating surgical plan. The treatment of these cysts is surgical excision, in a few cases enucleation of cyst may be sufficient.
References
Moody AB, Avery CM, Harrison JD (1998) Dermoid cyst of the parotid gland. Int J Oral Maxillofac Surg 27(6):461–462
Naujoks C, Handschel J, Braunstein S, Emaetig F, Depprich R, Meyer U, Kübler N (2007) Dermoid cyst of the parotid gland—a case report and brief review of the literature. Int J Oral Maxillofac Surg 36(9):861–863
Taylor BW, Erich JB (1967) Dermoid cysts of nose. In: Mayo clinic proceedings, vol 42, no. 8, p 488
New GB (1937) Dermoid cysts of the head and neck. Surg Gynecol Obstet 65:48–55
Smirniotopoulos JG, Chiechi MV (1995) Teratomas, dermoids, and epidermoids of the head and neck. Radiographics 15(6):1437–1455
Pryor SG, Lewis JE, Weaver AL, Orvidas LJ (2005) Pediatric dermoid cysts of the head and neck. Otolaryngol Head Neck Surg 132(6):938–942
Islam S, Hoffman GR (2009) Parotid dermoid cyst: a rare entity. J Laryngol Otol 123(2):1–4
Choi EC, Jin JB, Kim JY, Hong WP, Kim MJ, Park YK (1988) Dermoid cyst of the parotid gland. Yonsei Med J 29(2):199–203
Mukunyadzi P (2002) Review of fine-needle aspiration cytology of salivary gland neoplasms, with emphasis on differential diagnosis. Pathol Patterns Rev 118(suppl_1):S100–S115
Baschinsky D, Hameed A, Keyhani-Rofagha S (1999) Fine-needle aspiration cytological features of dermoid cyst of the parotid gland: a report of two cases. Diagn Cytopathol 20(6):387–388
Damar M, Erdem D, Dinç AE, Bişkin S, Bahadır B (2015) Dermoid cyst of the parotid gland. ENTcase 1(3):191–194
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interests.
Ethical Approval
The research involving a human participant.
Informed Consent
Written informed consent was obtained from participant included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Dwivedi, G., Gupta, V., Patnaik, U. et al. Dermoid Cyst of the Parotid Gland: A Rare Entity. Indian J Otolaryngol Head Neck Surg 71 (Suppl 1), 809–812 (2019). https://doi.org/10.1007/s12070-018-1560-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12070-018-1560-8