
Abstract
Solitary fibrous tumors of pleura are uncommon. Sometimes they pose challenge to differentiate from lung cancer. Here, we are briefly discussing about the literature review and management principles in relation to our experience. A total of three patients were presented in thoracic oncology unit of Rajiv Gandhi Cancer Institute in the last year. Correct diagnosis is the key as surgical resection is often curative and surgical resection is often possible despite huge sizes. Our aim is to highlight this uncommon entity and to gain some insight into its management.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Primary pleural tumors are rare and slowly growing. Mesotheliomas are the commonest primary tumor of pleura. They have diffuse involvement. Uncommon subset of localized pleural tumor is initially labeled as localized mesothelioma. They are distinct tumor, in relation to their origin. They originate from mesenchymal tissue of pleura, not from mesothelium. These tumors have nonspecific histopathologic appearance, specific IHC, and electron microscopic appearance. These are now called as solitary fibrous tumor of pleura (SFTP) [1–4]. Overall, they account for 5% of all pleural surface neoplasm and of them more than 80% are benign.
Our experience
We encountered four patients with diagnosis of SFTP during the last year; among them, one did not get treated at our institute. Here, we are describing clinical profile of three patients who were operated at our institute, with our experience in managing those (Table 1).
The first patient was a 56-year-old woman with no comorbidities presenting with complaints of dyspnea and chest pain of 3 months duration. She was evaluated with chest CT, which showed large (15 × 10 cm) well-marginated mass at the left side of the thoracic cavity, in relation to lingular lobe of the left lung. Trucut biopsy was done which showed solitary fibrous tumor. Her serum glucose level was within normal limits. She was taken for surgical resection after optimization. She required left posterolateral thoracotomy with en bloc resection of the mass with and wedge resection of lingular lobe of the left lung. She withstood the procedure well and intercostal chest drain (ICD) was removed on the third postoperative day. Histopathology (HPE) report showed solitary fibrous tumor of pleura (SFTP) grade II with all margin free (mitotic rare 4–5/10 hpf and Ki 67 index 8–10%). Case was discussed in multispecialty clinic (MSC) and decided to put on follow up with explained risk of high local recurrence possibility. She is under follow up and currently disease free about 1 year past surgery.
The second patient was a 31 year-old woman who presented with complaints of dyspnea and cough for the last 2 months. She was evaluated and detected to have a solid well-defined mass at the left upper lobe. Biopsy showed SFTP. She was optimized and taken for surgery. She underwent VATS (video assisted thoracoscopic surgery) resection of the mass (size, 6 cm × 4 cm) with en bloc resection of second rib (a segment of about 2 cm in continuity). Rib resection was done for easy access and not to rupture the tumor. Final HPE showed SFTP with all margins clear. Lesion was low grade. After MSC discussion, patient was put on follow up. She is now past the fourth month after surgery and currently disease free.
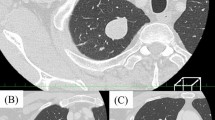
The third patient was also a woman, 59 years of age, who came to us with complaints of dyspnea and chest compression of 5 months duration. Her chest X-ray showed mediastinal widening with opacity at the left upper lung zone. Her chest CT scan showed a large 18 × 12 cm lobulated well-defined mass at the left side of chest cavity, in relation to the left upper lobe. The mass was causing mediastinal shift with compression of the left-sided pulmonary vessels and left main bronchus, with infiltration into the left upper lobe. Minimal pleural effusion was noted. There was no mediastinal lymph node enlargement. CT-guided biopsy showed spindle cell tumor. On IHC characterization, it was reported as SFTP, (Figs. 1 and 2). To assess resectability, we did a CT angiogram, which showed the mass compressing, but not infiltrating major vessels. (Fig. 3) Additionally, a feeding vascular pedicle arising from intercostal and internal mammary vessels were noted. The patient was taken for surgical resection after optimization. We anticipated difficult access and blood loss in view of the huge mass. We did posterolateral thoracotomy and noted a large 18 × 12 cm capsulated mass originating from parietal pleura and densely adherent to the left upper lobe, pericardium, and second rib, with mild pleural effusion (<200 ml). We resected the mass en bloc with the second rib and wedge resection of the left upper lobe. Tumor was hyper vascular. Procedure took 6 h to conclude. There was about 4.5 l of estimated blood loss with 6 units of packed red cell transfusion required. She was kept on elective ventilation for 12 h. She gradually recovered and ICDT was removed on postoperative day 5. Final HPE was SFTP low grade. Case was discussed in MSC and decision made to put on close watch as it was a low-grade lesion.

HPE slide showing haphazardously arranged spindle cells, with inspersed collagen bundles

Immunohistochemistry panel, see CD34+

A large well defines mass, with mediastinal shift, but not infiltrating into vessels (a–c) and follow up chest X-ray at 3 months showing well expanded lungs (d)
Brief review of the literature and discussion
SFTPs are rare entity and less than 800 cases have been reported as noted by De parrot et al. [4]. They commonly develop from pleura both parietal and visceral. Apart from this, it can develop from extrathoracic location including meninges, head and neck, breast, kidney, bladder, and spinal cord. They predominantly occur in the elderly with no sex predilection. No apparent genetic predilection was noticed [5]. They are slow growing and present as large masses. As they are extra pulmonary in location, symptoms usually develop when there is compression to vital structures or involvement of chest wall. Often, they present with cough, chest pain, and dyspnea. About 10–20% of patients might have hypertrophic pulmonary osteoarthropathy (Pierre-Marie–Bamberg syndrome). About 2–4% of these patients present with hypoglycemia particularly with malignant and extrathoracic tumors. This association is called as Doege-Potter syndrome (DPS). [6] General physical examination is usually non-contributory apart from occasional findings like clubbing and reduced air entry. Chest X-ray shows opacification at lung zones, as any solid lung mass, with occasionally pleural effusion [7].
CT scan is a defining and essential investigation. CT shows well-marginated solid mass with heterogeneous enhancement. Sometimes obvious pedunculation from visceral pleura may be seen. Sometimes when it develops from parietal pleura, it is called as inverted tumor. Well-defined large masses with no obvious infiltration and no mediastinal lymphadenopathy hints towards SFTP but no radiological findings are characteristic. Sometimes they show hyper intense and central necrosis, which make the clinical diagnosis even more difficult. Magnetic resonance imaging (MRI) does not provide additional diagnostic details. PET scan is unnecessary as these tumors are very rarely metastasize [8]. In all other scenarios, image-guided biopsy is needed. Our experience re-affirms the need for biopsy in large solid masses [9, 10].
Surgical resection with adequate margin is the main therapeutic modality. Traditionally, open surgical resection with lung parenchyma preservation, as much as possible has been a standard treatment. Video-assisted thoracoscopic surgical resection (VATS) can also be offered for smaller lesion with care not to rupture the tumor [11, 12]. Larger masses may pose surgical resection difficult. Sometimes en bloc resection including lung lobectomy, diaphragm, or rib resection may be needed. [13]. We needed some additional tissue in all three cases. One should be well prepared to manage excessive blood loss due to increased vascularity and ooze from lung surface and larger lung resection. Sometimes when more than 3–4 ribs need to sacrifice, one may need chest wall reconstruction. For larger and hypervascular masses, sometimes angioembolization can be done, if feeding vessels are identified.
Grossly, they are large, firm, well-encapsulated lobular, whorled mass with areas of occasional necrosis. On microscopic examination, they have elongated spindle cells arranged in haphazard or patternless manner with extracellular collagen bands. Area of necrosis, hemorrhage, myxomatous change, and vascular or stromal invasion with high mitotic rate/Ki 67 index suggests aggressive nature. [5, 14]. Panels of immunohistochemistry (IHC) markers are essential for diagnosis. They are of pleural origin, and showed CD 34 positivity with CK negative, as opposed to mesothelioma, which are positive for CK and negative for Vimentin/CD34 [4]. About 15–20% cases where CD34 is negative; STAT6 is another very sensitive marker of SFPT, which is a specific immunohistochemical marker. The diagnostic criteria and IHC characteristics of SFTP were suggested by England et al. in a review of 223 cases. [15].
De Parrot [4] and Robinson [16] described two broad subgroups of SFTP as benign and malignant based on gross appearance and microscopic appearance as described in Table 2.
High-grade lesions (malignant) have tendency of local recurrence, but adjuvant chemotherapy does not improve local control [7]. Postoperative radiotherapy may be added for incomplete surgical resection, if re-resection is not feasible. Adjuvant chemotherapy does not improve local control. The low-grade (benign) lesion rarely recurs but malignant (high grade) lesion has high rate of local recurrence. Most of the recurrences tend to occur within 24 months of the initial resection, but recurrence late up to 20 years has been reported. [7] So, these patients need long term follow up. In case of local recurrence, preferred therapeutic option is re-resection [4]. Neoadjuvant chemotherapy may be used for larger or borderline resectable lesions but sufficient data are lacking in literature [4, 9]. We discussed our patients for thoracic oncology; multispecialty clinic (MSC) as oncology puzzle and further plan was based on consensus decision.
Conclusion
Solitary fibrous tumor of pleura is a rare entity. Most of these are curable with surgery alone. Surgery may be challenging sometimes. High-grade or malignant lesions are having risk of local recurrence. No sufficient evidence exists regarding optimal adjuvant management of high-grade disease. Multispecialty clinic (MSC) discussion may be of value in decision-making. Present study should sensitize clinician regarding this uncommon yet important differential of lung masses.
References
Chan JKC. Solitary fibrous tumour—everywhere, and a diagnosis in vogue. Histopathology. 1997;31:568–76.
Klemperer P, Rabin CB. Primary neoplasm of the pleura: a report of five cases. Arch Pathol. 1931;11:385–412.
Stout AP, Murray MR. Localized pleural mesothelioma. Arch Pathol. 1942;34:951–64.
De Perrot M, Fischer S, Brundler MA, et al. Solitary fibrous tumors of the pleura. Ann Thorac Surg. 2002;74:285–93.
Shields TW 1994. Localized fibrous tumors of the pleura. In: Shields T W, ed. General Thoracic Surgery. 4th ed. Baltimore, Md: Williams & Wilkins;
Jang JG, Chung JH, Hong KS, et al. A case of solitary fibrous pleura tumor associated with severe hypoglycemia: Doege-Potter syndrome. Tuberc Respir Dis (Seoul). 2015;78:120–4.
Rosado-de-Christenson ML, Abbott GF, Mc Adams HP, et al. From the archives of the AFIP: localized fibrous tumors of the pleura. Radiographics. 2003;23:759–83.
Akman C, Cetinkaya S, Ulus S, et al. Pedunculated localized fibrous tumor of the pleura presenting as a moving chest mass. South Med J. 2005;98:486–8.
Mitchell JD. Solitary fibrous tumor of the pleura. Semin Thorac Car- diovasc Surg. 2003;15:305–9.
Robinson LA, Reilly RB. Localized pleural mesothelioma: the clinical spectrum. Chest. 1994;106:1611–5.
Sung SH, Chang JW, Kim J, et al. Solitary fibrous tumors of the pleura: surgical outcome and clinical course. Ann Thorac Surg. 2005;79:303–7.
Cardillo G, Facciolo F, Cavazzana AO, et al. Localized (solitary) fibrous tumors of the pleura: an analysis of 55 patients. Ann Thorac Surg. 2000;70:1808–12.
Okike N, Bernatz PE, Woolner LB. Localized mesothelioma of the pleura: benign and malignant variants. J Thorac Cardiovasc Surg. 1978;75:363–72.
Ordonez NG. Localized (solitary) fibrous tumor of the pleura. Adv Anat Pathol. 2000;7:327–40.
England DM, Hochholzer L, McCarthy MJ. Localized benign and malignant fibrous tumors of the pleura: a clinicopathologic review of 223 cases. Am J Surg Pathol. 1989;13:640–58.
Robinson A. Solitary fibrous tumor of the pleura. Cancer Control. 2006;13(4):264–9.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Financial funding statement
It is certified that the present study is not funded by any association/firm in any manner.
Conflict of interest
The authors declare that they have no conflict of interest.
Statement regarding research involving human participants and/or animals
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Rights and permissions
About this article

Cite this article
Ram, D., Sharma, A., Darlong, L.M. et al. Management of solitary fibrous tumor of the pleura: a rare differential of solid lung masses. Indian J Thorac Cardiovasc Surg 33, 29–33 (2017). https://doi.org/10.1007/s12055-016-0484-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12055-016-0484-8