
Abstract
Patients affected by pulmonary tuberculosis (PTB) manifest deficiencies in innate cellular immunity. The Tim-3/Galectin-9 axis is an important regulator of Th1 cell immunity, leading to Th1 cell apoptosis. Herein, this study aims to clarify the underlying roles of the Tim-3/Galectin-9 axis in T-cell immunity in PTB. Peripheral blood mononuclear cells (PBMCs) were extracted from subjects with and without PTB to examine the expression of CD4, CD8, CD25, and Tim-3 under the stimulation of Mycobacterium tuberculosis (MTB) and purified protein derivative (PPD). In addition, the expression of Tim-3 and Galectin-9 in PBMCs was determined. The Tim-3/Galectin-9 axis in the PBMCs was activated or blocked to detect the secreted levels of IFN-γ, TNF-α, IL-2, and IL-22. MTB stimulation increased the expression of CD4, CD8, CD25, Tim-3, and Galectin-9 in PBMCs. The blockade of Tim-3/Galectin-9 axis resulted in reduced secretion of IFN-γ, TNF-α, IL-2, and IL-22 from T-cells. Moreover, Tim-3+CD4+T, Tim-3+CD8+, and Tim-3+CD25+T cells exhibited a greater ability to inhibit the replication of MTB in macrophages. Taken conjointly, the blockade of Tim-3/Galectin-9 axis inhibits the secretion of inflammatory cytokines in T-cells to regulate the T-cell immunity in PTB.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Tuberculosis (TB), an infectious disease caused by Mycobacterium tuberculosis, is a huge threat to public health, with over 10.4 million new diagnosed cases as well as 1.9 million deaths in 2015 worldwide (Ortiz-Martinez 2017). According to the recent reports published on 19 March 2018 in the TB surveillance report by the European Centre for Disease Prevention and Control, the European Union and European Economic Area countries reported 58,994 TB cases in 2016 (Eurosurveillance Editorial Team 2018). Accounting for 25% of global TB incidence, China has the highest incidence of drug-resistant TB in the world (Huang et al. 2017). The causative agent of TB is Mycobacterium tuberculosis (MTB) (Isabel and Rogelio 2014). MTB exhibits possible pathogenesis of severe pneumonia and pulmonary scarring (Wu et al. 2011). MTB primarily affects the lung, contributing to the development of pulmonary tuberculosis (PTB) (Lai et al. 2014). Multiple risk factors for PTB have been identified such as diabetes mellitus, chronic kidney diseases, smoking, alcoholism, human immunodeficiency virus (HIV), chronic liver disease, and contact with TB-affected individuals (Gupta et al. 2011). Unfortunately, PTB recurrence is very common even after successful treatment from TB (Subbian et al. 2011). Intriguingly, recent data have highlighted that interventions through modulation of the host pathways might bring about effective therapy regimens to cure TB (Man et al. 2016). Moreover, T cell immunoglobulin-3 (Tim-3) has been indicated to potentially inhibit the growth and replication of intracellular bacteria by binding to its ligand Galectin-9, which is expressed by MTB-infected macrophages (Jayaraman et al. 2010).
Tim-3 was first discovered in 2002, and confirmed as a marker for the purpose of differentiating between CD8+ T cytotoxic type 1 cells and IFN-γ-producing CD4+ T helper type 1, and finally the S-type lectin, Galectin-9, was identified as the ligand of Tim-3 (Sakuishi et al. 2011). In addition, Tim-3 is known as a negative-regulatory molecule which plays a critical role in preventing tissue inflammation (Jayaraman et al. 2010). Furthermore, Tim-3 serves as an immunoinhibitory molecule by functioning in anti-tumor or antiviral immune evasion or immune tolerance and acts as a pro- and anti-inflammatory regulator of innate immune responses (Zhang et al. 2012). Meanwhile, the ligand of Tim-3, Galectin-9 is expressed in various kinds of cells and possesses the ability to regulate cell adhesion, differentiation, aggregation, and cell death (Li et al. 2012). Tim-3 has been demonstrated to interact with Galectin-9 to bring about the death of the Th1 cells and promote peripheral tolerance (Nebbia et al. 2012). Another study has shown that Tim-3, whose expression was found on effector CD4+ and CD8+ T-cells, could bind to Galectin-9, further leading to cell apoptosis as well as functional property changes; the interaction was illustrated to control tissue damage degree in some inflammatory diseases (Reddy et al. 2011). Additionally, Tim-3 has evolved so much to inhibit the growth of intracellular pathogens via its involved ligand Galectin-9, which in turn inhibits the expansion of effector Th1 cells so as to prevent further tissue inflammation (Jayaraman et al. 2010). More notably, one study demonstrated that Tim-3 could regulate Galectin-9 to activate macrophages and suppress MTB (Sada-Ovalle et al. 2015). It has also been suggested that the continued interaction between Tim-3 and Galectin-9 results in a bidirectional regulatory circuit that activates innate immune cells to clear intracellular pathogens, which in turn further up-regulates Tim-3 ligand and Galectin-9 and promotes termination of all Th1 responses (Jayaraman et al. 2010). Therefore, the current study proposed a hypothesis that the Tim-3/Galectin-9 axis might regulate the immunity of T-cells in PTB patients.
2 Materials and methods
2.1 Ethical statement
The current study was approved by the Ethics Committee of the First Hospital of Jilin University (ethical number: 201702005). Signed informed consents were obtained from all participants prior to the study.
2.2 Study subject
Healthy controls as well as patients harboring active PTB in both outpatient and inpatient departments were enrolled in the current study. The study populace included 50 active PTB patients, comprising of 30 males and 20 females aged 27–45 years, with a calculated median age of 35.5 ± 2.5 years. A diagnosis of active PTB was made in accordance with the diagnostic criteria for active PTB issued by the Chinese Ministry of Health in 2008. The following inclusion criteria protocols were enforced: (a) patients showed positive MTB in their sputum and pleural effusion, or displayed characteristic lesions of tuberculosis upon biopsy; (b) patients’ pulmonary parenchyma as well as bronchus showed characteristics of TB lesions; (c) patients had clinical manifestations of significant tuberculosis poisoning symptoms or other inspections were consistent with the characteristics of tuberculosis; (d) fast absorption of lesions along with pleural effusion after completing anti-tuberculosis treatment. Patients were excluded from the study if they sustained concurrent diseases, such as chronic pneumonia, lung cancer, and pneumoconiosis; or if they presented with any other concurrent infectious diseases, diabetes, hypertension, chronic inflammation, or autoimmune diseases. In addition, 40 latent patients with tuberculosis (LPTB) were also enrolled, consisting of 25 males and 15 females aged between 27 and 45 years, with a calculated median age of 36.2 ± 3.2 years. Patients from the LPTB group tested strongly positive for the tuberculin test, but showed no bacteriological and clinical signs of active PTB manifestation. Lastly, a total of 20 healthy controls (HC) including 13 males and 7 females were also enrolled, aged between 31 and 38 years, and with a median age of 34.5 ± 1.5 years. Participants were included in the HC group if they tested negative for the tuberculin test (PPD test) and serum anti-tuberculosis antibody, exhibited normal chest x-ray results and were not in contact with people with tuberculosis recently. There were no significant differences in regard to age and gender among the groups (table 1).
2.3 Isolation, culture, PPD treatment of peripheral blood mononuclear cells (PBMCs)
PBMCs were isolated using a lymphocyte separation medium (Gibco Company, Grand Island, NY, USA) according to the standard Ficoll density gradient centrifugation. After being fully washed, the PBMCs were cultured with Roswell Park Memorial Institute (RPMI) 1640 complete medium (Invitrogen Inc., Carlsbad, CA, USA) containing 10% fetal bovine serum (FBS) with the cell density adjusted to 5 × 105 cells/mL. The PBMCs were then inoculated in a 96-well plate (200 μL/well), incubated at 37°C with 5% CO2 in air for 24 h, and stimulated with the addition of 8 μL PPD (0.5 mg/mL) for 6 h.
2.4 Flow cytometry
Cells were detached with 0.25% trypsin, resuspended with 200 μL of PBS, and labeled with the addition of phycoerythrin (PE)-Cy7-labeled anti-human CD3 antibody, fluorescein isothiocyanate-labeled anti-human CD4 antibody, PE-Cy5-labeled anti-human CD8 antibody, PE-labeled anti-human CD25, or APC-labeled anti-human Tim-3 antibody (eBioscience, San Diego, CA, USA) and were all dyed at 4°C for 1 h in dark conditions. A Fluorescence Activated Cell Sorter (FACS) Calibur flow cytometry (Becton Dickinson, Franklin Lakes, NJ, USA) was employed to detect the expressions of the cell surface-related proteins and the CXP software (Beckman Coulter, Inc., Fullerton, CA, USA) was applied for thorough analysis of the obtained results. The protein expression rate was presented as the percentage of the positively expressed proteins, while protein expression intensity was expressed as median fluorescence intensity (MFI).
2.5 Plasmid construction and cell transfection
Total RNA content was extracted from the PBMCs in the HC group using the Trizol reagent (Invitrogen Inc., Carlsbad, CA, USA), and later reverse transcribed into cDNA in accordance with instructions provided by the M-MLV reverse transcription kit (Invitrogen Inc., Carlsbad, CA, USA). The artificially synthesized cDNA was regarded as a template, and the primers carrying XhoI and HindII restriction sites were designed (table 2). Full-length coding sequence of Tim-3 gene (Gene ID. NM_032782.4) was amplified by polymerase chain reaction (PCR) and then inserted into the pcDNA3.1 (+)/Myc HisB expression plasmid to construct the over-expression plasmid of Tim-3 into pcDNA3.1 (+)/Myc HisB-Tim-3. The Tim-3 siRNA or control siRNA was purchased from the Santa Cruz Company (CA, USA). Subsequently, PBMCs from 10 active PTB patients were seeded into 6 wells of a 6-well plate for overnight culture. When cell confluence reached 60 - 70%, the PBMCs were assigned into blank control (cells without any treatment), empty vector (cells transfected with 4 μg pcDNA3.1(+)/Myc HisB empty vector), Tim-3 over-expression (cells transfected with 4 μg pcDNA3.1(+)/Myc HisB-Tim-3), control siRNA (cells transfected with 50 nM control siRNA), Tim-3 siRNA (cells transfected with 50 nM Tim-3 siRNA), Tim-3 over-expression + Galectin-9 inhibitor (cells transfected with 4 μg pcDNA3.1(+)/Myc HisB-Tim-3 and 30 mM lactose [Promega Corp., Madison, Wisconsin, USA]), or Tim-3 siRNA + rhGalectin-9 (cells transfected with 50 nM Tim-3 siRNA and 20 μg/mL of recombinant human Galectin-9 protein [Galpharma Company, Takamatsu, Japan]) groups. After 48 h of transfection, 8 μL MTB special antibodies (0.5 mg/mL antigen PPD) were added to stimulate the PBMCs for another 6 h.
2.6 Reverse transcription quantitative polymerase chain reaction (RT-qPCR)
Total RNA content was extracted from the cells in each group using the Trizol reagent (Invitrogen Inc., Carlsbad, CA, USA), and then reverse transcribed to cDNA in accordance with instructions provided by the Moloney-Murine Leukemia Virus (M-MLV) reverse transcription kit (Invitrogen Inc., Carlsbad, CA, USA). Then, the SYBR Green Mix fluorescent dye method (Roche Pharma Switzerland Ltd.) was adopted to perform RT-qPCR. The primers (table 3) were synthetized by Shanghai Sangon Biological Engineering Technology & Services Co., Ltd. (Shanghai, China). β-actin was regarded as the internal reference, and the 2−ΔΔCt method was adopted to calculate the relative gene expressions of Tim-3 and Galectin-9 in each group.
2.7 Western blot assay
Cells were collected from each group after detachment with trypsin and lysed with an intense Radio-Immunoprecipitation assay (RIPA) lysate (Wuhan Boster Biological Technology Co., Ltd., Wuhan, China) containing a cocktail of protease inhibitors. Subsequently, a bicinchoninic acid protein method (Wuhan Boster Biological Technology Co., Ltd., Wuhan, China) was employed to quantify the protein concentration. Following protein separation with sodium dodecyl sulfate-polyacrylamide gel electrophoresis, the proteins were then transferred onto a polyvinylidene fluoride membrane. After that, the membrane was blocked with 5% bovine serum albumin for 2 h at room temperature and incubated at 4°C overnight with the primary antibody rabbit anti-human Tim-3 (ab185703, dilution ratio of 1:1000, Abcam Inc., Cambridge, UK), Galectin-9 (ab69630, dilution ratio of 1:500, Abcam Inc., Cambridge, UK) as well as β-actin (ab8227, dilution ratio of 1:1000, Abcam Inc., Cambridge, UK). Next, the membrane was incubated with a horseradish Peroxidase-labeled secondary antibody goat anti-rabbit (BA1055, dilution ratio of 1:3000, Wuhan Boster Biological Technology Co., Ltd., Wuhan, China) at room temperature for 1 h, and visualized using enhanced chemiluminescence (EMD Millipore Corporation, Billerica, MA, USA). The grey value analysis of target bands was calculated using the Image J software with β-actin serving as the internal reference (Chai et al. 2018).
2.8 Enzyme-linked immunosorbent assay (ELISA)
Cell supernatant from each group was centrifuged at 257g for 10 min to remove the impurities and cell debris. Subsequently, the expression of IFN-γ, TNF-α, IL-2, and IL-22 in the HC and PTB groups was detected according to the instructions of ELISA kits (Shanghai Yuan Ye Biotechnology Co., Ltd., Shanghai, China).
2.9 Magnetic activated cell sorting
Cells from each group were dispersed into a mononuclear cell suspension form at the number of cells reaching 1 × 108. CD4+, CD8+, and CD25+ T cells were all separately classified in accordance with instructions provided by the magnetic bead separation kit (Miltenyi Biotec, Gladbach, Germany) using an immunomagnetic bead separation method. Next, the PE-labeled anti-human Tim-3 flow antibody (Becton Dickinson, Franklin Lakes, NJ, USA) was added to label the cells. Lastly, a PE-labeled cell sorting kit (STEMCELL Technologies Inc., Canada) was employed to separate Tim-3+CD4+, Tim-3+CD8+, and Tim-3+CD25+ T cells and the purity was detected to be over 95% by flow cytometer.
2.10 Establishment of model of MTB-infected human macrophages
Human U973 macrophages (Shanghai Cell Bank of Chinese Academy of Sciences, Shanghai, China) were incubated in the RPMI 1640 medium containing 10% FBS at 37°C and 5% CO2 in air for 48 h. MTB infection was performed in accordance with the classic Roche culture method (Guthrie et al. 2018). During infection, MTB (Mavium, Shanghai Municipal Center for Disease Control and Prevention) and cells were mixed at a ratio of 20:1, followed by 4-h mild shaking at 37°C. The auramine O staining method demonstrated that over 90% of the cells were infected by MTB, and there were 1-5 bacteria in each cell. After an additional 4-h infection, the cells were washed with a medium three times to remove the bacteria which were not swallowed (Abreu et al. 2018).
2.11 Detection of mycobacterium growth condition in human macrophages
The density of macrophages infected by MTB was adjusted to 5 × 105 cells/mL, and the macrophages were cultured in the RPMI-1640 complete medium, which was then added to a 96-well circle plate with 200 μL macrophages in each well. Next, the macrophages were cultured after the addition of Tim-3-CD4+, Tim-3+CD4+, Tim-3+CD8+, Tim-3-CD8+, Tim-3+CD25+, and Tim-3-CD25+ T cells (5 × 105 cell/well) separately at 37°C and 5% CO2 in air for 24 h. After that, the cell lysis buffer (0.067% serine dehydratase [SDS] in Middlebrook7H9 medium) was added to the cells for further incubation. PBS + 20% BSA buffer was added to neutralize the SDS medium, and the Middlebrook7H9 medium was used so as to dilute the lysate 10-fold. Finally, the diluted lysates as well as the upper layer solution were added onto the agar of Middlebrook7H10 separately for further culture until the number of the colony of bacteria was adequate enough following its growth.
2.12 Statistical analysis
All data were analyzed using the SPSS 21.0 software (IBM Corp. Armonk, NY, USA). Measurement data were normally distributed and presented as mean±standard deviation. One-way analysis of variance (ANOVA) was conducted to compare the data among multiple groups, followed by Tukey post-hoc test. A value of p<0.05 was regarded statistically significant.
3 Results
3.1 Up-regulated CD4, CD8, CD25 and Tim-3 in PBMCs of patients infected with MTB
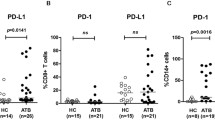
PBMCs were extracted from peripheral blood samples of HC, LPTB patients, and active PTB patients. The specific antigen of MTB was stained with or without PPD stimulation. In addition, the expression of CD4, CD8, CD25, and Tim-3 in PBMCs in each group was analyzed using a multi-color flow cytometer. The results (figure 1 and supplementary figure 1) indicated that the LPTB group as well as the active PTB group exhibited significantly increased expression ratio and expression intensity of CD4, CD8, CD25, and Tim-3 compared to the HC group (p < 0.01). Both the expression ratio and expression intensity of CD4, CD8, CD25, and Tim-3 in the active PTB group were significantly higher than those in the LPTB group (p<0.01). After PPD stimulation for 6 h, significantly increased CD4, CD8, CD25, and Tim-3 expression ratio and expression intensity were noted relative to the group devoid of any PPD stimulation (p<0.01). These results indicated that both the expression ratio and expression intensity of CD4, CD8, CD25, and Tim-3 were up-regulated in the presence of an MTB infection; additionally, the influence of MTB elevated the number of CD4+, CD8+, CD25+, and Tim-3+ lymphocytes in PBMCs.

Elevated expressions of CD4, CD8, CD25 and Tim-3 in PBMCs of MTB-infected patients. (A) flow cytometric images of CD4, CD8, CD25 and Tim-3 expression peak in PBMCs in each group; (B) expression ratio of CD4, CD8, CD25 and Tim-3 of PBMCs in each group; (C) expression intensity of CD4, CD8, CD25 and Tim-3 of PBMCs in each group; *, p < 0.05 compared with the group without PPD stimulation; #, p < 0.05 compared with the HC group with PPD stimulation for 6 h; &, p < 0.05 compared with the LPTB group with PPD stimulation for 6 h; measurement data were expressed as mean ± standard deviation and analyzed by one-way ANOVA, followed by Tukey post-hoc test. In the HC group, n = 20; in the LPTB group, n = 40, and in the active PTB group, n = 50.
3.2 Elevated Tim-3 and Galectin-9 expression in LPTB and active PTB patients
The mRNA and protein expression of Tim-3 and Galectin-9 were detected in HC, active PTB patients, and LPTB patients using RT-qPCR and Western blot assay (figure 2). RT-qPCR results demonstrated that the mRNA expressions of Tim-3 and Galectin-9 in the LPTB and active PTB groups were significantly elevated compared to the HC group; the results of Western blot assay revealed that the protein expressions of Tim-3 and Galectin-9 in the LPTB and active PTB groups were also notably increased relative to the HC group.

Raised expression of Tim-3 and Galectin-9 in LPTB patients and active PTB patients. (A) mRNA expression of Tim-3 and Galectin-9 in the HC, LPTB and active PTB groups as detected by RT-qPCR; (B) protein expression of Tim-3 and Galectin-9 in the HC, LPTB and active PTB groups as determined by Western blot assay; (C) quantitative analysis of Tim-3 and Galectin-9 protein expression in each group; *, p < 0.05 compared with the HC group; the measurement data were expressed as mean ± standard deviation and analyzed by one-way ANOVA, followed by Tukey post-hoc test. In the HC group, n = 20; in the LPTB group, n = 40, and in the active PTB group, n = 50.
3.3 Elevated Tim-3 and Galectin-9 expression in MTB-infected PBMCs
Additionally, the mRNA expression of Tim-3 and Galectin-9 was analyzed in PBMCs after transfection with different vectors and plasmids by RT-qPCR. No differences were noted in the expression of Tim-3 between the empty vector group and blank control group (p > 0.05), while Tim-3 expression was obviously increased in Tim-3 over-expression group (p < 0.05). This particular finding indicated that the overexpression plasmid (pcDNA3.1 (+)/Myc HisB-Tim-3) enabled efficient production of Tim-3 overexpression. Similarly, there were no significant differences detected in the Tim-3 gene expression between the control siRNA group and the blank control group (p > 0.05). Meanwhile, reduced Tim-3 gene expression was noted in the Tim-3 siRNA group compared with the blank control group (p < 0.05), indicating that Tim-3 siRNA effectively silenced the Tim-3 gene in PBMCs. Whereas, Tim-3 expression in the Tim-3 over-expression + Galectin-9 inhibitor group was not significantly different to that in the Tim-3 over-expression group (p > 0.05). No differences were also noted in Tim-3 expression among the Tim-3 siRNA + rhGalectin-9 group and the Tim-3 siRNA group (p > 0.05), suggesting that Tim-3 expression was not affected by the Galectin-9 expression. As for the Galectin-9 expression, the empty vector group exhibited no changes (p > 0.05), while the expression in the Tim-3 overexpression group was up-regulated compared to the blank control group (p < 0.05) (figure 3). At this juncture, we inferred that Tim-3/Galectin-9 axis-related genes might be over-expressed in PBMCs infected with MTB.

Elevated mRNA expression of Tim-3 and Galectin-9 in MTB-infected PBMCs. (A) relative expression of Tim-3 as detected by RT-qPCR in each group; (B) relative expression of Galectin-9 as detected by RT-qPCR in each group; *, p < 0.05 compared with the empty vector group; #, p < 0.05, compared with the control siRNA group; &, p < 0.05, compared with the Tim-3 over-expression group; ¥, p < 0.05, compared with the Tim-3 siRNA group; measurement data were expressed as mean ± standard deviation and analyzed by one-way ANOVA, followed by Tukey post-hoc test; each experiment was repeated three times, with cells from 3 independent donors.
Following detection of the mRNA expressions of Tim-3 and Galectin-9, Western blot assay was adopted to detect the protein expression of Tim-3 and Galectin-9 in different transfection groups, with the results presented in figure 4. In comparison with the blank control group, the protein expression of Tim-3 in the empty vector group and the control siRNA group showed no significant differences (p > 0.05). Tim-3 protein expression was significantly increased in the Tim-3 over-expression group (p < 0.01), while being markedly reduced in the Tim-3 siRNA group compared to the blank control group (p < 0.01). Besides, the Tim-3 overexpression+ Galectin inhibitor group exhibited significantly reduced Tim-3 protein expression relative to the Tim-3 over-expression group (p < 0.05), whereas increased Tim-3 protein expression was detected in the Tim-3 siRNA + rhGalectin-9 group in comparison with the Tim-3 siRNA group (p < 0.05). Furthermore, in comparison with the blank control group, the protein expression of Galectin-9 in the empty vector group as well as the control siRNA group showed no significant differences (p > 0.05), while increased Galectin-9 protein expression was noted in the Tim-3 overexpression group (p < 0.01). Moreover, reduced Galectin-9 protein expression was observed in the Tim-3 overexpression group relative to the blank control group (p < 0.05). Also, the Tim-3 over-expression + Galectin-9 inhibitor group demonstrated markedly decreased Galectin-9 protein expression compared to the Tim-3 overexpression group (p < 0.05). Meanwhile, up-regulated Galectin-9 protein levels were noted in the Tim-3 siRNA + rhGalectin-9 group compared to the Tim-3 siRNA group (p < 0.05). The aforementioned results revealed that Tim-3/Galectin-9 axis-related genes were elevated in PBMCs infected with MTB.

Increased protein expression of Tim-3 and Galectin-9 in MTB-infected PBMCs. (A) protein expression of Tim-3 and Galectin-9 as detected by Western blot assay in each group; (B) semi-quantitative results of protein expression of Tim-3 in each group; (C) semi-quantitative results of protein expression of Galectin-9 in each group; *, p < 0.05 compared with the empty vector group; #, p < 0.05, compared with the control siRNA group; &, p < 0.05, compared with the Tim-3 over-expression group; @, p < 0.05, compared with the Tim-3 siRNA group; measurement data were expressed as mean ± standard deviation and analyzed by one-way ANOVA, followed by Tukey post hoc-test; each experiment was repeated three times, with cells from 3 independent donors.
3.4 Blockade of the Tim-3/Galectin-9 axis inhibits the secretion of IFN-γ, TNF-α, IL-2 and IL-2 cytokines from T-cells
Furthermore, the expression of IFN-γ, TNF-α, IL-2, and IL-22 cytokines was detected in different transfection groups using ELISA. The results demonstrated that, when compared with the blank control group, the expressions of IFN-γ, TNF-α, IL-2, and IL-22 cytokines in the empty vector and the control siRNA group displayed no significant differences (p > 0.05). The Tim-3 overexpression group exhibited significantly increased expressions of IFN-γ, TNF-α, IL-2, and IL-22, which were all significantly reduced in the Tim-3 siRNA group compared to the blank control group (p < 0.05). It was also notable that the Tim-3/Galectin-9 axis was blocked by a combination of lactose and Galectin-9, thereby eliminating the up-regulatory effect of Tim-3 overexpression on the expression levels of IFN-γ, TNF-α, IL-2, and IL-22 (p < 0.05). Moreover, the use of a human recombinant Galectin-9 protein could be applied to eliminate the inhibitory effect that Tim-3 gene silencing exerts on the expressions of IFN-γ, TNF-α, IL-2, and IL-22 (p < 0.05) (figure 5). Based on these findings, it was suggested that dysregulation of the Tim-3/Galectin-9 axis could inhibit the secretion of inflammatory cytokines (IFN-γ, TNF-α, IL-2, and IL-22) from T-cells.

Diminished levels of inflammatory factors IFN-γ, TNF-α, IL-2, and IL-22 by inhibiting Tim-3 and Galectin-9 in MTB-infected PBMCs. *, p < 0.05 compared with the empty vector group; #, p < 0.05, compared with the control siRNA group; &, p < 0.05, compared with the Tim-3 overexpression group; @, p < 0.05, compared with the Tim-3 siRNA group; measurement data were expressed as mean ± standard deviation and analyzed by one-way ANOVA, followed by Tukey post-hoc test; each experiment was repeated three times, with cells from 3 independent donors.
3.5 Tim-3+CD4+T, Tim-3+CD8+ and Tim-3+CD25+T cells inhibit MTB replication ability
Finally, the MTB replication ability following MTB infection with macrophages is displayed in figure 6. Tim-3+CD4+, Tim-3+CD8+, and Tim-3+CD25+ T-cells were all cultured with autologous macrophages infected with MTB, and the T-lymphocyte subsets including Tim-3-CD4+, Tim-3-CD8+, and Tim-3-CD25+ were all regarded as part of the control group. Subsequently, the replication capacity of MTB of those T-lymphocyte subsets was observed, and it was found that the colony-forming unit did not differ greatly in each group at 0 h. However, at the 24 h and 48 h time intervals, when compared with Tim-3-CD4+, Tim-3-CD8+, and Tim-3-CD25+, the Tim-3+CD4+, Tim-3+CD8+, and Tim-3+CD25+ T cells all inhibited the growth of MTB in the MTB-infected macrophages (p < 0.05).

Inhibited MTB replication ability in MTB-infected macrophages in Tim-3+ CD4+, Tim-3+ CD8+ and Tim-3+ CD25+ cells. At the 24 h and 48 h time intervals, compared with Tim-3-CD4+, Tim-3-CD8+, and Tim-3-CD25+ T cells, the Tim-3+ CD4+, Tim-3+ CD8+, Tim-3+ CD25+ T cells significantly inhibited the growth of MTB in macrophages. *, p < 0.05 compared with the Tim-3-CD4+; #, p < 0.05 compared with the Tim-3-CD8+; &, p < 0.05 compared with the Tim-3-CD25+; measurement data were expressed as mean ± standard deviation and analyzed by one-way ANOVA, followed by Tukey post-hoc test; each experiment was repeated three times, with cells from 3 independent donors.
4 Discussion
TB is often regarded as the most challenging disease for doctors, accounting for high morbidity and mortality rates across the world (Abhimanyu et al. 2012). Moreover, the diagnosis of PTB remains to be an uphill battle due to varied, unusual presentations observed in different individuals (Park et al. 2010). Interestingly, recent evidence has indicated that the interaction between Tim-3 and Galectin-9 could potentially help to kill MTB (Sada-Ovalle et al. 2015). Thereby, the current study set out to explore the regulatory role Tim-3/Galectin-9 axis in the T-cell immunity of PTB, thereby providing a promising target for PTB therapy, and the findings suggested that the blockade of Tim-3/Galectin-9 axis enhanced T-cell immunity in PTB patients.
Initially, we uncovered that MTB infection increased the expression and number of CD4, CD8, CD25, and Tim-3 in the PBMCs of LPTB patients and active PTB patients relative to healthy controls. It is notable that different cytokines are known to function in the pathogenesis of PTB as well as MTB frequencies specific cells including CD4+ and CD8+ T cells (Nemeth et al. 2011). Further, a previous study conducted by Qiu et al. based on TB patients revealed that the number of CD4+ and CD8+ T cells was increased and T-cell immune responses in TB patients was regulated by Tim-3 (Qiu et al. 2012). Our study differs from the previous study in several aspects. Firstly, we selected active PTB patients, latent PTB patients, and healthy controls in the current study. Secondly, we detected the differential expression of Tim-3 and Galectin-9 and investigated the effects of Tim-3 on galectin-9 as well as the regulatory effects of over-expressed or depleted Tim-3 and Galectin-9 on the inflammatory response in PTB patients. Thirdly, we reported for the first time that CD25+ T cells, apart from CD4+ and CD8+ T cells, could also potentially inhibit PTB replication. All these aspects make our manuscript novel.
Our most significant finding was that the blockade of Tim-3/Galectin-9 axis could notably hinder the secretion of IFN-γ, TNF-α, IL-2, and IL-22 cytokines from T cells, thereby activating the immune function properties of the T-cell in PTB patients. Tim-3 is primarily expressed in Th1 cells, while a former study even vindicated its inhibitory role in immune reactions (Mariat et al. 2005). Moreover, we discovered that inactivation of the Tim-3/Galectin-9 axis could drastically reduce the immunosuppressive effect on Th1 cells and increase the levels of inflammatory factors such as IFN-γ, TNF-α, IL-2, and IL-22, thus augmenting the body’s resistance against TB. Similarly, Kuchroo et al. demonstrated that Tim-3 and Galectin-9 can interact to inhibit Th1 production by suppressing the expression of IFN-γ and IL-2 (Kuchroo et al. 2006). The activation of the Tim-3/Galectin-9 axis can regulate the dynamic balance of immune cells and their inflammatory reaction, as well as inhibit CD4+ and CD8+ cells, during which the inhibiting signal was produced to induce the apoptosis of Th1 cells and inhibit immune Th1 (Wang et al. 2008). The Tim-3/Galectin-9 pathway is known to regulate the inflammatory reaction of Th1 cells in two ways. One such way of regulation is that Th1 cells are killed by the Tim-3/Galectin-9 pathway: activating Tim-3 and Galectin-9 can activate caspase-1 to result in inflammatory apoptosis of caspase-1. The other mode was that Tim-3 and Galectin-9 regulate the death of T cells by inhibiting the production of CD11b+Ly-6G+ cells (Dardalhon et al. 2010). By inactivating the Tim-3/Galectin-9 pathway, the expression of Th1 cells was down-regulated, and the inhibiting activation of Th cells was significantly repressed (Mariat et al. 2005). However, evidence also demonstrated that in the early stages of infection, Treg cells were not induced to proliferate, and only wild-type MTB could induce Treg cells to proliferate, while Ag85B-deleted MTV could not effectively induce Treg cells to proliferate (Shafiani et al. 2010, Urdahl et al. 2011). Therefore, further studies will be conducted in the future with the aim to investigate whether Tregs affects the results obtained in our study.
Another critical discovery in our study was that Tim-3+CD4+T, Tim-3+CD8+, and Tim-3+CD25+ T cells were all capable of suppressing mycobacterial replication more powerfully than the collection of Tim-3-CD4+T, Tim-3-CD8+ T, and Tim-3-CD25+ T. Another study highlighted that CD25+ T lymphocytes isolated from the blood and pleural fluid of TB patients could repress the MTB-specific IFN-γ and IL-10 production in overall immunity, thus implicating CD25+ T lymphocytes in the pathogenesis of human TB (Chen et al. 2007). Consistently, it has also been indicated that Tim-3 was typically expressed on Th1 cells, which in turn produces cytokines such as IFN-γ, TNF-α, and IL-2 (Monney et al. 2002). IFN-γ is regarded a necessary factor in controlling the progression of MTB (Green et al. 2013). A prior study illustrated that blockade of the Tim-3 pathway could restore IFN-γ secretion as well as accelerate NK cells to control MTB in monocyte-derived macrophages (Wang et al. 2015). Meanwhile, Liu et al. demonstrated that the Tim-3/Galectin-9 axis could mediate T cell senescence, and blocking this pathway results in increased functionality of tumor-infiltrating Tim-3+ T cells in Hepatitis B virus-associated hepatocellular carcinoma (Li et al. 2012). Another observation was that the Tim-3/Galectin-9 axis compounding with 5-arylalkynyl substituents could exhibit potential anti-tubercular ability to suppress the growth of mycobacterium bovis as well as MTB (Srivastav et al. 2010). Moreover, through participation of the IL-1R, autocrine IL-1β signaling was a vital mechanism of Tim-3/Galectin-9 interaction induced antimicrobial activity in its infected macrophages (Jayaraman et al. 2010).
5 Conclusion
In conclusion, we found that inhibition of the Tim-3/Galectin-9 axis could regulate T-cell immunity in PTB patients by suppressing the secretion of inflammatory cytokines from T-cells, which provides a theoretical basis for deeper understanding of the specific mechanism by which the Tim-3/Galectin-9 axis affects immunity of T-cells.
References
Abhimanyu BM, Jha P and Indian Genome Variation C 2012 Footprints of genetic susceptibility to pulmonary tuberculosis: cytokine gene variants in north Indians. Indian J. Med. Res. 135 763–770
Abreu R, Essler L, Loy A, Quinn F and Giri P 2018 Heparin inhibits intracellular Mycobacterium tuberculosis bacterial replication by reducing iron levels in human macrophages. Sci. Rep. 8 7296
Chai D, Zhang L, Xi S, Cheng Y, Jiang H and Hu R 2018 Nrf2 Activation induced by Sirt1 ameliorates acute lung injury after intestinal ischemia/reperfusion through NOX4-mediated gene regulation. Cell Physiol. Biochem. 46 781–792
Chen X, Zhou B, Li M, Deng Q, Wu X, Le X, Wu C, Larmonier N, Zhang W, Zhang H, Wang H and Katsanis E 2007 CD4(+)CD25(+)FoxP3(+) regulatory T cells suppress Mycobacterium tuberculosis immunity in patients with active disease. Clin. Immunol. 123 50–59
Dardalhon V, Anderson AC, Karman J, Apetoh L, Chandwaskar R, Lee DH, Cornejo M, Nishi N, Yamauchi A, Quintana FJ, Sobel RA, Hirashima M and Kuchroo VK 2010 Tim-3/galectin-9 pathway: regulation of Th1 immunity through promotion of CD11b+Ly-6G+ myeloid cells. J. Immunol. 185 1383–1392
Eurosurveillance Editorial Team 2018 Note from the editors: World Tuberculosis Day 2018 and Special issue-Screening and prevention of infectious diseases in newly arrived migrants in Europe. Euro Surveill 23 180322-1 https://doi.org/10.2807/1560-7917.ES.2018.23.12.180322-1
Green AM, Difazio R and Flynn JL 2013 IFN-gamma from CD4 T cells is essential for host survival and enhances CD8 T cell function during Mycobacterium tuberculosis infection. J. Immunol. 190 270–277
Gupta S, Shenoy VP, Mukhopadhyay C, Bairy I and Muralidharan S 2011 Role of risk factors and socio-economic status in pulmonary tuberculosis: a search for the root cause in patients in a tertiary care hospital, South India. Trop. Med. Int. Health 16 74–78
Guthrie JL, Delli Pizzi A, Roth D, Kong C, Jorgensen D, Rodrigues M, Tang P, Cook VJ, Johnston J and Gardy JL 2018 Genotyping and Whole-Genome Sequencing to Identify Tuberculosis Transmission to Pediatric Patients in British Columbia, Canada, 2005–2014. J. Infect. Dis. 218 1155–1163
Huang Y, Wu Q, Xu S, Zhong J, Chen S, Xu J, Zhu L, He H and Wang X 2017 Laboratory-based surveillance of extensively drug-resistant tuberculosis in eastern China. Microb. Drug Resist. 23 236–240
Isabel BE and Rogelio HP 2014 Pathogenesis and immune response in tuberculous meningitis. Malays. J. Med. Sci. 21 4–10
Jayaraman P, Sada-Ovalle I, Beladi S, Anderson AC, Dardalhon V, Hotta C, Kuchroo VK and Behar SM 2010 Tim3 binding to galectin-9 stimulates antimicrobial immunity. J. Exp. Med. 207 2343–2354
Kuchroo VK, Meyers JH, Umetsu DT and DeKruyff RH 2006 TIM family of genes in immunity and tolerance. Adv. Immunol. 91 227–249
Lai SW, Wang IK, Lin CL, Chen HJ and Liao KF 2014 Splenectomy correlates with increased risk of pulmonary tuberculosis: a case-control study in Taiwan. Clin. Microbiol. Infect. 20 764–767
Li H, Wu K, Tao K, Chen L, Zheng Q, Lu X, Liu J, Shi L, Liu C, Wang G and Zou W 2012 Tim-3/galectin-9 signaling pathway mediates T-cell dysfunction and predicts poor prognosis in patients with hepatitis B virus-associated hepatocellular carcinoma. Hepatology 56 1342–1351
Man DK, Chow MY, Casettari L, Gonzalez-Juarrero M and Lam JK 2016 Potential and development of inhaled RNAi therapeutics for the treatment of pulmonary tuberculosis. Adv. Drug Deliv. Rev. 102 21–32
Mariat C, Sanchez-Fueyo A, Alexopoulos SP, Kenny J, Strom TB and Zheng XX 2005 Regulation of T cell dependent immune responses by TIM family members. Philos. Trans. R. Soc. Lond. B Biol. Sci. 360 1681–1685
Monney L, Sabatos CA, Gaglia JL, Ryu A, Waldner H, Chernova T, Manning S, Greenfield EA, Coyle AJ, Sobel RA, Freeman GJ and Kuchroo VK 2002 Th1-specific cell surface protein Tim-3 regulates macrophage activation and severity of an autoimmune disease. Nature 415 536–541
Nebbia G, Peppa D, Schurich A, Khanna P, Singh HD, Cheng Y, Rosenberg W, Dusheiko G, Gilson R, ChinAleong J, Kennedy P and Maini MK 2012 Upregulation of the Tim-3/galectin-9 pathway of T cell exhaustion in chronic hepatitis B virus infection. PLoS ONE 7 e47648
Nemeth J, Winkler HM, Boeck L, Adegnika AA, Clement E, Mve TM, Kremsner PG and Winkler S 2011 Specific cytokine patterns of pulmonary tuberculosis in Central Africa. Clin. Immunol. 138 50–59
Ortiz-Martinez Y 2017 Assessing worldwide research productivity on tuberculosis over a 40-year period: A bibliometric analysis. Indian J. Tuberc. 64 235–236
Park JS, Kang YA, Kwon SY, Yoon HI, Chung JH, Lee CT and Lee JH 2010 Nested PCR in lung tissue for diagnosis of pulmonary tuberculosis. Eur. Respir. J. 35 851–857
Qiu Y, Chen J, Liao H, Zhang Y, Wang H, Li S, Luo Y, Fang D, Li G, Zhou B, Shen L, Chen CY, Huang D, Cai J, Cao K, Jiang L, Zeng G and Chen ZW 2012 Tim-3-expressing CD4+ and CD8+ T cells in human tuberculosis (TB) exhibit polarized effector memory phenotypes and stronger anti-TB effector functions. PLoS Pathog. 8 e1002984
Reddy PB, Sehrawat S, Suryawanshi A, Rajasagi NK, Mulik S, Hirashima M and Rouse BT 2011 Influence of galectin-9/Tim-3 interaction on herpes simplex virus-1 latency. J. Immunol. 187 5745–5755
Sada-Ovalle I, Ocana-Guzman R, Perez-Patrigeon S, Chavez-Galan L, Sierra-Madero J, Torre-Bouscoulet L and Addo MM 2015 Tim-3 blocking rescue macrophage and T cell function against Mycobacterium tuberculosis infection in HIV+ patients. J. Int. AIDS Soc. 18 20078
Sakuishi K, Jayaraman P, Behar SM, Anderson AC and Kuchroo VK 2011 Emerging Tim-3 functions in antimicrobial and tumor immunity. Trends Immunol. 32 345–349
Shafiani S, Tucker-Heard G, Kariyone A, Takatsu K and Urdahl KB 2010 Pathogen-specific regulatory T cells delay the arrival of effector T cells in the lung during early tuberculosis. J. Exp. Med. 207 1409–1420
Srivastav NC, Rai D, Tse C, Agrawal B, Kunimoto DY and Kumar R 2010 Inhibition of mycobacterial replication by pyrimidines possessing various C-5 functionalities and related 2’-deoxynucleoside analogues using in vitro and in vivo models. J. Med. Chem. 53 6180–6187
Subbian S, Tsenova L, O’Brien P, Yang G, Koo MS, Peixoto B, Fallows D, Zeldis JB, Muller G and Kaplan G 2011 Phosphodiesterase-4 inhibition combined with isoniazid treatment of rabbits with pulmonary tuberculosis reduces macrophage activation and lung pathology. Am. J. Pathol. 179 289–301
Urdahl KB, Shafiani S and Ernst JD 2011 Initiation and regulation of T-cell responses in tuberculosis. Mucosal Immunol. 4 288–293
Wang F, He W, Yuan J, Wu K, Zhou H, Zhang W and Chen ZK 2008 Activation of Tim-3-Galectin-9 pathway improves survival of fully allogeneic skin grafts. Transpl. Immunol. 19 12–19
Wang F, Hou H, Wu S, Tang Q, Huang M, Yin B, Huang J, Liu W, Mao L, Lu Y and Sun Z 2015 Tim-3 pathway affects NK cell impairment in patients with active tuberculosis. Cytokine 76 270–279
Wu CY, Hu HY, Pu CY, Huang N, Shen HC, Li CP and Chou YJ 2011 Pulmonary tuberculosis increases the risk of lung cancer: a population-based cohort study. Cancer 117 618–624
Zhang Y, Ma CJ, Wang JM, Ji XJ, Wu XY, Moorman JP and Yao ZQ 2012 Tim-3 regulates pro- and anti-inflammatory cytokine expression in human CD14+ monocytes. J. Leukoc. Biol. 91 189–196
Acknowledgements
This study was supported by National Natural Science Foundation of China (No. 81670080). We appreciate the helpful comments from the reviewers of this paper.
Author information
Authors and Affiliations
Corresponding author
Additional information
Communicated by Dipankar Nandi.
Corresponding editor: Dipankar Nandi
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Figure 1
Flow cytometric data for sorting CD8+ T cells from healthy controls, LPTB patients and PTB patients. In the HC group, n = 20; in the LPTB group, n = 40; and in the active PTB group, n = 50 (EPS 10283 kb)
Rights and permissions
About this article

Cite this article
Kang, J., Wei, ZF., Li, MX. et al. Modulatory effect of Tim-3/Galectin-9 axis on T-cell-mediated immunity in pulmonary tuberculosis. J Biosci 45, 60 (2020). https://doi.org/10.1007/s12038-020-0023-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s12038-020-0023-z