
Abstract
Myringoplasty is one of the commonest operations performed on the middle ear. Our aim was to compare the results of endoscopic permeatal myringoplasty with that of conventional myringoplasty by post aural approach using operating microscope. A total of 120 patients having central perforation of tympanic membrane were randomly divided into two equal groups of 60 patients each. In the first group, endoscope was used and in the second group microscope was used to do myringoplasty. Temporalis fascia was used as a graft material. The patients were kept in follow-up for 1 year. The pre-operative and post-operative audiograms, post-operative pain, graft uptake and time taken for surgery were compared in both the groups. The graft uptake rate was 91.67% in the endoscopic group, whereas it was 93.3% in the microscopic group. Post-operative pain was significantly less in the endoscopic group as compared with microscopic group and not much difference was found in the gain in A-B gap in either group. The mean ABG gain was 16.16 dB (SD = 4.68) in endoscopic group and 19.54 dB (SD = 3.45) in microscopic group. On applying the Mann–Whitney U test, this finding was statistically significant (p value = 0.0001). In our study success rate was equal between endoscopic and microscopic technique. In terms of morbidity and postoperative recovery endoscope produced better results. Endoscopic tympanoplasty can be a good alternative of microscopic tympanoplasty.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The microscope revolutionised the surgical management of ear diseases but the basic optical properties of microscope have remained the same for the last 30 years [1]. In spite of various technical advancements in operating microscope, basic limitations could not be resolved [2]. With the advent of the rigid endoscopes for sinus surgery other extended applications in other fields have emerged. Mer and colleagues introduced the middle ear endoscopy in 1967. Since then endoscopes are increasingly used for various middle ear surgeries [3]. Though endoscopes were mainly introduced for sino nasal surgeries, its use is no more restricted to nasal surgeries with surgeons using the scope to access other areas like ear, larynx, skull base etc. [4, 5]. Usually myringoplasty is done by post aural or endaural approach using operating microscope, after advent of rigid endoscope surgeons are using them for ear surgeries like tympanoplasty, ossiculoplasty, myringotomy and grommet insertion [6, 7]. Endoscopes have lot of advantages over microscope. Unlike microscope, endoscope is easily transportable and hence ideal for use in ear surgery camps. There is paucity of data on endoscopic myringoplasty [1]. Also, more importantly there are very few comparative studies between traditional microscopic techniques and endoscopic techniques [1]. Hence there is a need of a comparative study between the microscopic and endoscopic techniques of myringoplasty. Our study is mainly aimed at evaluating the role and efficacy of rigid endoscopes in myringoplasty and compare myringoplasty done permeatally with help of rigid endoscopes with that of myringoplasty done by post aural approach using operating microscope.
Materials and Methods
This study was conducted at the department of otolaryngology of Navodaya Medical College, Raichur in Karnataka state from January 2011 to December 2013. The study was started after getting clearance from the institutional ethical committee of the institution. Written informed consent was taken from all the patients included in our study. A total of 120 patients were selected having central perforation of tympanic membrane. These 120 patients were randomly divided into two equal groups of 60 patients each. All patients were given serial numbers on first come first serve basis. The technique for dividing groups was simple randomization with odd serial numbers allotted for endoscopic technique and even serial numbers allotted for microscopic technique. All the patients underwent myringoplasty under local anaesthesia. All the cases were operated by a single surgeon. In the first group, endoscope was used and in the second group microscope was used to do myringoplasty. The technique used for endoscopic surgery was endomeatal tympano-meatal flap technique. Temporalis fascia was used as a graft material in both the methods of surgery. The patients were kept in follow-up for 1 year. The pre-operative and post-operative audiograms, post-operative pain, graft uptake and time taken for surgery were compared in both the groups. Mann–Whitney U test was used for statistical analysis and statistical significance (p value) calculated.
The selection criteria followed were:
Inclusion criteria-(1) Patients of chronic suppurative otitis media (CSOM) with dry central perforation presenting to the outpatient department. (2) patients of tubotympanic chronic suppurative otitis media with conductive hearing loss less than 40 dB (3) Dry ear for at least 6 months previously. Exclusion criteria-(1) Patients with active ear discharge or with history of episode of ear discharge in previous 6 months. (2) Patients with post-operative residual and recurrent perforations of tympanic membrane. (3) CSOM patients with ossicular chain abnormalities. (4) Patients with sensorineural hearing loss. (5) Patients with secondary cholesteatoma and granulation tissue in middle ear.
Surgical Procedure:
All these patients underwent surgery under local anaesthesia. The patient is premedicated with intramuscular injections of 1 ampoule fortwin, 1 ampoule phenergan and 1 ampoule glycopyrrolate. The external auditory canal is then anesthetised using 2% lignocaine with 1 in 200,000 adrenaline injection. Temporalis fascia graft is harvested under local anaesthesia conventionally and allowed to dry.
In endoscopic myringoplasty, 0° 4 mm rigid endoscope was used for the surgery. A 30° 4 mm rigid endoscope was used for some time in the middle of the surgery to inspect the middle ear cavity after the tympano-meatal flap was elevated. To begin with, using the 0° 4 mm endoscope, the margin of the perforation is freshened using a sickle knife or an angled pick. Using a circular knife a curvilinear incision is made about 5 mm lateral to the annulus extending between 11-o clock and 1 o-clock position. The skin is slowly elevated away from the bone of the external canal. The annulus is elevated and the middle ear mucosa is incised. This is followed by elevation of tympano meatal flap from the handle of malleus to access the middle ear cleft. After skeletonising the malleus handle, we place the temporalis fascia graft by underlay technique. The tympano-meatal flap is kept back over the temporalis fascia graft. Bits of gelfoam are placed over the tympanomeatal flap (Figs. 1, 2).

In endoscopic myringoplasty, malleus was skeletonised and tympano meatal flap was positioned antero-superiorly before placing the graft

In endoscopic myringoplasty, temporalis fascia was placed below the handle of malleus
In microscopic myringoplasty, after local infiltration in the post-aural region, Wilde’s incision was given to expose the external auditory canal. After retracting the pinna anteriorly using a Mollison’s retractor, the margin of the perforation is freshened using a sickle knife. The tympanomeatal flap was elevated 5 mm away from the tympanic annulus and the malleus handle is skeletonised. The temporalis fascia graft is placed below the handle of the malleus and spread uniformly. The tympano-meatal flap is spread back over the temporalis fascia. Bits of gelfoam are placed over the tympanomeatal flap. Post aural wound is sutured with 3-0 silk, which was removed after 1 week.
All the patients were discharged on second post-operative day with oral antibiotics and analgesics for 7 days. The patients were followed up for a minimum period of 1 year. The follow-up duration after surgery was 1 week, 2 weeks, 1 month, 2 months, 3 months, 6 months and 1 year. Audiometric assessment was done at 6 months and 1 year duration post-operatively. The final audiometric assessment done at 1 year end in all the patients was taken for analysis in our study. We did not lose any patient in our follow-up as we were in touch with our patients through mobile communication. However, in the endoscopic group, 5 patients were irregular in their follow-up and in the microscopic group, 4 patients were irregular in their follow-up. Notably, these patients were the ones with surgical failures.
Results
In the endoscopic group, out of 60 patients, 39 were males and 21 were females. The average age in this group was 28.5 years. In the microscopic group, out of 60 patients, 26 were males and 34 were females. The average age in this group was 31.4 years. There was no past history of ear surgery in any member of both the groups. The endoscopic group patients were discharged the same day evening after surgery, while the microscopic group patients were discharged the next day.
In the endoscopic myringoplasty group, after the first week after surgery, 46 patients out of 60 had intact ear drum and by 4th week after surgery, 52 patients out of 60 had intact ear drum. At the end of 1 year follow up, 55 patients had intact ear drum (Fig. 3). In the 5 patients who had graft failure, all had developed post-operative infection and they were irregular in their follow up. In the microscopic myringoplasty group, after the first week after surgery, 51 patients out of 60 had intact ear drum and by 4th week after surgery, 54 patients out of 60 had intact ear drum. At the end of 1 year follow up, 56 patients had intact ear drum. In the 4 patients who had graft failure, all the 4 patients had developed post-operative infection and were not regular in their follow-up. Hence, in our study, the graft uptake rate in endoscopic myringoplasty was 91.67% and in microscopic myringoplasty was 93.3%. Even though there was more number of persons showed intact ear drum at first, fourth week and one year after microscopic myringoplasty compared to endoscopic myringoplasty but the difference was not statistically significant in all the time period (p value > 0.05).

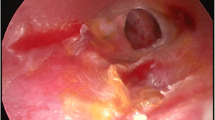
1 year follow up picture of a case of endoscopic myringoplasty shows successful graft uptake
In the endoscopic myringoplasty group, pre-operative air-bone gap was 30–35 dB in 44 patients and 35–40 dB in 16 patients. All the 55 cases of graft uptake cases of this group had an mean pure tone Air-Bone gap of 34.16 dB pre-operatively. All these 55 cases of graft uptake of this group had a mean pure tone Air-Bone gap of 18 dB at the end of 1 year follow up. Remaining 5 cases of graft failure did not show improvement in Air-Bone gap for obvious reasons. In the microscopic myringoplasty group, pre-operative air-bone gap was 30–35 dB in 41 patients and 35–40 dB in 19 patients (Fig. 4). All the 56 cases of graft uptake cases of this group had a mean pure tone Air-Bone gap of 35.54 dB pre-operatively. All the 56 cases of graft uptake cases of this group had a mean pure tone Air-Bone gap of 16 dB at the end of 1 year follow up. Remaining 4 cases of graft failure did not show improvement in Air-Bone gap. Hence, in our study, postoperative air bone gap was less than 20 dB in 91.67% of the patients in endoscopic group and 93.3% in microscopic group. The mean ABG gain was 16.16 dB (SD = 4.68) in endoscopic group and 19.54 dB (SD = 3.45) in microscopic group (Fig. 4). On applying the Mann–Whitney U test, this finding was statistically significant (Mean of ranks is 56 and Standard Deviation is 169.5. U statistic value = 880, Z-score = 3.89, p value = 0.0001).

Chart showing the air-bone gap levels pre- and post-operatively in both endoscopic and microscopic techniques
In endoscopic group no patient required bony canaloplasty while among microscopic group 8 patients required bony canaloplasty during the surgery to deal with the canal wall bulge. Higher number of patients undergoing microscopic myringoplasty needed bony canaloplasty compared to endoscopic myringoplasty and this difference was statistically significant (p value = 0.003).
The average time taken for surgery was less in the endoscopic group (1 h) as compared to the microscopic group (2 h).
The post-operative pain score as assessed using the WILDA’s pain assessment guide was found to be 5 in case of post aural myringoplasty as compared to 4 in case of endomeatal endoscopic myringoplasty.
Discussion
In our study, we found that the results of endoscopic technique and microscopic technique are similar with respect to graft uptake as well as hearing improvement. The endoscopic technique however, gave us added advantages like reduced surgical time, reduced post-operative pain and morbidity and reduced post-operative hospital stay.
Rigid endoscopes were first developed by Hopkins, using rod shaped glass lenses in the relay system [8, 9]. The rod lens provides a wider viewing angle and exceptional resolution and brightness [10]. The use of endoscopes in field of Otorhinolaryngology was initially limited to the nose, but with due course of time it is widely be used in various other surgeries like ear and micro laryngeal surgery.
The endoscopic myringoplasty offers the following advantages: (1) It visualizes the whole tympanic membrane and the ear canal without having to manipulate the patient’s head or the microscope. (2) It extends the operative field in transcanal procedures into structures usually hidden under the microscope (anterior tympanic perforation, posterior pocket, facial recess, and hypotympanum). (3) It is easier to visualize structures from multiple angles as opposed to the microscope’s single axis along the ear canal. (4) It provides extremely sharp image with high resolution. (5) The time duration of the surgery is reduced. 6) The post-operative pain and morbidity is reduced. (7) The average duration of hospital stay is reduced. Disadvantages of the endoscopic myringoplasty include the one-handed surgical technique, a loss of depth perception, limited magnification and the need for training [11, 12].
In our study, endoscopes allowed us close inspection and photo documentation of the tympanic membrane perforation, the drum remnant, the eustachian tube orifice, the middle ear mucosa and ossicular chain without elevation of tympanomeatal flap. The anatomical variations (tortuous or stenotic ear canal, anterior meatal overhang etc. that hamper the view of entire tympanic membrane during ear surgery were overcome by the use of endoscopes. Moreover, the permeatal route avoided post aural incision, resulting in less operative time and postoperative pain and morbidity. The patients were discharged on-the evening of the same day of surgery where as the patients of the microscopic group were discharged next day morning due to postoperative pain.
The results of endoscopic myringoplasty are comparable to the conventional myringoplasty done under operating microscope. In our study, there was 91.67% graft uptake rate in endoscopic group as compared to 93.3% in microscopic group. Postoperative air bone gap was less than 20 dB in 91.67% of the patients in endoscopic group and 93.3% in microscopic group. The mean ABG gain was 16.16 dB (SD = 4.68) in endoscopic group and 19.54 dB (SD = 3.45) in microscopic group. The above results are consistent with the earlier studies. In 2008, Satyawati Mohindra et al. did 49 cases of myringoplasty and 6 cases of ossiculoplasties through the transcanal route using rigid endoscopes. The success rate regarding perforation closure was 91.5% and average air bone gap improvement was 22.24 dB in the myringoplasty groups [4]. Ahmed ELGuindy (Tanta, Egypt) has evaluated the role of the rigid endoscope in the management of 36 cases of dry central perforation of the tympanic membrane. The graft uptake rate was 91.7% and air bone gap was closed to less than 10 dB in 83.3%. He used endoscope along with the manometry to evaluate the tubal function before ear surgery [8]. Previous comparative studies show that graft uptake rates are similar in both endoscopic and microscopic techniques of myringoplasty (Table 1).
In our study, in endoscopic group, no patient required bony canaloplasty while among microscopic group 8 patients required bony canaloplasty during the surgery to deal with the canal wall bulge. While operating the patient with microscope, tortuosity of the EAC and bony overhang hampers the view of the deeper structures. Because of which we need to frequently manipulate head of the patient. Sometimes, in spite of manipulations deeper structures could not be visualised. In such condition, bony canaloplasty becomes mandatory. This in turn may increase operative time. In contrast, endoscope can be easily negotiated through curvy External Auditory Canal. Thus endoscope brings surgeon’s eye to the tip of the scope. The wide angle of scope brings the tympanic membrane in one frame; more over the image can be magnified by just getting close to the structures. Thus there is no need of frequently manipulating patients head and moreover meatoplasty can be avoided [13]. Similar observations were made in two separate studies by Tarabichi [14] and Usami et al. [15].
In our study, the average time taken for surgery was less in the endoscopic group (1 h) as compared to the microscopic group (2 h). This was because the endoscopic group avoided post-aural incision and suturing. Also, the post-operative pain score as assessed using the WILDA’s pain assessment guide was found to be 5 in case of post aural myringoplasty ascompared to 4 in case of endomeatal endoscopic myringoplasty. In microscopic group temporalis fascia was used as a graft which was taken from a larger post aural incision with obvious more tissue dissection. In endoscope group, temporalis fascia was harvested through a smaller incision in temporal region with minimum tissue dissection. Thus endoscope group had relatively early wound healing and less morbidity in terms of postoperative pain and hospital stay as compared to microscopic group. Quraishi et al. has also reported about less post-operative pain and morbidity in their endoscopic myringoplasty series [16]. Also, unlike microscope, endoscope is easily transportable and hence ideal for use in ear surgery camps [13].
Blood soils the tip of endoscope which obscures the surgical field. So, while performing endoscopic myringoplasty, meticulous haemostasis is must for doing smooth surgeries. This problem can be solved by developing a stand for endoscope, which can fix the scope in desired position so both hands are free to operate [13]. Endoscopes provide monocular vision which leads to loss of depth perception [2]. So one has to be extra careful, while close to vital structures and positioning of the graft. This difficulty may be overcome by experience. Savlon is used as a defogging agent for endoscopes. Studies on effect of savlon on middle ear mucosa and inner ear are not sufficient, thus safety of savlon is yet to be established [13].
There are 2 major safety concerns with endoscopic ear surgery. One is excessive heat dissipation. This was evident only when a xenon light source was used. Adequate illumination of the middle ear space can be accomplished with lower settings on the regular light source (because of the size of the cavity) without the need of the xenon systems. Also, the tip of the endoscope requires continuous cleaning with antifog solution, which probably helps in cooling the endoscope. The other safety concern is accidental patient movement with secondary direct trauma by the tip of the endoscope. The relatively large diameter of the endoscope (4 mm) used in the study and the anatomy of the ear canal and middle ear space will usually preclude the introduction of the endoscope beyond the tympanic ring [5].
Our study was done with 60 patients in the endoscopic group and 60 patients in the microscopic technique group. Also, we have used simple randomisation technique while deciding the technique of myringoplasty to our patients. We had 5 patients in the endoscopic myringoplasty group and 4 patients in the microscopic myringoplasty group who were not properly motivated for regular follow-up which led to infection and subsequent failure in graft uptake. All these limitations of our study can be overcome by future studies with larger sample group, better randomization techniques and motivated patients who can come for regular follow-up.
Our study aimed at comparing the endoscopic technique and the microscopic technique for myringoplasty. All our patients underwent myringoplasty using temporalis fascia graft. There are several studies which suggest tragal cartilage and perichondrium graft placed as a butterfly fashion is equally efficient as a graft for myringoplasty during endoscopic technique [17, 18]. Further studies are required using the autologous tragal chondro-perichondrial graft. We have used 0° and 30° 4 mm rigid endoscopes during our endoscopic surgery. While some studies have used only 0° rigid 4 mm endoscope alone for myringoplasty [1], some have used all 0°, 30° and 70° rigid 4 mm endoscopes for myringoplasty [5]. Both the groups are having successful outcomes with regards to graft uptake and hearing improvement. We feel that 0° and 30° endoscopes should suffice for a successful tympanoplasty. Endoscopic myringoplasty avoids bony canaloplasty as it can be negotiated even in a curvy external auditory canal. On the other hand, bony canaloplasty becomes essential while doing myringoplasty using microscope in a curvy external auditory canal [14, 15].
The endoscopic technique is the future of myringoplasty and tympanoplasty. With results similar to the microscopic techniques and the added advantages, the endoscope may become more popular than the microscope. The endoscope holds the greatest promise in tympanoplasty and cholesteatoma surgery and should increase the utilization of transcanal over post-auricular procedures [5, 9]. Minimally invasive endoscopic and endoscope-assisted surgical techniques are increasingly being employed in the surgical management of cholesteatoma as they help in good visualization of residual cholesteatoma sites, such as the anterior and posterior epitympanic spaces, sinus tympani, facial recess, and hypotympanum. The endoscope is also being used for transcanal stapedotomy, endoscopic repair of cerebro-spinal fluid otorrhoea, management of meniere’s disease, management of perilymphatic fistulae and endoscopic cochlear implantation [19]. Thus endoscope holds the greatest promise in ear surgery in coming days.
Conclusion
Panoramic, wide angle, and magnified view provided by endoscope as well as ability to easily negotiate through EAC and uninterrupted picture overcomes most of the disadvantage of microscope. In our study success rate was comparable between endoscopic and microscopic technique. In terms of morbidity and postoperative recovery, endoscope produced better results. Loss of depth perception and one handed technique are some of the disadvantage of endoscope that can be overcome with practice and use of endo-holder. Thus endoscopic myringoplasty can be a good alternative of microscopic myringoplasty. In future endoscopes may be utilised for all types of ear surgeries like tympanoplasty, stapedotomy cholesteatoma surgeries and cochlear implant.
References
Harugop AS, Mudhol RS, Godhi RA (2008) A comparative study of endoscope assisted myringoplasty and microscope assisted myringoplasty. Indian J Otolaryngol Head Neck Surg 60:290–302
Glasscock ME, Shambaugh GE (2003) Tympanoplasty. In: Glasscock and Shambaugh, surgery of the ear, 5th edn. People’s Medical Publishing House, Connecticut, pp 350–370
El-Guindy A (1992) Endoscopic transcanal myringoplasty. J Laryngol Otol 106:493–495
Mohindra S, Panda NK (2010) Ear surgery without microscope; is it possible. Indian J Otolaryngol Head Neck Surg 62(2):138–141
Raj A, Meher R (2001) Endoscopic transcanal myringoplasty—a study. Indian J Otolaryngol head neck surg 53(1):47–49
Kakehata S, Futai K, Sasaki A, Shinkawa H (2006) Endoscopic transtympanic tympanoplasty in the treatment of conductive hearing loss: early results. Otol Neurotol 27(1):14–19
Buckingham RA (1963) Endoscopic otophotography. Laryngoscope 73:71–74
EL-Guindy A (1993) Endoscopic transcanal myringoplasty. J Laryngol Otol 106:493–495
Mc Kennan KX (1993) Endoscopic second look mastoidoscopy to rule out residual epitympanic—mastoid cholesteatoma. Laryngoscope 103:810–814
Kennady DW (1997) Endoscopic sinus surgery. Otolaryngol Clin N Am 30:313–330
Fry TL, Newton DF (1979) Otoscopy and photography. Ann Otolaryngol 88:771–773
Konrad HR et al (1979) Paediatric otoscopy and photography of the tympanic membrane. Otolaryngology 105:431–433
Patel J, Aiyer RG, Gajjar Y, Gupta R, Raval J, Suthar PP (2015) Endoscopic tympanoplasty vs microscopic tympanoplasty in tubotympanic CSOM: a comparative study of 44 cases. Int J Res Med Sci 3(8):1953–1957
Tarabichi M (1999) Endoscopic middle ear surgery. Ann Otol Rhinol Laryngol 108:39–46
Usami S, Iijima N, Fujita S et al (2001) Endoscope-assisted myringoplasty. Otorhinolaryngology 63:287–290
Quraishi MS, Jones NS (1995) Day care myringoplasty using tragal perichondrium. Clin Otolaryngol 20:12–14
Parelkar K, Nagle S, Jagade M, Thorawade V, Khairnar P, Attakil A, Pandare M, Nataraj R, Hanwate R, Kar R (2015) Triple-c cartilage tympanoplasty: case series. Int J Otolaryngol Head Neck Surg 4:26–31
Fernandes SV (2003) Composite chondro-perichondrial clip tympanoplasty: the triple-C technique. Otolaryngol Head Neck Surg Off J Am Acad Otolaryngol Head Neck Surg 128:267–272
Lela M, Michael W (2015) Minimally invasive transcanal endoscopic ear surgery, endoscopy—innovative uses and emerging technologies. In: Associate Prof. Amornyotin S (ed), InTech. doi: 10.5772/60551. http://www.intechopen.com/books/endoscopy-innovative-uses-and-emerging-technologies/minimally-invasive-transcanal-endoscopic-ear-surgery
Lakpathi G, Reddy LS (2016) Comparative study of endoscope assisted myringoplasty and microscopic myringoplasty. Indian J Otolaryngol Head Neck Surg 68:185. doi:10.1007/s12070-016-0970-8
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Jyothi, A.C., Shrikrishna, B.H., Kulkarni, N.H. et al. Endoscopic Myringoplasty Versus Microscopic Myringoplasty in Tubotympanic CSOM: A Comparative Study of 120 Cases. Indian J Otolaryngol Head Neck Surg 69, 357–362 (2017). https://doi.org/10.1007/s12070-017-1147-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12070-017-1147-9