
Abstract
According to the United States Centers for Disease Control and Prevention (CDC), as of July 11, 2016, the reported average incidence of children diagnosed with an autism spectrum disorder (ASD) was 1 in 68 (1.46%) among 8-year-old children born in 2004 and living within the 11 monitoring sites’ surveillance areas in the United States of America (USA) in 2012. ASD is a multifaceted neurodevelopmental disorder that is also considered a hidden disability, as, for the most part; there are no apparent morphological differences between children with ASD and typically developing children. ASD is diagnosed based upon a triad of features including impairment in socialization, impairment in language, and repetitive and stereotypic behaviors. The increasing incidence of ASD in the pediatric population and the lack of successful curative therapies make ASD one of the most challenging disorders for medicine. ASD neurobiology is thought to be associated with oxidative stress, as shown by increased levels of reactive oxygen species and increased lipid peroxidation, as well as an increase in other indicators of oxidative stress. Children with ASD diagnosis are considered more vulnerable to oxidative stress because of their imbalance in intracellular and extracellular glutathione levels and decreased glutathione reserve capacity. Several studies have suggested that the redox imbalance and oxidative stress are integral parts of ASD pathophysiology. As such, early assessment and treatment of antioxidant status may result in a better prognosis as it could decrease the oxidative stress in the brain before it can induce more irreversible brain damage. In this review, many aspects of the role of oxidative stress in ASD are discussed, taking into account that the process of oxidative stress may be a target for therapeutic interventions.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Autism spectrum disorder (ASD) is a complex neurodevelopmental syndrome, which usually occurs before 3 years of age. In general, ASD is characterized by (1) pervasive deficits in social interaction, (2) impairments in verbal and nonverbal communication, and (3) stereotyped patterns of interests and activities. Although ASD is fundamentally diagnosed on the basis of an evaluation of clinical and behavioral criteria, which should identify alterations in social interaction, deficits in verbal and nonverbal receptive/expression, speech, and hyper-focused repetitive behaviors, individuals diagnosed with ASD may also display a range of problematic behaviors including hyperactivity, poor attention, impulsivity, aggression, self-injury, and tantrums [1,2,3,4].
According to the reports from the US Center for Disease Control and Prevention (CDC), last updated on July 11, 2016, data collected at 11 separate reporting sites in 2012 showed that the reported average incidence of children diagnosed with an autism spectrum disorder (ASD) was 1 to 68 (1.46%), among 8-year-old children born in 2004 and living within the 11 monitoring sites’ surveillance areas in the USA held in 2012 (with a site ASD incidence ranging from about 1 in 122 (0.82%) to about 1 in 41 (2.46%) [5]. ASD is a multifaceted neurodevelopmental disorder that is also considered a hidden disability, as, for the most part.
Although there is no consensus today on the causes of ASD, multiple environmental and genetic risk factors have been proposed [6, 7]. The relationship between genetics and environment, which may elicit even immune and inflammatory responses in the brain, is thought to be a major key in the understanding of ASD pathophysiology and has in recent years become a subject of intensified research [8,9,10,11]. Diverse prenatal and perinatal environmental exposures are associated with an increased risk of ASD [12,13,14]. Prolonged exposure to environmental pollutants (oxidizing agents, heavy metals, herbicides, and pesticides), photosensitizers, UV light, or ionizing radiation have been studied as potential causal factors [15,16,17,18].
More recently, there is growing evidence supporting the role of oxidative stress in the pathophysiology of a number of neuropsychiatric diseases [19,21,21] and especially in ASD (Table 1) [43,44,45,46,46]. The response to oxidative stress is a keystone in neuroinflammation, in as much the latter is still considered one of the leading cause of ASD [47]. Children with ASD diagnosis are considered more vulnerable to oxidative stress because of their low plasma and cellular glutathione (L-γ-glutamyl-L-cysteinyl-glycine) levels and decreased glutathione reserve capacity [38, 48]. Several studies have suggested that the redox imbalance and oxidative stress are integral parts of ASD pathophysiology [49, 50]. There is also evidence to suggest a relationship between the oxidative stress found in subjects diagnosed with ASD and environmental exposures, particularly for heavy metals, such as mercury [17, 51,53,53].
Along with the host’s immune system, microbiota plays an essential role in the proper functioning of the body participating in metabolic tracts and acting as a source of key nutrients. In this sense, the intestinal microbial imbalance can be a consequence of the exposure to many environmental factors, including further microorganisms, xenobiotics, and pollutants. Alterations in the microbiota and the presence of enteric pathogens may contribute to microbial dysbiosis, with possible suggestions on ASD pathogenesis [54, 55]. Many studies have reported an increased presence of gastrointestinal (GI) symptoms in children with ASD. Altered microbiome profiles, pro-inflammatory responses, and impaired intestinal permeability have been observed in children with ASD and co-morbid GI symptoms. Recent data would suggest that GI impairments in autistic subjects are associated with mitochondria dysfunction and the enteric microbiome [50, 56, 57]. Metabolic disorders inducing GI are related to mitochondria redox imbalance [50]. The connection between redox impairment via a mitochondria dysfunction in the enteric milieu and GI has been recently investigated in a blinded case-control study with ten children with ASD and GI complaints, ten children with Crohn’s disease, and ten children with non-specific gastrointestinal complaints matched on age and gender and undergoing elective diagnostic colonoscopy [57].
Moreover, children with ASD experience significantly more GI symptoms than children without ASD [58], and their GI symptoms correlate strongly with their ASD severity [59]. Possible connections between the GI tract and mitochondrial abnormalities specific to ASD can be distinguished, such as mitochondrial dysfunction may result in GI dysfunction, exposures to environmental stressors which are associated with ASD can affect the GI tract and mitochondria, and also some substances may disrupt mitochondrial function (lipopolysaccharide or metabolites from enteric bacteria) [56].
In this review, many aspects of the role of oxidative stress in ASD are discussed, taking into account that the process of oxidative stress may be a target for therapeutic interventions. Early assessment and treatment of antioxidant status may result in a better prognosis as it may decrease the oxidative stress in the brain and the brain/gut axis before it can induce more irreversible brain damage.
The literature search was carried out using PubMed and Scopus, supplemented with Google Scholar and the reference lists of relevant papers.
Recent Insights on Oxidative Stress and Mitochondrial Dysfunction
Oxidative stress can be defined as an imbalance between pro-oxidants and antioxidants, resulting in a damaging action towards the cell caused by reactive oxygen species (ROS) or reactive nitrogen species (RNS) [60]. Fundamentally, ROS are signaling molecules, which may promote cell survival and tissue renewal [61, 62] or counteract cell survival gene expression, including the antioxidant enzymatic endowment, so leading cell to apoptosis [62]. The ability of cells to properly respond to oxidative stress occurs when “mild oxidative stress” is elicited, usually by a relatively low content of ROS, a condition called eustress [63]. The potentially damaging oxidative stress is called distress, and it is the major cause of neuroinflammation and impairment in the astrocyte-neuron crosstalk leading to ASD [11, 64,65,66,67,68]. The full comprehension of the role of ROS in ASD is still far to be elucidated. The classical overview about ROS homeostasis takes into account a balance between the antioxidant ROS scavenging system and the reactive free radicals produced during the activity of mitochondria, peroxisomes, endoplasmic reticulum, and proteasome [60]. Under normal conditions, a dynamic equilibrium exists between the production of ROS/RNS and the antioxidant capacity of the cell [69]. Fundamentally, ROS and RNS include superoxide (O2−), hydroxyl, peroxyl, alkoxy, hydrogen peroxide, and peroxynitrite free radicals [21, 63]. Superoxide is the first reduction product of molecular oxygen and is an important source of hydroperoxides, lipo-peroxides, and harmful free radicals [70]. These are considered main byproducts of the normal metabolism of oxygen or nitrogen and have important roles in a wide number of biological processes, such as the killing of bacteria. The excess amounts of ROS can be produced by the organism in response to pathogenic defenses or generated at normal levels but not neutralized due to the insufficient antioxidant capacity of the redox homeostasis system. ROS are formed as intermediates and byproducts in the energy production cycle in mitochondrial electron transfer chain reactions [71, 72]. The ability of ROS to be scavenged by the enzymatic system of which cells are endowed depends on a huge panoply of proteins, the major of which are superoxide dismutase (SOD), catalase (CAT), and glutathione peroxidase (GPx) [21, 60]. ROS are fundamentally produced by the oxidative reactions occurring during mitochondria activity, which is closely related to endoplasmic reticulum stress (ER stress) and the activity of peroxisomes and proteasomes [60]. The same mitochondria dysfunction depends on the elevated production of ROS by ER stress [73]. Recently reported data showed that the guanosine triphosphatase (GTPase) Rab32, a known regulator of the mitochondria-associated membrane (MAM) proteins, is strongly associated with ER stress, leading to both mitochondrial dysfunction and neurological disorders [74]. The cellular response to oxidative stress involves not only the full endowment of the CYP cytochrome family and many antioxidant enzymes but also complex signaling machinery leading to the expression of the transcription factor called nuclear factor (erythroid-derived 2)-like 2 (Nrf2), which is a leading factor in ROS scavenging [75,76,78]. Together with the Kelch-like ECH-associated protein 1, this factor plays a major role in the development of many neurodegenerative diseases [78, 79], including ASD [80,81,82].
Oxidative Stress in the Pathogenesis of Neurodegenerative Disorders and the Importance/Role of Selenium
Increased oxidative stress has been involved in the pathogenesis of several neurodegenerative diseases, including Alzheimer’s and Parkinson’s disease. In individuals with these diseases, the levels of glutathione peroxidase-4 (GPx4) and selenoprotein P (Sepp 1), as well as the expression of its regulatory genes, are usually in dyshomeostasis. In the Alzheimer’s disease, the form of β-amyloid plaques that are associated with low Se concentration and oxidative stress occur [83]. Recently, it was summarized in a review that Se and selenoproteins might be closely involved in neurotransmission due to the antioxidants, inflammation, influencing protein phosphorylation and ion channels, alteration of calcium homeostasis, and brain cholesterol metabolism [84]. Therefore, numerous brain diseases can be manifested with the aid of Se and selenoproteins. For instance, in relation to Alzheimer’s disease, maybe selenoproteins affect β-amyloid (Aβ) and hyperphosphorylated tau aggregation and toxicity as well as interact with redox-active metals (Cu, Fe, and Hg) in the brain. It can also be involved in antioxidant enzyme activity and to possess signaling functions via neuronal apolipoprotein E receptor-2 (ApoER2) [85].
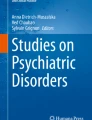
It is known that oxidative stress plays an important role also in the pathophysiology of ASD [23, 27, 86,87,88,89,90,91,92]. Many studies have reported evidence of oxidative stress in individuals with ASD [24, 27, 28, 32, 33, 35, 39,39,40, 86, 88, 93,93,94,96]. Oxidative stress leads to a number of changes such as lipid peroxidation, protein and DNA oxidation, inflammation, altered immune response, decreased DNA methylation, and epigenetic dysregulation [97] (Fig. 1).

The role of oxidative stress in the development and pathophysiology of ASD. Scheme of different pathways of oxidative stress in ASD adapted from [97] using literature sources [3, 38, 39, 91, 98,96,97,98,99,100,101,102,103,104,105,106,107,111]. See the text for details. ATP, adenosine triphosphate; CNS, central nervous system; CNVs, copy-number variations; GIT, gastrointestinal tract; ROS, reactive oxygen species; SOD, superoxide dismutase; CAT, catalase; GPx, glutathione peroxidase; GPX1, glutathione peroxidase 1 gene; GST, glutathione S-transferase; GST, glutathione-S-transferase gene
Blood Oxidative Stress Markers in ASD Patients
Antioxidant status in persons with ASD is diminished, suggesting pathology of ASD is associated with increased production of oxidative species and/or incorrect antioxidant metabolism. Thus, ASD can result from defects in the metabolism of cellular antioxidants which maintain intracellular redox status by quenching ROS [3]. Oxidative stress markers are highly associated with considerable cellular injury and manifest severe mitochondrial dysfunction in autistic pathology [24]. In patients with ASD, levels of various oxidative stress markers in blood were found to be increased (Table 1).
Lipid peroxidation in blood plasma is significantly increased in ASD children compared to their neurotypical siblings suggesting enhanced oxidative stress in ASD [23]. RBCs thiobarbituric acid reactive substances (TBARS) as a lipoxidation marker was found to be twice higher in ASD children than in age-matched controls [27]. Chauhan et al. [112] found the significantly increased levels of amino-glycerophospholipids (AGPs) in the blood plasma of children with ASD as compared to their neurotypical developmentally normal siblings, and proposed plasma AGP level as a potential diagnostic marker for ASD. Phospholipid composition of the erythrocyte membrane is altered in ASD. In the RBC membranes of children with ASD in comparison with their neurotypical siblings, the levels of phosphatidylethanolamine (PE) are reduced, whereas phosphatidylserine (PS) is elevated [112]. The increased oxidative stress in ASD can lead to loss of asymmetry of biological membrane and externalization of PS [113] and alteration of AGPs, i.e., PS and PE [23]. Significant depletion of total n-3 polyunsaturated fatty acids (PUFA) in RBC membranes [87] shows evidence of oxidative damage [114]. Lower erythrocyte and plasma GPx activities in ASD were also reported [32].
Selenium is an essential cofactor for GPx [115]. Increased lipid peroxidation [27] and decreased GPx in RBCs of children with ASD [32] suggest a potential deficiency of Se [116]. It was confirmed that GPx activity positively correlates with Se levels [117]. Lower GPx activity in Se deficiency is associated with peroxidative damage and mitochondrial dysfunction [118]. Pre-treatment with Se decreases lipid peroxidation and increases GPx activity [119]. In different studies of children with ASD, the activity of GPx is highly variable [120].
Also, glutathione redox imbalance is a typical event in ASD (Fig. 1, Table 1). Glutathione, an intracellular thiol tripeptide present in all mammalian tissues, plays a key role in cellular protection against oxidant damage [121]. Glutathione is an antioxidant with cellular protective functions, including ROS scavenging in the brain, and is involved in various cellular survival pathways in response to oxidative stress [122]. In ASD, genetic variations in glutathione-related pathways have been found [38, 123,123,125] and have been correlated with behavior in ASD individuals [126, 127]. Lower concentrations of reduced glutathione (GSH), higher levels of oxidized glutathione (GSSG), and a decrease in the GSH/GSSG redox ratio [35, 38, 93] in ASD patients compared to controls, have been reported. Also, lower GSH levels [128] and markers of increased oxidative stress [129] have been correlated with the severity of ASD. Furthermore, oxidative stress markers were also associated with the severity of gastrointestinal problems in ASD patients [130].
Moreover, the dysregulated pattern of metallothionein (MT) expression in ASD (Rett syndrome) was observed [41]. A higher level of MT mRNA expression in peripheral blood leucocytes (PBMCs) in ASD children compared with healthy children were reported [42] (Table 1). In humans, four main MT isoforms were described: the ubiquitous MT-1 and MT-2 [131]—from which MT-1A, MT-1E, and MT-2A are the most abundant ones [132], the brain-specific MT-3 [133], and the squamous epithelium-specific MT-4 [134]. MTs have been implied in neurodegenerative diseases [135,135,137], and abnormalities in their concentration or structure, as well as the presence of anti-MT antibodies, have been hypothesized to be associated with ASD [138].
Oxidative Stress in the Brain of ASD Patients and the Importance of Selenium as a Free Radical Scavenger
Physiological abnormalities characterizing ASD such as oxidative stress, mitochondrial dysfunction, and immune dysregulation/inflammation (Fig. 1) have been reported not only in studies examining peripheral biomarkers such as blood and urine but also in those focusing on the brain—they have found in brain tissue derived from patients with ASD. The brain regions in which these abnormalities have been found are involved in speech and auditory processing, social behavior, memory, sensory, and motor coordination [139].
The brain is extremely vulnerable to oxidative stress due to its limited antioxidant capacity, high energy demands, and high contents of unsaturated lipids and iron (Fe) [97]. The brain tissue has shown increased levels of markers of oxidative damage, coupled with decreased antioxidant status in the brain of ASD individuals compared with age-matched control persons [97]. In the brain, the levels of lipid hydroperoxide (LOOH) [22], a product of fatty acid oxidation; of malonyldialdehyde (MDA) [140], an end-product of lipid peroxidation; of 8-hydroxy-2′-deoxyguanosine (8-OH-dG) [26, 141,141,143], a marker of oxidative DNA damage; of protein carbonyl [97], a marker of protein oxidation; and of 3-nitrotyrosine (3-NT) [30], a marker of protein nitration, as well as the expression of carboxyethyl pyrrole (CEP), a marker of lipid-derived oxidative protein modification, were significantly increased in ASD individuals [29]. Also, a greater number of lipofuscin (a matrix of oxidized lipid and cross-linked protein)-containing brain cells was reported in language-related cortical areas 22, 39, and 44 in ASD [144]. ASD is associated with deficits in glutathione antioxidant defense in selective regions of the brain [145]. In the brain of ASD individuals, decreased the ratio of GSH/GSSG redox/antioxidant capacity and increased oxidative stress were found [146].
Figure 2 demonstrates oxidative stress formation in the brain of ASD patients and the substantial role of Se in protecting neuronal cells against oxidative damage and death. Oxidative stress is a major underlying cause of neurodegenerative and neuroinflammatory disorders and the blood-brain barrier (BBB) injury associated with them [152]. The BBB is a highly selective semipermeable border that separates the circulating blood from the brain, and extracellular fluid in the CNS [153] and is formed by endothelial cells of the capillary wall, astrocyte end-feet ensheathing the capillary, and pericytes embedded in the capillary basement membrane [148].

Schematic representation of oxidative stress in the brain of ASD patients and the importance of selenium in its reducing. (A) Intact (undamaged) blood-brain barrier (BBB) in healthy individuals—allows normal diffusion and transport across the BBB [147]. The BBB consists of three basic parts: endothelial cells of the blood capillary, astrocyte of the brain, and pericytes embedded in the basement membrane of the capillary [148]. In the healthy brain, the BBB is intact due to claudins, occludin, and junctional adhesion molecules (JAMs) which create together the tight junction between endothelial cells. Actin and the zona occludens (ZO-1 and ZO-2, etc.) also create a scaffold for the tight junction. This construction is also supported by the extracellular matrix (ECM) [147]. (B) BBB in ADS patients—oxidative stress at brain endothelial cells. If the BBB is damaged, an altered diffusion and transport across the BBB occur. In the unhealthy brain, reactive oxygen species (ROS) accumulate from various sources, including mitochondria (1), the lipid bilayer (2), microglia (3), and astrocytes (4). An excessive formation of ROS causes altering the tight junctions, the breakdown of the ECM by enzymes matrix metalloproteinases (MMPs) and subsequent loss of BBB integrity [147]. (C) Detoxification of hydrogen peroxide (H2O2) and lipid hydroperoxides (LOOH) by Se-dependent glutathione peroxidase (GPx) [149]. Se reduces lipid peroxidation and enhances the activity of the selenium-dependent antioxidant enzyme GPx [119]. GPxs are considered to be key players in important biological contexts far beyond the detoxification of hydroperoxides. Se-containing GPxs are only five from eight identified (GPx1–4 and 6) [150]. The main substrate of GPx1 is H2O2; however, it can also degrade fatty acid hydroperoxides [151]. GPx reduces free H2O2 to water and degrades LOOH to their corresponding alcohols and water. GPx activity requires two molecules of the tripeptide reduced glutathione (GSH) which is converted by the enzyme glutathione reductase (GR) to oxidized glutathione (GSSG) [149], NADPH (nicotinamide adenine dinucleotide phosphate) is consumed in the reaction to form of NADP+ (oxidized form of NADPH)
In the brain of a healthy human, the BBB is due to compact proteins such as claudins, occludin, and junctional adhesion molecules (JAMs) which form together with the tight junction between neighboring endothelial cells of brain capillaries [147] (Fig. 2). The tight junction proteins are then anchored in the endothelial cells by scaffolding proteins such as the zona occludens (ZO-1, ZO-2, ZO-3) [154]. Capillaries present in the CNS are considerably different from those in the remaining parts of the body due to BBB, which creates an irreplaceable filter protecting the brain [155, 156]. In addition to these protective layers, cerebral endothelial cells are equipped with a defense system against oxidative stress including increased GSH, GPx, glutathione reductase (GR), and catalase (CAT) compared to the rest of the brain [157]. Glutathione, in particular, has been shown to play an important role in the maintenance of BBB integrity [158]. Glutathione as a thiol tripeptide is an important antioxidant in the brain. Glutathione is critical for protecting dopamine neurons in the substantia nigra pars compacta from free radical damage [159]. Glutathione is involved in both neuroprotection against oxidative stress and neuroinflammation in ASD by improving the antioxidative stress system [160].
One of the most well-known mechanisms for disruption of the BBB from oxidative stress is via matrix metalloproteinase (MMP) activation which leads to degradation of extracellular matrix (ECM) around cerebral blood vessels and neurons [161] (Fig. 2). MMPs are activated by ROS and cause loss of BBB integrity, which leads to cerebral ischemia-reperfusion injury [162].
The increased production of ROS can exert oxidative stress, and if excess ROS are not properly regulated, they can cause damage to cellular lipids, proteins, and DNA [163]. The neuronal membrane is mainly formed with polyunsaturated fatty acids (PUFAs), especially docosahexaenoic acid [164]. PUFAs are highly susceptible to lipid peroxidation [165,165,167], which leads to lipid hydroperoxide formation, often as a response to oxidative stress [165]. Products from lipid peroxidation such as 4-hydroxynonenal (HNE) are cytotoxic to neurons [167], and its high level has been found in a variety of neurodegenerative diseases [167,167,169].
Oxidative Stress, the Central Nervous System, and Neurobehavioral Disorders
The central nervous system (CNS) is particularly vulnerable to oxidative stress because of its limited antioxidant capacity, higher energy requirements, and higher levels of lipids/ketones and iron [170]. The brain makes up about 2% of body mass but consumes 20% of the body’s metabolic oxygen. Thus, neurons consume a disproportionately large share of the body’s energy [171]. Because of the neurons’ lack of glutathione production capacity, the CNS has a limited capacity to detoxify ROS. Therefore, neurons are the first cells to be affected by the increase in ROS and the shortage of antioxidants. In this sense, neurons are the cells most susceptible to oxidative stress [170, 172, 173]. Moreover, antioxidants are required for neuronal survival during the early critical period of CNS development [20].
As such, oxidative stress has been implicated in the pathology of several other neurobehavioral disorders, including schizophrenia, bipolar disorder, and Alzheimer’s disease [174,174,175,177]. Children are more vulnerable to oxidative stress than adults because of their naturally low GSH levels from conception through infancy [178]. Altogether, these studies suggest that the brain is highly vulnerable to oxidative stress, particularly during the early stage of its development, which may result in neurodevelopmental disorders such as ASD. An increasing amount of recent evidence suggests that redox imbalance and oxidative stress may also contribute to autism pathophysiology [49, 179, 180].
Evidence of Oxidative Stress in Autism Spectrum Disorder
Children with ASD seem to be more vulnerable to oxidative stress in the form of increased lipid peroxidation due to deficient antioxidant defense mechanism, especially as young children (newborns) [181,181,183]. This finding suggests that early antioxidant supplementation would have a better prognosis as it may decrease the oxidative stress before that stress can induce more irreversible brain damage [49, 184]. Several lines of evidence support an association of oxidative stress with ASD. First, there is evidence of reduced endogenous antioxidant capacity. Specifically, reduced enzymatic activities of GPx, SOD, and CAT and reduced levels of total glutathione and cysteine have been reported [31, 33]. The significant decreases in the levels of homocysteine, cystathionine, cysteine, and GSH indicate that the trans-sulfuration enzymatic pathway is most probably less efficient in children having ASD diagnosis. The reduction in the levels of these metabolites is consistent with the decrease in methionine levels [185]. Also, there is an increase in the level of GSSG and a decrease in the level of GSH. Collectively, the observed changes in the levels of all those factors are strong evidence that oxidative stress is elevated in those children who have ASD diagnosis [186].
Levels of exogenous antioxidants, including vitamin C, vitamin E, and vitamin A in plasma, and zinc and selenium in erythrocytes were also reportedly reduced in individuals diagnosed with ASD [38, 187, 188]. Moreover, altered (increased) oxidative stress in children with ASD is derived from evidence of their impaired energy metabolism [189].
Magnetic resonance spectroscopic examination of the brains of ASD individuals has found reduced synthesis of ATP. Elevated lactate and pyruvate levels have also been reported [189]. Furthermore, reports have been published showing an improvement in certain behaviors following antioxidant administration to individuals with ASD. In a double-blind, placebo-controlled trial, the authors reported that high-dose vitamin C or carnosine improved autistic behavior over baseline in those who received the test substances while the blinded controls’ were essentially unchanged [190]. Likewise, children diagnosed with ASD, who had decreased blood levels of the antioxidants GSH and cysteine as well as a decreased GSH/GSSG ratio compared to the controls, had increases of these following a 3-week supplementation with betaine and folinic acid [33, 191].
Furthermore, increased excretion of oxidative stress biomarkers has been reported in children with ASD (Table 1). Specifically, the excretion of an F2-isoprostane, 8-iso-prostaglandin F2α, is increased in children with ASD diagnosis [28]. The isoprostane is a product of non-enzymatic oxidation of arachidonic acid and is widely recognized as a reliable marker of lipid peroxidation [192]. Recent evidence supports the hypothesis that 8-isoprostane and cysteinyl-leukotrienes are possible markers for the early diagnosis of ASD [193]. Nitric oxide, a free radical that can block energy production, was found to be increased in ASD as compared to age and sex-matched controls [31]. Also, elevated nitrite concentrations have been detected in individuals with ASD diagnosis along with elevations of thiobarbituric acid reactive substances and xanthine oxidase activity in red cells [194].
Furthermore, evidence of oxidative stress in individuals with ASD diagnosis has been recently assessed by the observation that decreased serum levels of SOD might be implicated in the onset and development of ASD diagnosis in children [45]. All these reports strongly suggest that oxidative stress is of the utmost importance in ASD pathogenesis and development.
Finally, based on a recently reviewed relationship between those with ASD diagnosis and their gut microbiome, propionic acid (PPA), which is released from gut microbiome and might have toxic effects, besides some beneficial action, on the mitochondria, may play a key role in those who have ASD diagnosis and PPA has been recently related to the pathogenesis of ASD [195].
Role of Oxidative Stress in Autism Spectrum Disorder
Metallothioneins are small-molecular-weight proteins with free radical scavenging properties. MTs have important roles in metal homeostasis and detoxification. There are four MT isoforms: MT-1, MT-2, MT-3, and MT-4. The classification into classes is based on the position of cysteine residues in the MT polypeptide chain. MT-1 and MT-2 are located in all tissues (particularly the kidney and liver), MT-3 is brain tissue-specific and is known as a growth inhibitory factor which may provide a neuroprotective and antioxidative effect, and MT-4 which is expressed in squamous epithelia associated with the oral mucosa, esophagus, and upper stomach [196, 197]. Metallothionein-3 is mainly expressed in the CNS. MT-3 possesses a unique neuronal growth inhibitory activity, and the levels of this intra- and extracellularly occurring metalloprotein are markedly diminished in the brain of patients affected by a number of metal-linked neurodegenerative disorders. The list of MT-3 functions suggests that it has a role not only in the CNS but also outside this organ. MT-3 in the CNS regulates divalent heavy metal homeostasis. Owing to its antioxidant properties and modulator function not only for Zn but also for Cu in the extra- and intracellular space, MT-3 protects neuronal cells from the toxicity of various Cu(II)-bound amyloids. Earlier studies suggest that Cu dyshomeostasis may contribute to ASD [198]. It is supposed that altered Cu metabolism in ASD may be related to impaired MT system functioning and activation of free radical oxidation [199, 200]. Moreover, certain interactions between zinc and copper may also significantly contribute to ASD pathogenesis via the modulation of the MT system-mediated excitotoxicity [18].
In animal studies, because of the lower enzyme activity levels of SOD and GPx in males than in females, oxidative damage to mitochondrial DNA is 4-fold higher in males compared to females [201]. The higher GSSG level, a reliable marker of intracellular oxidative stress, found in individuals with ASD diagnosis, is supported by the previous work of James et al. [38] that recorded 72% higher GSSG in children with ASD diagnosis as compared to GSSG levels found in neurotypical children. The unexpected, non-significant change in the activity of glutathione reductase (GR) in children having ASD diagnosis, when its activity was compared to the levels in the neurotypical children used as controls, could be explained on the basis that under physiological conditions, GR activity is sufficient to maintain an expected GSH/GSSG ratio. However, excessive intracellular oxidative stress that exceeds the reducing capacity of the patient’s GR efficiency will induce the export of GSSG to the plasma in an attempt to regain intracellular redox homeostasis [38, 202]. Also, there is a reported association between genetic predisposition and ASD diagnosis, suggesting that GST contributes to the risk of oxidative stress and ASD [38, 203].
In this context, a fundamental role is exerted by thioredoxin (Trx) levels. The key biological activities of Trx that apply to human diseases can be categorized as antioxidative, growth-promoting, anti-apoptotic, and inflammation-modulating. Beyond its protective role, the Trx system is involved in various cellular processes, such as cell-cell communication, transcriptional regulation, cell signaling, and DNA synthesis [204,204,206]. Any particular biological property of Trx is unlikely to be either “good” or “bad” in human diseases. Furthermore, the function of Trx depends on the activity of the thioredoxin reductase (TrxR). Overexpression of TrxR as a major antioxidant enzyme could support the hypothesis that oxidative stress is linked with the etiology of ASD [33].
There is mounting evidence that abnormalities of the patients’ levels of ROS and NO may underlie a wide range of neuropsychiatric disorders. Abnormal methionine metabolism, high levels of homocysteine, and oxidative stress are also generally associated with neuropsychiatric disorders. NO signaling has been implicated in some physiological functions such as the release of noradrenaline and dopamine. It is thought to have neuroprotective effects at low to moderate concentrations, but excessive NO production can cause oxidative stress to neurons, thus impairing their function [90]. In children with ASD, there were higher levels of homocysteine, which was negatively correlated with GPx activity, low human paraoxonase 1 arylesterase activity, and suboptimal levels of vitamin B12 [207,207,209]. Lipid peroxidation was found to be elevated in individuals having ASD diagnosis, indicating that increased oxidative stress was causally linked to the diagnosis. Moderate to dramatic increases in isoprostane levels decreased levels of phosphatidylethanolamine, and increased levels of phosphatidylserine were observed in children with ASD diagnosis as compared to neurotypical controls. Furthermore, levels of major antioxidant proteins transferrin (iron-binding protein) and ceruloplasmin (copper-binding protein) were found to be significantly reduced in sera of those children with ASD diagnosis. A strong correlation was observed between the reduced levels of these proteins and the child’s loss of previously acquired language skills [90].
Another study measured levels of metabolites in methionine pathways in children with ASD diagnosis and found that plasma methionine and the ratio of S-adenosylmethionine (SAM) to S-adenosyl-homocysteine (SAH), an indicator of methylation capacity, were significantly decreased in the children with ASD diagnosis relative to neurotypical controls [38]. Also, plasma levels of cysteine, GSH, and the ratio of GSH/GSSG, indicative of antioxidant capacity and redox homeostasis, were significantly decreased in the group with ASD diagnosis [50, 210, 211]. The same study evaluated common polymorphic variants known to modulate these metabolic pathways in 360 children diagnosed with ASD and in 205 healthy neurotypical controls. Differences in allele frequency and/or significant gene-gene interactions were studied for relevant genes encoding the reduced folate carrier polymorphism (RFC 80G), transcobalamin II (TCN2 776G), catechol-O-methyltransferase (COMT 472G), methylenetetrahydrofolate reductase (MTHFR 677C and 1298A), and glutathione-S-transferase (GST M1) [38]. Only reduced folate carrier C1 G allele frequency is shown to be elevated in the mothers, but not in the fathers or the ASD children.
Possible Conditions Making Neurons in Pediatric Subjects’ Brain Particularly Vulnerable to Oxidative Stress
The high rate of aerobic metabolism and elevated concentrations of oxidizable molecules such as polyunsaturated fatty acids and catecholamines as well iron make the nervous tissue especially vulnerable to the oxidative stress [22]. Also, several proteins that are involved in normal brain function are vulnerable to oxidative modifications that change their activity. ROS play a critical role in both normal and pathological cell signaling pathways, including kinase activity, calcium homeostasis, and gene regulation. Also, the activities of the receptor and non-receptor types of protein kinase C, protein tyrosine kinases and transcription factors such as nuclear factor kappa-light-chain-enhancer of activated B cells (NF-kappaB) are controlled by oxidative stress [26]. Membrane phospholipids are linked to most neuronal membrane proteins. Abnormalities in the metabolism of transitional metals such as copper (a pro-oxidant metal) selectively oxidized phosphatidylethanolamine in liposomes containing brain lipids cause deleterious effects in those diagnosed with autism [22, 52, 86, 212]. Excitotoxicity has been reported as a contributing factor in oxidative stress, as well as a result of oxidative stress. Glutamic acid decarboxylase (GAD), an enzyme that transforms glutamate to γ-aminobutyric acid (GABA), a glutamate transporter; glutamine synthase; and GABA receptors are susceptible to oxidative stress [90]. Reduced GABA and elevated extracellular glutamate are renowned for increasing excitotoxicity [213]. Increased levels of plasma glutamate and reduced levels of GAD and glutamine have been reported in individuals with ASD [86, 213, 214].
Oxidative Stress and Immune System Response in ASD?
Previous studies have reported a relationship between deleterious immune system response and oxidative stress. Alterations in phagocyte functions, such as chemotaxis, adherence, or tumor necrosis factor-α (TNF-α) production, have been reportedly correlated with oxidative stress in endotoxin-stimulated septic shock [45, 215]. The oxidant and antioxidant balance are fundamental for the normal functioning of the immune system’s cells because these cell functions are specially linked to ROS generation [86, 215]. Serotonin, found mostly in the gut where the majority (about 70%) of the human immune system resides, is an immune system modulator among its other functions. Elevated serotonin levels have been found in the blood of patients with ASD diagnosis [216,216,218]. Its increased levels might also lead to gut dysfunction and immune alterations in such subjects. Decreased response to T cell mitogens, depletion of CD4+ (cluster of differentiation 4) T-helper/inducer cells, reduced natural killer cell activity, and increased neopterin levels in urine and plasma are immune system abnormalities in individuals with ASD [86, 202]. The pathogenesis of a patient diagnosed with ASD includes an imbalance in serum cytokines and immunoglobulins [219, 220], and inappropriate antibody response to the combined live measles, mumps, and rubella (MMR) virus vaccine [86, 221]. ROS and oxidative stress could participate in exacerbating the neuroinflammation pattern observed in ASD [11, 222].
Conclusion
Oxidative stress-induced mechanisms are believed to be the major cause for ASD [24] along with certain other physiological abnormalities, which characterize this disease such as mitochondrial dysfunction and immune dysregulation/inflammation [139]. Figure 1 summarizes many of the knowledge addressed in this review. Interactions between genetic and environmental factors may potentiate increased oxidative stress in ASD children [3]. Among genetic factors, polymorphisms of genes involved in the metabolism of glutathione [3] such as GPX1 [98] and GST [99], abnormality in genes of oxidative stress, and detoxification pathways are known [38, 100, 101]. Also, copy-number variations (CNVs) in ADS pathogenesis have been described [102]. Environmental factors include a number of influences that can threaten the individual prenatally or perinatally as well as postnatally [97]. These include the exposure of the mother or the child to heavy metals [17, 91, 223,223,224,225,226,227,228,229,230,232], infections [103], some drugs [97, 233], and other toxins from the environment such as cigarette smoke, polluted air, and organophosphate pesticides [91]. Recently, increased risk for an atypical autism diagnosis following a thimerosal-containing vaccine has been reported [234].
Moreover, the amount of Hg in the hair of children with ASD showed a significant correlation with the number of maternal dental amalgams [233]. In children with ASD, 2.5-fold higher oral antibiotic use during their first 18 months of life was observed [233]. Mitochondrial dysfunction and aberrant accumulation of transition metals may lead to the excessive generation of ROS [235]. Increased generation of ROS and decreased antioxidant defense lead to an imbalance between the production of free radicals and the ability of the body to counteract or detoxify their harmful effects—oxidative stress [97]. Oxidative stress causes a variety of undesirable processes such as oxidative degradation of lipids, proteins, and DNA [236], and inflammation changes [97, 237] which can cause damage brain tissue damage [104], modifies the immune response [97] and inhibits methionine synthase [105, 238], resulting in decreased DNA methylation [106] and epigenetic dysregulation, which all lead to the clinical symptoms of ASD [97].
The evidence indicates that oxidative stress is an integral part of the pathophysiology (or physiopathology) of ASD and is related to the severity of the characteristic symptoms exhibited by subjects having ASD. However, the ability to fully elucidate the mechanisms by which ROS and RNS exacerbate or induce ASD during neurodevelopment is still far to be fully accomplished and ask for further insightful evidence and clinical reports. While the current literature suggests that improving the oxidative status of children with ASD diagnosis has the potential to reduce the affected child’s symptoms, a suggestion that should be considered as a target for ameliorative therapeutic interventions, many further research studies are needed to comprehend how helping children with this pathology.
References
Barnard-Brak L, Richman DM, Chesnut SR, Little TD (2016) Social Communication Questionnaire scoring procedures for autism spectrum disorder and the prevalence of potential social communication disorder in ASD. Sch Psychol Q 31:522–533
Sanchack KE, Thomas CA (2016) Autism spectrum disorder: primary care principles. Am Fam Physician 94:972–979
Raymond LJ, Deth RC, Ralston NV (2014) Potential role of selenoenzymes and antioxidant metabolism in relation to autism etiology and pathology. Autism Res Treat 2014:164938. https://doi.org/10.1155/2014/164938
Endreffy I, Bjørklund G, Dicső F, Urbina MA, Endreffy E (2016) Acid glycosaminoglycan (aGAG) excretion is increased in children with autism spectrum disorder, and it can be controlled by diet. Metab Brain Dis 31:273–278
Symes W, Humphrey N (2010) Peer-group indicators of social inclusion among pupils with autistic spectrum disorders (ASD) in mainstream secondary schools: a comparative study. Sch Psychol Int 31:478–494
Saad K, Abdel-rahman AA, Elserogy YM, Al-Atram AA, Cannell JJ, Bjørklund G, Abdel-Reheim MK, Othman HA et al (2016) Vitamin D status in autism spectrum disorders and the efficacy of vitamin D supplementation in autistic children. Nutr Neurosci 19:346–351
Al-Ayadhi LY, Elamin NE (2013) Camel milk as a potential therapy as an antioxidant in autism spectrum disorder (ASD). Evid Based Complement Alternat Med 2013:602834. https://doi.org/10.1155/2013/602834
Schaafsma SM, Gagnidze K, Reyes A, Norstedt N, Månsson K, Francis K, Pfaff DW (2017) Sex-specific gene–environment interactions underlying ASD-like behaviors. Proc Natl Acad Sci U S A 114:1383–1388. https://doi.org/10.1073/pnas.1619312114
Skaper SD, Facci L, Zusso M, Giusti P (2018) An inflammation-centric view of neurological disease: beyond the neuron. Front Cell Neurosci 12:72. https://doi.org/10.3389/fncel.2018.00072
Herbert MR (2011) SHANK3, the synapse, and autism. N Engl J Med 365:173–175
Bjørklund G, Saad K, Chirumbolo S, Kern JK, Geier DA, Geier MR, Urbina MA (2016) Immune dysfunction and neuroinflammation in autism spectrum disorder. Acta Neurobiol Exp (Wars) 76:257–268
Roberts AL, Lyall K, Hart JE, Laden F, Just AC, Bobb JF, Koenen KC, Ascherio A et al (2013) Perinatal air pollutant exposures and autism spectrum disorder in the children of nurses’ health study II participants. Environ Health Perspect 121:978–984. https://doi.org/10.1289/ehp.1206187
Surén P, Roth C, Bresnahan M, Haugen M, Hornig M, Hirtz D, Lie KK, Lipkin WI et al (2013) Association between maternal use of folic acid supplements and risk of autism spectrum disorders in children. JAMA 309:570–577
Atladóttir HÓ, Thorsen P, Østergaard L, Schendel DE, Lemcke S, Abdallah M, Parner ET (2010) Maternal infection requiring hospitalization during pregnancy and autism spectrum disorders. J Autism Dev Disord 40:1423–1430
Hepel M, Stobiecka M (2011) Interactions of herbicide atrazine with DNA. Nova Science Publishers, New York
Stobiecka M, Prance A, Coopersmith K, Hepel M (2011) Antioxidant effectiveness in preventing paraquat-mediated oxidative DNA damage in the presence of H2O2. Oxford University Press, Washington
Bjørklund G, Skalny AV, Rahman MM, Dadar M, Yassa HA, Aaseth J, Chirumbolo S, Skalnaya MG et al (2018) Toxic metal(loid)-based pollutants and their possible role in autism spectrum disorder. Environ Res 166:234–250
Skalny AV, Simashkova NV, Skalnaya AA, Klyushnik TP, Bjørklund G, Skalnaya MG, Tinkov AA (2017) Assessment of gender and age effects on serum and hair trace element levels in children with autism spectrum disorder. Metab Brain Dis 32:1675–1684
Cipolla CM, Lodhi IJ (2017) Peroxisomal dysfunction in age-related diseases. Trends Endocrinol Metab 28:297–308
Islam MT (2017) Oxidative stress and mitochondrial dysfunction-linked neurodegenerative disorders. Neurol Res 39:73–82
Fransen M, Nordgren M, Wang B, Apanasets O (2012) Role of peroxisomes in ROS/RNS-metabolism: implications for human disease. Biochim Biophys Acta 1822:1363–1373. https://doi.org/10.1016/j.bbadis.2011.12.001
Chauhan A, Gu F, Essa MM, Wegiel J, Kaur K, Brown WT, Chauhan V (2011) Brain region-specific deficit in mitochondrial electron transport chain complexes in children with autism. J Neurochem 117:209–220
Chauhan A, Chauhan V, Brown WT, Cohen I (2004) Oxidative stress in autism: increased lipid peroxidation and reduced serum levels of ceruloplasmin and transferrin-the antioxidant proteins. Life Sci 75:2539–2549
Essa MM, Guillemin GJ, Waly MI, Al-Sharbati MM, Al-Farsi YM, Hakkim FL, Ali A, Al-Shafaee MS (2012) Increased markers of oxidative stress in autistic children of the Sultanate of Oman. Biol Trace Elem Res 147:25–27
Altun H, Şahin N, Kurutaş EB, Karaaslan U, Sevgen FH, Fındıklı E (2018) Assessment of malondialdehyde levels, superoxide dismutase, and catalase activity in children with autism spectrum disorders. Psychiatry Clin Psychopharmacol 28:408–415. https://doi.org/10.1080/24750573.2018.1470360
González-Fraguela ME, Hung ML, Vera H, Maragoto C, Noris E, Blanco L, Galvizu R, Robinson M (2013) Oxidative stress markers in children with autism spectrum disorders. Br J Med Med Res 3:307–317. https://doi.org/10.9734/BJMMR/2013/2335
Zoroglu SS, Armutcu F, Ozen S, Gurel A, Sivasli E, Yetkin O, Meram I (2004) Increased oxidative stress and altered activities of erythrocyte free radical scavenging enzymes in autism. Eur Arch Psychiatry Clin Neurosci 254:143–147
Ming X, Stein T, Brimacombe M, Johnson W, Lambert G, Wagner G (2005) Increased excretion of a lipid peroxidation biomarker in autism. Prostaglandins Leukot Essent Fatty Acids 73:379–384
Evans TA, Siedlak SL, Lu L, Fu X, Wang Z, McGinnis WR, Fakhoury E, Castellani RJ et al (2008) The autistic phenotype exhibits a remarkably localized modification of brain protein by products of free radical-induced lipid oxidation. Am J Biochem Biotechnol 4:61–72
Sajdel-Sulkowska E, Lipinski B, Windom H, Audhya T, McGinnis W (2008) Oxidative stress in autism: elevated cerebellar 3-nitrotyrosine levels. Am J Biochem Biotechnol 4:73–84
Söğüt S, Zoroğlu SS, Özyurt H, Yılmaz HR, Özuğurlu F, Sivaslı E, Yetkin Ö, Yanık M et al (2003) Changes in nitric oxide levels and antioxidant enzyme activities may have a role in the pathophysiological mechanisms involved in autism. Clin Chim Acta 331:111–117
Yorbik O, Sayal A, Akay C, Akbiyik D, Sohmen T (2002) Investigation of antioxidant enzymes in children with autistic disorder. Prostaglandins Leukot Essent Fatty Acids 67:341–343
Al-Gadani Y, El-Ansary A, Attas O, Al-Ayadhi L (2009) Metabolic biomarkers related to oxidative stress and antioxidant status in Saudi autistic children. Clin Biochem 42:1032–1040
Al-Yafee YA, Al-Ayadhi LY, Haq SH, El-Ansary AK (2011) Novel metabolic biomarkers related to sulfur-dependent detoxification pathways in autistic patients of Saudi Arabia. BMC Neurol 11:139. https://doi.org/10.1186/1471-2377-11-139
James SJ, Cutler P, Melnyk S, Jernigan S, Janak L, Gaylor DW, Neubrander JA (2004) Metabolic biomarkers of increased oxidative stress and impaired methylation capacity in children with autism. Am J Clin Nutr 80:1611–1617
Geier DA, Kern JK, Garver CR, Adams JB, Audhya T, Nataf R, Geier MR (2009) Biomarkers of environmental toxicity and susceptibility in autism. J Neurol Sci 280:101–108
Geier DA, Kern JK, Garver CR, Adams JB, Audhya T, Geier MR (2009) A prospective study of transsulfuration biomarkers in autistic disorders. Neurochem Res 34:386–393. https://doi.org/10.1007/s11064-008-9782-x
James SJ, Melnyk S, Jernigan S, Cleves MA, Halsted CH, Wong DH, Cutler P, Bock K et al (2006) Metabolic endophenotype and related genotypes are associated with oxidative stress in children with autism. Am J Med Genet B Neuropsychiatr Genet 141:947–956
Melnyk S, Fuchs GJ, Schulz E, Lopez M, Kahler SG, Fussell JJ, Bellando J, Pavliv O et al (2012) Metabolic imbalance associated with methylation dysregulation and oxidative damage in children with autism. J Autism Dev Disord 42:367–377
James SJ, Melnyk S, Fuchs G, Reid T, Jernigan S, Pavliv O, Hubanks A, Gaylor DW (2008) Efficacy of methylcobalamin and folinic acid treatment on glutathione redox status in children with autism. Am J Clin Nutr 89:425–430
Pintaudi M, Veneselli E, Voci A, Vignoli A, Castiglione D, Calevo MG, Grasselli E, Ragazzoni M et al (2016) Blood oxidative stress and metallothionein expression in Rett syndrome: probing for markers. World J Biol Psychiatry 17:198–209. https://doi.org/10.3109/15622975.2015.1077990
Vergani L, Cristina L, Paola R, Luisa AM, Shyti G, Edvige V, Giuseppe M, Elena G et al (2011) Metals, metallothioneins and oxidative stress in blood of autistic children. Res Autism Spectr Disord 5:286–293
Nadeem A, Ahmad SF, Attia SM, AL-Ayadhi LY, Al-Harbi NO, Bakheet SA (2019) Dysregulated enzymatic antioxidant network in peripheral neutrophils and monocytes in children with autism. Prog Neuro-Psychopharmacol Biol Psychiatry 88:352–359
Eshraghi R, Deth RC, Mittal R, Aranke M, Kay S-IS, Moshiree B, Eshraghi A (2018) Early disruption of the microbiome leading to decreased antioxidant capacity and epigenetic changes: implications for the rise in autism. Front Cell Neurosci 12:256. https://doi.org/10.3389/fncel.2018.00256
Wang Y, Zhao S, Liu X, Zheng Y, Li L, Meng S (2018) Oxytocin improves animal behaviors and ameliorates oxidative stress and inflammation in autistic mice. Biomed Pharmacother 107:262–269
Messina A, Monda V, Sessa F, Valenzano A, Salerno M, Bitetti I, Precenzano F, Marotta R et al (2018) Sympathetic, metabolic adaptations, and oxidative stress in autism spectrum disorders: how far from physiology? Front Physiol 9:261. https://doi.org/10.3389/fphys.2018.00261
McDougle CJ, Carlezon WA Jr (2013) Neuroinflammation and autism: toward mechanisms and treatments. Neuropsychopharmacology 38:241–242. https://doi.org/10.1038/npp.2012.174
Rose S, Bennuri SC, Wynne R, Melnyk S, James SJ, Frye RE (2016) Mitochondrial and redox abnormalities in autism lymphoblastoid cells: a sibling control study. FASEB J 31:904–909
Yui K, Kawasaki Y, Yamada H, Ogawa S (2016) Oxidative stress and nitric oxide in autism spectrum disorder and other neuropsychiatric disorders. CNS Neurol Disord Drug Targets 15:587–596
Frye RE, James SJ (2014) Metabolic pathology of autism in relation to redox metabolism. Biomark Med 8:321–330
Tschinkel PFS, Bjørklund G, Conón LZZ, Chirumbolo S, Nascimento VA (2018) Plasma concentrations of the trace elements copper, zinc and selenium in Brazilian children with autism spectrum disorder. Biomed Pharmacother 106:605–609
Macedoni-Lukšič M, Gosar D, Bjørklund G, Oražem J, Kodrič J, Lešnik-Musek P, Zupančič M, France-Štiglic A et al (2015) Levels of metals in the blood and specific porphyrins in the urine in children with autism spectrum disorders. Biol Trace Elem Res 163:2–10
Mostafa GA, Bjørklund G, Urbina MA, Al-Ayadhi LY (2016) The levels of blood mercury and inflammatory-related neuropeptides in the serum are correlated in children with autism spectrum disorder. Metab Brain Dis 31:593–599
Liu X, Cao S, Zhang X (2015) Modulation of gut microbiota–brain axis by probiotics, prebiotics, and diet. J Agric Food Chem 63:7885–7895
Doenyas C (2018) Gut microbiota, inflammation, and probiotics on neural development in autism spectrum disorder. Neuroscience 374:271–286
Frye RE, Rose S, Slattery J, MacFabe DF (2015) Gastrointestinal dysfunction in autism spectrum disorder: the role of the mitochondria and the enteric microbiome. Microb Ecol Health Dis 26:27458. https://doi.org/10.3402/mehd.v26.27458
Rose S, Bennuri SC, Murray KF, Buie T, Winter H, Frye RE (2017) Mitochondrial dysfunction in the gastrointestinal mucosa of children with autism: a blinded case-control study. PLoS One 12:e0186377. https://doi.org/10.1371/journal.pone.0186377
McElhanon BO, McCracken C, Karpen S, Sharp WG (2014) Gastrointestinal symptoms in autism spectrum disorder: a meta-analysis. Pediatrics 133:872–883
Adams JB, Johansen LJ, Powell LD, Quig D, Rubin RA (2011) Gastrointestinal flora and gastrointestinal status in children with autism–comparisons to typical children and correlation with autism severity. BMC Gastroenterol 11:22. https://doi.org/10.1186/1471-230X-11-22
Chirumbolo S, Bjørklund G (2017) PERM hypothesis: the fundamental machinery able to elucidate the role of xenobiotics and hormesis in cell survival and homeostasis. Int J Mol Sci 18. https://doi.org/10.3390/ijms18010165
Costanzo M, Boschi F, Carton F, Conti G, Covi V, Tabaracci G, Sbarbati A, Malatesta M (2018) Low ozone concentrations promote adipogenesis in human adipose-derived adult stem cells. Eur J Histochem:62. https://doi.org/10.4081/ejh.2018.2969
Galiè M, Costanzo M, Nodari A, Boschi F, Calderan L, Mannucci S, Covi V, Tabaracci G et al (2018) Mild ozonisation activates antioxidant cell response by the Keap1/Nrf2 dependent pathway. Free Radic Biol Med 124:114–121. https://doi.org/10.1016/j.freeradbiomed.2018.05.093
Moldogazieva N, Mokhosoev I, Feldman N, Lutsenko S (2018) ROS and RNS signalling: adaptive redox switches through oxidative/nitrosative protein modifications. Free Radic Res 52:507–543. https://doi.org/10.1080/10715762.2018
Bjørklund G, Kern JK, Urbina MA, Saad K, ElHoufey AA, Geier DA, Chirumbolo S, Geier MR, Mehta JA, Aaseth J (2018) Cerebral hypoperfusion in autism spectrum disorder. Acta Neurobiol Exp 78:9. https://doi.org/10.21307/ane-2018-005
Russo FB, Freitas BC, Pignatari GC, Fernandes IR, Sebat J, Muotri AR, Beltrão-Braga PCB (2018) Modeling the interplay between neurons and astrocytes in autism using human induced pluripotent stem cells. Biol Psychiatry 83:569–578
Niki E (2016) Oxidative stress and antioxidants: distress or eustress? Arch Biochem Biophys 595:19–24
Taetzsch T, Levesque S, McGraw C, Brookins S, Luqa R, Bonini MG, Mason RP, Oh U et al (2015) Redox regulation of NF-κB p50 and M1 polarization in microglia. Glia 63:423–440
El-Ansary A, Bjørklund G, Khemakhem AM, Al-Ayadhi L, Chirumbolo S, Ben Bacha A (2018) Metabolism-associated markers and Childhood Autism Rating Scales (CARS) as a measure of autism severity. J Mol Neurosci 65:265–276. https://doi.org/10.1007/s12031-018-1091-5
Granot E, Kohen R (2004) Oxidative stress in childhood—in health and disease states. Clin Nutr 23:3–11
Dmitriev L (2007) The involvement of lipid radical cycles and the adenine nucleotide translocator in neurodegenerative diseases. J Alzheimers Dis 11:183–190
Patti ME, Corvera S (2010) The role of mitochondria in the pathogenesis of type 2 diabetes. Endocr Rev 31:364–395
Tripathy BC, Oelmüller R (2012) Reactive oxygen species generation and signaling in plants. Plant Signal Behav 7:1621–1633. https://doi.org/10.4161/psb.22455
Murphy MP (2013) Mitochondrial dysfunction indirectly elevates ROS production by the endoplasmic reticulum. Cell Metab 18:145–146. https://doi.org/10.1016/j.cmet.2013.07.006
Haile Y, Deng X, Ortiz-Sandoval C, Tahbaz N, Janowicz A, Lu J-Q, Kerr BJ, Gutowski NJ et al (2017) Rab32 connects ER stress to mitochondrial defects in multiple sclerosis. J Neuroinflammation 14:19. https://doi.org/10.1186/s12974-016-0788-z
Ma Q (2013) Role of nrf2 in oxidative stress and toxicity. Annu Rev Pharmacol Toxicol 53:401–426. https://doi.org/10.1146/annurev-pharmtox-011112-140320
Antunes dos Santos A, Ferrer B, Marques Gonçalves F, Tsatsakis A, Renieri E, Skalny A, Farina M, Rocha J et al (2018) Oxidative stress in methylmercury-induced cell toxicity. Toxics:6. https://doi.org/10.3390/toxics6030047
Nguyen T, Nioi P, Pickett CB (2009) The Nrf2-antioxidant response element signaling pathway and its activation by oxidative stress. J Biol Chem 284:13291–13295
Yamazaki H, Tanji K, Wakabayashi K, Matsuura S, Itoh K (2015) Role of the Keap1/Nrf2 pathway in neurodegenerative diseases. Pathol Int 65:210–219
Kansanen E, Kuosmanen SM, Leinonen H, Levonen A-L (2013) The Keap1-Nrf2 pathway: mechanisms of activation and dysregulation in cancer. Redox Biol 1:45–49. https://doi.org/10.1016/j.redox.2012.10.001
Singh K, Connors SL, Macklin EA, Smith KD, Fahey JW, Talalay P, Zimmerman AW (2014) Sulforaphane treatment of autism spectrum disorder (ASD). Proc Natl Acad Sci U S A 111:15550–15555. https://doi.org/10.1073/pnas.1416940111
Calabrese V, Giordano J, Ruggieri M, Berritta D, Trovato A, Ontario M, Bianchini R, Calabrese E (2016) Hormesis, cellular stress response, and redox homeostasis in autism spectrum disorders. J Neurosci Res 94:1488–1498
Sandberg M, Patil J, D'angelo B, Weber SG, Mallard C (2014) NRF2-regulation in brain health and disease: implication of cerebral inflammation. Neuropharmacology 79:298–306
Takemoto AS, Berry MJ, Bellinger FP (2010) Role of selenoprotein P in Alzheimer’s disease. Ethn Dis 20(1 Suppl 1):S1-92-5
Solovyev ND (2015) Importance of selenium and selenoprotein for brain function: from antioxidant protection to neuronal signalling. J Inorg Biochem 153:1–12
Solovyev N, Drobyshev E, Bjørklund G, Dubrovskii Y, Lysiuk R, Rayman MP (2018) Selenium, selenoprotein P, and Alzheimer’s disease: is there a link? Free Radic Biol Med 127:124–133. https://doi.org/10.1016/j.freeradbiomed.2018.02.030
Chauhan A, Chauhan V (2006) Oxidative stress in autism. Pathophysiology 13:171–181
Bell J, MacKinlay E, Dick J, MacDonald D, Boyle R, Glen A (2004) Essential fatty acids and phospholipase A2 in autistic spectrum disorders. Prostaglandins Leukot Essent Fatty Acids 71:201–204
Osredkar J, Gosar D, Maček J, Kumer K, Fabjan T, Finderle P, Šterpin S, Zupan M et al (2019) Urinary markers of oxidative stress in children with autism spectrum disorder (ASD). Antioxidants (Basel) 8. https://doi.org/10.3390/antiox8060187
Chauhan A, Chauhan V, Brown T (2010) Autism: oxidative stress, inflammation, and immune abnormalities. CRC Press, Boca Raton
McGinnis WR (2004) Oxidative stress in autism. Altern Ther Health Med 10:22–36
Parker W, Hornik CD, Bilbo S, Holzknecht ZE, Gentry L, Rao R, Lin SS, Herbert MR et al (2017) The role of oxidative stress, inflammation and acetaminophen exposure from birth to early childhood in the induction of autism. J Int Med Res 45:407–438
Bernhoft R, Buttar R (2008) Autism: a multi-system oxidative and inflammatory disorder. Townsend Letter 86–90
James SJ, Rose S, Melnyk S, Jernigan S, Blossom S, Pavliv O, Gaylor DW (2009) Cellular and mitochondrial glutathione redox imbalance in lymphoblastoid cells derived from children with autism. FASEB J 23:2374–2383
Meguid NA, Dardir AA, Abdel-Raouf ER, Hashish A (2011) Evaluation of oxidative stress in autism: defective antioxidant enzymes and increased lipid peroxidation. Biol Trace Elem Res 143:58–65
Rose S, Melnyk S, Trusty TA, Pavliv O, Seidel L, Li J, Nick T, James SJ (2012) Intracellular and extracellular redox status and free radical generation in primary immune cells from children with autism. Autism Res Treat 2012:986519. https://doi.org/10.1155/2012/986519
Yao Y, Walsh WJ, McGinnis WR, Praticò D (2006) Altered vascular phenotype in autism: correlation with oxidative stress. Arch Neurol 63:1161–1164
Fatemi SH, Aldinger KA, Ashwood P, Bauman ML, Blaha CD, Blatt GJ, Chauhan A, Chauhan V et al (2012) Consensus paper: pathological role of the cerebellum in autism. Cerebellum 11:777–807
Ming X, Johnson WG, Stenroos ES, Mars A, Lambert GH, Buyske S (2010) Genetic variant of glutathione peroxidase 1 in autism. Brain and Development 32:105–109
Williams TA, Mars AE, Buyske SG, Stenroos ES, Wang R, Factura-Santiago MF, Lambert GH, Johnson WG (2007) Risk of autistic disorder in affected offspring of mothers with a glutathione S-transferase P1 haplotype. Arch Pediatr Adolesc Med 161:356–361
Serajee FJ, Nabi R, Zhong H, Mahbubul Huq A (2004) Polymorphisms in xenobiotic metabolism genes and autism. J Child Neurol 19:413–417
Paşca SP, Nemeş B, Vlase L, Gagyi CE, Dronca E, Miu AC, Dronca M (2006) High levels of homocysteine and low serum paraoxonase 1 arylesterase activity in children with autism. Life Sci 78:2244–2248
Posar A, Visconti P (2017) Autism in 2016: the need for answers. J Pediatr 93:111–119. https://doi.org/10.1016/j.jped.2016.09.002
Grabrucker AM (2013) Environmental factors in autism. Front Psychiatry 3:118. https://doi.org/10.3389/fpsyt.2012.00118
Streit WJ, Mrak RE, Griffin WST (2004) Microglia and neuroinflammation: a pathological perspective. J Neuroinflammation 1:14. https://doi.org/10.1186/1742-2094-1-14
Deth R, Muratore C, Benzecry J, Power-Charnitsky VA, Waly M (2008) How environmental and genetic factors combine to cause autism: a redox/methylation hypothesis. Neurotoxicology 29:190–201
Muratore CR, Hodgson NW, Trivedi MS, Abdolmaleky HM, Persico AM, Lintas C, De La Monte S, Deth RC (2013). Age-dependent decrease and alternative splicing of methionine synthase mRNA in human cerebral cortex and an accelerated decrease in autism. PLoS One 2013;8:e56927. https://doi.org/10.1371/journal.pone.0056927
Buie T, Campbell DB, Fuchs GJ 3rd, Furuta GT, Levy J, Vandewater J, Whitaker AH, Atkins D et al (2010) Evaluation, diagnosis, and treatment of gastrointestinal disorders in individuals with ASDs: a consensus report. Pediatrics 125(Suppl 1):S1–S18. https://doi.org/10.1542/peds.2009-1878C10.1542/peds.2009-1878C
Pastural E, Ritchie S, Lu Y, Jin W, Kavianpour A, Khine Su-Myat K, Heath D, Wood PL et al (2009) Novel plasma phospholipid biomarkers of autism: mitochondrial dysfunction as a putative causative mechanism. Prostaglandins Leukot Essent Fatty Acids 81:253–264. https://doi.org/10.1016/j.plefa.2009.06.003
Rossignol DA, Frye RE (2012) A review of research trends in physiological abnormalities in autism spectrum disorders: immune dysregulation, inflammation, oxidative stress, mitochondrial dysfunction and environmental toxicant exposures. Mol Psychiatry 17:389–401. https://doi.org/10.1038/mp.2011.165
Rossignol D, Frye R (2012) Mitochondrial dysfunction in autism spectrum disorders: a systematic review and meta-analysis. Mol Psychiatry 17:290–314. https://doi.org/10.1038/mp.2010.136
Xia W, Zhou Y, Sun C, Wang J, Wu L (2010) A preliminary study on nutritional status and intake in Chinese children with autism. Eur J Pediatr 169:1201–1206
Chauhan V, Chauhan A, Cohen IL, Brown WT, Sheikh A (2004) Alteration in amino-glycerophospholipids levels in the plasma of children with autism: a potential biochemical diagnostic marker. Life Sci 74:1635–1643
Jain SK (1985) In vivo externalization of phosphatidylserine and phosphatidylethanolamine in the membrane bilayer and hypercoagulability by the lipid peroxidation of erythrocytes in rats. J Clin Invest 76:281–286
Peet M, Murphy B, Shay J, Horrobin D (1998) Depletion of omega-3 fatty acid levels in red blood cell membranes of depressive patients. Biol Psychiatry 43:315–319
Halliwell B, Gutteridge JM (1999) Free radicals, other reactive species and disease. In: Halliwell B, Gutteridge JM (eds) Free radicals in biology and medicine. Clarendon Press, Oxford, pp. 617–783
Jory J, McGinnis WR (2008) Red-cell trace minerals in children with autism. Am J Biochem Biotechnol 4:101–104
Stockler-Pinto M, Mafra D, Farage N, Boaventura G, Cozzolino S (2010) Effect of Brazil nut supplementation on the blood levels of selenium and glutathione peroxidase in hemodialysis patients. Nutrition 26:1065–1069
Fang YZ, Yang S, Wu G (2002) Free radicals, antioxidants, and nutrition. Nutrition 18:872–879
Santamaría A, Salvatierra-Sánchez R, Vázquez-Román B, Santiago-López D, Villeda-Hernández J, Galván-Arzate S, Jiménez-Capdeville ME, Ali SF (2003) Protective effects of the antioxidant selenium on quinolinic acid-induced neurotoxicity in rats: In vitro and in vivo studies. J Neurochem 86:479–488
Skalny AV, Skalnaya MG, Bjørklund G, Gritsenko VA, Aaseth J, Tinkov AA (2018) Selenium and autism spectrum disorder. In: Michalke B (ed) Selenium. Molecular and Integrative Toxicology. Springer, Cham, pp. 193–210
Cadenas E (2004) Mitochondrial free radical production and cell signaling. Mol Asp Med 25:17–26
Song J, Park J, Oh Y, Lee JE (2015) Glutathione suppresses cerebral infarct volume and cell death after ischemic injury: involvement of FOXO3 inactivation and Bcl2 expression. Oxidative Med Cell Longev 2015:426069. https://doi.org/10.1155/2015/426069
Boris M, Goldblatt A, Galanko J, James SJ (2004) Association of MTHFR gene variants with autism. J Am Phys Surg 9:106–108
Bowers K, Li Q, Bressler J, Avramopoulos D, Newschaffer C, Fallin MD (2011) Glutathione pathway gene variation and risk of autism spectrum disorders. J Neurodev Disord 3:132–143. https://doi.org/10.1007/s11689-011-9077-4
Frustaci A, Neri M, Cesario A, Adams JB, Domenici E, Dalla Bernardina B, Bonassi S (2012) Oxidative stress-related biomarkers in autism: systematic review and meta-analyses. Free Radic Biol Med 52:2128–2141
Goin-Kochel RP, Porter AE, Peters SU, Shinawi M, Sahoo T, Beaudet AL (2009) The MTHFR 677C→ T polymorphism and behaviors in children with autism: exploratory genotype–phenotype correlations. Autism Res 2:98–108
Guo T, Chen H, Liu B, Ji W, Yang C (2012) Methylenetetrahydrofolate reductase polymorphisms C677T and risk of autism in the Chinese Han population. Genet Test Mol Biomarkers 16:968–973. https://doi.org/10.1089/gtmb.2012.0091
Adams J, Baral M, Geis E, Mitchell J, Ingram J, Hensley A, Zappia I, Newmark S et al (2009) The severity of autism is associated with toxic metal body burden and red blood cell glutathione levels. J Toxicol 2009:532640. https://doi.org/10.1155/2009/532640
Ghezzo A, Visconti P, Abruzzo PM, Bolotta A, Ferreri C, Gobbi G, Malisardi G, Manfredini S et al (2013) Oxidative stress and erythrocyte membrane alterations in children with autism: correlation with clinical features. PLoS One 8:e66418. https://doi.org/10.1371/journal.pone.0066418
Gorrindo P, Lane CJ, Lee EB, McLaughlin B, Levitt P (2013) Enrichment of elevated plasma F2t-isoprostane levels in individuals with autism who are stratified by presence of gastrointestinal dysfunction. PLoS One 8:e68444. https://doi.org/10.1371/journal.pone.0068444
Coyle P, Philcox J, Carey L, Rofe A (2002) Metallothionein: the multipurpose protein. Cell Mol Life Sci 59:627–647
Alonso-Gonzalez C, Mediavilla D, Martinez-Campa C, Gonzalez A, Cos S, Sanchez-Barcelo EJ (2008) Melatonin modulates the cadmium-induced expression of MT-2 and MT-1 metallothioneins in three lines of human tumor cells (MCF-7, MDA-MB-231 and HeLa). Toxicol Lett 181:190–195
Uchida Y, Takio K, Titani K, Ihara Y, Tomonaga M (1991) The growth inhibitory factor that is deficient in the Alzheimer’s disease brain is a 68 amino acid metallothionein-like protein. Neuron 7:337–347
Haq F, Mahoney M, Koropatnick J (2003) Signaling events for metallothionein induction. Mutat Res 533:211–226
Lanza C, Morando S, Voci A, Canesi L, Principato MC, Serpero LD, Mancardi G, Uccelli A et al (2009) Neuroprotective mesenchymal stem cells are endowed with a potent antioxidant effect in vivo. J Neurochem 110:1674–1684
Penkowa M, Sørensen BL, Nielsen SL, Hansen PB (2009) Metallothionein as a useful marker in Hodgkin lymphoma subclassification. Leuk Lymphoma 50:200–210
Vergani L, Lanza C, Borghi C, Scarabelli L, Panfoli I, Burlando B, Dondero F, Viarengo A et al (2007) Efects of growth hormone and cadmium on the transcription regulation of two metallothionein isoforms. Mol Cell Endocrinol 263:29–37
Singh VK, Hanson J (2006) Assessment of metallothionein and antibodies to metallothionein in normal and autistic children having exposure to vaccine-derived thimerosal. Pediatr Allergy Immunol 17:291–296
Rossignol DA, Frye RE (2014) Evidence linking oxidative stress, mitochondrial dysfunction, and inflammation in the brain of individuals with autism. Front Physiol 5:150. https://doi.org/10.3389/fphys.2014.00150
Muthaiyah B, Essa M, Chauhan V, Brown W, Wegiel J, Chauhan A (2009) Increased lipid peroxidation in cerebellum and temporal cortex of brain in autism: Op04-02. J Neurochem 108(Suppl. 1):73
Chauhan A, Audhya T, Chauhan V (2011) Increased DNA oxidation in the cerebellum, frontal and temporal cortex of brain in autism. Trans Am Soc Neurochem 42:81
Sajdel-Sulkowska EM, Xu M, Koibuchi N (2009) Increase in cerebellar neurotrophin-3 and oxidative stress markers in autism. Cerebellum 8:366–372
Yui K, Tanuma N, Yamada H, Kawasaki Y (2017) Decreased total antioxidant capacity has a larger effect size than increased oxidant levels in urine in individuals with autism spectrum disorder. Environ Sci Pollut Res Int 24:9635–9644. https://doi.org/10.1007/s11356-017-8595-3
Lopez-Hurtado E, Prieto JJ (2008) A microscopic study of language-related cortex in autism. Am J Biochem Biotechnol 4:130–145
Chauhan A, Audhya T, Chauhan V (2012) Brain region-specific glutathione redox imbalance in autism. Neurochem Res 37:1681–1689
Rose S, Melnyk S, Pavliv O, Bai S, Nick T, Frye R, James S (2012) Evidence of oxidative damage and inflammation associated with low glutathione redox status in the autism brain. Transl Psychiatry 2:e134. https://doi.org/10.1038/tp.2012.61
Freeman LR, Keller JN (2012) Oxidative stress and cerebral endothelial cells: regulation of the blood–brain-barrier and antioxidant based interventions. Biochim Biophys Acta 1822:822–829. https://doi.org/10.1016/j.bbadis.2011.12.009
Ballabh P, Braun A, Nedergaard M (2004) The blood–brain barrier: an overview: structure, regulation, and clinical implications. Neurobiol Dis 16:1–13
Ellwanger JH, Franke SI, Bordin DL, Pra D, Henriques JA (2016) Biological functions of selenium and its potential influence on Parkinson’s disease. An Acad Bras Cienc 88:1655–1674
Brigelius-Flohé R, Maiorino M (2013) Glutathione peroxidases. Biochim Biophys Acta 1830:3289–3303. https://doi.org/10.1016/j.bbagen.2012.11.020
Sultan CS, Saackel A, Stank A, Fleming T, Fedorova M, Hoffmann R, Wade RC, Hecker M et al (2018) Impact of carbonylation on glutathione peroxidase-1 activity in human hyperglycemic endothelial cells. Redox Biol 16:113–122
Haorah J, Ramirez SH, Schall K, Smith D, Pandya R, Persidsky Y (2007) Oxidative stress activates protein tyrosine kinase and matrix metalloproteinases leading to blood–brain barrier dysfunction. J Neurochem 101:566–576
Daneman R, Prat A (2015) The blood–brain barrier. Cold Spring Harb Perspect Biol 7:a020412. https://doi.org/10.1101/cshperspect.a020412
Abbott NJ, Patabendige AA, Dolman DE, Yusof SR, Begley DJ (2010) Structure and function of the blood–brain barrier. Neurobiol Dis 37:13–25
Liebner S, Czupalla CJ, Wolburg H (2011) Current concepts of blood-brain barrier development. Int J Dev Biol 55:467–476
Zlokovic BV (2008) The blood-brain barrier in health and chronic neurodegenerative disorders. Neuron 57:178–201
Tayarani I, Chaudiere J, Lefauconnier JM, Bourre JM (1987) Enzymatic protection against peroxidative damage in isolated brain capillaries. J Neurochem 48:1399–1402
Agarwal R, Shukla GS (1999) Potential role of cerebral glutathione in the maintenance of blood-brain barrier integrity in rat. Neurochem Res 24:1507–1514
Smeyne M, Smeyne RJ (2013) Glutathione metabolism and Parkinson’s disease. Free Radic Biol Med 62:13–25
Ghanizadeh A, Akhondzadeh S, Hormozi M, Makarem A, Abotorabi-Zarchi M, Firoozabadi A (2012) Glutathione-related factors and oxidative stress in autism, a review. Curr Med Chem 19:4000–4005
Gu Y, Dee CM, Shen J (2011) Interaction of free radicals, matrix metalloproteinases and caveolin-1 impacts blood-brain barrier permeability. Front Biosci (Schol Ed) 3:1216–1231
Gu Y, Zheng G, Xu M, Li Y, Chen X, Zhu W, Tong Y, Chung SK et al (2012) Caveolin-1 regulates nitric oxide-mediated matrix metalloproteinases activity and blood–brain barrier permeability in focal cerebral ischemia and reperfusion injury. J Neurochem 120:147–156
Tinggi U (2008) Selenium: Its role as antioxidant in human health. Environ Health Prev Med 13:102–108. https://doi.org/10.1007/s12199-007-0019-4
Halliwell B (2001) Role of free radicals in the neurodegenerative diseases. Drugs Aging 18:685–716
Catalá A (2009) Lipid peroxidation of membrane phospholipids generates hydroxy-alkenals and oxidized phospholipids active in physiological and/or pathological conditions. Chem Phys Lipids 157:1–11
Devasagayam T, Boloor K, Ramasarma T (2003) Methods for estimating lipid peroxidation: an analysis of merits and demerits. Indian J Biochem Biophys 40:300–308
Markesbery W, Lovell M (1998) Four-hydroxynonenal, a product of lipid peroxidation, is increased in the brain in Alzheimer’s disease. Neurobiol Aging 19:33–36
Butterfield DA, Bader Lange ML, Sultana R (2010) Involvements of the lipid peroxidation product, HNE, in the pathogenesis and progression of Alzheimer’s disease. Biochim Biophys Acta 1801:924–929. https://doi.org/10.1016/j.bbalip.2010.02.005
Zarkovic K (2003) 4-hydroxynonenal and neurodegenerative diseases. Mol Asp Med 24:293–303
Wang X, Michaelis EK (2010) Selective neuronal vulnerability to oxidative stress in the brain. Front Aging Neurosci 2:12. https://doi.org/10.3389/fnagi.2010.00012
Shulman RG, Rothman DL, Behar KL, Hyder F (2004) Energetic basis of brain activity: implications for neuroimaging. Trends Neurosci 27:489–495
Klein JA, Ackerman SL (2003) Oxidative stress, cell cycle, and neurodegeneration. J Clin Invest 111:785–793
Dávila D, Torres-Aleman I (2008) Neuronal death by oxidative stress involves activation of FOXO3 through a two-arm pathway that activates stress kinases and attenuates insulin-like growth factor I signaling. Mol Biol Cell 19:2014–2025
Lindqvist D, Dhabhar FS, James SJ, Hough CM, Jain FA, Bersani FS, Reus VI, Verhoeven JE et al (2017) Oxidative stress, inflammation and treatment response in major depression. Psychoneuroendocrinology 76:197–205
Morris G, Walder K, McGee SL, Dean OM, Tye SJ, Maes M, Berk M (2017) A model of the mitochondrial basis of bipolar disorder. Neurosci Biobehav Rev 74:1–20
Sawa A, Sedlak TW (2016) Oxidative stress and inflammation in schizophrenia. Schizophr Res 176:1–2
Swomley AM, Butterfield DA (2015) Oxidative stress in Alzheimer disease and mild cognitive impairment: evidence from human data provided by redox proteomics. Arch Toxicol 89:1669–1680
Erden-İnal M, Sunal E, Kanbak G (2002) Age-related changes in the glutathione redox system. Cell Biochem Funct 20:61–66
Feng C, Chen Y, Pan J, Yang A, Niu L, Min J, Meng X, Liao L et al (2017) Redox proteomic identification of carbonylated proteins in autism plasma: insight into oxidative stress and its related biomarkers in autism. Clin Proteomics 14:2. https://doi.org/10.1186/s12014-017-9138-0
Morakotsriwan N, Wattanathorn J, Kirisattayakul W, Chaisiwamongkol K (2016) Autistic-like behaviors, oxidative stress status, and histopathological changes in cerebellum of valproic acid rat model of autism are improved by the combined extract of purple rice and silkworm pupae. Oxidative Med Cell Longev 2016:3206561. https://doi.org/10.1155/2016/3206561
Poggi C, Dani C (2018) Sepsis and oxidative stress in the newborn: from pathogenesis to novel therapeutic targets. Oxidative Med Cell Longev 2018:9390140. https://doi.org/10.1155/2018/9390140
Schiavone S, Colaianna M, Curtis L (2015) Impact of early life stress on the pathogenesis of mental disorders: relation to brain oxidative stress. Curr Pharm Des 21:1404–1412
Brunst KJ, Baccarelli AA, Wright RJ (2015) Integrating mitochondriomics in children’s environmental health. J Appl Toxicol 35:976–991
Meguid NA, Anwar M, Bjørklund G, Hashish A, Chirumbolo S, Hemimi M, Sultan E (2017) Dietary adequacy of Egyptian children with autism spectrum disorder compared to healthy developing children. Metab Brain Dis 32:607–615
Main PA, Angley MT, Thomas P, O’Doherty CE, Fenech M (2010) Folate and methionine metabolism in autism: a systematic review. Am J Clin Nutr 91:1598–1620
Hegazy HG, Ali EH, Elgoly AHM (2015) Interplay between pro-inflammatory cytokines and brain oxidative stress biomarkers: evidence of parallels between butyl paraben intoxication and the valproic acid brain physiopathology in autism rat model. Cytokine 71:173–180
Chirumbolo S, Bjørklund G, Sboarina A, Vella A (2017) The role of vitamin D in the immune system as a pro-survival molecule. Clin Ther 39:894–916
Crăciun EC, Bjørklund G, Tinkov AA, Urbina MA, Skalny AV, Rad F, Dronca E (2016) Evaluation of whole blood zinc and copper levels in children with autism spectrum disorder. Metab Brain Dis 31:887–890
Al-Mosalem O, El-Ansary A, Attas O, Al-Ayadhi L (2009) Metabolic biomarkers related to energy metabolism in Saudi autistic children. Clin Biochem 42:949–957
Chez MG, Buchanan CP, Aimonovitch MC, Becker M, Schaefer K, Black C, Komen J (2002) Double-blind, placebo-controlled study of L-carnosine supplementation in children with autistic spectrum disorders. J Child Neurol 17:833–837
Hassan WM, Al-Ayadhi L, Bjørklund G, Alabdali A, Chirumbolo S, El-Ansary A (2018) The use of multi-parametric biomarker profiles may increase the accuracy of ASD prediction. J Mol Neurosci 66:85–101. https://doi.org/10.1007/s12031-018-1136-9
Montuschi P, Barnes PJ, Roberts LJ (2004) Isoprostanes: markers and mediators of oxidative stress. FASEB J 18:1791–1800
Qasem H, Al-Ayadhi L, El-Ansary A (2016). Cysteinyl leukotriene correlated with 8-isoprostane levels as predictive biomarkers for sensory dysfunction in autism. Lipids Health Dis 2016 Aug 17;15:130. https://doi.org/10.1186/s12944-016-0298-0
Zoroğlu SS, Yürekli M, Meram İ, Söğüt S, Tutkun H, Yetkin O, Sivasli E, Savaş HA et al (2003) Pathophysiological role of nitric oxide and adrenomedullin in autism. Cell Biochem Funct 21:55–60
Frye R, Rose S, Chacko J, Wynne R, Bennuri S, Slattery J, Tippett M, Delhey L et al (2016) Modulation of mitochondrial function by the microbiome metabolite propionic acid in autism and control cell lines. Transl Psychiatry 6:e927. https://doi.org/10.1038/tp.2016.189
Nakamura S, Shimazawa M, Hara H (2018) Physiological roles of metallothioneins in central nervous system diseases. Biol Pharm Bull 41:1006–1013
Mirończuk-Chodakowska I, Witkowska AM, Zujko ME (2018) Endogenous non-enzymatic antioxidants in the human body. Adv Med Sci 63:68–78
Stern BR, Solioz M, Krewski D, Aggett P, Aw TC, Baker S, Crump K, Dourson M et al (2007) Copper and human health: biochemistry, genetics, and strategies for modeling dose-response relationships. J Toxicol Environ Health B Crit Rev 10:157–222
Faber S, Zinn GM, Kern Ii JC, Skip Kingston H (2009) The plasma zinc/serum copper ratio as a biomarker in children with autism spectrum disorders. Biomarkers 14:171–180
Bjørklund G (2013) The role of zinc and copper in autism spectrum disorders. Acta Neurobiol Exp (Wars) 73:225–236
Borrás C, Sastre J, García-Sala D, Lloret A, Pallardó FV, Viña J (2003) Mitochondria from females exhibit higher antioxidant gene expression and lower oxidative damage than males. Free Radic Biol Med 34:546–552
Bjørklund G, Chirumbolo S (2017) Role of oxidative stress and antioxidants in daily nutrition and human health. Nutrition 33:311–321
Qasem H, Al-Ayadhi L, Bjørklund G, Chirumbolo S, El-Ansary A (2018) Impaired lipid metabolism markers to assess the risk of neuroinflammation in autism spectrum disorder. Metab Brain Dis 1–13
Zhang Q-b, Gao S-j, Zhao H-x (2015) Thioredoxin: a novel, independent diagnosis marker in children with autism. Int J Dev Neurosci 40:92–96
Lillig CH, Holmgren A (2007) Thioredoxin and related molecules–from biology to health and disease. Antioxid Redox Signal 9:25–47
Tinkov AA, Bjørklund G, Skalny AV, Holmgren A, Skalnaya MG, Chirumbolo S, Aaseth J (2018) The role of the thioredoxin/thioredoxin reductase system in the metabolic syndrome: towards a possible prognostic marker? Cell Mol Life Sci:1–20
Ghanizadeh A, Moghimi-Sarani E (2013) A randomized double blind placebo controlled clinical trial of N-acetylcysteine added to risperidone for treating autistic disorders. BMC Psychiatry 13:196. https://doi.org/10.1186/1471-244X-13-196
Kałużna-Czaplińska J, Żurawicz E, Michalska M, Rynkowski J (2013) A focus on homocysteine in autism. Acta Biochim Pol 60:137–142
Tu WJ, Yin CH, Guo YQ, Li SO, Chen H, Zhang Y, Feng YL, Long BH (2013) Serum homocysteine concentrations in Chinese children with autism. Clin Chem Lab Med 51:e19–e22. https://doi.org/10.1515/cclm-2012-0196
Endres D, van Elst LT, Meyer SA, Feige B, Nickel K, Bubl A, Riedel A, Ebert D et al (2017) Glutathione metabolism in the prefrontal brain of adults with high-functioning autism spectrum disorder: an MRS study. Mol Autism 8(1):10. https://doi.org/10.1186/s13229-017-0122-3
Kern JK, Geier DA, Sykes LK, Haley BE, Geier MR (2016) The relationship between mercury and autism: a comprehensive review and discussion. J Trace Elem Med Biol 37:8–24
Siddiqui MF, Elwell C, Johnson MH (2016) Mitochondrial dysfunction in autism spectrum disorders. Autism Open Access 6. https://doi.org/10.4172/2165-7890.1000190
Al-Otaish H, Al-Ayadhi L, Bjørklund G, Chirumbolo S, Urbina MA, El-Ansary A (2018) Relationship between absolute and relative ratios of glutamate, glutamine and GABA and severity of autism spectrum disorder. Metab Brain Dis 33:843–854
Rojas DC, Singel D, Steinmetz S, Hepburn S, Brown MS (2014) Decreased left perisylvian GABA concentration in children with autism and unaffected siblings. Neuroimage 86:28–34
El-Ansary A, Bjørklund G, Chirumbolo S, Alnakhli OM (2017) Predictive value of selected biomarkers related to metabolism and oxidative stress in children with autism spectrum disorder. Metab Brain Dis 32:1209–1221
Mawe G, Coates M, Moses P (2006) Intestinal serotonin signalling in irritable bowel syndrome. Aliment Pharmacol Ther 23:1067–1076
Montgomery AK, Shuffrey LC, Guter SJ, Anderson GM, Jacob S, Mosconi MW, Sweeney JA, Turner JB et al (2018) Maternal serotonin levels are associated with cognitive ability and core symptoms in autism spectrum disorder. J Am Acad Child Adolesc Psychiatry 57:867–875. https://doi.org/10.1016/j.jaac.2018.06.025
Edwards KA, Madden AM, Zup SL (2018) Serotonin receptor regulation as a potential mechanism for sexually dimorphic oxytocin dysregulation in a model of autism. Brain Res 1701:85–92
Ashwood P, Krakowiak P, Hertz-Picciotto I, Hansen R, Pessah I, Van de Water J (2011) Elevated plasma cytokines in autism spectrum disorders provide evidence of immune dysfunction and are associated with impaired behavioral outcome. Brain Behav Immun 25:40–45
Ahmad SF, Nadeem A, Ansari MA, Bakheet SA, Attia SM, Zoheir KM, Al-ayadhi LY, Alzahrani MZ et al (2017) Imbalance between the anti-and pro-inflammatory milieu in blood leukocytes of autistic children. Mol Immunol 82:57–65
Mostafa GA, Bjørklund G, Urbina MA, Al-Ayadhi LY (2016) The positive association between elevated blood lead levels and brain-specific autoantibodies in autistic children from low lead-polluted areas. Metab Brain Dis 31:1047–1054
Saad K, Elserogy Y, Al-Atram AA, Mohamad IL, ElMelegy TT, Bjørklund G, El-Houfy AA (2015) ADHD, autism and neuroradiological complications among phenylketonuric children in upper Egypt. Acta Neurol Belg 115:657–663
Skalny A, Simashkova N, Skalnaya M, Klyushnik T, Chernova L, Tinkov A (2018) Mercury and autism spectrum disorders (in Russian). Zh Nevrol Psikhiatr Im S S Korsakova 118:75–79. https://doi.org/10.17116/jnevro20181185275
Saghazadeh A, Rezaei N (2017) Systematic review and meta-analysis links autism and toxic metals and highlights the impact of country development status: Higher blood and erythrocyte levels for mercury and lead, and higher hair antimony, cadmium, lead, and mercury. Prog Neuro-Psychopharmacol Biol Psychiatry 79:340–368
Adams J, Howsmon DP, Kruger U, Geis E, Gehn E, Fimbres V, Pollard E, Mitchell J et al (2017) Significant association of urinary toxic metals and autism-related symptoms—a nonlinear statistical analysis with cross validation. PLoS One 12:e0169526. https://doi.org/10.1371/journal.pone.0169526
Qin YY, Jian B, Wu C, Jiang CZ, Kang Y, Zhou JX, Yang F, Liang Y (2018) A comparison of blood metal levels in autism spectrum disorder and unaffected children in Shenzhen of China and factors involved in bioaccumulation of metals. Environ Sci Pollut Res Int 25:17950–17956. https://doi.org/10.1007/s11356-018-1957-7
Wu J, Liu DJ, Shou XJ, Zhang JS, Meng FC, Liu YQ, Han SP, Zhang R et al (2018) Chinese children with autism: a multiple chemical elements profile in erythrocytes. Autism Res 11:834–845. https://doi.org/10.1002/aur.1949
Metwally FM, Abdelraoof ER, Rashad H, Hasheesh A, Elsedfy Z, Gebril O, Meguid N (2015) Toxic effect of some heavy metals in Egyptian autistic children. Int J Pharm Clin Res 7:206–211
Yasuda H, Yasuda Y, Tsutsui T (2013) Estimation of autistic children by metallomics analysis. Sci Rep 3:1199. https://doi.org/10.1038/srep01199
Yasuda H, Tsutsui T (2013) Assessment of infantile mineral imbalances in autism spectrum disorders (ASDs). Int J Environ Res Public Health 10:6027–6043
Mold M, Umar D, King A, Exley C (2018) Aluminium in brain tissue in autism. J Trace Elem Med Biol 46:76–82
Gorini F, Muratori F, Morales MA (2014) The role of heavy metal pollution in neurobehavioral disorders: a focus on autism. Rev J Autism Dev Disord 1:354–372. https://doi.org/10.1007/s40489-014-0028-3
Adams JB, Romdalvik J, Levine K, Hu LW (2008) Mercury in first-cut baby hair of children with autism versus typically-developing children. Toxicol Environ Chem 90:739–753
Geier DA, Kern JK, Geier MR (2017) Increased risk for an atypical autism diagnosis following thimerosal-containing vaccine exposure in the United States: a prospective longitudinal case-control study in the vaccine safety datalink. J Trace Elem Med Biol 42:18–24
Zhao Y, Zhao B (2013) Oxidative stress and the pathogenesis of Alzheimer’s disease. Oxidative Med Cell Longev 2013:316523. https://doi.org/10.1155/2013/316523
Bhat AH, Dar KB, Anees S, Zargar MA, Masood A, Sofi MA, Ganie SA (2015) Oxidative stress, mitochondrial dysfunction and neurodegenerative diseases; a mechanistic insight. Biomed Pharmacother 74:101–110
Yang X (2012) Oxidative stress and autism. Int J Pediatr 39:99–101
Hodgson NW, Waly MI, Al-Farsi YM, Al-Sharbati MM, Al-Farsi O, Ali A, Ouhtit A, Zang T et al (2014) Decreased glutathione and elevated hair mercury levels are associated with nutritional deficiency-based autism in Oman. Exp Biol Med 239:697–706
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Bjørklund, G., Meguid, N.A., El-Bana, M.A. et al. Oxidative Stress in Autism Spectrum Disorder. Mol Neurobiol 57, 2314–2332 (2020). https://doi.org/10.1007/s12035-019-01742-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12035-019-01742-2