
Abstract
Atrial myxomas are the most common cardiac tumors, rarely presenting with both systemic embolization and intracranial aneurysms. A 34-year-old woman presented with acute limb ischemia of both lower limbs and right upper limb and on evaluation was diagnosed with left atrial myxoma and intracranial aneurysms. She underwent embolectomy and intracranial aneurysm repair followed by successful excision of left atrial myxoma after 4 weeks. This case is reported for the rare association of myxoma with intracranial aneurysm along with systemic embolization which has not been reported in the literature.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Atrial myxomas are the most common cardiac tumors [1, 2]. Clinical features are usually dependent on the location of the tumor, propensity of systemic embolization, or non-specific constitutional symptoms. Here, we describe a patient who had a myxoma with multiple cerebral aneurysms and systemic embolization, which is rare.
Case report
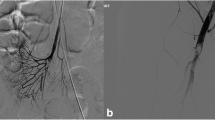
A 34-year-old female presented to the emergency department with complaints of severe pain in both lower limbs and the right upper limb for the past 6 hours. On evaluation, there was absence of pulse in bilateral popliteal, femoral, anterior tibial, posterior tibial, dorsalis pedis, and in right brachial, right radial, and ulnar arteries. Acute limb ischemia was suspected and urgent computed tomography (CT) angiography of the abdominal aorta until bilateral lower limbs and bilateral upper limbs was done. CT angiography revealed hypodense filling defect in the infra-renal abdominal aorta extending until the bilateral common iliac arteries and also in the right brachial artery until its bifurcation (Fig. 1a and b).

a Filling defect in the right brachial artery. b Filling defect in the bilateral common iliac arteries
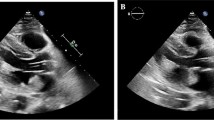
The patient was started on heparin as per acute limb ischemia protocol with serial activated partial thromboplastin clotting time (aPTT) monitoring and aPTT was kept in the range of 60–80 s. Following initial stabilization, the patient underwent echocardiography, which revealed 41 × 30 mm mass in the left atrium (LA) attached to the inter-atrial septum, prolapsing into the left ventricle (LV) (Fig. 2a and b) and causing moderate mitral regurgitation. After obtaining informed consent, the patient was then taken up for Fogarty’s embolectomy surgery which was done via bilateral femoral approach and a large myxomatous tissue was removed (Fig. 3a). Fogarty embolectomy was also done from the right brachial artery and similar myxomatous tissue was extracted (Fig. 3b). Postoperatively, the patient had pulses in both lower limb femoral, popliteal, anterior tibial, posterior tibial, dorsalis pedis, and in right brachial, radial, and ulnar arteries. Histopathology confirmed it to be myxoma.

a Left atrial mass. b Moderate mitral regurgitation

a Myxomatous tissue removed from the right femoral artery. b Myxomatous tissue from the right brachial artery
The patient also had history of transient ischemic attacks for which CT of the brain was done to look for any tumor embolization, which surprisingly revealed multiple saccular aneurysms from bilateral cerebral arteries with right temporal hematoma. The reason for cerebral bleed was probably due to rupture of one of the larger aneurysms (Fig. 4). She then underwent right temporal craniotomy and excision of larger aneurysm uneventfully. After 4 weeks, she was taken up for LA myxoma excision. Median sternotomy was done. Systemic heparinization followed by aorto-bicaval cannulation was performed and cardiopulmonary bypass (CPB) initiated. Trans-right atrial LA myxoma excision was done under mild hypothermic cardioplegic arrest. The resulting defect was closed with an autologous pericardial patch. She had an uneventful postoperative period. On follow-up after 6 months, she was asymptomatic, able to perform her household activities, and all peripheral pulses were palpable, and echocardiography revealed no residual tumor with an LV ejection fraction of 65%.

Multiple intracranial aneurysm
Discussion
Cardiac tumors are amongst the rare diseases of the heart with an incidence of 0.02%. Atrial myxomas constitute more than 50% of all benign cardiac neoplasms with majority arising from the LA [1, 2]. The patient may present with symptoms of cardiac failure, depending upon the site of mass and level of obstruction caused by the mass. Patients also exhibit a variety of neurologic syndromes even in the absence of cardiac symptoms [3]. Systemic embolization is the second frequent presentation (29%) in patients with left atrial myxomas and embolization occurs frequently to cerebral vessels resulting in stroke (21%) [4]. There are also some rare neurological complications associated with myxoma such as cerebral aneurysms [5, 6] and myxomatous metastasis [3, 7, 8]. In the index case, it was a combination of cardiac myxoma with cerebral aneurysms and systemic embolization.
Cerebral aneurysms following cardiac myxomas are rare. The true incidence of myxoma-related aneurysms is unknown with only around 40 cases reported in the literature. Aneurysms secondary to cardiac myxoma may present before or after excision of the primary tumor. These aneurysms are usually multiple with fusiform or saccular shape, but mostly fusiform (91%) [5, 6]. In the present case, it was multiple with both fusiform and saccular types and was present before excision of the primary tumor.
The mechanism for aneurysm formation has not been well understood. The theory of “Metastasize and Infiltrate” remains the most acceptable one. Myxoma fragments metastasize to the brain and infiltrate the arterial wall thereby interrupting the elastic lamina, leading to vessel dilatation and aneurysm formation. Histological studies have demonstrated proliferation of myxoma cells in the wall of aneurysms and interruption of the internal elastic lamina by invading cells. The same picture was seen in our patient’s histopathological examination [5, 6].
Magnetic resonance imaging (MRI) and CT scans can detect small infarcts, cerebral hemorrhage, or cerebral infarction. Myxomatous aneurysms on MRI may appear as tubular outpouchings of cerebral arteries within the sulci on T1- and T2-weighted images. On a CT scanner, aneurysms appear hyperdense spontaneously secondary to the accumulation of myxoid matrix in the wall of the aneurysm [8].
Resection of LA myxoma requires CPB support. Considering the risks of the extension of intracranial bleed in our patient, the cardiac surgery was delayed by 4 weeks.
Conclusion
The triad of cardiac myxoma with intracranial aneurysm along with systemic embolization should be kept in mind in evaluating cardiac myxoma patients and preoperative CT or MRI of the brain should be mandatory to prevent disastrous complications.
References
Radoi MP, Stefanescu F, Arsene D. Brain metastases and multiple cerebral aneurysms from cardiac myxoma: case report and review of the literature. Br J Neurosurg. 2012;26:893–5. https://doi.org/10.3109/02688697.2012.692841.
Lee VH, Connolly HM, Brown RD Jr. Central nervous system manifestations of cardiac myxoma. Arch Neurol. 2007;64:1115–20. https://doi.org/10.1001/archneur.64.8.1115.
Xu Q, Zhang X, Wu P, Wang M, Zhou Y, Feng Y. Multiple intracranial aneurysms followed left atrial myxoma: case report and literature review. J Thorac Dis. 2013;5:E227–31. https://doi.org/10.3978/j.issn.2072-1439.2013.11.27.
Ekmektzoglou KA, Samelis GF, Xanthos T. Heart and tumors: location, metastasis, clinical manifestations, diagnostic approaches and therapeutic considerations. J Cardiovasc Med (Hagerstown). 2008;9:769–77. https://doi.org/10.2459/JCM.0b013e3282f88e49.
Pinede L, Duhaut P, Loire R. Clinical presentation of left atrial cardiac myxoma A series of 112 consecutive cases. Medicine (Baltimore). 2001;80:159–72. https://doi.org/10.1097/00005792-200105000-00002.
Furuya K, Sasaki T, Yoshimoto Y, Okada Y, Fujimaki T, Kirino T. Histologically verified cerebral aneurysm formation secondary to embolism from cardiac myxoma. Case report J Neurosurg. 1995;83:170–3. https://doi.org/10.3171/jns.1995.83.1.0170.
Reynen K. Cardiac myxomas. N Engl J Med. 1995;333:1610–7. https://doi.org/10.1056/NEJM199512143332407.
Hwang BJ, Connelly MM, Lev MH. Distinctive MR imaging appearance of hemorrhagic cerebral aneurysms associated with atrial myxoma. AJR Am J Roentgenol. 2001;177:925–7. https://doi.org/10.2214/ajr.177.4.1770925.
Acknowledgements
No assistance taken from anybody for this work.
Funding
None.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval
Not required as per our institute protocol.
Informed consent
Informed consent was obtained from the patient for submission and publication of this report.
Statement of human and animal rights
The study has been performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors.
Conflict of interest
No conflicts of interest.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Kumar, N., Raja, J., Bansal, V. et al. A rare triad in left atrial myxoma. Indian J Thorac Cardiovasc Surg 39, 531–534 (2023). https://doi.org/10.1007/s12055-023-01540-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12055-023-01540-5